

TL;DR
- Treat psychosocial hazards like physical hazards — the same risk-management cycle applies: identify, assess, control using the hierarchy, monitor, and review.
- Job design is the biggest driver — workload, pace, autonomy, and role clarity cause more harm than interpersonal conflict, yet most organisations only assess bullying and harassment.
- Default to the top of the hierarchy — EAPs and resilience training sit at the bottom; they must not replace job redesign, workload restructuring, or scheduling changes.
- Cross-jurisdictional duty is expanding — Australia now mandates the hierarchy of controls for psychosocial risks; the UK, EU, and Canada impose enforceable or strongly referenced duties; only the US lacks a specific standard.
- One-off assessments fail — psychosocial risk management is a continuous programme integrated into the OHS management system, not a filed compliance exercise.
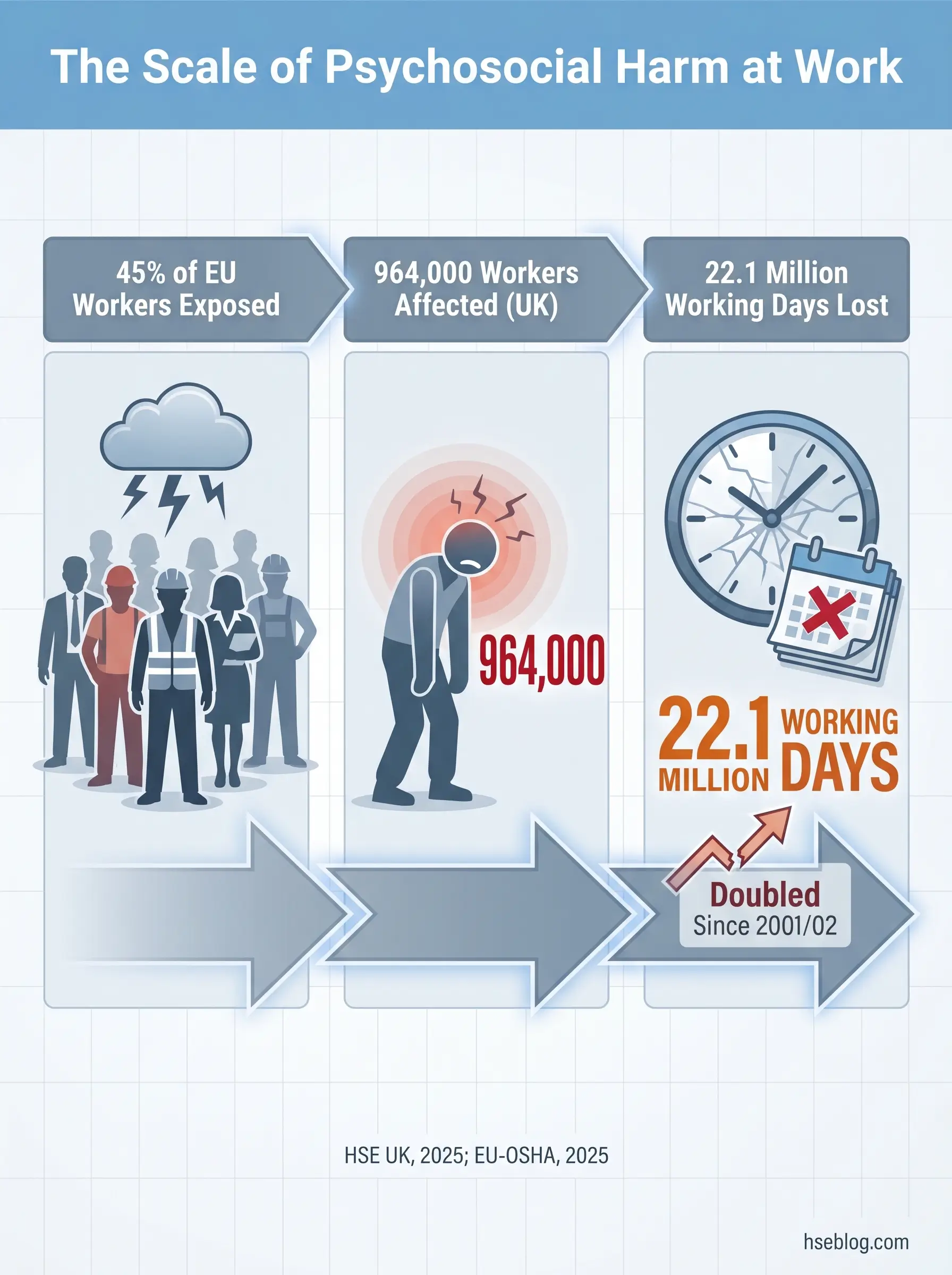
In 2024/25, 964,000 workers in Great Britain reported suffering from work-related stress, depression, or anxiety — the highest figure since records began and double the rate recorded in 2001/02 (HSE UK, 2025). Psychosocial risk factors at work are characteristics of job design, work organisation, social conditions, and management practices that have the potential to cause psychological or physical harm. Identifying and controlling these factors requires the same systematic process used for physical hazards: hazard identification, risk assessment, application of the hierarchy of controls, and ongoing review — now explicitly codified in frameworks including ISO 45003:2021 and Australia’s WHS Regulations.
