

TL;DR
- Urine testing dominates — it remains the only specimen type approved for federally mandated testing under SAMHSA and DOT, used by the vast majority of employers
- Fentanyl joins the federal panel — effective July 7, 2025, SAMHSA added fentanyl and norfentanyl to the authorized testing panel for both urine and oral fluid (Federal Register, 90 FR 3850)
- Oral fluid testing is gaining ground — DOT authorized oral fluid as an alternative to urine in 2023, but implementation awaits HHS laboratory certification
- Cannabis is the hardest policy call — over 40 US states have legalized medical cannabis, and a growing number restrict employer action on positive THC results, while DOT testing requirements remain unchanged
- Method selection should match risk — the strongest programs layer methods strategically rather than relying on a single specimen type
The most common types of drug tests used in the workplace analyze urine, hair, oral fluid, blood, or breath to detect controlled substances or their metabolites. Urine remains the most widely used method and the only specimen currently approved for US federally mandated testing. The standard 5-panel test screens for amphetamines, cocaine, marijuana (THC), opiates/opioids, and PCP, while expanded panels add substances such as benzodiazepines, barbiturates, and fentanyl — which joins the federal authorized panel effective July 7, 2025.
The combined US workforce urine drug test positivity rate held at 4.4% in 2024 (Quest Diagnostics, 2025) — a figure that has remained above 4% for a decade. Behind that number sits a more troubling pattern: fentanyl positivity in random workplace tests ran 707% higher than in pre-employment screening (Quest Diagnostics, 2025), meaning workers are passing their initial test and using fentanyl afterward. The data reveals something that a pre-employment-only testing strategy will never catch.
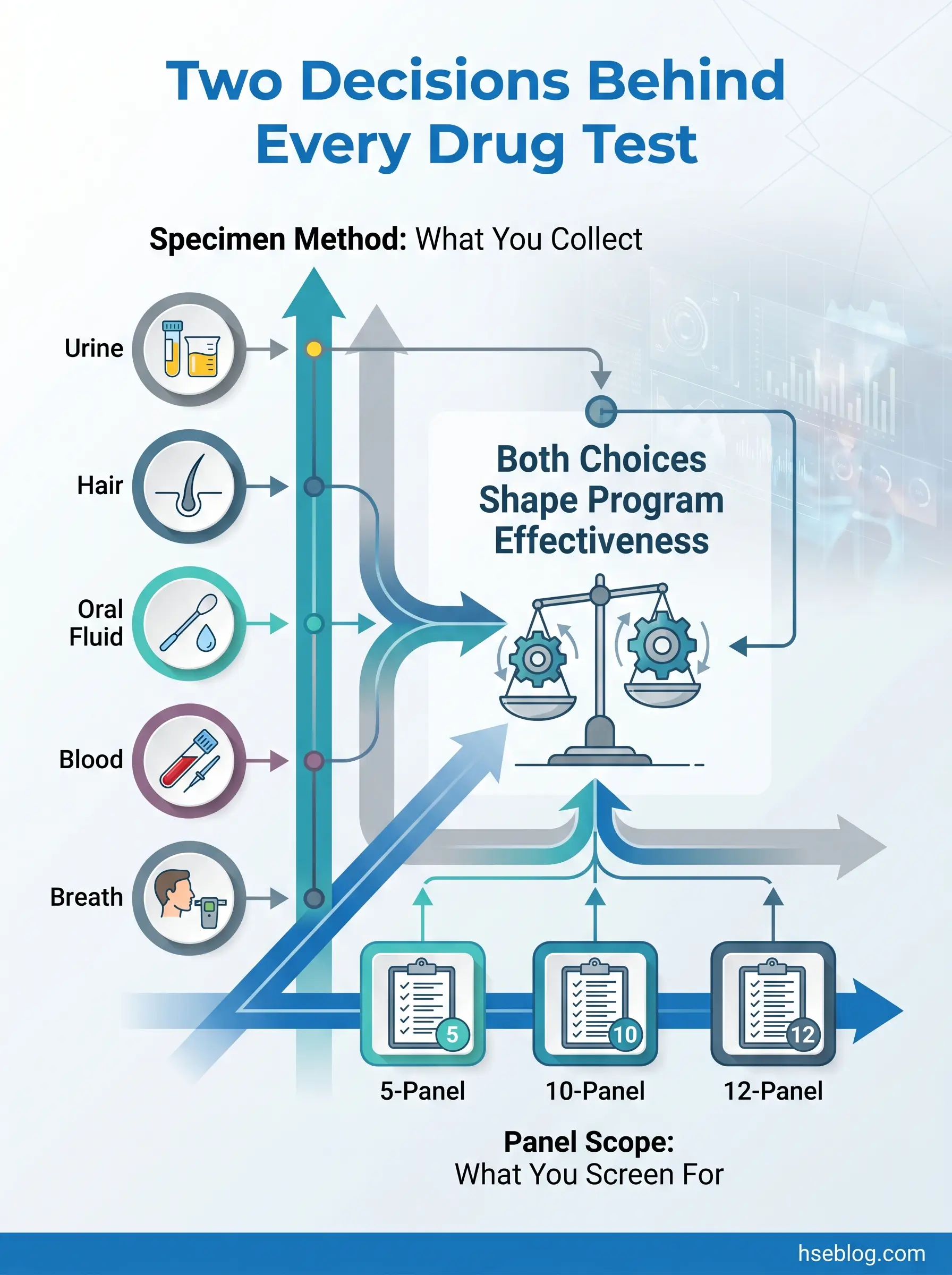
That gap between what employers think their drug testing program detects and what it actually misses is the central problem this article addresses. The confusion starts with terminology — when someone asks about the “type” of drug test, they could mean the specimen collected (urine, hair, saliva, blood, breath) or the substances screened (5-panel, 10-panel, 12-panel). These are two separate axes, and conflating them leads to programs that screen for the wrong things using the wrong method at the wrong time. What follows is a structured breakdown of both dimensions, grounded in the current regulatory landscape — including the two most consequential developments of 2025: the addition of fentanyl to the federal testing panel and the ongoing impact of state cannabis employment-protection laws on panel selection.
