

TL;DR
- If a worker notifies you in writing that she is pregnant, has given birth within the past six months, or is breastfeeding — an individual risk assessment is legally required, not optional. The duty sits with the employer.
- If existing controls cannot eliminate a significant hazard — UK and EU law require a three-step hierarchy: adjust working conditions → offer suitable alternative work on equal terms → suspend on full pay. Skipping to suspension or early maternity leave is unlawful.
- If the assessment is completed once at notification and never revisited — it has failed. The hazard profile shifts through each trimester and again on return to work.
- If you operate across UK, EU, and US sites — apply the stricter standard. EU and UK law prohibit specific exposures outright; the US Pregnant Workers Fairness Act 2023 frames the same problem as case-by-case reasonable accommodation.
A new and expectant mothers risk assessment identifies and controls workplace hazards affecting pregnant workers, those who have given birth within six months, or breastfeeding workers. UK employers must conduct an individual assessment once written notification is received and follow a legal hierarchy: adjust conditions, offer alternative work on equal terms, or suspend on full pay as a last resort.
Approximately 54,000 mothers a year in the UK are dismissed, made compulsorily redundant, or treated so poorly they feel forced to leave their jobs (Department for Business, Innovation and Skills and Equality and Human Rights Commission, 2016). One in twenty-five mothers reported leaving a job specifically because workplace health and safety risks were not adequately addressed (BIS/EHRC, 2016). Behind those numbers sit individual cases where a risk assessment was either never conducted, completed once and forgotten, or so generic it did nothing to protect the person carrying it.
A new and expectant mothers risk assessment is the legal mechanism that prevents most of those failures — but only when treated as a living conversation about a specific person’s specific role, not a downloaded template signed and filed. This guide walks through what the assessment must cover, when it must be reviewed, how the hazard profile changes across trimesters, and how to manage the escalation pathway when controls cannot eliminate the risk. It draws on UK, EU, US, and ILO frameworks because a growing share of HSE practitioners now operate across jurisdictions where the rules diverge sharply.
Competent-person caveat: This article provides general HSE knowledge on pregnancy and maternity risk assessment. Life-critical decisions about exposure to chemicals, biological agents, ionising radiation, or fitness for specific tasks must be made by a competent person with relevant training and, where appropriate, in consultation with an occupational health physician, the worker’s GP, or midwife. The information here does not replace that advice or a workplace-specific risk assessment.
What Is a New and Expectant Mothers Risk Assessment?
The phrase covers three distinct categories of worker, not one. UK and EU law define a “new or expectant mother” as a worker who is pregnant, has given birth within the previous six months, or is currently breastfeeding. Each category carries different hazard concerns, different review trigger points, and — in some jurisdictions — different prohibited exposures. Treating them as a single status is one of the most common documentation errors I see when reviewing assessments.
The duty operates on two levels, which sit on top of each other rather than substituting for one another:
- The generic assessment, conducted as part of the employer’s general workplace risk assessment under Regulation 3 of the Management of Health and Safety at Work Regulations 1999. This must consider risks to women of childbearing age, even before any worker is pregnant.
- The individual assessment, triggered specifically once a worker provides written notification of pregnancy, recent birth, or breastfeeding. This is governed by Regulation 16 of the same instrument and focuses on the specific person, role, and circumstances.
The practical reading of this clause on most sites is that the generic assessment carries the heavier preventive weight, because the highest-risk window for chemical and biological teratogenicity is the first trimester — often before the worker has notified, and sometimes before she knows she is pregnant. Yet most organisations I review treat the generic component as a tick-box exercise filed once and never revisited, leaving the individual assessment to start from scratch the moment an email arrives. That sequencing is backwards.
| Aspect | Generic assessment | Individual assessment |
|---|---|---|
| Trigger | Required regardless of notification | Written notification from the worker |
| Scope | All women of childbearing age | The specific named worker |
| Frequency | Reviewed as part of the wider site risk assessment cycle | At notification and at each material change |
| Role | Identifies hazards and baseline controls | Tailors controls to the individual’s role and circumstances |
Watch For: Templates that conflate the two assessments into a single document completed only on notification. By the time the form is opened, the worker has already worked through the most teratogenically sensitive weeks of pregnancy — often without controls calibrated for that exposure window.
