

TL;DR
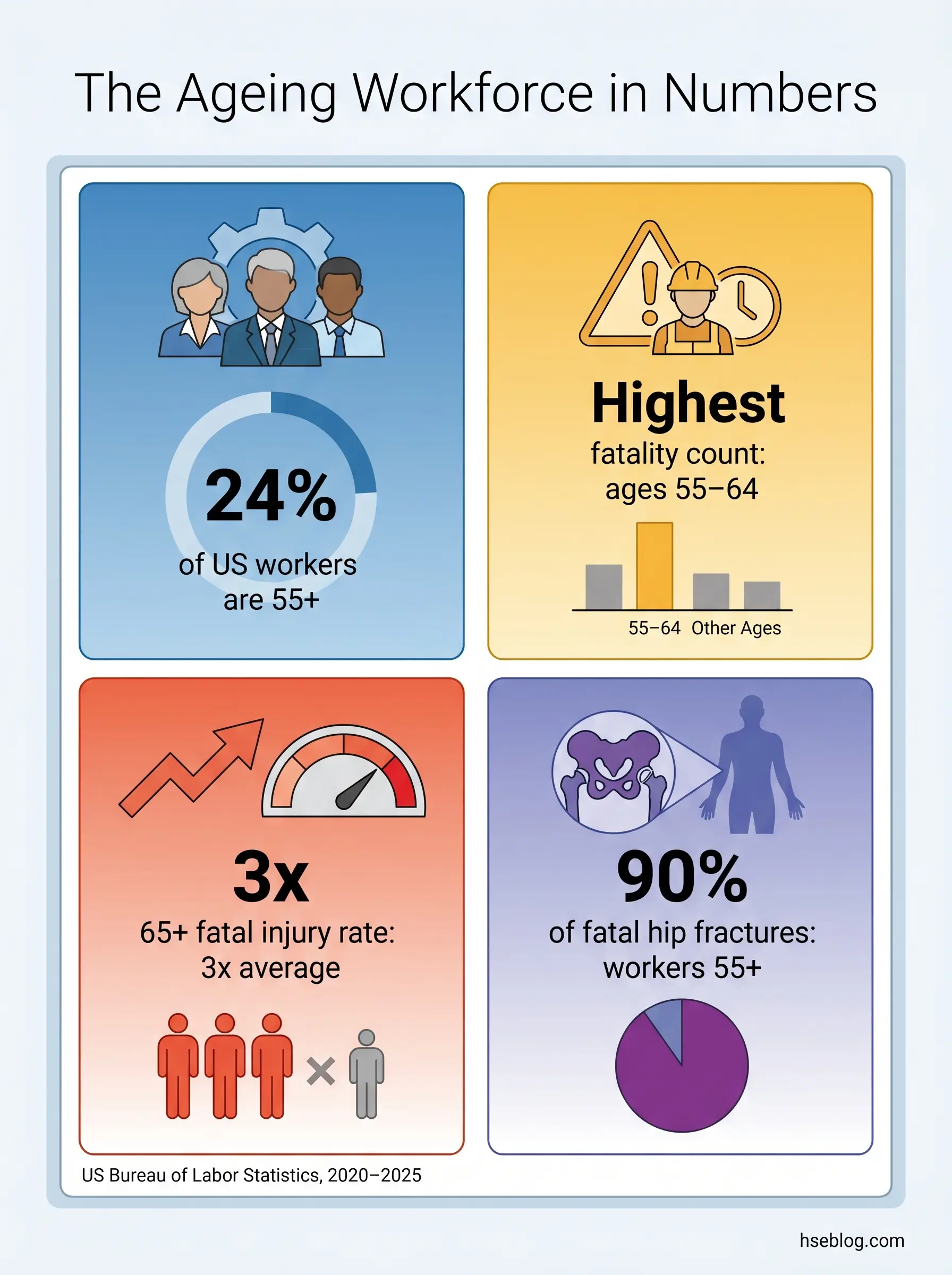
- 1,089 workers aged 55–64 died on the job in the US in 2023 — the highest fatality count of any age group, accounting for 20.6% of all workplace deaths (US Bureau of Labor Statistics, 2025).
- Fatal injury rate for workers 65+ ran at approximately 10.3 per 100,000 full-time equivalents — roughly triple the all-worker rate of 3.5 (BLS, 2020).
- 90% of fatal occupational hip fractures from 1992–2017 were sustained by workers aged 55 and over (BLS, 2020).
- Approximately one in four US workers (24%) is aged 55 or older, with the proportion still rising (NIOSH, citing BLS Current Population Survey, 2021).
Ageing workforce safety addresses the occupational risks that change as workers age — particularly increased injury severity, longer recovery, and musculoskeletal vulnerability. Effective accommodations follow the hierarchy of controls, prioritising engineering solutions like ergonomic workstations and mechanical aids over administrative adjustments, and integrate age-awareness into existing risk assessments rather than creating separate, potentially discriminatory processes.