What Is Workplace Drug Testing and Why Do Employers Use It?
Workplace drug testing is the laboratory analysis of biological specimens — urine, hair, oral fluid, blood, breath, or sweat — to detect the presence of controlled substances or their metabolites in an employee’s body. The practice serves three distinct employer objectives that often overlap but should not be confused: safety (preventing impairment-related incidents in safety-sensitive roles), compliance (meeting federal and state mandates such as DOT 49 CFR Part 40 and the Drug-Free Workplace Act of 1988), and liability management (reducing insurance costs, workers’ compensation claims, and negligent-hiring exposure).
The most consistent source of confusion among HR professionals setting up or evaluating testing programs is the failure to distinguish between these two axes. “What type of drug test should we use?” is actually two questions: what specimen do we collect, and what substances do we screen for? The specimen method determines the detection window, collection logistics, adulteration risk, and cost. The panel configuration determines which drug classes appear in the results. A program that selects the right method but the wrong panel — or vice versa — creates a false sense of security. The sections below address each axis separately before bringing them together in a decision framework.
Urine Drug Testing (Urinalysis)
Urine remains the default specimen in workplace drug testing for a straightforward reason: it is the only specimen type currently approved for federally mandated testing under both SAMHSA’s Mandatory Guidelines (88 FR 70768, US federal) and DOT 49 CFR Part 40 (US federal). For any employer operating under federal mandates, urine is not a choice — it is a requirement.
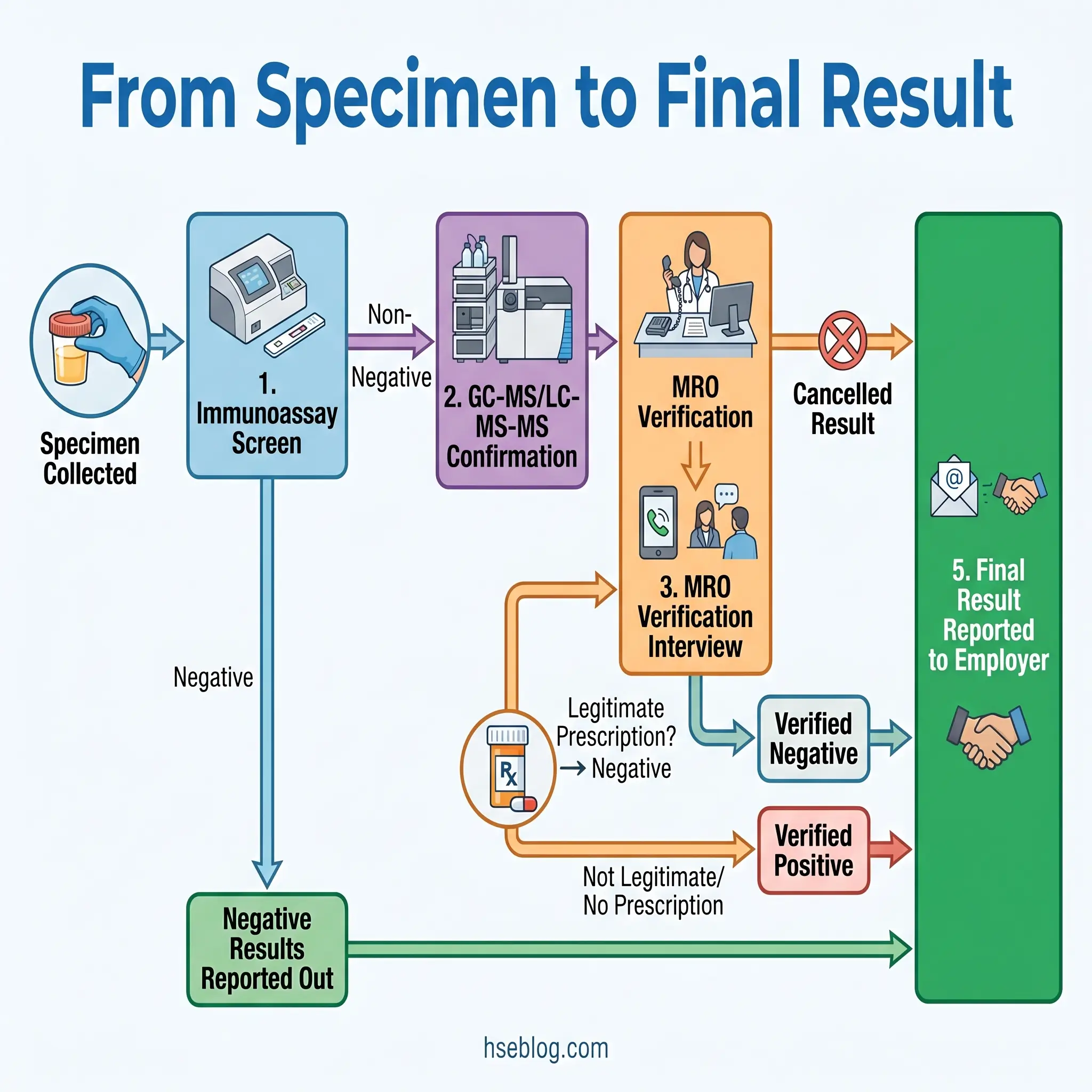
The analytical process follows a two-step protocol. An initial immunoassay screen rapidly identifies specimens that are presumptively positive for target drug classes. Any specimen that screens non-negative then undergoes confirmatory testing using gas chromatography-mass spectrometry (GC-MS) or liquid chromatography-tandem mass spectrometry (LC-MS-MS), which eliminates false positives and identifies the specific substance. This screening-then-confirmation architecture is critical to understand because the initial immunoassay alone is not definitive — it is a sorting mechanism.