Legal Duties: Who Is Responsible and What the Law Requires
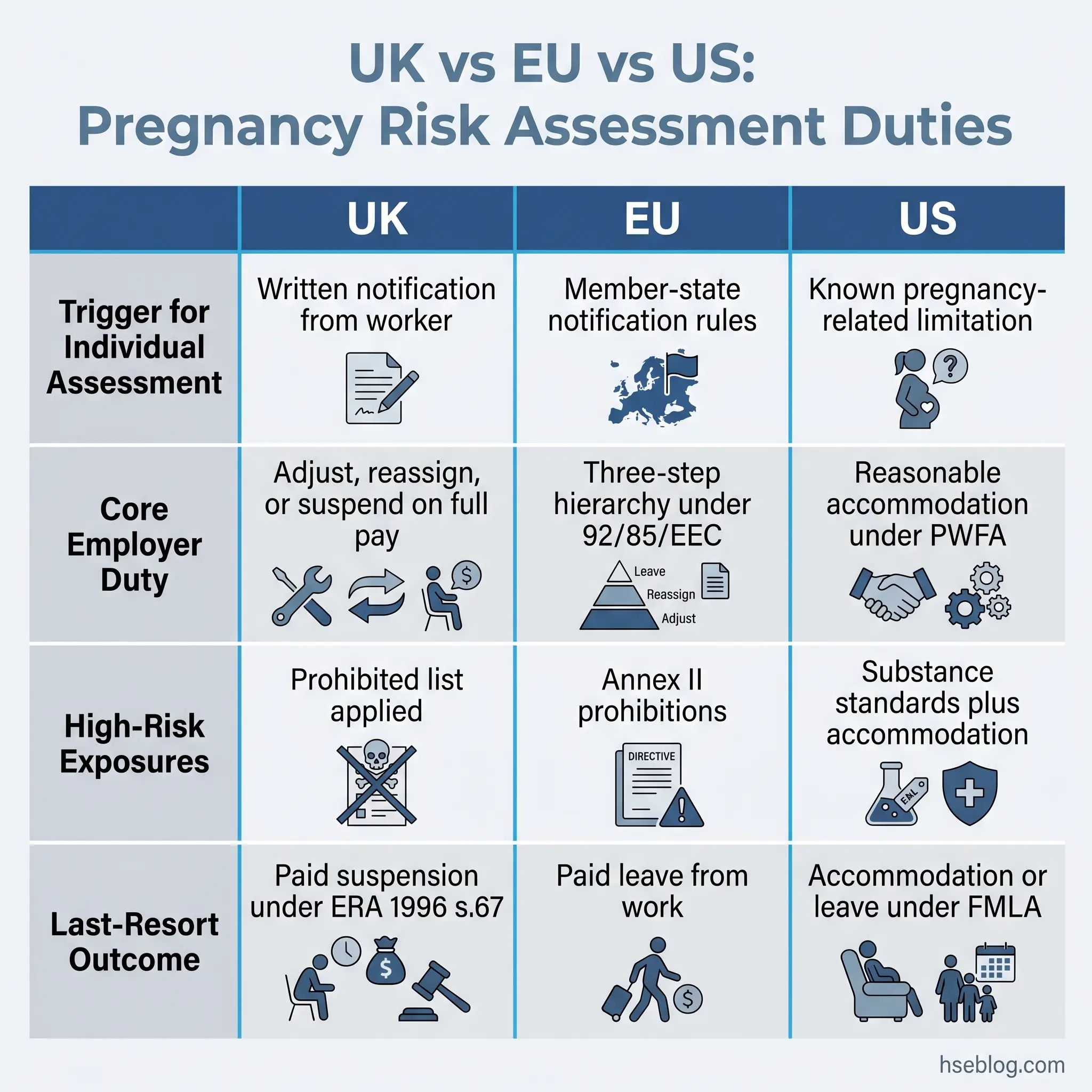
Regulation 16 of the Management of Health and Safety at Work Regulations 1999 places the assessment duty squarely on the employer — not on the worker, not on occupational health, not on a contracted advisor. The employer can delegate the conduct of the assessment but cannot delegate the legal responsibility for it. Section 67 of the Employment Rights Act 1996 then governs what happens when the assessment identifies risks that cannot be controlled in the existing role: suitable alternative work must be offered on the same terms and pay before any suspension can take effect. The Equality Act 2010 sits over both, making it unlawful to dismiss or treat a worker unfavourably because of pregnancy, maternity leave, or breastfeeding.
Across the Channel, EU Council Directive 92/85/EEC operates on a similar architecture but with one structural difference: Annex II prohibits exposure of pregnant or breastfeeding workers to specified agents outright, irrespective of control measures. Lead and lead derivatives, mercury, and underground mining work all sit on this prohibition list. There is no employer discretion to risk-assess these into compliance — the exposure must end. UK retained law follows the same approach.
The US position is structurally different. The Pregnant Workers Fairness Act 2023, with the EEOC’s final rule effective 18 June 2024, frames the problem as reasonable accommodation rather than prescribed prohibition. Employers covered by the Act must provide accommodations for known limitations related to pregnancy, childbirth, or related medical conditions unless doing so would impose undue hardship. OSHA’s general duty clause and substance-specific standards (such as 29 CFR 1910.1025 for lead) overlay this with concrete exposure limits. The PUMP Act extends related protections to nursing workers.