Regulatory content here reflects general HSE professional understanding of the jurisdictions referenced, current as of early 2026. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.
That single statistic from HSE UK’s November 2025 annual release landed heavily across the occupational health community. Stress, depression, and anxiety now account for approximately 22.1 million lost working days annually in Great Britain alone — more than half of all work-related ill health (HSE UK, 2025). The numbers represent a system-level failure, not an epidemic of individual fragility.
The cost is simultaneously human and institutional. HSE UK estimates workplace injuries and new cases of work-related ill health cost the UK economy £22.9 billion per year (HSE UK, 2025). Across the EU, nearly 45% of workers report facing risk factors that can adversely affect their mental health (EU-OSHA, 2025). This article maps what those risk factors are, how to identify them with rigour, and how to control them using the same hierarchy that governs every other workplace hazard — because that is exactly what they are.
What Are Psychosocial Risk Factors at Work?
Psychosocial risk factors are the specific characteristics of how work is designed, organised, managed, and socially experienced that carry the potential to cause psychological or physical harm. They are not the same as “workplace stress” — a distinction that matters enormously for how organisations respond.
The concept traces back to the ILO/WHO Joint Committee’s 1984 definition, which identified interactions between work environment, job content, organisational conditions, and workers’ capacities as determinants of health outcomes. Since then, the terminology has evolved, but a persistent confusion remains in practice: the terms hazard, risk factor, and risk are used interchangeably when they mean different things.
Hazard, Risk Factor, and Risk — Why the Distinction Matters
Practitioners who conflate these terms end up writing risk assessments that describe feelings rather than identify controllable work conditions. The table below clarifies the relationship.
| Term | Definition | Workplace Example |
|---|---|---|
| Psychosocial hazard | A source or situation with potential to cause psychological or physical harm | Aggressive client-facing role |
| Psychosocial risk factor | The specific work characteristic contributing to the hazard | Lack of de-escalation training, no post-incident support, inadequate staffing |
| Psychosocial risk | The likelihood and severity that those risk factors will cause harm | High probability of anxiety, PTSD, or burnout without controls |
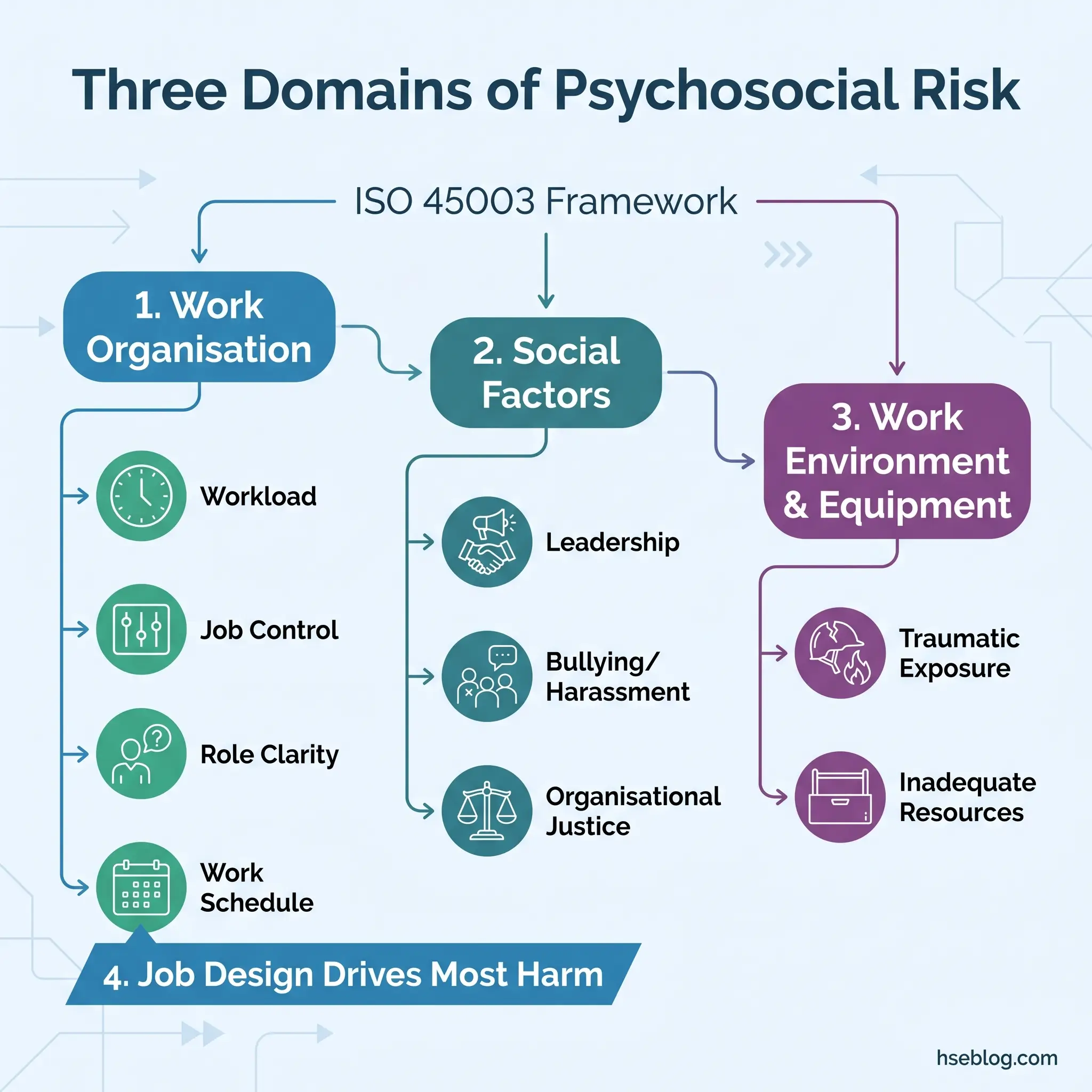
ISO 45003:2021 organises psychosocial hazards into three domains that provide the most practical assessment structure currently available:
- How work is organised — job demands, workload, pace, schedule, autonomy, role clarity, career development, remote work
- Social factors at work — leadership, relationships, organisational culture, bullying, harassment, recognition, support
- Work environment and equipment — physical conditions interacting with psychological strain, inadequate resources, traumatic exposure
The reason this three-domain structure matters is operational. Organisations that treat “psychosocial” as synonymous with “stress” — and therefore route it to a wellbeing programme — consistently underperform on identification and control. Psychosocial risk management is a hazard-management discipline governed by the same duty of care as noise, chemicals, or working at height. Framing it as a wellness initiative disconnects it from the risk-assessment process where it belongs.