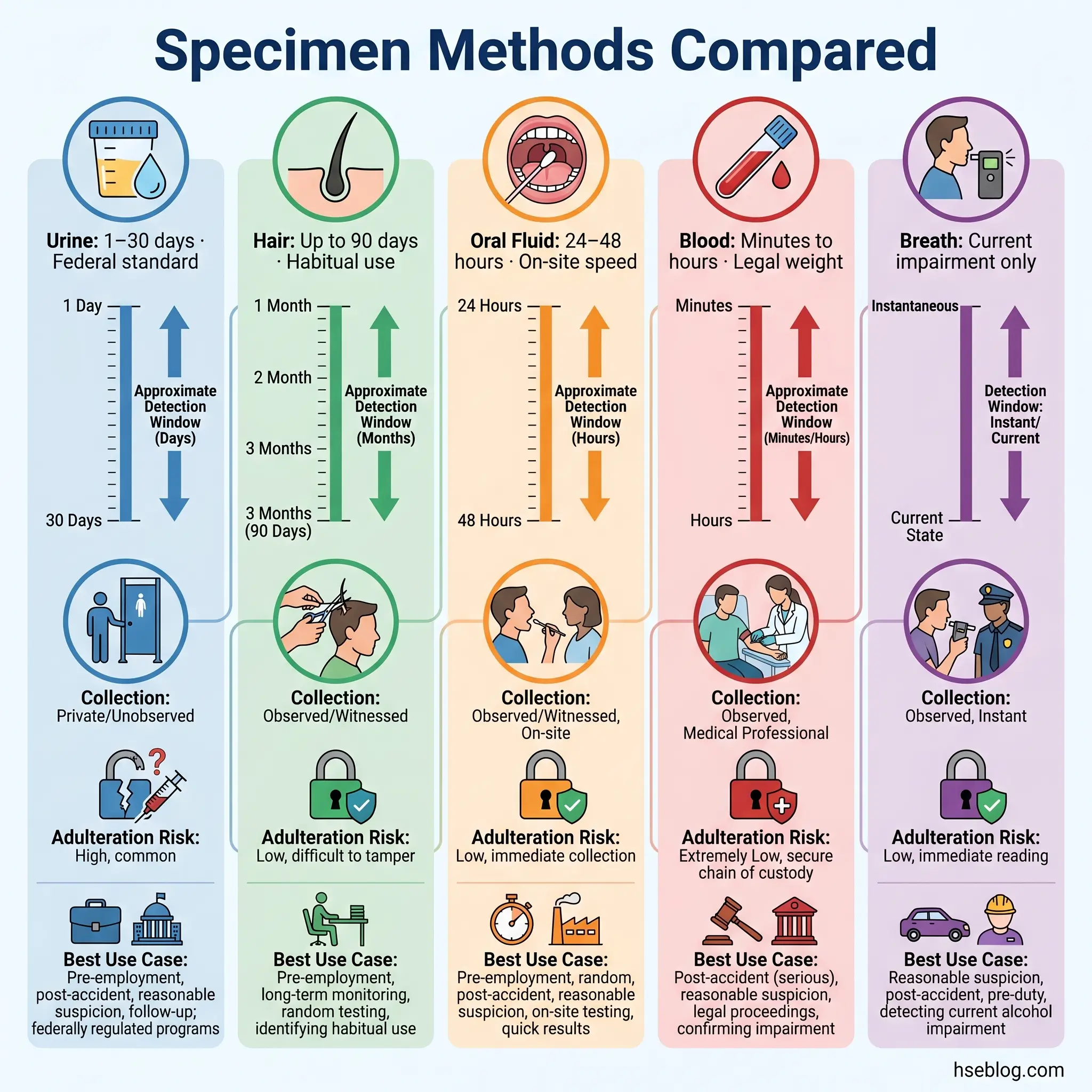
Detection windows for urine testing vary significantly by substance and usage pattern. Most substances — cocaine, amphetamines, opiates — are detectable for roughly 1–7 days after use. Chronic cannabis users present the widest variation: occasional users may clear within a few days, while heavy daily users can test positive for 30 days or longer. Specimen validity testing (SVT) detects attempts to defeat the test through dilution, substitution, or chemical adulteration — a countermeasure that has become standard in regulated programs.