International framing comes from the ILO Maternity Protection Convention, 2000 (No. 183). Article 3 obliges ratifying states to ensure that pregnant or breastfeeding women are not required to perform work prejudicial to their health or that of the child. The Convention has been ratified by a relatively small number of states, but its principles inform expectations in many more.
Jurisdiction Note: When the same chemical agent is treated differently across jurisdictions — for example, an exposure that would be outright prohibited in the EU but permitted with accommodation in the US — the operationally and ethically defensible position is to apply the stricter standard. EU-OSHA’s summary of Directive 92/85/EEC and the EEOC’s PWFA guidance lay out the two regimes side by side.
A development worth flagging: the UK Employment Rights Act 2025 introduces enhanced dismissal protections for pregnant workers and those returning from maternity leave, expected to take effect in 2027 (Acas, 2025). Between 2007/08 and 2019/20, Employment Tribunals received between 1,200 and 1,900 pregnancy-related dismissal and detriment claims annually (UK Government, 2025). Once the new protections come into force, the evidentiary weight of a properly conducted, contemporaneously documented risk assessment will rise sharply — it becomes the central artefact distinguishing a lawful redundancy or capability dismissal from a discriminatory one.
Regulatory currency note: Regulatory content in this article reflects general HSE professional understanding of the listed jurisdictions as of 2026. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.
The Three-Step Action Hierarchy When Risk Cannot Be Eliminated
Once the assessment identifies a risk that cannot be eliminated through engineering controls, PPE, or procedural changes within the existing role, UK and EU law require employers to work through three actions in order. They are sequential, not interchangeable.
- Action 1 — Adjust the working conditions or hours. This is the lowest-friction option. Examples include shifting from night to day shifts, reducing total hours, redistributing manual handling tasks, providing seating for predominantly standing roles, or removing the worker from a specific exposure (such as anaesthetic gas in a recovery suite) while keeping the rest of the role intact.
- Action 2 — Offer suitable alternative work. If adjustment is not feasible, the employer must offer alternative work on the same terms and conditions, including pay. The alternative must be genuinely suitable — not menial, not punitive, not at a different site that creates a meaningful commuting problem.
- Action 3 — Suspend on full pay. Only when neither of the above is possible. Section 67 of the Employment Rights Act 1996 makes this a paid suspension, not maternity leave. The distinction matters: maternity leave consumes the statutory entitlement and starts the maternity pay clock; paid suspension does neither.