1,089 workers aged 55 to 64 died on the job in the United States in 2023 — the highest fatality count of any age group, accounting for 20.6% of all workplace deaths that year (US Bureau of Labor Statistics, 2025). The figure tells two stories at once. The first is demographic: there are more older workers than ever, so it follows that more appear in fatality counts. The second is a safety story, and it is the one that should keep HSE managers awake. Once age is normalised against population, the fatal injury rate for workers 65 and over runs at about 10.3 per 100,000 full-time equivalents, against an all-worker rate of 3.5 (BLS, 2020). Older workers do not have more incidents — they have more lethal ones.
Workforce participation by people aged 55 and older has shifted from exception to structural fact. Pension ages have risen, knowledge-economy roles have extended viable careers, and millions continue beyond the dates earlier generations stepped away. Ageing workforce safety is therefore not a niche topic but a re-shaping of what risk assessment, control selection, and accommodation actually mean across the next two decades. This article walks through the physiological and cognitive changes that genuinely matter at work, the injury paradox that shapes their consequence, how to adapt risk assessments without creating a discriminatory parallel system, the accommodations that work in practice, the legal intersection across the US, UK, and EU, and the cultural conditions that allow the whole system to function.
Why an Ageing Workforce Changes Workplace Safety Priorities
Approximately one in four US workers — about 24% — was aged 55 or older as of 2021 (NIOSH, citing BLS Current Population Survey). In the United Kingdom, people aged 50 and over account for around a third of the workforce, and the cohort aged 65 and over has more than doubled since 2000 (Office for National Statistics, 2023). The European Union’s employment rate for the 55–64 age band reached 58.5% by 2018 and continues to climb. None of this is reversing. Pension ages are rising, mortgages run longer, and a generation reaching state retirement age in better health than its predecessors is choosing — or needing — to keep working.
The business case for retaining older workers is straightforward: lower turnover, retained institutional knowledge, supervision and mentoring capacity, and in many cases a steadier hand on operational decisions. None of that materialises automatically. It depends on whether the safety system around the work has adapted to the age profile of the people now performing it.
A consistent failure mode runs across organisations that have not adapted: ageing workforce safety gets treated as a human resources topic — pension planning, succession charting, generational tension — while the safety operating system runs on unchanged assumptions. The result is a quiet drift between the design demands of the work and the functional capacity of the people doing it. The drift does not show up in routine incident frequency, which is why it is often missed. It shows up in severity statistics, return-to-work durations, and the small subset of incidents that turn fatal.
EU-OSHA’s 2025–2034 strategy explicitly identifies the ageing workforce as one of the defining societal developments shaping occupational safety policy for the decade ahead (EU-OSHA, 2025). That positioning matters. It marks the point at which age has moved from a HR demographic detail into a core OSH planning variable.
Age-Related Physiological and Cognitive Changes That Affect Workplace Safety