Watch For: Organizations that rely exclusively on pre-employment urine testing create a significant blind spot. Quest Diagnostics data consistently shows dramatically different positivity rates between pre-employment and random testing — the 2025 Drug Testing Index reported for-cause testing positivity at 33.1% (Quest Diagnostics, 2025), compared to far lower rates at pre-employment. A single-occasion testing strategy catches the careless applicant; it misses the experienced user who abstains long enough to pass the gate.
Hair Follicle Drug Testing
Hair testing operates on a fundamentally different biological mechanism than urine. As blood circulates through the hair follicle during growth, drugs and their metabolites become permanently embedded in the hair shaft. A standard hair analysis uses 1.5 inches of head hair, representing approximately 90 days of growth — giving hair testing the longest detection window of any routine workplace method.
This extended window makes hair testing particularly effective at identifying patterns of habitual use rather than single instances of exposure. It detects cocaine, amphetamines, opioids, PCP, and cannabis metabolites reliably across the 90-day window. Body hair can be used when head hair is unavailable, though it reflects a longer but less precisely defined detection period due to variable growth cycles.
Hair testing carries two important limitations that practitioners must weigh. First, there is an approximate 7–10 day delay between substance use and detectability — drugs must be incorporated into the hair shaft as it grows past the scalp. Second, peer-reviewed research has raised concerns about potential racial bias in hair testing, particularly regarding melanin binding of certain drug metabolites. These concerns have contributed to hair testing not being approved for federally mandated testing under SAMHSA or DOT. SAMHSA proposed hair testing guidelines in 2020 but has not finalized them.
A consistent practitioner observation: employers who switch to hair testing for pre-employment screening often see a notable shift in what they detect. Cannabis detection may decrease (due to the delay before detectability), while stimulant-use patterns that urine missed — because of cocaine’s short urine detection window — become visible. The method does not simply look further back; it changes the substances you are most likely to find.
Oral Fluid (Saliva) Drug Testing
Oral fluid testing has more regulatory momentum behind it right now than any other specimen type. DOT authorized oral fluid as an alternative to urine for safety-sensitive transportation employees effective June 1, 2023, under 49 CFR Part 40. A November 2024 final rule (89 FR 87792, effective December 5, 2024, US federal) further clarified collector qualification requirements. However, implementation remains in a holding pattern: the US Department of Health and Human Services has not yet certified any laboratories for DOT oral fluid testing. Until that certification occurs, DOT-regulated employers cannot actually switch to oral fluid.
The operational advantages of oral fluid testing are substantial. Collection is directly observed — the collector watches the donor place the swab in their mouth — which virtually eliminates substitution and adulteration, the two most persistent vulnerabilities in urine collection. Oral fluid detects parent compounds rather than metabolites, making it a closer proxy for recent use and potential impairment compared to urine’s metabolite-based detection. And collection can happen on-site, immediately, without sending the worker to an off-site collection facility.
The detection window is shorter — typically 24–48 hours for most substances — which is simultaneously the method’s limitation and its strength. For pre-employment screening or habitual-use detection, a 48-hour window is insufficient. For post-accident or reasonable-suspicion testing, however, that window aligns precisely with the question being asked: was this person using substances in the period leading up to this event? The ability to collect a specimen on-site, immediately after an incident, without the delays inherent in urine collection logistics, makes oral fluid operationally transformative for time-critical safety situations.
Blood Drug Testing
Blood testing provides the most accurate snapshot of what is actively circulating in a person’s body at the moment of collection. It measures parent drug concentrations directly and correlates most closely with current impairment — which is precisely why it carries significant weight in legal proceedings and post-incident forensic analysis.
The practical constraints are equally clear. The detection window is measured in hours, not days. Collection requires a trained phlebotomist, is invasive, and costs considerably more than urine or oral fluid. For routine workplace screening, blood testing is neither practical nor cost-effective.
Where blood testing matters in workplace contexts is in serious incident investigations. After a fatality or major accident, employers or investigators sometimes request blood analysis for its legal defensibility and precision. The critical variable practitioners must account for is time-to-collection — every hour of delay between the incident and the blood draw degrades the evidentiary value. If a worker is transported to a hospital, treated, and then tested hours later, the results may no longer reflect the substance levels present at the time of the incident. That delay must be documented meticulously.
Breath Alcohol Testing
Breath alcohol testing occupies a unique position because it directly measures current impairment rather than past exposure. An Evidential Breath Testing (EBT) device analyzes blood alcohol concentration through breath, delivering immediate results that indicate the subject’s intoxication level at the moment of testing.