The judgment call here is between Action 1 and Action 2. In most operational contexts the balance favours Action 1 because it preserves the worker’s role, team relationships, and professional continuity. Action 2 should follow when the role is structurally incompatible with pregnancy or breastfeeding (a confined-space rescue post, for example), not when adjustment merely requires effort.
When to Conduct and Review the Risk Assessment
A consistent failure mode in published Employment Tribunal decisions and HSE enforcement notices is the one-and-done assessment: completed within days of notification, signed by the line manager, and never opened again. By the third trimester the worker’s mobility, fatigue, balance, and circulatory load have all changed — but the controls remain calibrated for week 12. The result is either a worker silently coping with an unsuitable role or an avoidable incident that the existing assessment, on paper, said had been “controlled.”
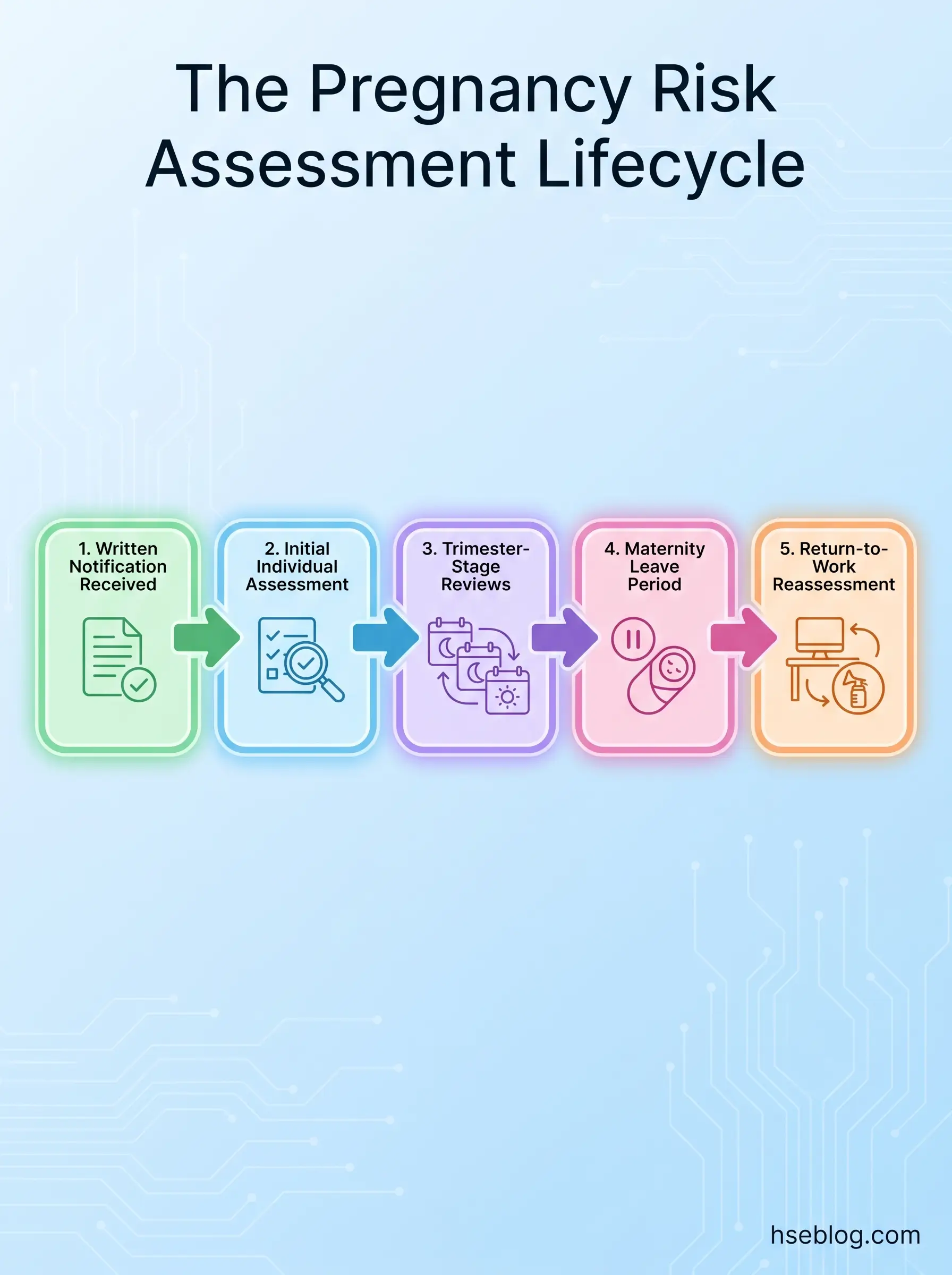
The assessment should be reviewed at five trigger points:
- On written notification of pregnancy — the initial individual assessment.
- At each trimester transition — typically once between weeks 14 and 26, and again from week 27 onwards. Some workplaces add a 36-week review where physical demand is significant.
- On material change to work activity or workplace — new equipment, relocation, role change, project mobilisation, change in shift pattern.
- On medical advice from GP, midwife, or occupational physician — particularly where a medical condition such as pre-eclampsia, gestational diabetes, or hyperemesis gravidarum is identified.
- On return to work — separately for breastfeeding workers and for those returning within six months of birth, with attention to post-caesarean recovery, pelvic floor recovery, and lactation needs.
Treating the assessment as a scheduled conversation rather than a form release puts the worker, who knows her body and her role better than anyone else, at the centre of the process. Without that conversation, the document degrades into something an employment tribunal will read with suspicion.
How to Conduct the Risk Assessment: Step-by-Step Process
The assessment is collaborative by design — it requires input from the worker, the line manager, and where applicable a safety representative or occupational health professional. The HSE’s employer guidance on risk assessment for pregnant workers sets out the regulatory floor; the procedural detail below adds the practitioner layer.
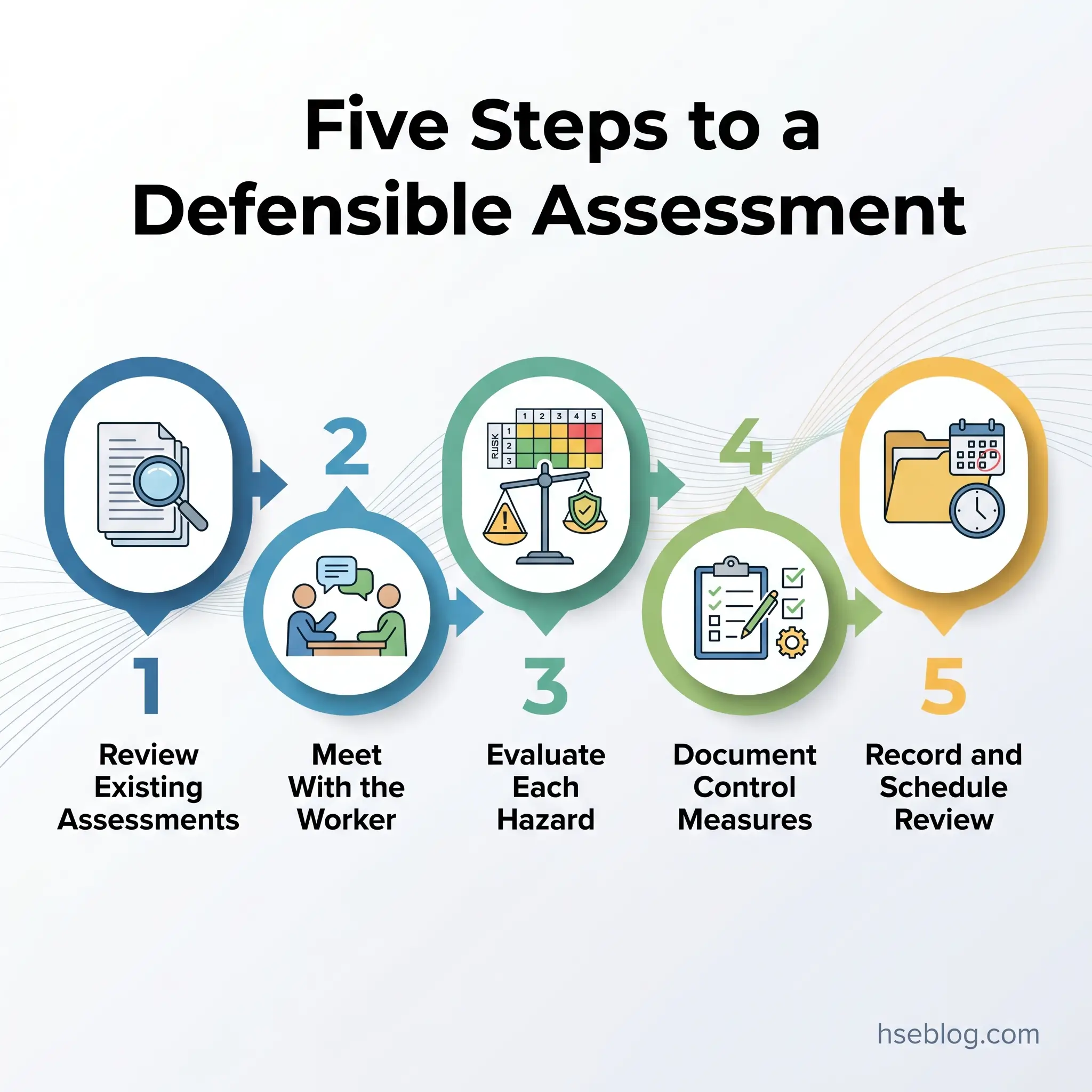
Step 1 — Review existing workplace risk assessments. Pull the general role-based assessment, any task-specific assessments (manual handling, COSHH, DSE, lone working), and the current generic women-of-childbearing-age assessment. Identify which existing hazards become more significant or change character during pregnancy, recent post-birth, or breastfeeding. This step is often skipped, with the assessor starting from a blank pregnancy template — losing the institutional knowledge already captured in those baseline documents.
