
TL;DR
- If your testing panel still excludes fentanyl, you are missing a critical risk signal — fentanyl positivity in random tests is 707% higher than in pre-employment screens (Quest Diagnostics, 2025), and polysubstance co-positivity with marijuana has doubled since 2020.
- If your policy hasn’t been reviewed since 2023, it is likely non-compliant — at least 12 US states modified drug testing statutes in 2024–2025, and 8 states now prohibit adverse employment actions based on off-duty legal cannabis use.
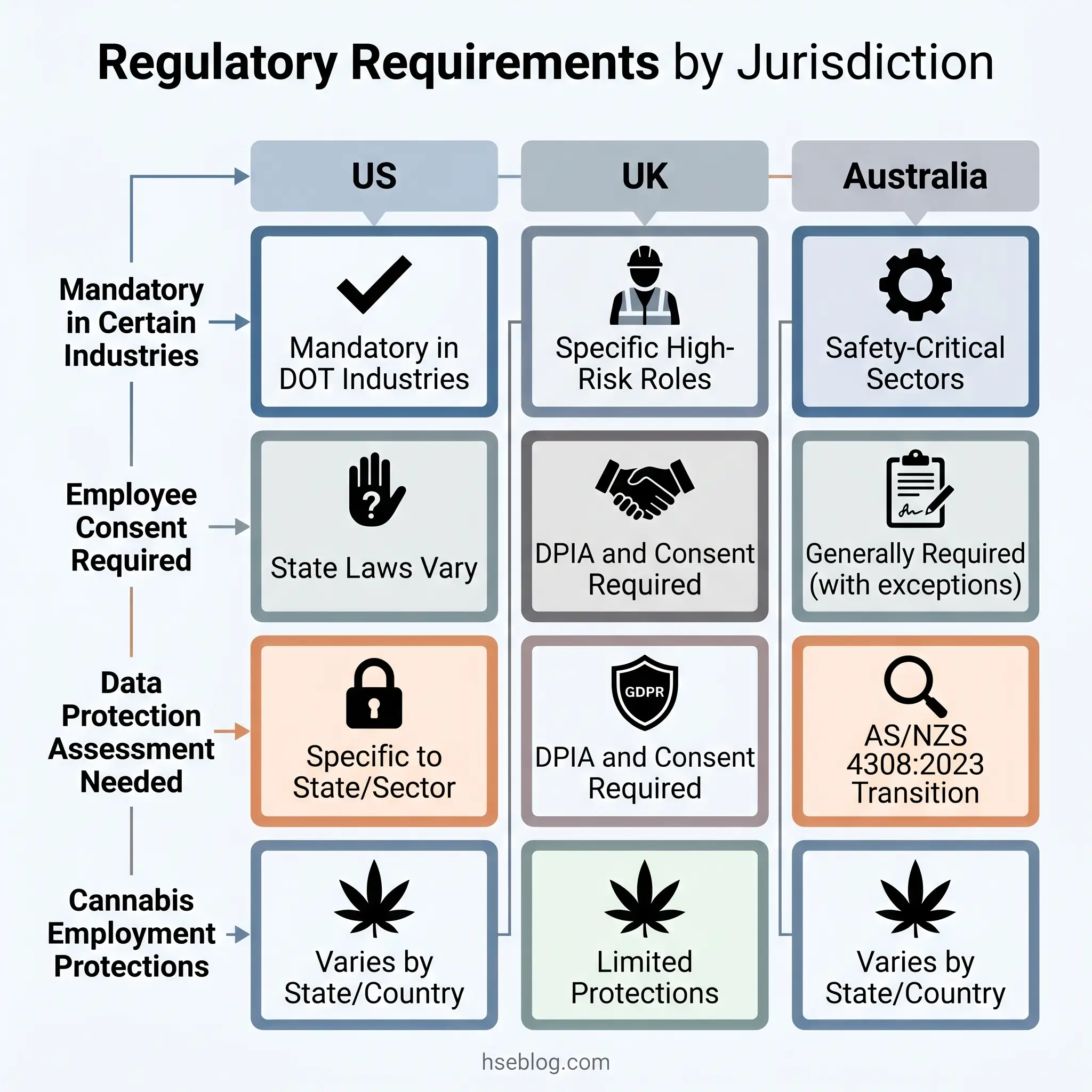
- If you operate in both the US and UK, you cannot apply a single testing policy — UK programmes require a Data Protection Impact Assessment and informed consent under UK GDPR, obligations that have no direct US federal equivalent.
