

TL;DR — Key Numbers
- 50 µg/m³ — OSHA’s permissible exposure limit for respirable crystalline silica across construction and general industry (29 CFR 1926.1153 / 1910.1053), now matched by MSHA’s April 2024 final rule for all miners.
- 25 µg/m³ — The ACGIH TLV (adopted 2006), the most protective widely cited occupational benchmark, and also the OSHA action level that triggers monitoring and medical surveillance obligations.
- 296 confirmed silicosis cases in California alone between 2019 and 2024, with 82% linked to engineered stone fabrication (California Department of Public Health / AJPH, 2025). One in four of those workers was referred for lung transplant evaluation.
- 12,900+ deaths annually from silicosis worldwide, with approximately 230 million people exposed to crystalline silica globally (Global Burden of Disease Study 2021, published 2024).
Silica dust exposure occurs when workers cut, drill, grind, or crush materials containing crystalline silica, generating respirable particles that cause irreversible lung disease including silicosis, lung cancer, and COPD. Occupational exposure limits range from 25 µg/m³ (ACGIH TLV) to 100 µg/m³ (UK WEL), with OSHA setting its PEL at 50 µg/m³. Employers must implement engineering controls, exposure monitoring, and medical surveillance to protect workers.
Globally, more than 12,900 people die from silicosis every year, and approximately 230 million are exposed to crystalline silica in occupational settings (Global Burden of Disease Study 2021, published 2024). Behind that number is a disease mechanism that has been understood for over a century — inhaled silica particles lodge deep in lung tissue and trigger irreversible fibrotic scarring — yet silica-related fatalities and diagnoses continue to climb, driven by new exposure sources and persistent control failures across industries.
The urgency sharpened dramatically between 2023 and 2025. Australia enacted the world’s first national ban on engineered stone. OSHA launched a focused inspection initiative targeting fabrication shops and found exposure levels up to six times the permissible limit. MSHA issued a final rule halving the mining sector’s silica PEL. This article covers the full risk picture — what respirable crystalline silica is, how it damages health, where the exposure limits stand across jurisdictions, and which controls actually reduce exposure at source rather than shifting the burden to the worker.
What Is Respirable Crystalline Silica?
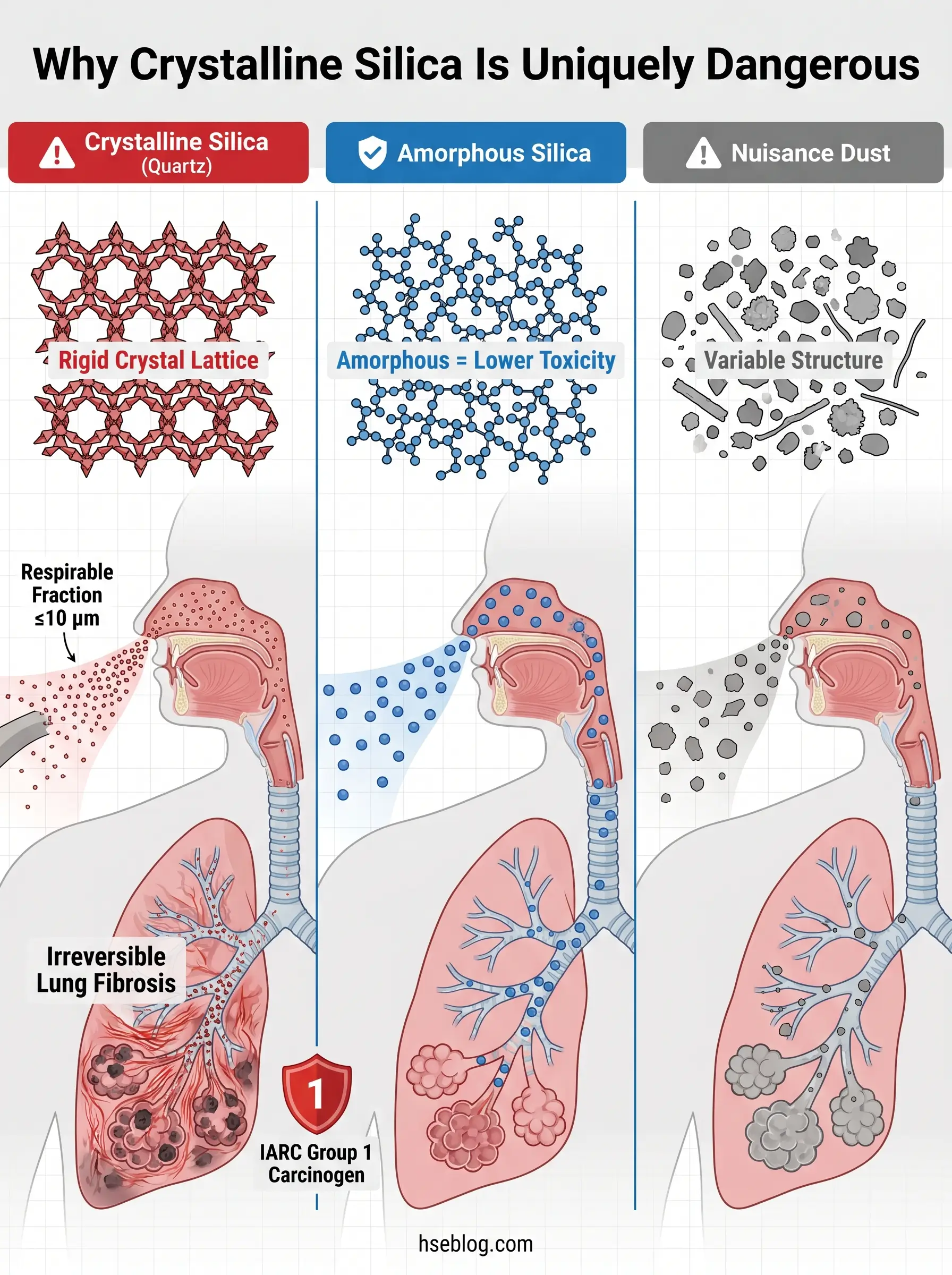