Step 2 — Meet with the worker. Schedule a private, structured conversation. Cover her specific circumstances, any medical advice received, any concerns about specific tasks, fatigue patterns, antenatal appointment scheduling, commuting, and rest needs. The worker frequently identifies risks the manager has not considered — a corridor temperature, a step ladder used twice a week, a stockroom layout that requires a twist to reach a top shelf — and this conversation is where those become visible.
Step 3 — Evaluate each identified hazard. Match each hazard to the worker’s role, current trimester, and any medical recommendations. The same hazard category (manual handling, for example) may carry very different residual risk depending on whether the worker is at week 10 with mild morning sickness or week 32 with reduced mobility and altered centre of gravity.
Step 4 — Determine and document control measures. For each significant hazard, document the existing controls, the residual risk, the additional controls being put in place, the responsible person, and the date by which the additional controls must be implemented. Vague entries (“monitor situation,” “discuss with manager”) signal an assessment that has not been completed properly.
Step 5 — Record findings, share with the worker, and schedule the next review. The worker should receive a copy and be invited to question or correct anything that does not match her experience of the role. The next review date should be entered now, not left to be set later.
Audit Point: When auditing a completed assessment, the most diagnostic question is not “have all the boxes been ticked?” but “could a stranger reading this document, six months after it was written, identify which controls were specific to this worker and which were copy-pasted from a template?” If the answer is no, the assessment will not survive a competent tribunal review.
Workplace Hazards to Assess for New and Expectant Mothers
The hazard catalogue below is structured by category. None of it is exhaustive — site-specific assessment will identify hazards that no generic list can predict — but these are the categories that consistently appear in HSE guidance, EU Directive 92/85/EEC annexes, and OSHA reproductive hazards literature.
Physical hazards. Manual handling carries elevated significance during pregnancy because of ligament laxity (relaxin-mediated joint loosening) and progressive postural instability. Whole-body vibration, ionising radiation, extreme temperatures, work at height, and slip/trip exposures all warrant specific evaluation. Noise exposure is increasingly recognised as a foetal hazard from around the second trimester onwards, when sound transmits through the abdominal wall to the developing auditory system.