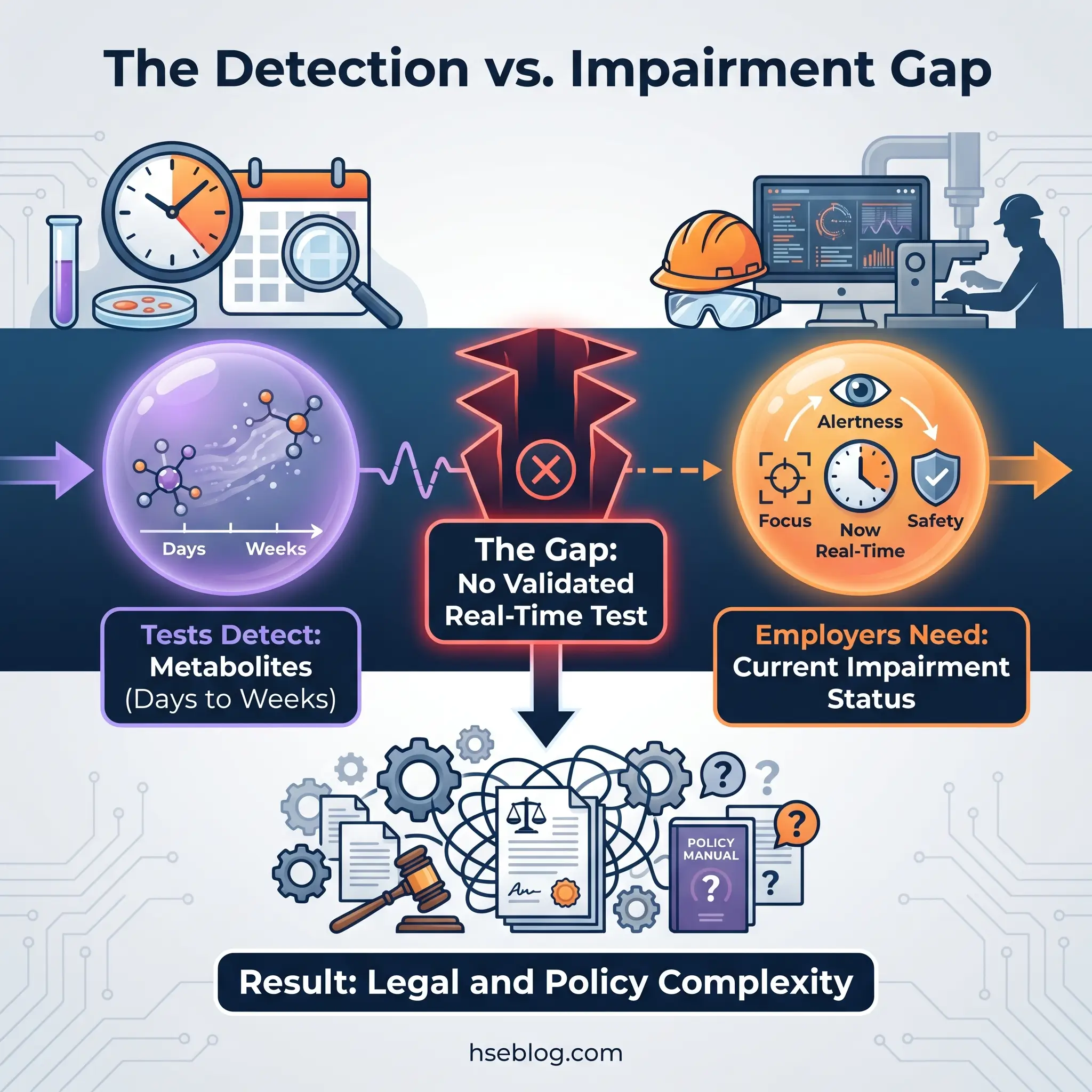
- If you rely solely on urine testing for marijuana, you are detecting metabolites that persist for days to weeks — not current impairment. No validated real-time marijuana impairment test exists as of 2026.
Workplace drug and alcohol testing is the process of analysing biological specimens — urine, oral fluid, hair, blood, or breath — to detect prohibited substances in employees or job applicants. Employers use testing to maintain workplace safety, satisfy regulatory obligations such as 49 CFR Part 40 (US) and the Health and Safety at Work etc. Act 1974 (UK), reduce liability, and support drug-free workplace programmes. The most consequential challenge facing testing programmes in 2026 is the gap between substance detection and impairment measurement — particularly for cannabis.
What Is Workplace Drug and Alcohol Testing?
Workplace drug and alcohol testing examines biological specimens collected from employees or applicants to identify the presence of drugs, drug metabolites, or alcohol. The process spans two distinct functions that are frequently conflated: detecting whether a substance has been in someone’s system within a defined window, and determining whether someone is currently impaired. That distinction — detection versus impairment — drives the most consequential policy decisions employers face today, particularly as cannabis legalisation accelerates across jurisdictions.