Under DOT 49 CFR Part 40 (US federal), breath alcohol testing is mandatory for safety-sensitive transportation workers. The protocol is straightforward: a screening test result of 0.02 BAC or higher triggers a confirmation test on a certified EBT device. A confirmed result of 0.04 or higher constitutes a DOT violation. The binary clarity of breath alcohol — either a worker is above the threshold now or they are not — is precisely what makes it operationally simpler to interpret than drug testing, which detects metabolites from past use without directly measuring current impairment.
Less Common Testing Methods: Sweat Patches and Fingerprint Testing
Two additional methods appear in specific operational niches. Sweat patches are adhesive patches worn on the skin for days to weeks, collecting perspiration that contains drug metabolites over the wear period. This provides cumulative exposure data and is primarily used in criminal justice supervision and rehabilitation monitoring — not routine workplace screening.
Fingerprint drug screening is an emerging technology with growing adoption in UK workplaces. It analyzes trace drug metabolites secreted in sweat from the fingertips, offering rapid, non-invasive screening with a narrower detection window of approximately 16 hours. Neither method is SAMHSA-approved or DOT-authorized. They fill monitoring niches — continuous supervision, rapid fitness-for-duty spot checks — but are not yet viable as primary screening tools for most employers.
What Do Workplace Drug Tests Screen For? Understanding Drug Panels
The second axis of workplace drug testing — and the one that drives the most consequential policy decisions in 2025 — is the panel configuration. Each panel number represents the count of drug classes screened, and the differences between them are not trivial.
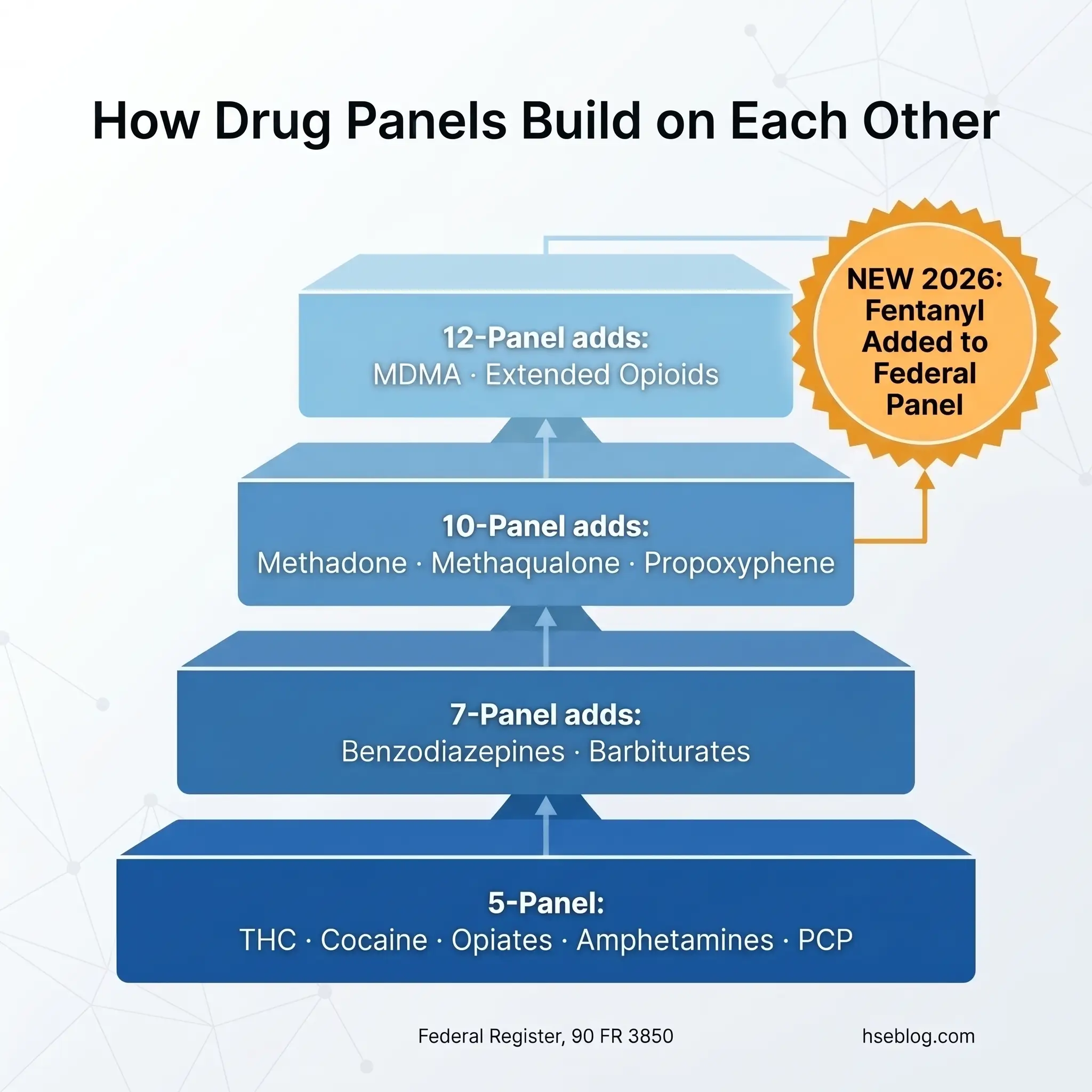
The standard 5-panel test, mandated by SAMHSA and DOT for federal and safety-sensitive transportation workers, screens for five drug classes: amphetamines, cocaine, marijuana metabolites (THC), opiates/opioids, and phencyclidine (PCP). The DOT expanded opioid panel now includes four semi-synthetic opioids — hydrocodone, oxycodone, hydromorphone, and oxymorphone — in addition to codeine and morphine.