Chemical hazards. Lead and lead compounds, mercury, pesticides, cytotoxic drugs, anaesthetic gases, and solvents are all in scope. Under EU Directive 92/85/EEC Annex II, exposure to certain agents — including lead and its derivatives — is prohibited for pregnant or breastfeeding workers regardless of control measures. UK COSHH Regulations 2002 require that the assessment specifically consider whether the worker is pregnant or breastfeeding. The first trimester is the highest-risk window for teratogenicity, which is why the generic assessment for all women of childbearing age matters operationally.
Biological hazards. Rubella, hepatitis B, varicella (chickenpox), toxoplasmosis, cytomegalovirus, parvovirus B19, Zika, and a range of other agents present specific concerns during pregnancy. Healthcare, education, veterinary, agricultural, laboratory, and waste-handling roles all warrant biological-agent assessment. Vaccination status documentation is part of this — workers without immunity to rubella or varicella may need temporary redeployment from paediatric care during outbreaks.
Ergonomic and DSE hazards. Prolonged sitting raises deep vein thrombosis risk, which itself increases through pregnancy. Workstation fit changes as abdominal size increases — desk depth, keyboard position, and chair adjustability all become factors that worked fine pre-pregnancy and stop working at 28 weeks. Display screen equipment assessments under the Health and Safety (Display Screen Equipment) Regulations 1992 should be reopened, not assumed.
Psychosocial hazards. Work-related stress, excessive workload, pace pressures, and pregnancy-related bullying or harassment all sit within the assessment scope. Stress is not a soft hazard here — chronic occupational stress has been associated with adverse pregnancy outcomes in published occupational health literature, and the Equality Act 2010 captures pregnancy-related harassment as unlawful discrimination.
Working conditions. Night work, lone working, excessive hours, inadequate rest facilities, and insufficient access to toilets or drinking water all need explicit evaluation. Night work in particular has been associated in published research with adverse pregnancy outcomes and warrants pattern adjustment where the worker requests it on medical advice.
How Risks Change by Trimester
A risk profile set at week 8 does not survive contact with week 32. The differentiating value of a competently conducted assessment is its responsiveness to this evolution.
| Stage | Dominant physiological changes | Risk-profile shifts |
|---|---|---|
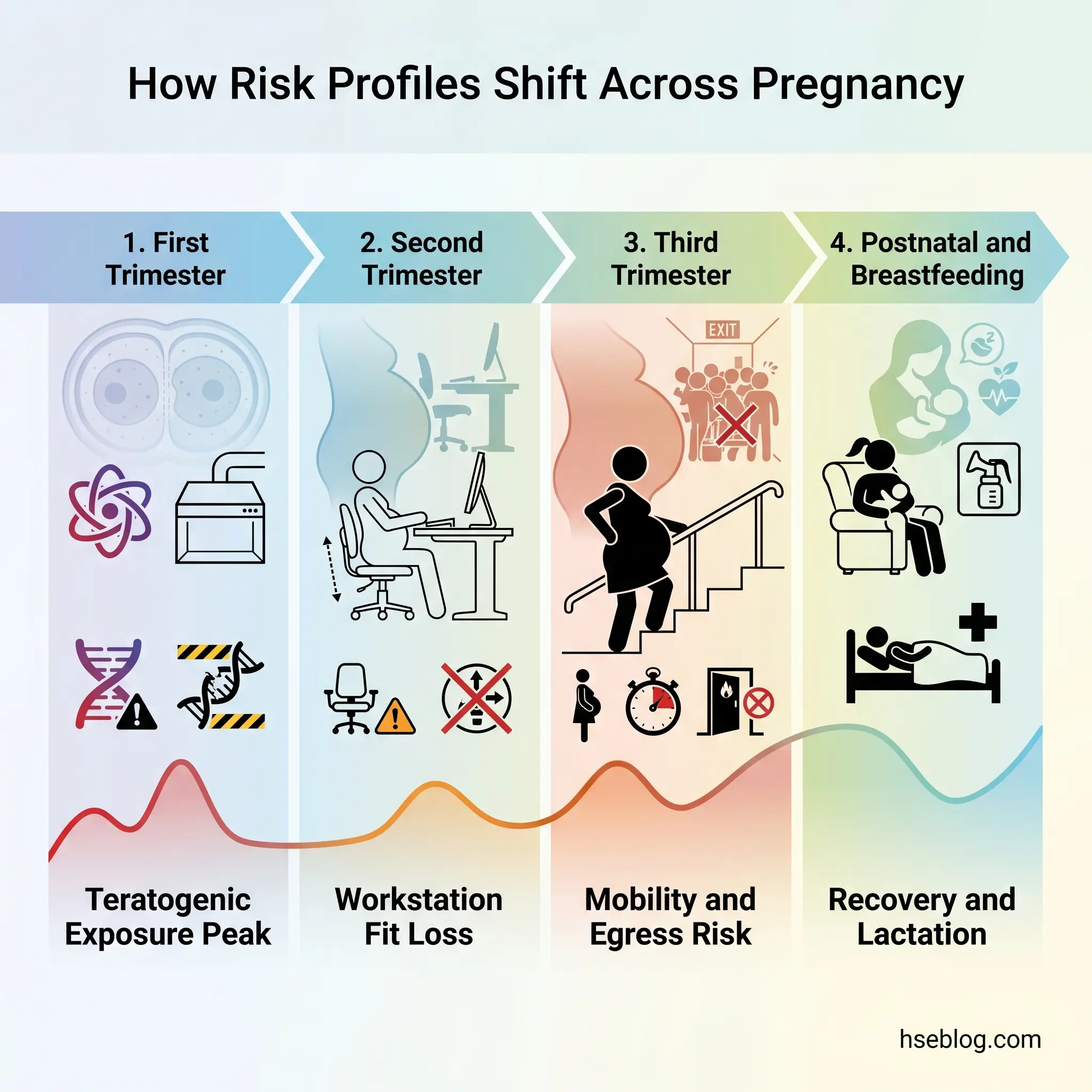
| First trimester (weeks 1–13) | Fatigue, nausea, hormonal shifts; embryonic organogenesis | Highest teratogenic vulnerability to chemical and biological agents; concentration impacts from morning sickness; worker may not yet have notified |
| Second trimester (weeks 14–27) | Abdominal expansion, balance changes beginning, increased blood volume | Workstation fit deterioration; manual handling capacity reducing; sustained chemical sensitivity |
| Third trimester (weeks 28–40) | Significant mobility reduction, increased DVT risk, fatigue, Braxton Hicks contractions | Egress and emergency response capacity reduced; prolonged standing or sitting both problematic; potential pre-eclampsia screening relevant |
| Postnatal/breastfeeding | Recovery from birth (vaginal or caesarean), pelvic floor weakness, lactation | Manual handling capacity reduced post-caesarean; breastmilk transfer of certain chemicals; need for expressing facilities and breaks |