Crystalline silica is silicon dioxide (SiO₂) arranged in a rigid, repeating crystal lattice. Quartz — the most common form — makes up a significant fraction of the earth’s crust and is present in concrete, sandstone, granite, morite, brick, and dozens of manufactured products. Cristobalite and tridymite are less common crystalline forms encountered in high-temperature industrial processes.
The hazard does not come from handling silica-containing materials intact. It emerges when those materials are mechanically disturbed — cut, drilled, ground, crushed, or blasted — generating airborne dust. The respirable fraction, particles 10 micrometers (µm) or smaller, is small enough to bypass the nose and upper airways and penetrate deep into the gas-exchange region of the lungs. The International Agency for Research on Cancer (IARC) classifies respirable crystalline silica from occupational sources (quartz and cristobalite) as a Group 1 carcinogen — confirmed to cause cancer in humans.
Approximately 2.3 million workers in the United States alone face occupational silica exposure, with construction accounting for the largest share (OSHA/NIOSH, cited through 2024–2025).
A critical misconception undermines dust-control compliance on nearly every site where I have reviewed silica management programs: the assumption that visible dust equals dangerous dust. The most hazardous silica exposure episodes often occur when the air appears relatively clear. Respirable particles — the ones that penetrate the deepest lung tissue — are invisible to the naked eye. If workers and supervisors judge exposure by what they can see, they will consistently underestimate the risk.
| Feature | Crystalline Silica (Quartz) | Amorphous Silica |
|---|---|---|
| Crystal structure | Ordered, rigid lattice | Disordered, non-crystalline |
| Common sources | Concrete, sandstone, granite, brick, mortar | Diatomaceous earth, silica gel, glass |
| IARC classification | Group 1 — carcinogenic to humans | Group 3 — not classifiable |
| Fibrotic potential | High — causes silicosis | Low — generally lower toxicity |
| Regulatory OEL | Strictly regulated (50 µg/m³ OSHA PEL) | Higher limits; nuisance-dust thresholds often apply |
Health Hazards of Silica Dust Exposure
The toxicological mechanism is straightforward and unforgiving. When respirable crystalline silica particles reach the alveoli, macrophages attempt to engulf them. The rigid crystal structure resists breakdown, the macrophages die, and the repeated cycle of failed clearance triggers chronic inflammation and progressive fibrotic scarring. Once established, silicosis is irreversible and incurable — no treatment reverses the fibrosis.