A frequently overlooked dimension: psychosocial risk factors cause physical harm, not only psychological distress. Chronic occupational stress alters musculoskeletal tension patterns, changes work behaviours (skipping breaks, rushing tasks), and is linked to elevated cardiovascular risk. HSE UK explicitly recognises the psychosocial–musculoskeletal disorder pathway in its guidance — the two hazard categories interact, and assessing them separately misses the combined risk profile.
Common Psychosocial Risk Factors: A Categorised Overview
The most useful way to map psychosocial risk factors is through ISO 45003’s three-domain structure, with specific factors listed within each. Flat, unnumbered lists — common in competing guidance — obscure the critical insight that work-organisation factors statistically cause more harm than interpersonal factors, despite receiving less assessment attention.
Domain 1: How Work Is Organised
These are the factors most frequently overlooked in risk assessments because they implicate management decisions rather than individual behaviour.
- Job demands and workload — sustained excessive volume, cognitive complexity, or pace without adequate recovery. The risk is not temporary pressure; it is chronic demand exceeding resources.
- Work schedule and hours — extended shifts, unpredictable schedules, insufficient rest between shifts, and night work. Fatigue interacts with every other psychosocial factor.
- Job control and autonomy — workers with little decision-making authority over how or when they complete tasks face consistently higher stress. Karasek’s job demand-control model identifies low control under high demand as the highest-risk configuration.
- Role clarity and role conflict — ambiguous responsibilities, contradictory instructions from multiple supervisors, or scope creep without renegotiation.
- Career development and job insecurity — stagnation, unclear progression, restructuring threats, or precarious employment contracts.
- Remote and isolated work — geographical or social isolation, lone working without adequate check-in protocols, and the loss of informal peer support.
Domain 2: Social Factors at Work
- Leadership and management practices — inconsistent, absent, or punitive supervision. The quality of the immediate line-manager relationship is the single strongest social predictor of psychosocial harm.
- Interpersonal relationships — poor team dynamics, unresolved conflict, and exclusion.
- Organisational culture and justice — perceived unfairness in decisions, promotions, workload distribution, or disciplinary processes.
- Bullying, harassment, and violence — these receive the most assessment attention but represent only part of the social-factor landscape.
- Recognition and reward — effort–reward imbalance sustained over time.
- Support systems — inadequate peer support, inaccessible management, or absent occupational health resources.
Domain 3: Work Environment and Equipment
- Physical conditions with psychological impact — noise, heat, poor lighting, and cramped spaces generate psychological strain compounding physical risk.
- Inadequate tools or resources — being expected to meet standards without functioning equipment or sufficient staffing.
- Traumatic event exposure — direct exposure to death, serious injury, or threats. Relevant to emergency services, healthcare, and transport sectors.
- Vicarious and secondary trauma — indirect exposure through handling distressing content, debriefing affected colleagues, or reviewing incident materials.
Emerging and Post-Pandemic Psychosocial Risk Factors
Several risk factors have either intensified or appeared since 2020, yet most organisational risk registers have not been updated to reflect them.