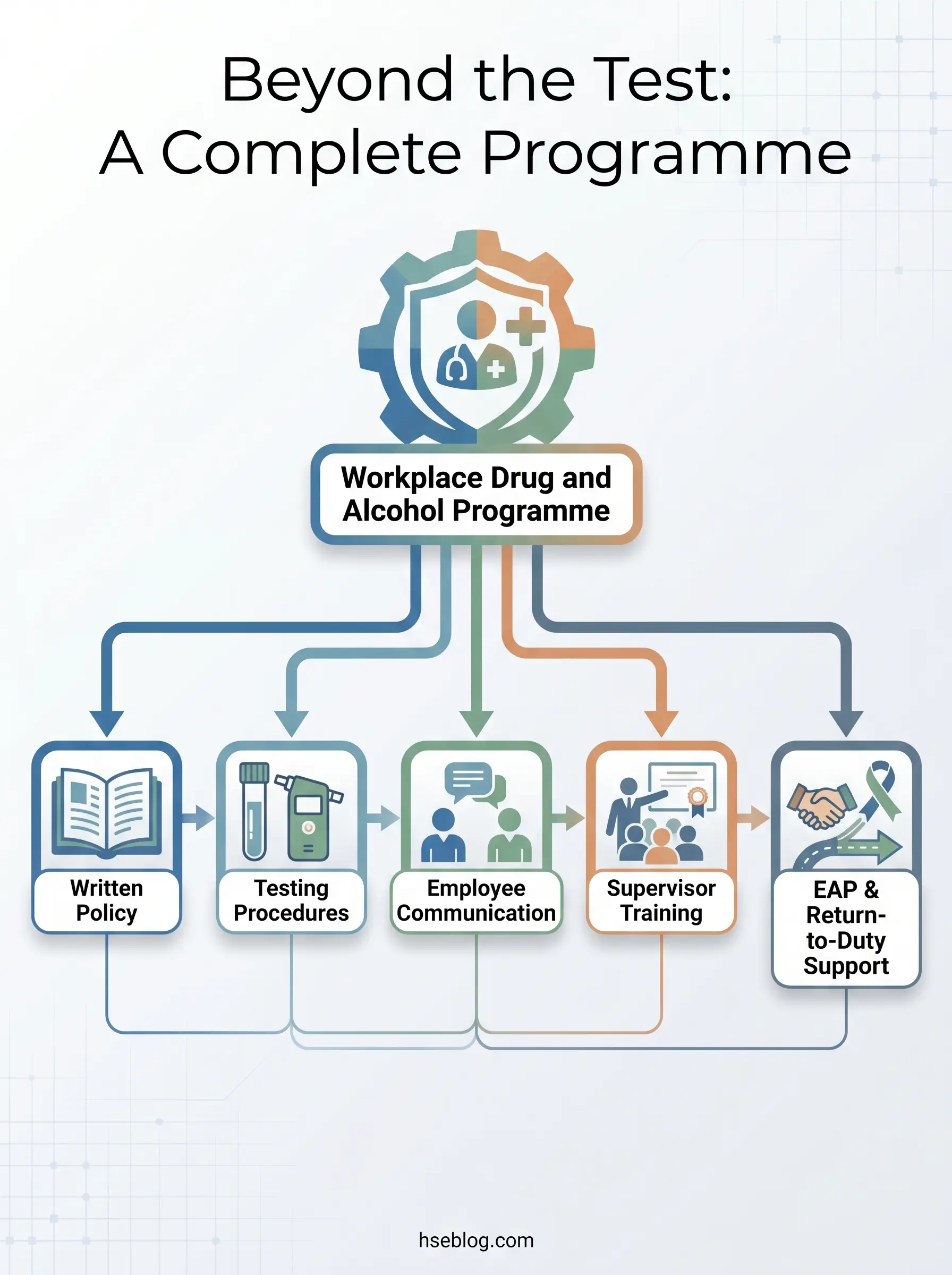
Testing is most prevalent in industries where impairment creates immediate physical danger: transportation, construction, manufacturing, mining, healthcare, and energy. In the US, industry surveys estimate that 50%–60% of employers conduct some form of workplace drug testing (industry surveys, 2025–2026). The programmes affect employers, employees, applicants, and increasingly contractors and temporary workers under host-employer policies. Yet the most common organisational mistake is treating testing as a standalone compliance checkbox rather than one component of a broader substance-misuse management programme. Testing without a clear written policy, employee communication, and genuine support mechanisms — like employee assistance programmes — tends to generate adversarial dynamics rather than meaningful safety improvement.
Why Employers Conduct Drug and Alcohol Testing
The business case for testing rests on a layered risk analysis — not simply “because the regulation says so.” Substance impairment degrades judgment, slows reaction time, and impairs coordination, all of which correlate directly with higher incident rates in safety-critical operations. An employer’s duty of care — codified under the General Duty Clause in US OSHA law and Section 2 of the Health and Safety at Work etc. Act 1974 in the UK — extends to managing foreseeable risks, including those created by impaired workers operating equipment, handling hazardous materials, or working at height.
Regulatory mandates make testing non-negotiable in certain sectors. DOT-regulated industries in the US — aviation, rail, trucking, transit, pipelines, maritime — must comply with 49 CFR Part 40’s comprehensive testing requirements. Federal contractors holding contracts valued at $100,000 or more, and all federal grant recipients, fall under the Drug-Free Workplace Act of 1988, which mandates a written drug-free workplace policy and awareness programme. Several US states offer tangible financial incentives: Alabama, Florida, and Georgia, among others, provide workers’ compensation insurance premium discounts for employers who maintain certified drug-free workplace programmes.
The economic argument extends beyond insurance. Lost productivity attributable to alcohol misuse alone costs approximately £7.3 billion per year in the UK (Institute of Alcohol Studies, cited by British Safety Council, 2024). The strongest programmes, in my professional observation, frame testing as one element of a broader safety culture rather than a punitive surveillance tool. Organisations that couple testing with genuine employee support and rehabilitation pathways consistently see better long-term outcomes — in retention, in incident reduction, and in programme credibility — than those that rely on a test-and-terminate approach.
Types of Workplace Drug and Alcohol Tests
Testing occasions are not interchangeable. Each has a distinct trigger, legal framework, and operational purpose. Treating them identically in policy or practice creates compliance gaps that surface during audits or litigation.