The relevant changes are the ones that intersect with workplace demands. A general biology lesson is not the point. There are two categories worth distinguishing because they drive different control strategies. Normative age-related changes affect almost everyone gradually and respond to universal design — better lighting, lower lifting demands, clearer signage. Pathological conditions are more common with age but not universal, and they require individual health surveillance rather than blanket assumptions. Confusing the two is how organisations end up over-engineering controls for some workers while missing them entirely for others.
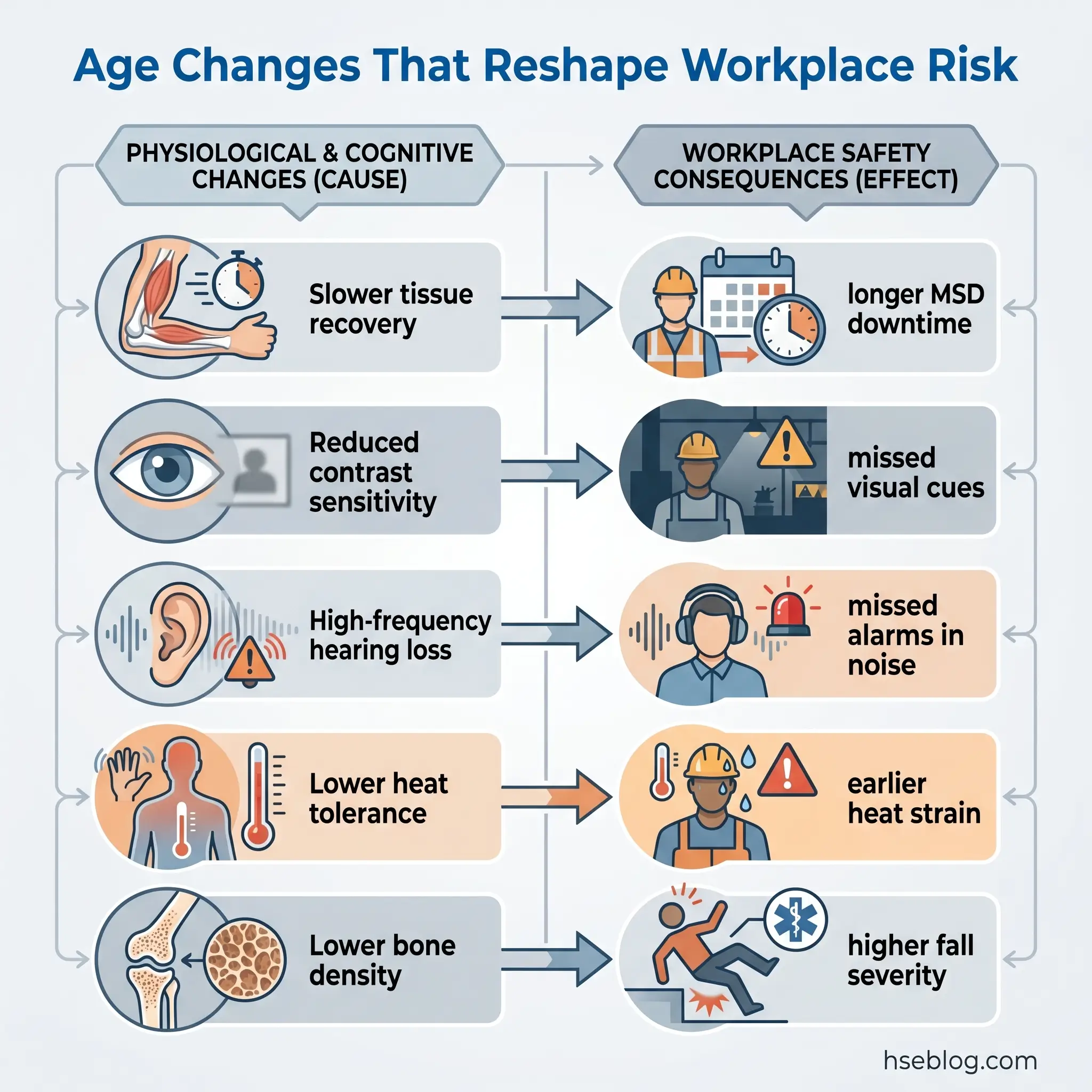
Musculoskeletal change is the most operationally consequential. Grip strength and peak muscle force decline gradually from around the fifth decade. Bone mineral density falls, more steeply in post-menopausal women. Connective tissue recovers more slowly from strain. The implication is not that older workers cannot lift — most can, and many lift more competently than younger workers because their technique is better — but that the same load produces longer recovery, and the consequence of a slip or trip is biomechanically more serious.
Vision changes earlier than most people expect. Presbyopia — the loss of near focus — typically begins in the early forties. Contrast sensitivity declines, dark adaptation slows, and glare recovery takes longer. For task design, this changes what counts as legible signage, adequate task lighting, and acceptable display contrast. The hazard is not that older workers cannot see. It is that hazard recognition relies on visual cues calibrated for younger eyes.
Hearing loss with age, especially in higher frequencies (presbycusis), has a specific operational consequence: spoken warnings and high-pitched alarms in noisy environments may register late or not at all. This matters most in transport, manufacturing, and emergency response.
Thermoregulation declines with age. Sweat response is reduced, cardiovascular reserve is lower, and hypertension and cardiovascular medication are more common — the latter sometimes blunting the body’s heat-stress response further. In hot environments and during heavy work, the same conditions that produce mild discomfort in a younger worker can produce dangerous heat strain in an older one. Arthritis and hypertension are the two most prevalent chronic conditions in workers over 55, affecting 47% and 44% respectively (NIOSH).
Cognitive change is the area most often misread. Reaction time slows modestly. Working memory capacity for novel material may decline. But crystallised intelligence — accumulated knowledge, pattern recognition, situational judgment — typically holds steady or improves through later working life. Net safety performance on familiar tasks is often equal to or better than that of less experienced workers, because experience compensates for raw processing speed and frequently overrides it. The experienced operator is, on average, the safer operator.
Recovery is the single most important data point for safety planning. When older workers are injured, the injuries are more likely to be severe, lost-time durations are longer, and full recovery is less certain. The change in capacity is gradual; the change in consequence is steep.
A pattern worth flagging: safety managers consistently over-index on reaction-time decline, which is rarely the proximate cause of incidents involving experienced workers, and under-index on recovery-time extension, which dramatically affects lost-time injury costs and return-to-work outcomes. The decline in resilience after an event is what actually reshapes risk economics for an ageing workforce.