Technostress and digital overload now function as standalone psychosocial hazards — constant connectivity, notification fatigue, and the cognitive load of managing multiple platforms create demand patterns that did not exist a decade ago. Algorithmic management — where task allocation, pace, performance monitoring, or scheduling is determined by software rather than human supervisors — generates a specific form of anxiety rooted in loss of control and perceived surveillance.
Hybrid work isolation interacts with existing risk factors in ways organisations rarely assess. A worker with moderate workload and adequate supervisor support in an office environment may experience the same workload as high-demand and the same supervisor as absent when working remotely three days a week. The risk profile changes without the hazard register changing.
Perhaps most critically, many organisations embedded crisis-era workloads as permanent norms after the pandemic without reassessing psychosocial risk. What was an emergency arrangement — higher caseloads, reduced staffing, compressed timelines — became an unexamined baseline. The risk factors were never temporary, but the assumption that they would revert was.
How to Identify Psychosocial Risk Factors in the Workplace
Identification is where most psychosocial risk management programmes either succeed or collapse. The process requires multiple data sources because no single method captures the full picture — and every major jurisdiction mandates worker consultation as a non-optional element.
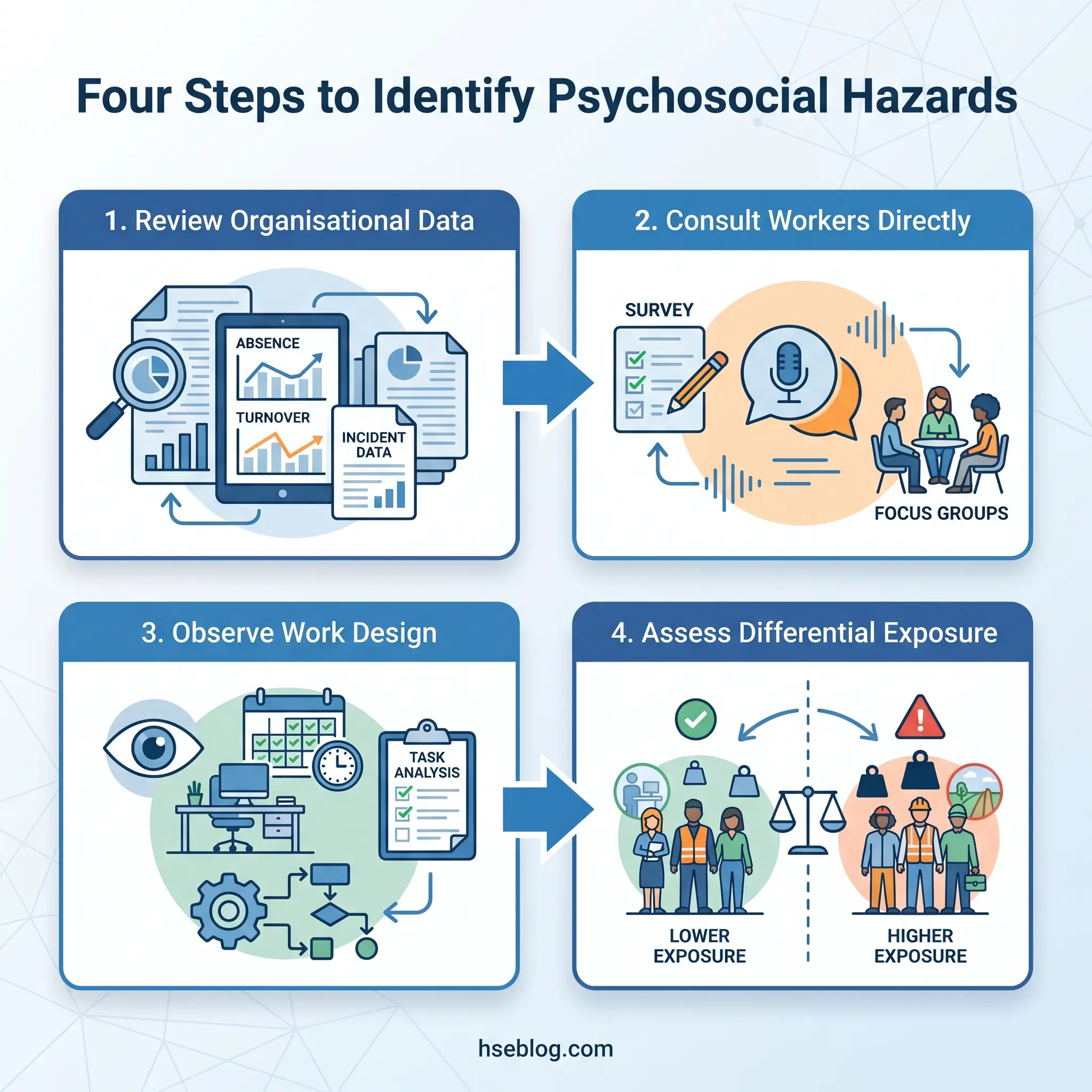
Step 1: Review Organisational Data
Before launching any survey, mine the data already available. Patterns in existing records often signal psychosocial risk factors that workers have not yet articulated.