Expanded panels add drug classes beyond the federal baseline. A 10-panel test typically adds benzodiazepines, barbiturates, methadone, methaqualone, and propoxyphene. A 12-panel configuration commonly adds MDMA (ecstasy) and extended opioid variants. Private employers not subject to federal mandates have broad latitude to customize their panels based on industry risk profile, state law, and regional substance-use patterns.
The most significant panel development in years takes effect on July 7, 2025: SAMHSA’s addition of fentanyl and norfentanyl to the federal authorized testing panel for both urine and oral fluid (Federal Register, 90 FR 3850, US federal). This matters because fentanyl is a synthetic opioid that does not cross-react with the standard opiate immunoassay — meaning standard 5-panel tests have been unable to detect it. Quest Diagnostics reported fentanyl positivity in random workplace tests was over seven times higher than in pre-employment screening in 2024 (Quest Diagnostics, 2025), and 60% of fentanyl-positive specimens also tested positive for other substances. The fentanyl blind spot is closing, but private employers must affirmatively add fentanyl-specific testing to their panels — it does not happen automatically.
The other panel decision generating the most policy revision work is whether to retain or remove THC. A growing number of states restrict employer actions based on positive cannabis results. “No-THC” panel options are increasingly available for employers in those jurisdictions. The fentanyl and THC decisions together are driving more panel configuration changes than any other factor in the current landscape.
Drug Panel Configurations: Comparison
| Panel | Drug Classes Screened | Typical Use |
|---|---|---|
| 5-Panel | Amphetamines, Cocaine, THC, Opiates, PCP | Federal/DOT mandate; most common baseline |
| 7-Panel | 5-panel + Benzodiazepines, Barbiturates | Healthcare, extended risk profiles |
| 10-Panel | 7-panel + Methadone, Methaqualone, Propoxyphene | Law enforcement, government, high-security |
| 12-Panel | 10-panel + MDMA, Extended Opioids | Comprehensive private-sector programs |
| Fentanyl Add-On | Fentanyl, Norfentanyl (separate immunoassay) | Federal panel effective July 7, 2025; private employers by election |
When Do Employers Conduct Drug Tests? Testing Occasions Explained
When an employer tests matters as much as how they test. Six standard testing occasions form the backbone of workplace drug testing programs, each with distinct regulatory bases and operational triggers.
Pre-employment testing is the most common occasion. A conditional job offer is extended, contingent on the applicant passing a drug test. While widespread, pre-employment testing alone creates the blind spot described earlier — it captures only the moment of hiring.
Random testing is unannounced and targets employees selected through a statistically valid random-selection process. DOT mandates minimum annual random testing rates — 50% of the covered workforce for drugs and 10% for alcohol in most transportation modes (49 CFR Part 40, US federal). Random testing is the most effective deterrent against ongoing use because employees cannot predict when they will be selected.
Post-accident testing is triggered by specific incident criteria. This is where programs most frequently break down in practice. Employers either test too broadly — every minor first-aid incident — or too narrowly, testing only after fatalities. Poorly defined triggering criteria create legal exposure and union grievance vulnerability. The testing policy must specify objective, measurable triggers: injury requiring off-site medical treatment, fatality, significant property damage, or receipt of a moving violation related to the incident.
Reasonable suspicion testing requires trained supervisors to document specific, contemporaneous behavioral observations — slurred speech, impaired coordination, unusual behavior, the odor of alcohol. The documentation requirement is critical; a hunch is not reasonable suspicion. DOT requires that at least one trained supervisor make the determination for covered employees.
Return-to-duty and follow-up testing apply after an employee has violated the drug and alcohol policy and completed evaluation by a Substance Abuse Professional (SAP). The employee must pass a return-to-duty test before resuming safety-sensitive duties and then undergo unannounced follow-up testing for a minimum of six direct-observation tests in the first 12 months.
Periodic or annual testing is tied to scheduled physicals or license renewals. Because employees receive advance notice, it is the weakest deterrent against active substance use.
How Are Drug Test Results Interpreted? The Role of the MRO
The path from specimen collection to a reported result involves more steps — and more safeguards — than most employers realize. Understanding this chain is essential for anyone administering a testing program.
The initial immunoassay screen is designed for speed and sensitivity. It identifies specimens that are presumptively positive for target drug classes. However, immunoassay is inherently prone to cross-reactivity: certain over-the-counter medications (pseudoephedrine can trigger an amphetamine screen), dietary items (poppy seeds can produce opiate results), and prescription drugs can produce initial positive results in the absence of illicit substance use. This is why no employment decision should ever be based on an unconfirmed immunoassay result alone.
Non-negative specimens proceed to confirmatory testing using GC-MS or LC-MS-MS — analytical methods that identify the specific molecular structure of the substance present, effectively eliminating cross-reactivity false positives. Only after confirmation does the result reach the Medical Review Officer.