The mapping of change to control tier is more disciplined than it looks at first glance.
| Age-Related Change | Workplace Safety Implication | Primary Control Tier |
|---|---|---|
| Reduced grip strength, slower tissue recovery | MSD risk; longer recovery from strains and sprains | Engineering (mechanical aids, load reduction) |
| Presbyopia, lower contrast sensitivity, slower dark adaptation | Hazard recognition in low light; signage and display misreading | Engineering (lighting, signage, display contrast) |
| High-frequency hearing loss | Missed alarms and verbal warnings in noisy areas | Engineering (alarm design); Administrative |
| Reduced thermoregulation; cardiovascular load | Heat stress; medication interaction | Engineering (cooling); Administrative (work-rest) |
| Slower reaction time on novel tasks | Modest; offset by experience on familiar tasks | Administrative (task assignment, training) |
| Lower bone density, fragility | Severe injury from falls and impacts | Engineering (fall prevention, surfaces) |
The Injury Paradox: Fewer Incidents, Greater Severity
Older workers report fewer occupational injuries than younger workers. They also die from work injuries at a higher rate. Both statements are true, and the tension between them is the defining feature of ageing workforce safety planning.
Workers aged 55 to 64 had the highest fatality count of any age group in the US in 2023, with 1,089 deaths — 20.6% of all workplace fatalities (BLS, 2025). The 65-plus cohort, smaller in absolute numbers, carried the highest fatal injury rate at approximately 10.3 per 100,000 full-time equivalents, roughly three times the all-worker average (BLS, 2020). The leading fatal event types for older workers are transportation incidents and falls. Hip fractures are particularly diagnostic: 90% of fatal occupational hip fractures from 1992 to 2017 were sustained by workers aged 55 and over (BLS, 2020). What would be a recoverable injury at 30 becomes a sentinel event at 70.
The non-fatal picture follows the same logic. When older workers are injured, the average days away from work per case is higher, and the recovery curve is shallower. Musculoskeletal disorders — the dominant occupational health burden across the working population — hit harder and resolve more slowly with age.
For HSE planning the implication is precise: incident frequency is not the right indicator for ageing workforce safety performance. Severity rates, lost-time duration, and the proportion of incidents producing fatality or permanent disability are the data signals that matter.
This article provides general HSE knowledge. Life-critical work — manual handling at scale, working at height, hot work, lone working in remote settings — must be planned and supervised by a competent person with relevant training, jurisdiction-specific authorisation, and site-specific risk assessment. The information here does not replace that. Recognised training pathways include NEBOSH, IOSH, OSHA outreach, and equivalent regional certifications.
How to Adapt Risk Assessments for an Ageing Workforce
A practical question that comes up often: do older workers need a separate risk assessment? In most jurisdictions, the answer is no. The HSE in the United Kingdom is unambiguous on this point — there is no requirement for a separate risk assessment for older workers (HSE guidance on health and safety for older workers). The duty under the Management of Health and Safety at Work Regulations 1999 (UK), Regulation 3, is to make a suitable and sufficient assessment of risks, considering individual worker characteristics where relevant. Age may be one such characteristic, but it sits alongside many others. The same logic applies under the EU Framework Directive 89/391/EEC, Article 6(2)(d), which requires employers to adapt work to the individual.
Designing a parallel, age-segmented assessment system is operationally cumbersome and legally risky — it can amount to indirect discrimination if it imposes less favourable treatment based on chronological age rather than demonstrated capacity.
The correct integration approach has a few moving parts:
- Build age-relevant factors into the standard reassessment trigger list. Significant changes to a task, equipment, or work environment already trigger reassessment. Add: known capability changes within the team, return-to-work events, near-misses involving fatigue or recovery issues, and shifts in shift-pattern demand.
- Assess task demands against individual capabilities, not chronological age. The question is whether the person doing this task today can perform it safely under reasonably foreseeable conditions. Age can correlate with capability, but it is not capability.
- Consult the worker. Older workers have the deepest knowledge of the task and of their own functional capacity. They are the primary source for “what feels different from how it used to,” which is often the earliest indicator that a control needs review.
- Use objective measures alongside self-report. Workers may under-report declining capacity for understandable reasons — stigma, fear of role loss, pride in performance. Functional capacity assessments where roles justify them, structured manual handling assessments, and occupational health surveillance fill the gap. Apply them on a non-discriminatory basis to all workers in equivalent roles.
- Document the safety rationale for any task-related adjustment. This is the single most useful protection against discrimination challenge, because it ties the decision to demonstrated risk rather than assumed limitation.
Field Test: A useful diagnostic question for any risk assessment review — if a worker’s functional capacity has shifted measurably in the past 12 months, for any reason, has the assessment been re-examined? If the answer is “no, the task hasn’t changed,” the assessment is incomplete. The standard is suitable and sufficient over time, not at a point.
The common failure mode is treating ageing workforce risk assessment as a one-off exercise — a tick-box audit, a single “older worker checklist” cycled once and filed away. The standard against which an assessment is judged in most jurisdictions is whether it remains suitable and sufficient over time. Ageing is, by definition, a change-over-time phenomenon. The integration must be cyclical, not episodic.