Silicosis presents in three clinical forms, distinguished by exposure intensity and latency period. Chronic silicosis develops after 10 to 20 or more years of lower-level cumulative exposure and is the most common form. Accelerated silicosis appears within 5 to 10 years following heavier exposure. Acute silicosis — the rarest and most rapidly fatal form — can develop within weeks to months after massive uncontrolled exposure, such as enclosed dry sandblasting without respiratory protection.
The disease spectrum extends well beyond silicosis itself. Respirable crystalline silica exposure increases the risk of lung cancer in a dose-dependent relationship across all major histologic types. Chronic obstructive pulmonary disease, chronic bronchitis, and emphysema are all associated with cumulative silica inhalation. Evidence links silica exposure to kidney disease and several autoimmune conditions including rheumatoid arthritis, systemic lupus erythematosus, and scleroderma. Silica also impairs alveolar macrophage function, increasing susceptibility to tuberculosis — a complication with significant implications in regions where TB remains endemic.
Watch For: Silicosis can develop and progress after exposure has ceased. Workers who left silica-exposed jobs years ago may still present with new or worsening disease. This latency characteristic means occupational health surveillance must extend beyond the active employment period.
The Engineered Stone Silicosis Crisis
The defining occupational health story in silica exposure over the past five years is the global surge in accelerated silicosis cases among engineered stone countertop fabricators. Engineered stone — manufactured quartz composite used for kitchen and bathroom countertops — can contain up to 90% crystalline silica, substantially more than natural stone such as granite.
The crisis has driven regulatory responses without modern precedent. Australia banned the manufacture, supply, processing, and installation of engineered stone effective 1 July 2024, with an import prohibition from 1 January 2025 — the first national prohibition of engineered stone anywhere in the world. In California, state surveillance identified 296 confirmed silicosis cases between 2019 and 2024, of which 243 (82%) were associated with engineered stone fabrication. Twenty-five percent of those engineered stone cases were referred for lung transplant evaluation, and 12% received transplants (California Department of Public Health / American Journal of Public Health, 2025).
OSHA launched a focused inspection initiative targeting engineered stone fabrication in September 2023. By May 2025, that initiative had conducted 371 inspections with 574 silica air samples; 117 of those samples exceeded the PEL (OSHA Office of Health Enforcement, presented at AIHA Connect, May 2025).
What makes this crisis operationally distinct from historical silicosis patterns is the compressed timeline. Accelerated silicosis is presenting in young fabrication workers after just 5 to 7 years of exposure — a drastically shorter latency than the decades historically associated with chronic silicosis in mining and construction. This compressed timeline is forcing occupational health physicians to rethink screening frequency and has directly influenced regulatory decisions, including Cal/OSHA’s adoption of a permanent standard for engineered stone work in December 2024 mandating continuous water flow, banning dry sweeping, and requiring powered air-purifying respirators for high-exposure tasks.