The first-trimester problem is the structural one — most of the highest-risk exposures occur before notification, which is why the proactive generic assessment for all women of childbearing age cannot be skipped without leaving an unmanaged hazard window in the system.
What Should a Pregnancy Risk Assessment Template Include?
A well-structured template is a scaffold for the conversation, not a substitute for it. The sections below describe the essential information architecture — any template a practitioner downloads or designs in-house should contain these components, and any that omits them is structurally inadequate regardless of how polished the formatting looks.
- Section A — Worker and assessment details. Worker name, role, location, line manager, expected due date or birth date, date of written notification, assessor name and role, assessment date.
- Section B — General arrangements. Rest facility location and access, antenatal appointment process and time-off arrangements, expressing/breastfeeding facility (if applicable), communication plan during maternity leave, named keep-in-touch contact.
- Section C — Hazard identification table. A row per significant hazard, with columns for: hazard description, who is at risk (mother, child, both), existing controls, residual risk rating, additional controls required, responsible person, target completion date, and review date.
- Section D — Return-to-work assessment (added on return). Breastfeeding status, post-birth physical considerations, any medical recommendations from GP or midwife, adjusted controls.
- Section E — Sign-off and review schedule. Worker signature acknowledging receipt and opportunity to comment, line manager signature, date of next scheduled review, distribution list.
The most common template failure I see is the pre-populated generic hazard list — a single roster of office-style hazards applied unchanged to laboratory, warehouse, healthcare, or field-based roles. The hazard table should be opened blank and built from the worker’s actual role; pre-populated lists encourage assessors to tick through hazards that do not apply and miss hazards that do.
Employer Obligations for Rest, Welfare, and Breastfeeding Facilities
Regulation 25 of the Workplace (Health, Safety and Welfare) Regulations 1992 requires UK employers to provide suitable rest facilities for pregnant and breastfeeding workers. Suitable means more than a chair in a corner of the open-plan office. The facility should be private, comfortable, near toilet facilities, and accessible without prior booking. Toilets themselves are explicitly inadequate as rest facilities — the regulation makes this distinction directly.
For breastfeeding workers, the facility must additionally support expressing breastmilk: a private, lockable space with seating, access to a power supply, and a means of safely refrigerating expressed milk. Sites that nominally have such a room but require it to be booked through facilities a week in advance, or that share it with prayer or first-aid functions, are non-compliant in practice even if compliant on paper.
The US PUMP for Nursing Mothers Act establishes parallel obligations for break time and a private, non-bathroom space for expressing milk for up to one year after a child’s birth. ILO Convention No. 183 Article 10 goes further, requiring that breastfeeding breaks be counted as paid working time in ratifying states.
The frequently non-compliant detail across all three regimes is the same: a room exists, but the practical access is so constrained that the worker chooses not to use it, expresses less frequently than her body needs, and either reduces her milk supply or cuts breastfeeding short. The point of the facility is not its existence; it is the worker’s reliable, dignified use of it.