Workplace Accommodations and Controls Using the Hierarchy of Controls
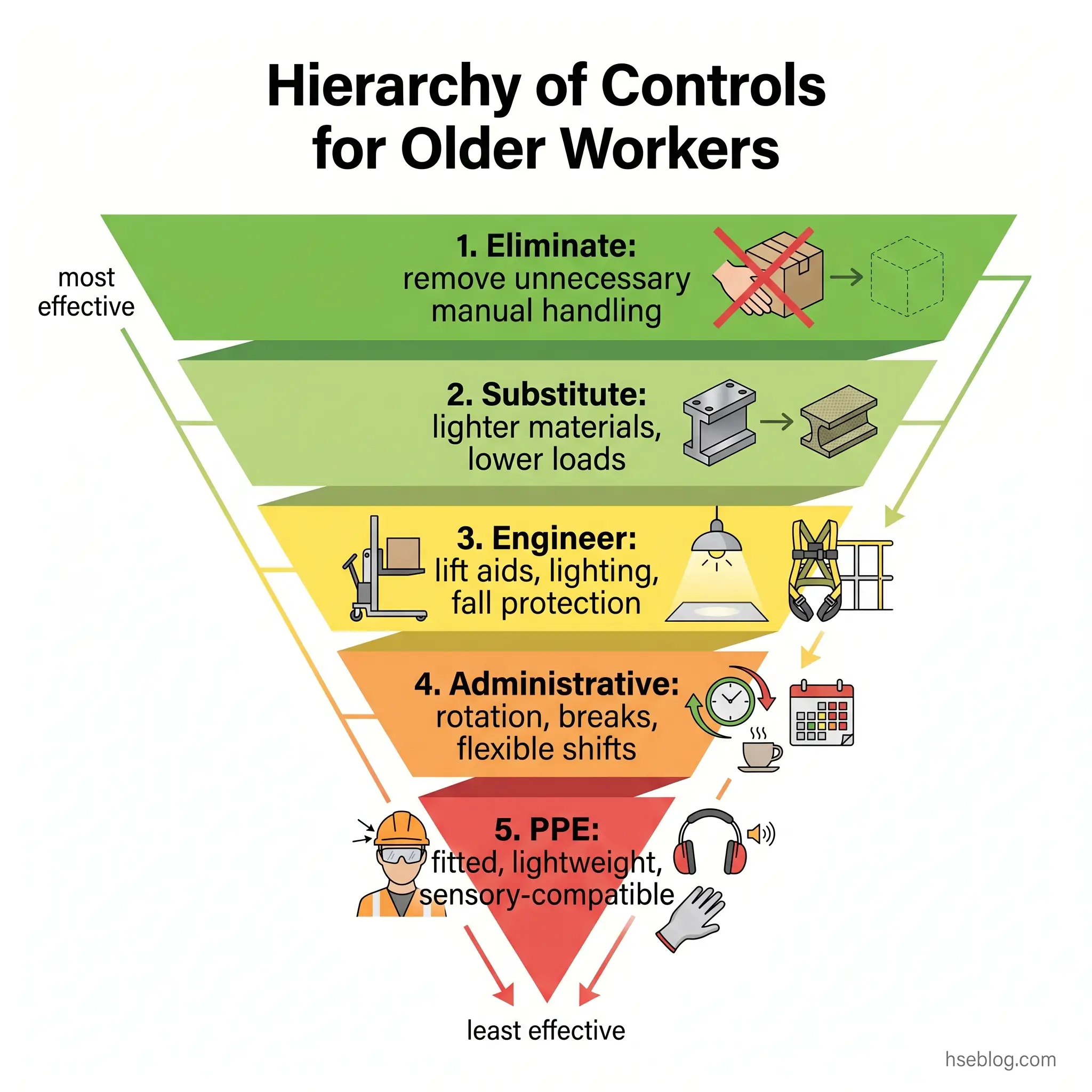
The hierarchy of controls applies here in its standard form, but the application is hazard-specific. Defaulting to PPE or administrative tweaks is the most common error — it puts the burden of capability gap onto the worker rather than designing it out of the work. The order matters because effectiveness and durability decrease as you move down the hierarchy.
Elimination and substitution come first. Tasks with no inherent value that nonetheless impose physical load can sometimes be eliminated entirely — manual handling that exists because of legacy layout, working at height that platform alternatives now make unnecessary. Substitution applies where a hazardous material, process, or piece of equipment can be replaced with a less demanding alternative that delivers the same operational outcome.
Engineering controls produce the most durable risk reduction, and this is where the bulk of accommodation work concentrates. Examples that map directly to age-related risks:
- Adjustable workstations (sit-stand desks, height-adjustable benches, positioning aids) reduce the awkward postures that compound MSD risk.
- Mechanical lifting aids — pallet jacks, scissor-lift tables, powered drivers, patient-handling equipment, exoskeleton supports for sustained overhead or stooped work.
- Anti-fatigue flooring in standing workstations.
- Improved general and task lighting, with task-specific illumination for detail work.