The MRO is a licensed physician with specialized training in substance abuse disorders and drug testing interpretation. The MRO role is the most misunderstood in the entire testing chain. Many employers treat MRO review as a rubber-stamping formality. In reality, the MRO conducts a verification interview with the donor to determine whether a legitimate medical explanation exists — a valid prescription, a documented medical condition, an interfering substance. A significant percentage of laboratory-confirmed positives are reclassified by the MRO after legitimate prescriptions are verified. Employers who bypass, rush, or pressure the MRO process expose themselves to wrongful-termination liability and, in DOT-regulated settings, regulatory enforcement.
Audit Point: Federal and DOT-regulated employees have the right to request split-specimen testing — a second aliquot of the original specimen is sent to a different SAMHSA-certified laboratory for independent analysis. This safeguard exists precisely because the consequences of a confirmed positive are severe, and the system must withstand challenge.
How Does Cannabis Legalization Affect Workplace Drug Testing?
No single issue is generating more policy disruption in workplace drug testing than cannabis. The landscape is shifting on multiple fronts simultaneously, and practitioners managing multi-state operations face genuinely incompatible regulatory obligations.
Over 40 US states have legalized medical cannabis, and more than 24 have legalized recreational use. That alone would complicate workplace testing. But the sharper problem is the growing wave of state employment-protection laws — enacted in California, Washington, New York, Minnesota, Connecticut, and others — that restrict employers from taking adverse action against employees or applicants based on positive cannabis test results, particularly when the use is off-duty and lawful under state law.
In December 2025, the Trump administration signed an Executive Order directing the rescheduling of marijuana from Schedule I to Schedule III. This generated significant confusion. Rescheduling to Schedule III does not equal federal legalization, and it does not change current DOT testing requirements. DOT published a December 19, 2025 compliance notice confirming that all current marijuana testing requirements remain in effect for safety-sensitive transportation workers, regardless of scheduling status. However, if marijuana does become a Schedule III substance through formal rulemaking, potential ADA implications could emerge — accommodation requests from employees using prescribed Schedule III substances may increase.
Marijuana positivity in post-accident workplace testing reached 7.3% in 2024 (Quest Diagnostics, 2025), just below the record high of 7.5% in 2023. Cannabis remains the most frequently detected substance in workplace testing. The data underscores the central tension: current immunoassay-based drug tests detect THC metabolites indicating past use, not active impairment. A worker who used cannabis legally, off-duty, three days ago will test positive on a urine screen despite being completely unimpaired at work. This metabolite-presence-versus-impairment gap is the fundamental challenge that no current testing method has fully resolved.
The practical response for many employers has been to adopt “no-THC” panel configurations in states with employment-protection laws, removing THC from the screening panel entirely while retaining it for DOT-mandated testing where federal law still requires it. Multi-state employers increasingly maintain jurisdiction-specific policy matrices — a testing policy that is legally required in one state may be prohibited in another. There is no one-size-fits-all answer here, and any article claiming otherwise is oversimplifying a genuinely fractured regulatory environment.
Jurisdiction Note: Non-US employers face entirely different frameworks. In the UK, the Health and Safety Executive provides guidance but workplace drug testing is not federally mandated; employer policies must comply with employment law and data protection requirements. Australia follows AS/NZS 4308:2008 for urine testing with its own cut-off levels that differ from SAMHSA thresholds. In Canada, drug testing must be balanced against human rights protections, and random testing of non-safety-sensitive workers has been significantly restricted by court decisions. SAMHSA cut-offs, DOT mandates, and US state cannabis laws do not apply outside the United States.
How to Choose the Right Drug Testing Method for Your Workplace
Selecting the right testing approach is not about identifying the single “best” method — it is about matching methods to specific operational needs, regulatory requirements, and risk profiles.