- Absence and sick-leave trends — rising short-term absences, Monday/Friday clustering, and long-term stress-related leave.
- Turnover and exit interview themes — departure reasons citing workload, management, or “culture” are psychosocial signals.
- Incident and near-miss reports — reports mentioning fatigue, distraction, rushing, or communication failure point to underlying psychosocial conditions.
- Grievance and complaint records — volume and type, particularly interpersonal conflict and management conduct.
- Workers’ compensation claims — claims for psychological injury or stress-related conditions.
Step 2: Consult Workers Directly
Surveys provide breadth; focus groups provide depth. The most common failure in psychosocial risk identification is relying on anonymous surveys alone — they tell you what workers report experiencing but not why. Without the “why,” control measures become generic.
- Anonymous surveys — validated tools (see below) administered to all workers. Anonymity is critical for honest reporting.
- Focus groups — small-group discussions facilitated by someone independent of line management, exploring the themes surveys surface.
- One-to-one conversations — particularly for workers who may not engage with group settings or surveys.
- Safety committee input — health and safety representatives often hold intelligence that formal channels miss.
Step 3: Observe and Analyse Work Design
Direct observation fills gaps that self-report cannot cover. Workers may normalise conditions that an external assessment would flag.
Walk the work environment with psychosocial factors in mind. Map workload distribution across shifts. Review roster patterns for fatigue risk. Examine how tasks are assigned, supervised, and reviewed.
Step 4: Account for Differential Exposure
Not all workers experience the same psychosocial risk profile in the same workplace. Gender, age, disability, cultural background, and employment type (casual, contract, gig) all influence exposure. Young and precarious workers are disproportionately exposed to job insecurity and low control. Workers in client-facing roles carry higher interpersonal-conflict risk. Night-shift workers face compounded fatigue and social isolation.
Identification that treats the workforce as homogeneous will miss the groups carrying the highest burden.
Validated Assessment Tools and Frameworks
Selecting the right survey tool matters. Organisations sometimes adopt a tool without checking whether it covers the risk factors most relevant to their sector — a healthcare setting and a logistics operation share some psychosocial risks but diverge sharply on others.
| Tool | Origin / Jurisdiction | Dimensions Covered | Cost | Best Suited For |
|---|---|---|---|---|
| HSE Indicator Tool | UK | Six Management Standards areas: demands, control, support, relationships, role, change | Free | UK employers benchmarking against HSE standards |
| COPSOQ III | International (Danish origin) | Broad range: demands, influence, social support, meaning, predictability, rewards, and more | Open-source | Multi-jurisdictional or research-grade assessments |
| People at Work | Australia | Aligned with Australian WHS Regulations; covers 14 psychosocial hazard groups | Free | Australian PCBUs meeting WHS obligations |
| ISO 45003 Annex A | International | Framework reference listing psychosocial hazard examples across three domains | Standard purchase | Organisations structuring assessments against ISO 45003 |
All survey tools share a critical limitation: they measure perception, not objective hazard presence. A team may report high satisfaction despite objectively excessive workload if normalisation has set in. Surveys must always be triangulated with organisational data and observational methods.
Assessing and Prioritising Psychosocial Risks
Once risk factors are identified, the assessment challenge is determining which combinations create the highest probability and severity of harm. The standard likelihood × consequence matrix applies, but psychosocial risks require adaptation.
Three dimensions govern the assessment, as specified in Safe Work Australia’s Model Code of Practice for managing psychosocial hazards:
- Duration — how long is the worker exposed? A single difficult interaction differs fundamentally from months of sustained role ambiguity.
- Frequency — how often does exposure occur? Daily aggressive client contact versus occasional project-deadline pressure.
- Severity — how intense is the exposure? Mild time pressure versus exposure to traumatic events.
The number of workers affected and whether effective controls already exist also factor into prioritisation.
The Interaction Effect — What Most Assessments Miss
The biggest assessment pitfall is treating each psychosocial risk factor in isolation. Published evidence consistently shows that psychosocial risks operate cumulatively and interactively. A moderate workload combined with low job control and poor supervisor support produces a risk profile far greater than any single factor would predict alone.
The job demand-control model demonstrates this interaction directly: high demands paired with high control produce active, engaged work; the same high demands paired with low control produce the highest-strain configuration. Assessment that scores each factor on its own scale and averages them will systematically underestimate combined risk.
Practical recommendation: when completing the risk register, assess the cluster of risk factors present in a work group or role, not each factor independently. Document interaction effects explicitly — “high workload + low autonomy + limited supervisor access” as a combined risk profile, not three separate line items.