- Higher-contrast signage and displays, larger fonts on instrumentation, redesigned alarm tones to include lower frequencies that survive presbycusis.
- Noise reduction at source — through enclosure, damping, or substitution — which preserves communication ability across age groups.
- Guardrail systems and fall-prevention engineering above OSHA, HSE, or EU minimum where the workforce profile justifies it.
Administrative controls layer on top of engineering, not as a substitute:
- Flexible scheduling and self-paced work where the task allows.
- Job rotation to reduce cumulative repetitive strain on any one body region.
- Additional or longer rest breaks, particularly for repetitive or postural work.
- Phased retirement structured against task demands, not just hour reduction.
- Mentoring or supervisory reassignment that uses experience without imposing peak physical load.
- Avoidance of extended or night shifts where operationally possible.
- Refresher training in accessible formats with adequate absorption time.
PPE adjustments are the last layer. Properly sized and fitted equipment matters more than catalogue assumptions — fit needs change over time. Lightweight alternatives that meet the same protection standard reduce cumulative load. Prescription safety eyewear, hearing protection compatible with hearing aids, and impact-absorbing footwear all sit here.
A pattern worth flagging: engineering controls installed to support older workers — better lighting, mechanical aids, lower manual handling demand — consistently reduce injury rates across all age groups. Age-inclusive design is universal good design. The investment case is not “for older workers”; it is for the whole workforce, with the strongest measurable benefit going to the cohort most exposed to severity escalation.
Ergonomic Interventions for Physically Demanding Roles
For sectors where physical demand cannot be fully eliminated — construction, manufacturing, healthcare, logistics — ergonomic redesign carries most of the weight. A few principles are worth being specific about.
Position work in the “power zone.” Tasks performed between mid-thigh and chest height require the least biomechanical compromise and produce the lowest cumulative load across a working career.
Use mechanical aids consistently, not only when convenient. Powered drivers, lift assists, patient-handling equipment, pallet jacks, and scissor-lift tables produce the bulk of their benefit when they become the default tool, not the optional one. Cultural acceptance of using the aid matters as much as having it on site.
Build longer recovery intervals into repetitive tasks. The biology of tissue recovery extends with age. Older workers performing the same repetitive cycle are not less capable; they need more time between exposures to recover at the cellular level. Work-rest scheduling that respects this prevents the cumulative micro-trauma that becomes a chronic shoulder, back, or knee.
Consider paired-task models where they fit. Experienced older workers contribute judgment, planning, and process knowledge; younger workers handle peak physical demand. Both gain — knowledge transfers, peak load is matched to capacity, and the team is more resilient than either group working alone.
The Job Accommodation Network publishes detailed accommodations guidance for an ageing workforce organised by functional limitation, and the catalogue there is one of the more usable reference resources for HSE and HR practitioners.
Navigating the Legal Intersection: Safety Duties and Age Discrimination Law
Two legal frameworks apply to every age-related accommodation: the duty to ensure safety, and the duty not to discriminate. They look like a tension, but they operate in parallel — each is a constraint on how the other is implemented.
Regulatory content here reflects general HSE professional understanding of US, UK, and EU requirements as of 2025. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.
Under US law, the OSHA General Duty Clause (Section 5(a)(1) of the OSH Act, 1970) requires employers to provide a workplace free from recognised hazards likely to cause death or serious physical harm. The duty applies to all workers regardless of age. The Age Discrimination in Employment Act (ADEA, 29 U.S.C. §§ 621–634) prohibits employment discrimination against workers aged 40 and over. The bona fide occupational qualification exception for age is narrow and largely confined to roles where age limits are demonstrably necessary for safe operation — most case law has involved transportation and public safety roles. The Americans with Disabilities Act adds reasonable accommodation duties for workers with disabilities, which correlate with age but are not equivalent to it.
In the UK, the Health and Safety at Work etc. Act 1974, Section 2, requires employers to ensure the health, safety, and welfare of all employees, so far as is reasonably practicable. The Management of Health and Safety at Work Regulations 1999, Regulation 3, require risk assessment that considers individual circumstances, including age where relevant. The Equality Act 2010 prohibits direct and indirect age discrimination but allows treatment that is a proportionate means of achieving a legitimate aim, including health and safety outcomes.
Across the EU, Framework Directive 89/391/EEC, Article 6(2)(d), requires employers to adapt work to the individual — workplace design, equipment choice, working methods. The Employment Equality Directive 2000/78/EC prohibits age discrimination but allows justified health and safety distinctions. ISO 45001:2018, Clause 6.1.2, in its global form, requires organisations to consider worker diversity, including age, when identifying hazards and assessing risks.
Jurisdiction Note: The EU’s Framework Directive imposes a positive duty to adapt work to the worker. The US OSHA General Duty Clause prohibits known hazards but is less prescriptive about adaptation as a duty in itself. In practice, both routes converge on the same accommodations — but the documentation expected by enforcement differs. UK and EU inspectors are likely to ask what was adapted and how. US OSHA inspections focus on whether the recognised hazard was controlled.