Silica Dust Exposure Limits: A Multi-Jurisdictional Comparison
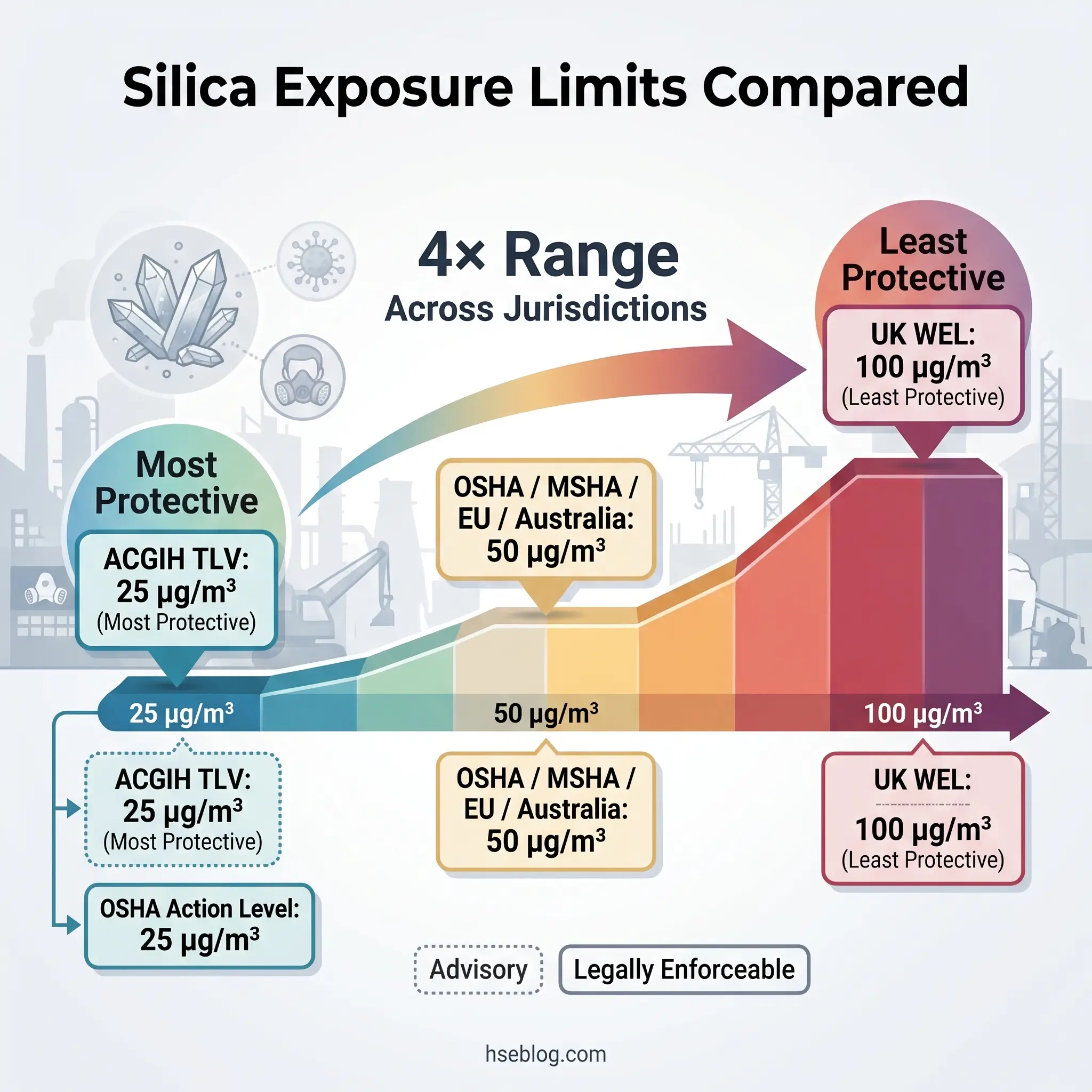
No other occupational hazard demonstrates the regulatory fragmentation problem quite like crystalline silica. Depending on the jurisdiction, the enforceable exposure limit for the same substance ranges from 25 µg/m³ to 100 µg/m³ — a fourfold difference. For multinational employers or HSE professionals working across borders, understanding which number applies and which one should govern operational decisions is essential.