What Controls Reduce Psychosocial Risk? The Hierarchy of Controls Applied
The hierarchy of controls applies to psychosocial hazards in exactly the same way it applies to physical hazards — a principle now explicitly codified in Australia’s WHS Regulations and reinforced in ISO 45003. The overwhelmingly common failure pattern is that organisations default to the bottom of the hierarchy, offering EAPs and resilience training while leaving the job demands, shift patterns, and management practices that generate the risk entirely untouched.
This inverts the hierarchy and shifts the burden of coping onto individual workers.
Elimination
Remove the hazard source entirely. This is rarely discussed for psychosocial risks, but it is possible.
- Removing exposure to aggressive clients by changing the service-delivery model (e.g., moving from face-to-face to mediated communication for high-risk interactions).
- Eliminating unnecessary overtime by redesigning rosters or redistributing workload to match actual capacity.
- Removing a role that combines inherently conflicting responsibilities and splitting it into coherent positions.
Substitution
Replace a high-risk work arrangement with a lower-risk alternative.
- Replacing isolated lone work with paired arrangements or buddy systems.
- Substituting rotating shifts with fixed shifts where worker preference allows — reducing circadian disruption and social-life conflict.
- Replacing manual grievance processes with accessible, confidential reporting systems that reduce fear of retaliation.
Engineering and Design Controls
These are the “job redesign” interventions — structural changes to how work is designed.
- Workload redistribution based on actual task-time analysis rather than assumed capacity.
- Scheduling redesign — maximum shift lengths, minimum rest periods, predictable rosters published in advance.
- Physical environment improvements — quiet spaces for focused work, adequate break areas, separation of high-noise areas from cognitive-task areas.
Administrative Controls
Policies, procedures, training, and supervision standards that reduce risk without changing the underlying work design.
- Clear role descriptions reviewed when responsibilities change.
- Management training in psychosocial risk awareness, early-warning recognition, and supportive supervision.
- Incident-reporting systems that capture psychosocial near-misses — not only physical.
- Return-to-work programmes for workers recovering from psychological injury.
Individual-Level Measures (The PPE Equivalent)
EAPs, resilience training, stress-management workshops, and mindfulness programmes sit here. They address individual coping capacity rather than the organisational conditions generating harm.
Research evidence shows individual-level interventions alone produce limited and short-lived effects. They are useful as supplementary measures within a comprehensive programme but must never substitute for organisational-level controls higher in the hierarchy.
The judgment call for practitioners: when leadership proposes an EAP as the psychosocial risk response, the question to ask is — “What organisational change does this sit alongside?” If the answer is none, the hierarchy has been inverted.

Sector-Specific Control Examples
Generic control lists fail because psychosocial risk profiles differ sharply across industries. Below are targeted examples for sectors where psychosocial harm is most prevalent.
- Healthcare — Fatigue-management rostering using evidence-based shift limits; structured critical-incident debriefing protocols; patient-aggression prevention through environmental design (escape routes, panic alarms, separated waiting areas).
- Construction — Addressing cultural barriers to reporting psychological distress through peer-support champion networks; fatigue-management policies tied to travel time and early starts; normalising mental-health conversations through toolbox-talk integration.
- Education — Workload protocols capping preparation-to-contact-hour ratios; student-behaviour management systems that reduce individual teacher burden; structured supervision for early-career staff.
- Office/knowledge work — Digital-disconnection policies with enforced out-of-hours email restrictions; meeting-load management (maximum meeting hours per day); psychosocial risk assessment specific to hybrid-work arrangements, covering isolation, work–life boundary erosion, and manager accessibility.
The Regulatory Landscape: Legal Duties Across Jurisdictions
No single international treaty mandates psychosocial risk management uniformly. Instead, a patchwork of national legislation, voluntary standards, and enforceable codes of practice governs the duty — and the trend line is toward greater enforceability everywhere.
The table below maps the current state across major jurisdictions.
| Jurisdiction | Primary Framework | Key Duty | Enforcement Status | Hierarchy of Controls Mandated? | Recent Development |
|---|---|---|---|---|---|
| International | ISO 45003:2021 | Guidelines for managing psychosocial risks within ISO 45001 systems | Voluntary, non-certifiable | Recommended | Increasingly referenced by regulators |
| UK | HSE Management Standards + HSWA 1974 s.2 | Ensure health of employees, including mental health | Enforceable under HSWA 1974 | Implied through general duty | HSE signalling enforcement shift toward organisational mental-health failures (2025) |
| EU | Framework Directive 89/391/EEC + Social Partner Agreements (2004, 2007) | Assess and manage all workplace risks including psychosocial | Enforceable via member-state transposition | Implied through general principles of prevention | EU-OSHA Healthy Workplaces Campaign 2026–2028 focused on mental health at work |
| Australia | Safe Work Australia Model Code of Practice (2022) + WHS Regulations | Identify psychosocial hazards, assess risk, apply hierarchy of controls | Mandatory and enforceable | Explicitly mandated | WHS Regulation amendments effective April 2023 (Commonwealth) |
| Canada | CSA Z1003-13 (R2022) | Systematic approach to psychological health and safety; identifies 13 factors | Voluntary national standard (free access) | Recommended | Reaffirmed 2022; referenced increasingly in provincial OHS guidance |
| US | OSHA General Duty Clause (Section 5(a)(1)) | No specific psychosocial standard; General Duty Clause applied to workplace violence, severe harassment | Limited, case-by-case enforcement | Not specified | No dedicated standard in development |
The Convergence Trend
The direction is unmistakable. Australia moved from voluntary guidance to enforceable regulation in 2022–2023. The UK’s HSE is actively investigating suspected organisational failures in managing mental health risks — signalling a shift from guidance to enforcement (HSE UK, 2025). The EU-OSHA’s Healthy Workplaces Campaign 2026–2028, titled “Together for mental health at work,” is the organisation’s most direct focus on psychosocial risk prevention to date, supported by ESENER 2024 data showing that only 39% of EU workplaces have a formal stress-prevention action plan (EU-OSHA, 2024).