Pre-Employment Testing
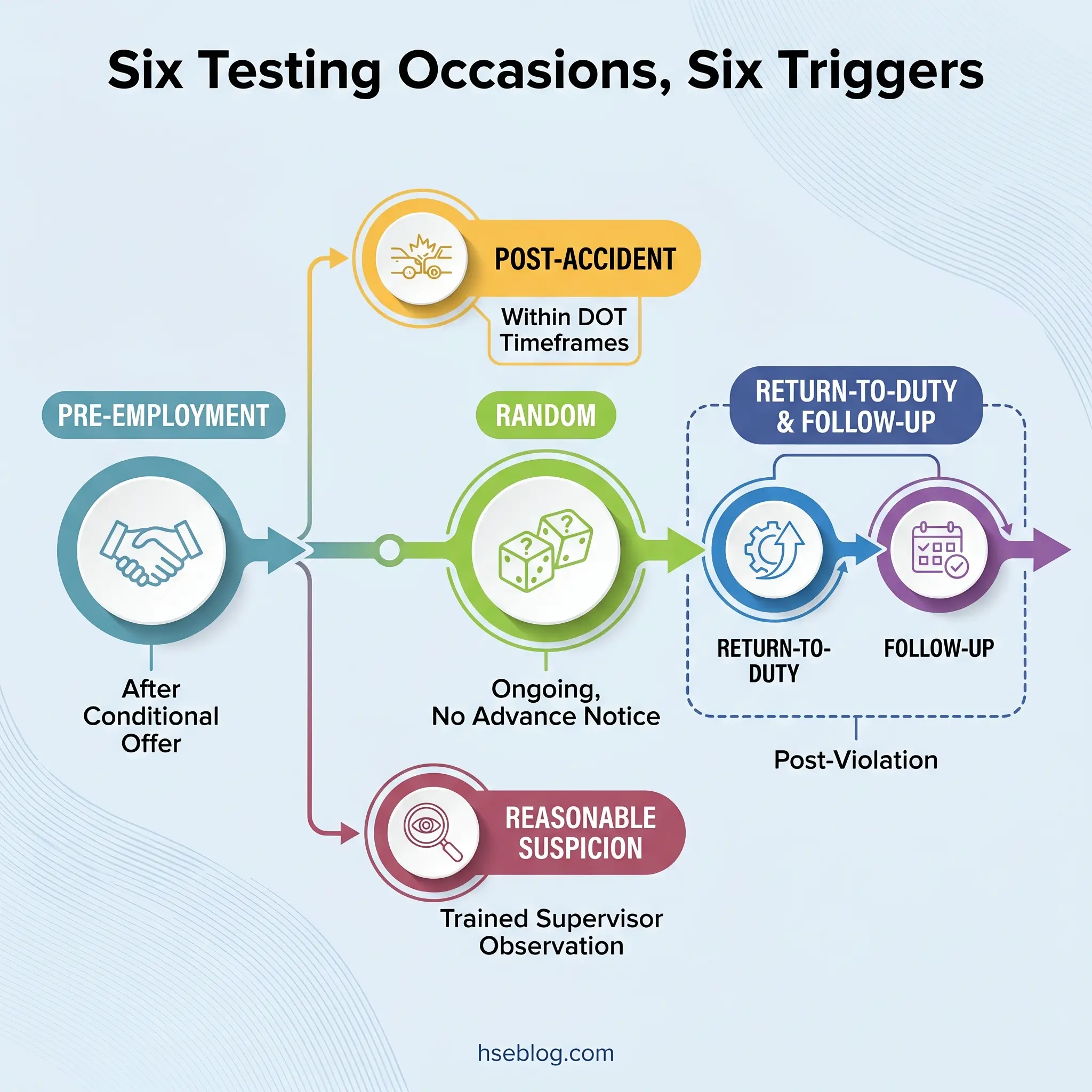
Conducted after a conditional offer of employment. Under the Americans with Disabilities Act (US), testing before a conditional offer is prohibited — the offer must come first, and it may be contingent on passing the test. Pre-employment testing is the most common testing occasion and the one most candidates expect.
Random Testing
Employees are selected from a pool using a scientifically valid random selection method — typically a computer-generated random number matched against the pool. DOT-regulated employers must meet minimum annual testing rates: 50% of the covered employee pool for drugs and 10% for alcohol. The selection is genuinely random; no advance notice of specific test dates is given, though the programme itself must be disclosed in writing.
Post-Accident and Post-Incident Testing
Triggered by a workplace incident meeting defined criteria. OSHA’s 2018 memorandum on post-incident drug testing clarified that most workplace drug testing is permissible, including post-incident testing, provided it is not used to penalise employees for reporting injuries. The key requirement: test all employees whose conduct could have contributed to the incident, not only the injured worker. DOT imposes strict timeframes — alcohol testing must occur within 8 hours of the incident, drug testing within 32 hours.
Reasonable Suspicion / For-Cause Testing
Initiated when a trained supervisor observes specific, contemporaneous indicators of possible impairment — slurred speech, unsteady gait, the odour of alcohol, erratic behaviour. This is the testing occasion where programmes most often fail legally. Supervisors who confuse legitimate impairment indicators with symptoms of medical conditions protected under the ADA expose the employer to discrimination claims. Without documented supervisor training and contemporaneous written observations, a for-cause test can become the foundation of a costly lawsuit rather than a safety intervention.
Return-to-Duty Testing
Follows a violation and is conducted only after the employee has completed evaluation by a Substance Abuse Professional (SAP) and any recommended treatment or education. A negative return-to-duty test is required before the employee can resume safety-sensitive duties under DOT regulations.
Follow-Up Testing
Ongoing unannounced testing after an employee returns to duty following a violation. DOT requires a minimum of six tests in the first 12 months, with follow-up potentially extending to 60 months based on the SAP’s recommendation.
Periodic and Blanket Testing
Some industries link drug testing to annual physical examinations. Blanket screening — testing all employees during a defined event or period — is also practised, though it carries distinct legal requirements around notice and consent that vary by jurisdiction. In the UK, blanket testing is particularly difficult to justify under the proportionality requirements of the ICO’s employment practices guidance.
Audit Point: Review your testing policy for each occasion type independently. The legal requirements for random selection methodology, reasonable suspicion documentation, and post-accident timeframes are distinct — a generic “we test when needed” clause does not satisfy any of them.