The practical resolution that holds across all three jurisdictions has the same structure:
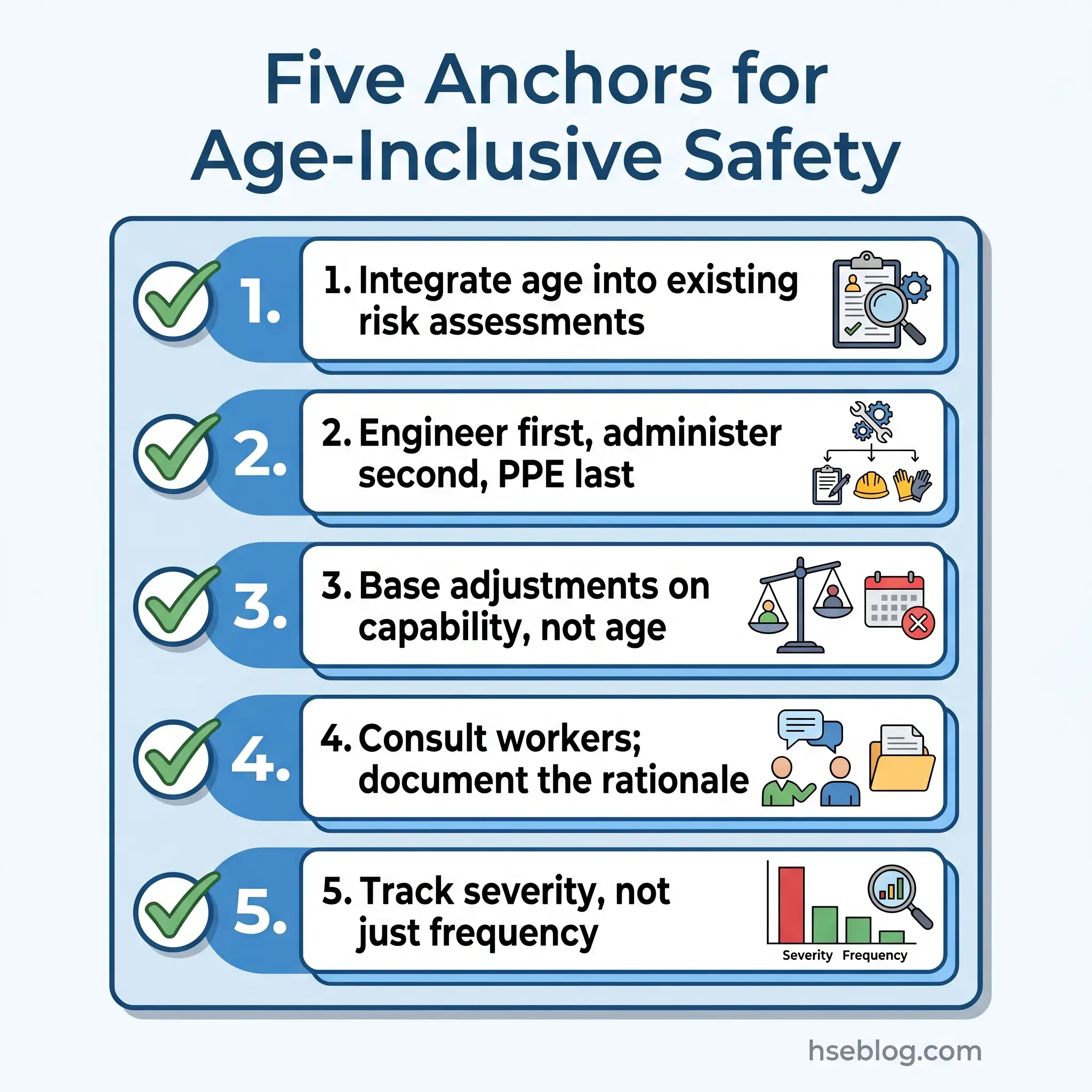
- Base accommodations on individual functional assessment, not on chronological age.
- Document the safety rationale for any adjustment.
- Consult the affected worker.
- Apply the same assessment framework consistently, regardless of which worker is being assessed.
- Avoid blanket policies tied to age (mandatory retirement, age-based duty restrictions) unless they meet the narrow, justified exception in the relevant jurisdiction.
The anxiety that surfaces most often in safety-management discussions is the fear that any age-related adjustment will provoke a discrimination complaint. The risk runs the other way more reliably. Failing to adapt work to a known capability change exposes the organisation to safety enforcement and to civil negligence claims — and the documentary trail in those cases tends to show that the capability change was visible, raised, and not acted on.
What Does an Age-Friendly Workplace Safety Culture Look Like?
Compliance gets a workplace through audits. Culture is what determines whether the controls survive contact with daily work. The organisations that produce the strongest safety outcomes for older workers tend to share a few characteristics, and the diagnostic feature is often what they don’t do.