Organisations operating across jurisdictions often benchmark against the least demanding standard. The practitioner recommendation is the reverse: benchmark against ISO 45003 as the global best-practice floor, then layer jurisdiction-specific obligations on top. This approach absorbs future regulatory tightening rather than requiring reactive catch-up.
The WHO Guidelines on Mental Health at Work (2022) and the ILO/WHO Joint Policy Brief reinforce the direction, recommending organisational interventions targeting psychosocial risk factors integrated into OHS systems — not standalone wellbeing programmes.
How Do You Conduct a Psychosocial Risk Assessment?
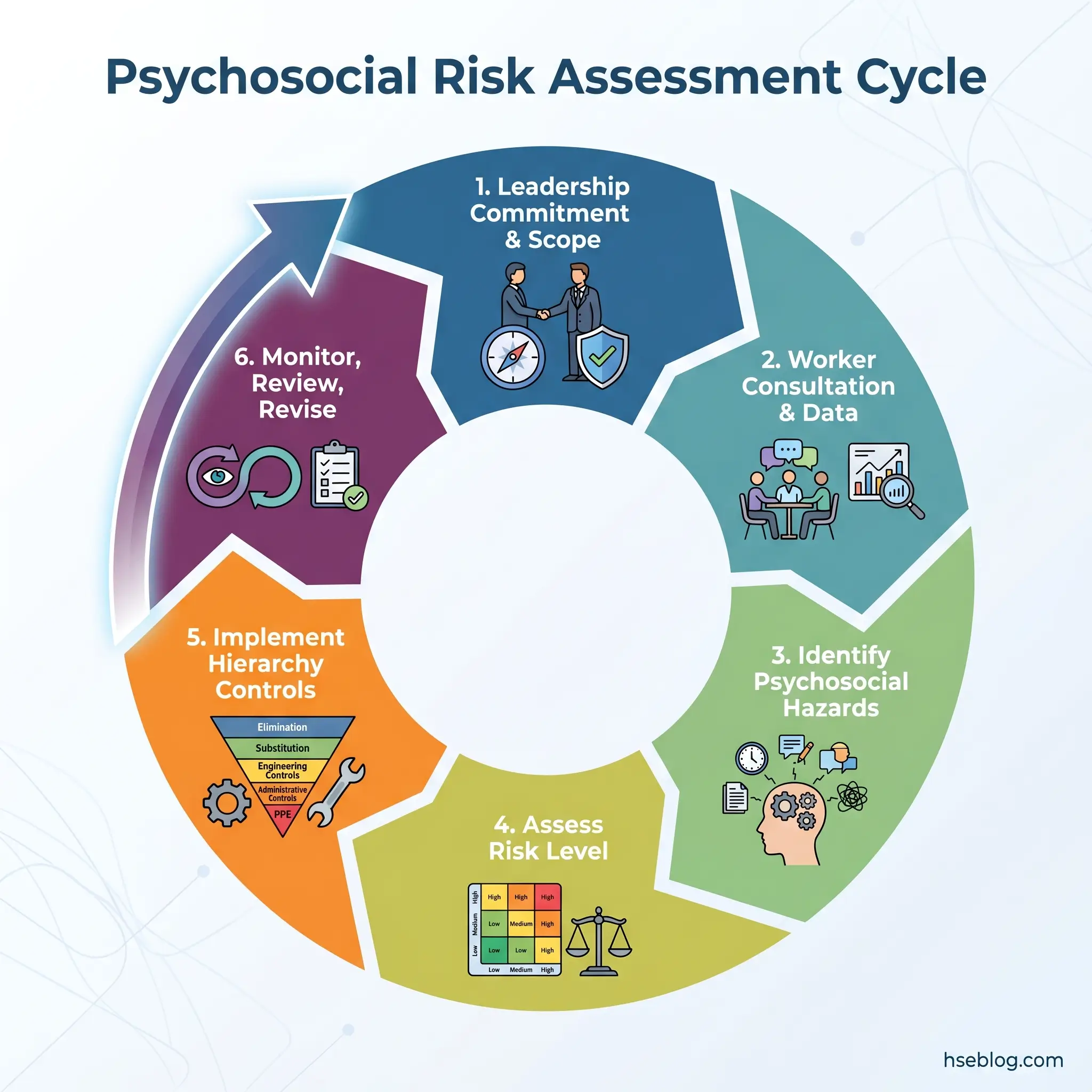
A psychosocial risk assessment follows six steps — the same systematic cycle used for any workplace hazard, adapted for factors that are organisational rather than physical.