What Happens If the Risk Cannot Be Removed? Alternative Work and Paid Suspension
When the assessment identifies a significant residual risk that adjustments cannot address, the legal pathway is the three-step hierarchy outlined earlier. The substantive content of each step deserves more direct attention because this is the section employers most often handle wrongly — and the section that increasingly drives Employment Tribunal claims.
Suitable alternative work means work the worker can reasonably be expected to do, on the same terms, at the same pay, at a comparable location, with similar status and progression prospects. A senior laboratory analyst placed in a generic admin pool is not on suitable alternative work. The shift from pipetting cytotoxic agents to keying expense reports may eliminate the chemical hazard, but it changes the role’s character so fundamentally that it usually fails the suitability test.
Paid suspension under Section 67 of the Employment Rights Act 1996 is a last resort. It must be on full normal pay — not statutory sick pay, not statutory maternity pay, not a reduced rate. The worker remains employed and remains in continuous service. Crucially, paid suspension is not maternity leave. Conflating the two is one of the most damaging managerial errors. Forcing or pressuring a worker to start maternity leave early because the employer has identified a risk it cannot or will not control may itself constitute pregnancy discrimination under the Equality Act 2010 and unlawful dismissal under associated case law.
The UK Employment Rights Act 2025 enhanced dismissal protections, expected to come into force in 2027 (Acas, 2025), will sharpen the consequences of mishandling this pathway. A worker dismissed during the protected period — including return-from-maternity-leave dismissals — will be presumed to have been dismissed unlawfully unless the employer can demonstrate otherwise. The risk assessment, the documented control hierarchy, the offer letter for any alternative role, and the suspension paperwork all become primary evidence.
Common Mistakes in New and Expectant Mothers Risk Assessments
Reviewing the pattern across published Employment Tribunal decisions, EHRC research findings, and HSE guidance updates, the same failures reappear:
- No assessment after notification. The worker emails her line manager on 3 March; six weeks later there is no documented assessment. This is the simplest and most common breach, and the EHRC’s pregnancy discrimination research repeatedly identifies it as a starting point for downstream detriment.
- Generic template applied unchanged. The same office-worker template used for a delivery driver, a theatre nurse, and a research chemist. The hazards do not transfer; the template’s apparent completeness conceals the gap.
- One-and-done. Initial assessment completed at week 9, never reviewed, and the worker is still on the original controls at week 36 with markedly different physical capacity.
- Hierarchy collapsed. Manager skips Action 1 and Action 2 and proposes “early maternity leave” or unpaid time off. This converts a manageable adjustment problem into a discrimination claim.
- Confusing paid suspension with maternity leave. As above, but documented in writing, which is harder to walk back.
- Ignoring breastfeeding return. The return-to-work assessment is omitted entirely, expressing facilities are unavailable in practice, and the worker either weans early or leaves the job.
- Excluding the worker. The assessment is completed by the manager alone, presented for signature, and treated as a formality. The worker’s role-specific knowledge is missed entirely.
- Skipping the proactive generic assessment. No assessment of risks to women of childbearing age until someone announces a pregnancy. The first-trimester teratogenic window has already closed by then.
The most insidious failure underlying several of the above is treating the risk assessment as a liability document — written defensively to protect the employer from claims — rather than as an operational tool to protect the worker. Defensive assessments record hazards thoroughly but engage shallowly with whether the controls are actually working for the individual. They tend to read well and protect badly.

Frequently Asked Questions
What This Guide Comes Down To
A defensible risk assessment for a new or expectant mother is built from four operational decisions, not from a template. First, run the generic assessment for all women of childbearing age before anyone announces a pregnancy — that is where the first-trimester window is actually managed. Second, treat the individual assessment as a structured conversation with the worker, not a document the manager completes alone. Third, follow the legal hierarchy — adjust, then reassign, then suspend on full pay — without collapsing it into one shortcut decision. Fourth, schedule the next review before closing the current one.
For UK employers, the timing of these disciplines matters more in 2026 than it did before. The Employment Rights Act 2025 enhanced dismissal protections (Acas, 2025), expected to take effect in 2027, will make the contemporaneously documented risk assessment the central evidence in any contested dismissal during the protected period. Multinational employers carrying obligations across the EU’s prescriptive prohibition model and the US’s accommodation-based model should default to the stricter standard — both legally and ethically, that is the operationally defensible position.
The 54,000 mothers a year (BIS/EHRC, 2016) pushed out of work through poor treatment, and the one in twenty-five (BIS/EHRC, 2016) who left specifically because health and safety risks were not addressed, did not lose their jobs to a missing form. They lost them to risk assessments that were either never written, written once and abandoned, or written defensively for the employer rather than honestly for the worker. The job of the practitioner conducting a new and expectant mothers risk assessment is to make sure the document does what it was designed to do.