Drug and Alcohol Testing Methods: Specimens and Detection Windows
The specimen you choose determines what your programme can and cannot detect. Each method carries trade-offs in detection window, invasiveness, regulatory acceptance, and vulnerability to evasion.
| Method | Detection Window | DOT-Approved | Invasiveness | Best For |
|---|---|---|---|---|
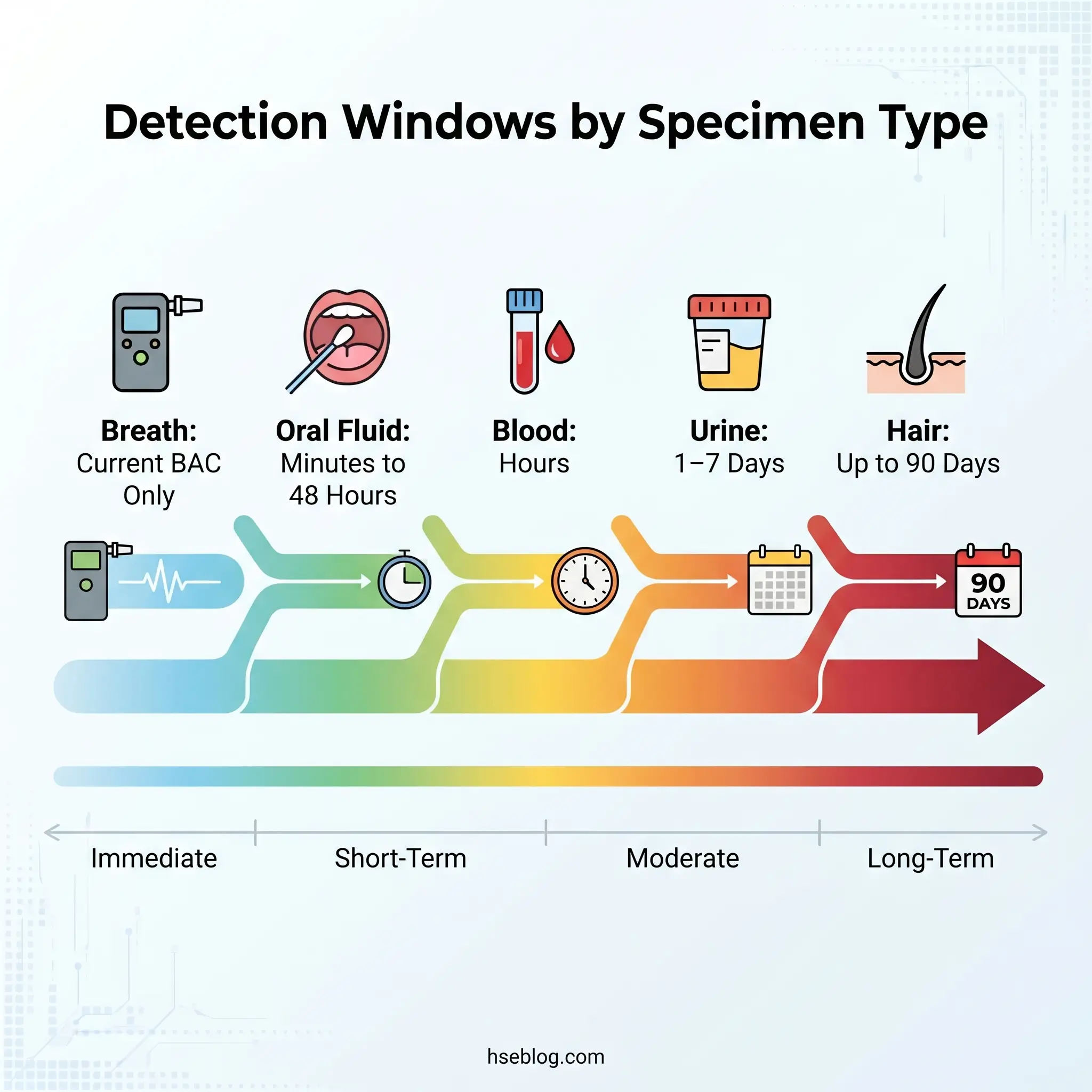
| Urine | 1–7 days (most substances) | Yes (drugs) | Moderate | Routine compliance, broadest regulatory acceptance |
| Oral Fluid | Minutes to 48 hours | Pending HHS lab certification | Low | Recent use detection, post-accident, reasonable suspicion |
| Hair Follicle | Up to 90 days | No | Low | Long-term use patterns, pre-employment screening |
| Blood | Hours | No (workplace) | High | Forensic accuracy, rarely used in workplace settings |
| Breath (BAT) | Current BAC | Yes (alcohol only) | Low | Immediate alcohol impairment, DOT alcohol compliance |
Urine remains the only currently DOT-approved specimen for drug testing and is the most widely used across all industries. Its detection window of one to seven days for most substances makes it effective for identifying recent use, though it is susceptible to adulteration and substitution — which is why chain of custody procedures and specimen validity testing exist.
Oral fluid testing has surged by more than 40% in employer adoption between 2023 and 2026. The SAMHSA workplace drug testing resources page reflects HHS’s publication of mandatory guidelines for oral fluid testing in October 2023 (88 FR 70814), establishing it as an approved specimen type alongside urine for federal testing. However, DOT cannot adopt oral fluid until HHS certifies laboratories to perform the analysis — and as of January 2026, no laboratory has received that certification. Oral fluid’s shorter detection window makes it a better proxy for recent use, which is precisely why it is gaining traction for reasonable-suspicion and post-accident scenarios.