- Secure leadership commitment and define scope. Without visible senior-management sponsorship, the assessment lacks authority to drive change. Define which work groups, roles, or locations the assessment will cover.
- Consult workers and gather data. Deploy validated survey tools, conduct focus groups, and review organisational records. Worker consultation is a legal requirement in every jurisdiction with enforceable psychosocial-risk duties.
- Identify the psychosocial hazards present. Map findings against the three ISO 45003 domains. Name the specific risk factors — “excessive workload due to staffing shortfall in Team X,” not “stress.”
- Assess the risk level. Evaluate duration, frequency, and severity of exposure. Consider the number of workers affected. Critically, assess interaction effects between co-occurring risk factors.
- Implement controls using the hierarchy. Prioritise elimination and design-level interventions. Document the rationale for control selection, including why higher-order controls were or were not feasible.
- Monitor, review, and revise. Psychosocial risk assessment is not a one-off compliance exercise. Review triggers include organisational change, critical incidents, monitoring data showing adverse trends, and regular scheduled periods (annually at minimum).
The legal requirement in Australia, the UK, and the EU is to document the process and its outcomes. The practical requirement everywhere is to close the loop — feed results into the management system, track corrective actions, and verify that controls are effective.
Building a Sustainable Psychosocial Risk Management Programme
The transition from “we did a risk assessment” to “we manage psychosocial risk” is where most organisations stall. The assessment becomes a filed report rather than a living management tool — and the risk factors it identified continue unchanged.
A sustainable programme requires four elements operating continuously.
Governance and Accountability
Ownership must be explicit. Psychosocial risk management typically falls between OHS and HR — and in that gap, nobody acts. Assign clear accountability at senior-management level, establish a cross-functional team (OHS, HR, operations, worker representatives), and include psychosocial risk as a standing agenda item in safety committee meetings and board-level OHS reporting.
Worker representation is not optional. The most effective programmes involve health and safety representatives and, where applicable, union delegates in every stage — from assessment design through control selection to review.
Competency
Not every OHS professional is competent to assess psychosocial risks. The skill set differs from physical-hazard assessment. Competency requirements include understanding of psychosocial hazard mechanisms, proficiency with validated assessment tools, facilitation skills for focus groups, and the ability to interpret interaction effects between risk factors.
Recognised training pathways include NEBOSH and IOSH qualifications with psychosocial-risk modules, Safe Work Australia’s guidance materials, and the WHO’s training resources. Organisations should identify competency gaps and address them before launching assessment programmes.
Integration With the OHS Management System
Psychosocial risks belong in the same risk register as physical risks — not in a separate HR document. They belong in toolbox talks, incident-investigation protocols, and corrective-action tracking systems. ISO 45003 is designed as a companion to ISO 45001, and the integration point is straightforward: psychosocial hazards are hazards, managed through the same plan-do-check-act cycle.
Monitoring Indicators
Effective programmes track both leading and lagging indicators.
- Leading indicators — survey participation rates, number of psychosocial hazards identified, control-implementation completion rates, worker feedback-loop activity, training completion.
- Lagging indicators — absence rates (particularly stress-related), workers’ compensation claims for psychological injury, turnover rates, grievance volumes, and trends in exit-interview themes.
Success requires tying psychosocial risk data to the same governance cadence as physical-risk data — the same reporting cycles, the same corrective-action deadlines, the same close-out verification.
Frequently Asked Questions

Conclusion
The pattern across organisations that fail at psychosocial risk management is remarkably consistent: they treat psychosocial factors as a wellbeing concern rather than an occupational hazard, default to individual-level interventions at the bottom of the hierarchy, conduct a single risk assessment that gets filed and forgotten, and assess each risk factor in isolation rather than as an interacting cluster. Every one of these failures is a structural choice, not a resource constraint.
The single highest-impact change most organisations can make is to stop separating psychosocial risks from their existing OHS management system. When psychosocial hazards sit in the same risk register, follow the same corrective-action process, and report through the same governance structures as chemical exposures or working at height, they stop being treated as discretionary. They become what they are — workplace hazards with a legal, moral, and operational obligation to control.
With 29% of EU workers reporting stress, depression, or anxiety (EU-OSHA, 2025), and the UK recording its highest-ever figure for work-related psychological ill health, the gap between published guidance and workplace practice remains wide. Closing it does not require new science or novel frameworks. It requires applying the risk-management discipline this profession already knows — identification, assessment, hierarchy-based control, and continuous review — to the hazards that now cause the majority of occupational harm.