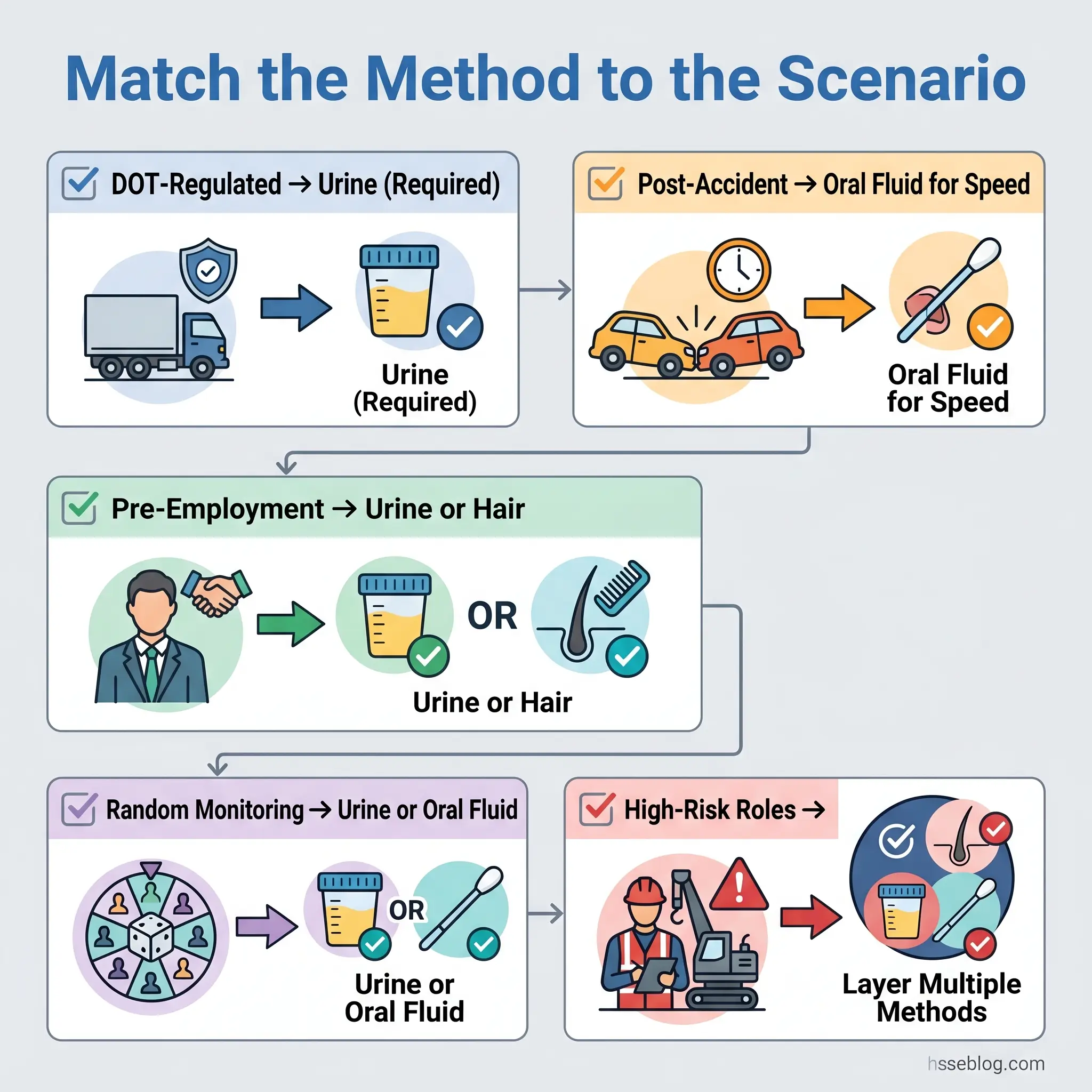
For DOT-regulated employers, the decision is currently constrained: urine is mandatory until HHS certifies oral fluid laboratories for DOT testing. Once that certification occurs, oral fluid becomes an authorized alternative — and for post-accident and reasonable-suspicion scenarios, its on-site collection speed will make it the operationally superior choice in many situations. DOT has also proposed a September 2025 rulemaking to add fentanyl to the DOT drug testing panel, which may further influence method selection.
For non-regulated private employers, the landscape is wider. Pre-employment screening has the most flexibility — urine provides cost-effective broad coverage; hair testing identifies habitual use patterns across 90 days; oral fluid catches very recent use. The choice depends on what the employer is trying to detect. For ongoing monitoring, random urine testing remains the standard, with oral fluid gaining ground where state law permits it.
The strongest programs do not rely on a single method. A combination of pre-employment hair testing (catching habitual users whose pattern spans months) with random oral fluid testing (catching recent on-the-job use that urine’s longer collection logistics would miss) covers a broader risk surface than any standalone approach. For high-risk, safety-sensitive roles outside DOT regulation, this layered strategy addresses both the habitual-use and recent-use detection gaps that a urine-only program leaves open.
Budget reality shapes these decisions. Urine testing costs the least per specimen. Hair testing costs more but provides 90 days of coverage in a single collection. Blood testing is the most expensive and least practical for routine screening. The cost comparison should be evaluated per unit of risk reduction, not per specimen — a more expensive method that catches what a cheaper method misses may cost less in prevented incidents, workers’ compensation claims, and liability exposure.
Frequently Asked Questions
Choosing a Testing Strategy That Actually Works
The difference between a drug testing program that protects a workforce and one that merely checks a compliance box comes down to three decisions: which specimens to collect, which substances to screen for, and when to test. Each decision must be calibrated to the employer’s regulatory obligations, operational risk profile, and jurisdictional constraints — not defaulted to whatever the testing vendor offers as standard.
The 2025 regulatory landscape is making two of these decisions harder and one easier. Fentanyl’s addition to the federal panel is overdue and straightforward — any employer who has not added fentanyl-specific testing to their panel is flying blind to a substance driving significant workplace positivity. The DOT oral fluid authorization, once HHS certifies laboratories, will give safety-sensitive employers a faster, harder-to-cheat collection method for the scenarios where speed matters most. Cannabis remains the unresolved problem: metabolite-based testing cannot distinguish between a worker who used cannabis legally at home three days ago and one who used it an hour before arriving at work. Until a validated impairment-detection method exists for cannabis, employers in states with employment-protection laws will continue managing a genuine operational contradiction.
Programs built on a single specimen type, a single testing occasion, and an outdated panel configuration are the ones that fail silently. The data showing seven times higher fentanyl positivity in random versus pre-employment testing is not an abstract statistic — it is the measurable cost of that silent failure. Layering methods, updating panels, and defining testing triggers with precision are the operational controls that turn a testing policy from a document into a deterrent.