Hair follicle testing offers the longest detection window at approximately 90 days, making it resistant to short-term evasion. Its limitation is a roughly seven-day blind spot after ingestion — hair growth takes time to incorporate drug metabolites. It is not DOT-approved.
Breath alcohol testing using an evidential breath testing device measures current blood alcohol concentration, making it the closest thing to a true impairment test in the standard toolkit. It is the DOT-standard method for alcohol testing and provides immediate, quantitative results.
An emerging strategic approach combines specimen types — using urine for routine DOT compliance while deploying oral fluid for reasonable-suspicion or post-accident situations where detecting recent use matters more than historical exposure. This dual-method strategy acknowledges that no single specimen type answers every question a testing programme needs to ask.
What Substances Do Workplace Drug Tests Detect?
Standard panel configurations have remained remarkably static for decades — even as the substances driving workplace risk have shifted dramatically. The standard 5-panel test, which dominates US workplace testing, detects amphetamines, cocaine, marijuana (THC), opiates, and phencyclidine (PCP). Extended panels add benzodiazepines, barbiturates, methadone, MDMA, and other substances in 7-, 10-, or 12-panel configurations.
The most significant panel change in years took effect on July 7, 2025: HHS added fentanyl and norfentanyl to the authorised federal workplace drug testing panel for employees in safety-sensitive, security-sensitive, and national security positions. DOT has proposed aligning its transportation testing panels with a final rule anticipated in early 2026. The urgency behind this addition is visible in the data — the 2025 Quest Diagnostics Drug Testing Index found that fentanyl positivity in random tests reached 1.13% compared to just 0.14% in pre-employment tests, a 707% disparity (Quest Diagnostics, 2025). That gap signals post-hire substance use that pre-employment screening entirely misses.
Employers who remain on legacy 5-panel configurations should evaluate whether their workforce risk profile justifies panel expansion. The fentanyl data alone makes a compelling case for safety-critical roles. Emerging substances — synthetic cannabinoids, ketamine, kratom — present additional detection challenges that standard panels do not address.
Alcohol is tested separately via breath alcohol testing or oral fluid. It is not part of numbered drug panels.
Watch For: Employers frequently assume their standard panel is “enough” because it has always been enough. The substance landscape of 2026 is not the substance landscape of 2010. A 5-panel test designed around the drugs of the 1980s does not capture the fentanyl risk that the 2025 Quest DTI data makes unmistakable.
How Does the Drug and Alcohol Testing Process Work?
The credibility of any test result depends entirely on the integrity of the process that produced it. A positive result from a flawed collection or broken chain of custody is worse than no test at all — it exposes the employer to legal challenge while providing no reliable safety information.
The process follows a defined sequence, each step carrying specific legal and procedural requirements:
- Specimen collection. A trained collector obtains the specimen using standardised procedures. For DOT testing, the collection must follow 49 CFR Part 40 protocols exactly. The collector completes a Federal Drug Testing Custody and Control Form (CCF) — a multi-part document that accompanies the specimen through every subsequent step. Urine collections may be unobserved, monitored (collector present but not watching), or directly observed (required in specific circumstances such as return-to-duty testing or when a previous specimen was reported as substituted or adulterated).
- Chain of custody. The CCF establishes an unbroken documented chain from collection through laboratory receipt, analysis, and reporting. Any gap in this chain — a missing signature, an unsealed specimen, an unaccounted transit period — can render the result legally indefensible.
- Initial screening (immunoassay). The laboratory performs an initial screen using immunoassay technology, which identifies specimens that exceed established cutoff concentrations. Specimens that screen negative are reported as negative. Specimens that screen positive or are flagged for validity concerns proceed to confirmatory testing.
- Confirmatory testing (GC-MS or LC-MS/MS). Gas chromatography-mass spectrometry or liquid chromatography-tandem mass spectrometry confirms the identity and quantity of the detected substance. This step eliminates the cross-reactivity issues that can cause immunoassay false positives.
- Medical Review Officer (MRO) review. A licensed physician specifically trained in drug testing interpretation reviews all non-negative results. The MRO contacts the donor, evaluates whether a legitimate medical explanation exists — such as a valid prescription — and makes the final determination. This step is required for all DOT testing and is the safeguard most responsible for preventing wrongful actions based on prescription medications, certain foods (poppy seeds), or other innocent exposures.
- Result reporting. The MRO reports the final result to the employer’s designated representative. Result categories include negative, positive (with substance identified), dilute, substituted, adulterated, or invalid. Donors have the right to request testing of the split specimen (Bottle B) at a different HHS-certified laboratory.
The MRO step is where competent programmes separate from problematic ones. Without it, false positives from prescription opioids, certain antidepressants, or even poppy seed consumption can lead to wrongful termination and expensive litigation.
Legal Framework for Workplace Drug and Alcohol Testing
No section of a testing programme generates more liability than the legal framework — and no section is more frequently misunderstood. The regulatory landscape varies not just between countries but, within the US, between states and even municipalities. A testing practice that is routine in one jurisdiction may be illegal in another.
US Federal Law
Three federal pillars govern workplace drug testing in the United States. The Drug-Free Workplace Act of 1988 (41 USC §§ 8101–8106) applies to federal contractors receiving contracts valued at $100,000 or more and all federal grant recipients. It mandates a written drug-free workplace policy and drug awareness programme but, notably, does not itself mandate testing — it creates the framework within which testing programmes operate.