They don’t run “older worker safety programmes” as separate initiatives. They build flexible, consultative, individually responsive safety systems from the start, which happen to serve older workers particularly well — and serve everyone else better as well.
Worker consultation is a structural feature of good practice. Older workers are the primary source of knowledge about how the task actually behaves, where its hazards sit, and what their own functional limits look like. Designing controls without that input is a guaranteed way to produce solutions that workers route around.
Training delivery matters more than training content. Self-paced delivery, practical rather than screen-only formats, and adequate time for absorption produce better retention across all age groups, but the difference is most pronounced for older workers learning new procedures or technology. One-off training events have weaker durability than spaced, repeated, contextual learning.
NIOSH’s Total Worker Health framework and ageing-and-work resources integrate workplace safety with broader worker wellbeing — chronic disease management, occupational health surveillance over the working life, and the recognition that a worker’s health status outside work shapes their risk profile inside it. The framework is particularly useful for ageing workforce planning because the chronic conditions that interact with workplace risk — arthritis, hypertension, diabetes, cardiovascular disease — accumulate over the working life and benefit from integrated rather than fragmented attention.
Knowledge transfer is the underrated outcome of an age-inclusive system. Tacit safety knowledge — hazard-recognition patterns, near-miss intuition, the small adjustments that experienced workers make to keep a task safe — is the form of knowledge most likely to be lost when an older worker leaves. Structured mentoring, paired-task models, and supervisory reassignment to experienced workers all serve to capture and transfer that knowledge before the retirement cliff.
Proactive reporting of capability change is the cultural prerequisite. Workers will not volunteer information about declining capacity if doing so risks their job, their hours, or their professional identity. A culture that frames early reporting as preventive — and that has visible accommodation pathways rather than hidden ones — converts a hidden risk into a managed one.
EU-OSHA’s resources on managing safety in an ageing workforce, including the e-guide and case studies, illustrate what this cultural integration looks like across different European industries.
Sector-Specific Risks: Where Ageing Workforce Safety Matters Most
Some sectors carry the ageing workforce safety challenge more sharply than others, due to the combination of physical demand, hazardous environments, and an above-average older worker share.
Construction is the most consequential. The sector recorded the highest fatality count of any US industry in 2023, with falls to lower level remaining the leading fatal event type. Older construction workers carry the steepest severity penalty because falls are the dominant fatal hazard, and bone density and recovery capacity decline with age. Mechanical lifting, fall-protection systems above the regulatory minimum, and task scheduling that puts demanding work at the start of the shift rather than the end are the practical levers.
Healthcare presents a different profile. Patient handling produces sustained musculoskeletal load, shift work imposes circadian disruption, and the workforce skews older — particularly in nursing and care roles. The single highest-impact intervention is patient-handling equipment used as the default, supported by no-manual-lift policies. Shift design that limits consecutive nights, especially after age 50, reduces fatigue accumulation that worsens with age.
Manufacturing involves repetitive motion, noise exposure, and machine guarding. Ergonomic redesign of repetitive workstations produces large reductions in MSD incidence across age groups, with the largest absolute benefit going to older workers who would otherwise be most exposed to cumulative damage.
Agriculture stands out as the sector with the most disproportionately older workforce. BLS analysis of fatal injury data has shown that the great majority of farmer fatalities occurred among workers aged 55 and over, with solo working, equipment hazards, and limited emergency response as the structural drivers. The accommodations that work in larger workplaces — engineering redesign, mechanical aids, paired tasks — are harder to apply on small farms. The lever there is community-level intervention: tractor rollover protection retrofits, lone worker monitoring, and access to occupational health services.
Frequently Asked Questions
Conclusion
The mistake organisations make most consistently is treating ageing workforce safety as a problem of older workers, when the real problem is the assumption that the work has stayed the same. Tasks designed when the average operator was 35 do not become harder because workers have aged; they reveal themselves as having always required more compensation than the system acknowledged. Younger workers absorb that compensation invisibly. Older workers carry the cost in severity statistics.
The single highest-impact change is shifting the design baseline. Workstations, lifting demands, signage, lighting, alarms, and shift patterns calibrated to the demands of an inclusive age range — not the unspoken default of a younger worker — produce safer outcomes for everyone, with the strongest measurable benefit for the cohort most exposed to severity escalation. The hierarchy of controls is not optional in this conversation. Engineering out the demand carries more durable risk reduction than administrative adjustment, which carries more than PPE substitution.
What makes ageing workforce safety look complicated is the legal overlay. What makes it tractable is treating the law as a guide to method rather than a barrier to action. Base every accommodation on demonstrated functional capacity and documented safety rationale; consult the worker; apply the framework consistently to everyone in the role. Organisations that do this end up with safer workplaces, more resilient workforces, and a far smaller exposure to both discrimination and negligence claims than organisations that froze in fear of either.