The Omnibus Transportation Employee Testing Act of 1991, implemented through 49 CFR Part 40, establishes comprehensive mandatory testing procedures for all DOT-regulated industries. This is the most prescriptive federal testing regime, specifying collection procedures, laboratory requirements, MRO protocols, SAP evaluation, and employer record-keeping obligations in exhaustive detail.
The ADA protects employees with substance use disorders who are in recovery and not currently using illegal drugs. It also prohibits pre-offer drug testing and requires that test results be treated as confidential medical records stored separately from general personnel files. Title VII, the FCRA, and the NLRA impose additional constraints around discriminatory application, background check procedures, and collective bargaining rights respectively.
US State Variation
State-level divergence is accelerating. At least 12 US states modified drug testing statutes in 2024–2025. Eight states currently prohibit employers from taking adverse employment action based on off-duty legal cannabis use: California, Connecticut, Montana, Nevada, New Jersey, New York, Rhode Island, and Washington. Some states require specific pre-test notice, written policy distribution, or confirmatory testing before adverse action. Others restrict testing to specific occasions or industries.
The practical consequence for multi-state employers is significant. A uniform national policy that works in Texas may violate New York City’s employment protections or California’s off-duty cannabis use restrictions. Jurisdictional policy mapping — reviewing requirements in every state where employees work — is not an optional refinement. It is the difference between a compliant programme and litigation.
Jurisdiction Note: Municipal-level drug testing ordinances add another layer. San Francisco, New York City, and Philadelphia, among others, have enacted local restrictions that may exceed state-level requirements. Multi-location employers should verify local rules alongside state and federal obligations.
UK Legal Framework
The UK has no standalone drug testing legislation. Instead, the legal basis for workplace testing is assembled from multiple sources. The Health and Safety at Work etc. Act 1974, Section 2 imposes a general duty on employers to ensure, so far as is reasonably practicable, the health, safety and welfare of all employees — which extends to managing risks from substance impairment. The Transport and Works Act 1992, Road Traffic Act, and Misuse of Drugs Act 1971 provide additional industry-specific obligations.
The critical UK distinction is the privacy framework. The ICO’s employment practices guidance on drug and alcohol testing classifies drug and alcohol test results as special-category personal data under UK GDPR. Employers must conduct a Data Protection Impact Assessment (DPIA) before implementing a testing programme, obtain informed written consent, and demonstrate that testing is proportionate to the risks of the specific role. The HSE guidance on managing drug and alcohol misuse at work provides the regulatory authority’s overview of employer duties.
This proportionality requirement means blanket testing of all employees is extremely difficult to justify in UK law. Testing programmes must be targeted to roles where impairment creates genuine safety risk.
Australian Framework
AS/NZS 4308:2023, published in November 2023, updated the standard governing urine drug specimen collection, storage, and analysis for workplace testing in Australia and New Zealand. Organisations have a three-year transition period to November 2026 to align with the updated standard.
Employee Rights and Privacy Protections
Across all jurisdictions, employees retain core protections. In the US, the scope of these protections varies by state — some require informed consent before any test, others permit testing as a condition of employment without separate consent. In the UK, informed written consent is required, and an employee who has not consented to testing in their employment contract may have constructive dismissal grounds if testing is imposed unilaterally.
Confidentiality obligations are universal. Under the ADA, test results are medical records requiring separate file storage. In the UK, UK GDPR and the ECHR Article 8 right to private life impose stringent data-handling requirements. Employees everywhere retain the right to contest or explain positive results, and prescription medication disclosure is protected from use as grounds for adverse action when a valid prescription exists.
Building a Compliant Drug and Alcohol Testing Policy
Understanding the legal framework is necessary but insufficient. The framework must be translated into a written policy that is operationally clear, legally defensible, consistently applied, and regularly reviewed.
A compliant policy must address each of the following components in writing. Vagueness in any of them becomes a liability when challenged:
- Scope and covered positions. Define which roles are subject to testing and whether contractors and temporary workers are included. Safety-sensitive role definitions should reference specific job functions, not just titles.
- Prohibited conduct. State precisely what is prohibited — possession, use, impairment on duty, and the distinction between on-duty and off-duty conduct (especially critical in states with cannabis employment protections).
- Testing occasions. Specify each type of test the programme uses and the triggering conditions for each.
- Substances tested. List the specific panel and any additional substances. Update this section when panel changes occur (such as the 2025 fentanyl addition).
- Consequences of positive results and refusal. Define the range of disciplinary outcomes, including whether a SAP evaluation and return-to-duty pathway is available.
- Appeal and contest procedures. Document the employee’s right to contest a result, request split-specimen testing, and explain positive results to the MRO.
- EAP referral. Include information on the employee assistance programme, voluntary self-referral options, and the distinction between voluntary disclosure and test-triggered violations.
Distribution requires written acknowledgement signed by all covered employees. Supervisor training is essential — particularly for reasonable-suspicion determination, which requires recognising indicators of impairment, documenting observations contemporaneously, and following the correct referral procedure without diagnosing or speculating about substances.
The Fix That Works: Build a regulatory review trigger directly into the policy document itself. Specify that a mandatory policy review is triggered by any of the following: change in applicable federal, state, or local law; new SAMHSA or DOT guidelines; addition of new testing substances to the panel; a workplace incident revealing a policy gap; or expansion into a new jurisdiction. At minimum, review annually. A policy that was current in 2023 may be non-compliant in 2026 — the legislative pace on cannabis alone guarantees it.
The Marijuana Testing Challenge: Navigating Legalisation and Impairment
Cannabis is the single most complex operational issue in workplace drug testing. No other substance presents the same collision of federal prohibition, accelerating state legalisation, inadequate testing science, and genuine workplace safety concern.
The current landscape: 40 US states plus the District of Columbia permit medical marijuana. Twenty-four states plus DC allow recreational use. Federally, marijuana remains Schedule I. In December 2025, President Trump signed an Executive Order directing the DOJ and DEA to expedite reclassification from Schedule I to Schedule III. However, rescheduling has not been finalised through the full federal rulemaking process, and the operational implications for workplace testing are frequently overstated.
On December 19, 2025, DOT issued a compliance notice confirming that its marijuana testing requirements remain unchanged regardless of state legalisation or federal rescheduling. Even if rescheduling to Schedule III is finalised, Schedule III substances (such as ketamine and certain anabolic steroids) are not automatically removed from workplace testing panels. The rescheduling discussion, while legally significant, does not currently change what employers in DOT-regulated industries must do.
The deeper problem is scientific, not legal. Current urine tests detect THC-COOH, a metabolite that persists in the body for days to weeks after use depending on frequency, body composition, and metabolism. A positive urine test for THC does not indicate current impairment — it indicates use within the detection window. Oral fluid narrows the window to roughly 24–48 hours, providing a better proxy for recent use, but it is still not a true impairment test. No validated, legally defensible real-time marijuana impairment test exists as of 2026. Emerging technologies — including a THC breathalyser under development through a partnership between Cannabix Technologies and Omega Laboratories (announced May 2024) — remain pre-market.
The data, meanwhile, confirms the workplace safety concern is real. Marijuana post-accident positivity reached 7.3% in 2024, near the record high of 7.5% in 2023 (Quest Diagnostics, 2025). Fentanyl co-positivity with marijuana doubled from 10% in 2020 to 22% of fentanyl-positive specimens in 2024 (Quest Diagnostics, 2025), indicating increasing polysubstance use patterns.
The judgment call for employers is nuanced. Reflexively dropping marijuana from testing panels to avoid legal complexity introduces a different risk — one the post-accident positivity data quantifies. The more defensible approach involves policy differentiation: maintain testing for safety-sensitive roles where impairment creates immediate physical danger, consider accommodation frameworks for non-safety-sensitive positions in states with employment protections, and document the safety rationale for every testing decision. The documentation is critical — if challenged, “we’ve always tested for it” is not a defensible rationale. “Our risk assessment identifies the following impairment-related safety risks for this role” is.
Emerging Trends in Workplace Drug and Alcohol Testing
Several developments are actively reshaping how testing programmes operate, and employers who do not adapt will find their programmes both less effective and less defensible.
Fentanyl panel expansion is the most operationally urgent change. HHS added fentanyl and norfentanyl to the federal workplace testing panel effective July 7, 2025. DOT alignment is anticipated in early 2026. The case for expansion is quantified: the 2025 Quest Diagnostics Drug Testing Index showed fentanyl positivity in random tests at 1.13% versus 0.14% in pre-employment tests — a 707% difference that reveals post-hire fentanyl use invisible to pre-employment screening alone (Quest Diagnostics, 2025). The polysubstance dimension makes this more urgent: 60% of fentanyl-positive specimens in the general US workforce in 2024 were also positive for other drugs (Quest Diagnostics, 2025).
Oral fluid adoption continues its rapid trajectory. The more-than-40% surge in employer adoption between 2023 and 2026 reflects the practical advantages — less invasive collection, better detection of recent use, harder to adulterate. The bottleneck remains laboratory certification: until HHS certifies laboratories for oral fluid analysis, DOT-regulated employers cannot use it for mandated testing.
Overall positivity rates remain elevated. US general workforce urine drug test positivity stood at 4.4% in 2024, declining slightly from 4.6% in 2023 but remaining near a decade-high (Quest Diagnostics, 2025). Among federally mandated safety-sensitive workers, for-cause testing positivity reached 12.6% and post-accident positivity was 4.5% in 2024 (Quest Diagnostics, 2025). The construction sector continues to show the highest positivity at approximately 7%.
Remote and decentralised workforce testing is evolving through at-home collection kits with virtual proctoring — a direct response to the growth of distributed workforces that cannot easily attend centralised collection sites. These methods are gaining acceptance but raise chain-of-custody questions that have not been fully resolved in regulation.
Frequently Asked Questions

Conclusion
Workplace drug and alcohol testing is entering a period of faster change than at any point since the Drug-Free Workplace Act established the modern framework in 1988. Three converging forces are driving that change: the fentanyl crisis is reshaping what testing panels must detect, cannabis legalisation is rewriting which tests are legally defensible, and oral fluid technology is about to transform how specimens are collected — once HHS laboratory certification clears the final regulatory bottleneck.
Programmes built for the substance landscape of five or ten years ago are operating with structural blind spots. A 5-panel urine test designed around the drug threats of the 1980s does not capture fentanyl. A uniform national policy does not survive contact with eight states’ cannabis employment protections. A reasonable-suspicion procedure without trained supervisors and contemporaneous documentation is a discrimination claim waiting to happen. The programmes that will remain both effective and legally defensible are those designed around the risks of 2026 — not the compliance requirements of 2010.
The path forward requires three commitments: evaluate panel expansion against your workforce risk profile and the 2025 fentanyl data; map your testing policy against every jurisdiction where your employees work, including state and municipal requirements; and build regulatory review triggers into the policy itself so it evolves as the law does. Testing is a powerful safety tool, but only when the programme behind it is as current as the risks it is meant to address.