| Jurisdiction | Body | Limit (8-hr TWA) | Legal Status | Year Adopted/Revised |
|---|---|---|---|---|
| US — Construction & General Industry | OSHA | 50 µg/m³ | Enforceable PEL | 2016 (effective 2017/2018) |
| US — Mining | MSHA | 50 µg/m³ | Enforceable PEL | 2024 (MNM compliance April 2026, subject to litigation) |
| US — Action Level | OSHA/MSHA | 25 µg/m³ | Triggers monitoring & medical surveillance | 2016 / 2024 |
| US — Recommended | NIOSH | 50 µg/m³ | Advisory REL (up to 10-hr day) | — |
| International — Advisory | ACGIH | 25 µg/m³ | TLV — not legally binding | 2006 |
| United Kingdom | HSE | 100 µg/m³ (0.1 mg/m³) | Enforceable WEL under COSHH/EH40 | Updated 2020 |
| European Union | EU Commission | 50 µg/m³ (0.05 mg/m³) | BOEL under Directive 2017/2398 | 2017 (transitional 0.1 mg/m³ for some sectors until Dec 2023) |
| Australia | Safe Work Australia | 50 µg/m³ (0.05 mg/m³) | Enforceable WES | — |
The OSHA PEL and MSHA PEL are now aligned at 50 µg/m³ following MSHA’s April 2024 final rule, which halved the previous PEL for metal/non-metal (MNM) mines from 100 µg/m³. Compliance for MNM mines is set for April 8, 2026, though this deadline is subject to ongoing litigation and a judicial stay issued in early April 2025. The ACGIH TLV of 25 µg/m³, adopted in 2006, remains the most protective widely cited benchmark.
A failure mode I consistently observe across exposure monitoring programs: organizations treat the PEL as a performance target rather than a regulatory ceiling. Every jurisdiction’s silica standard requires reducing exposure as low as reasonably practicable (ALARP under UK and Australian frameworks) or to the lowest feasible level (US). An air sample returning 48 µg/m³ is technically below the OSHA PEL, but it represents a control failure, not a control success. The intent of every standard is continued reduction, not compliance at the margin.
Jurisdiction Note: The UK’s WEL of 100 µg/m³ is the least protective major-jurisdiction limit currently in force — double the OSHA PEL and four times the ACGIH TLV. HSE UK has indicated it keeps the limit under review, but as of 2025, no revision has been proposed. UK-based employers operating to the COSHH principle of “as low as reasonably practicable” should target well below the WEL regardless of its numerical value.
Why Exposure Limits Differ and Which One to Follow
The disparity exists because regulatory bodies use different criteria to set limits. Health-based recommendations like the ACGIH TLV are derived from the best available toxicological and epidemiological evidence about the threshold at which disease risk becomes unacceptable. Legally enforceable limits like the OSHA PEL factor in economic and technical feasibility — what industry can reasonably achieve — which typically results in a higher number.
The practical guidance for HSE professionals managing silica exposure across jurisdictions is straightforward. Apply the most protective limit your jurisdiction allows, and in multinational operations, default to the ACGIH TLV of 25 µg/m³ as the reference benchmark. Where the enforceable limit is higher, treat it as the legal floor, not the operational target.
The MSHA 2024 rule illustrates how limits evolve. For decades, MNM miners worked under a PEL of 100 µg/m³ — double what OSHA required for construction and general industry workers exposed to the same substance. The April 2024 final rule closed that gap. Employers who had already adopted the OSHA PEL or the ACGIH TLV as their internal standard faced minimal compliance disruption. Those who had relied on the higher MSHA limit faced significant operational changes.
Who Is at Risk? High-Exposure Industries and Tasks
Silica exposure is not confined to one sector. It spans construction, manufacturing, mining, maritime, and — increasingly — small fabrication shops that process engineered stone countertops. The approximately 2.3 million exposed workers in the US alone (OSHA/NIOSH) work across all of these industries, and the exposure profile varies dramatically by task.
Construction generates the largest exposed population. The highest-risk tasks include concrete cutting and sawing, mortar grinding, masonry work (cutting brick and block), tunnel boring, road milling, abrasive blasting with silica-containing media, and drywall finishing with joint compound. OSHA’s Table 1 under 29 CFR 1926.1153 lists 18 specific construction tasks precisely because the variety and frequency of silica-generating operations in this sector demand task-level control specifications.
Manufacturing presents concentrated exposures in glass production, ceramics and pottery, foundry operations (mold-making and shakeout), concrete products manufacturing, and brick production. These operations typically occur in enclosed or semi-enclosed environments where airborne concentrations can build rapidly without adequate ventilation.
Mining and quarrying exposes workers during drilling, blasting, crushing, and material transport. Haul-road dust in open-pit operations is often overlooked as a silica source. MSHA’s April 2024 final rule directly addresses this sector’s historically higher permissible limits.
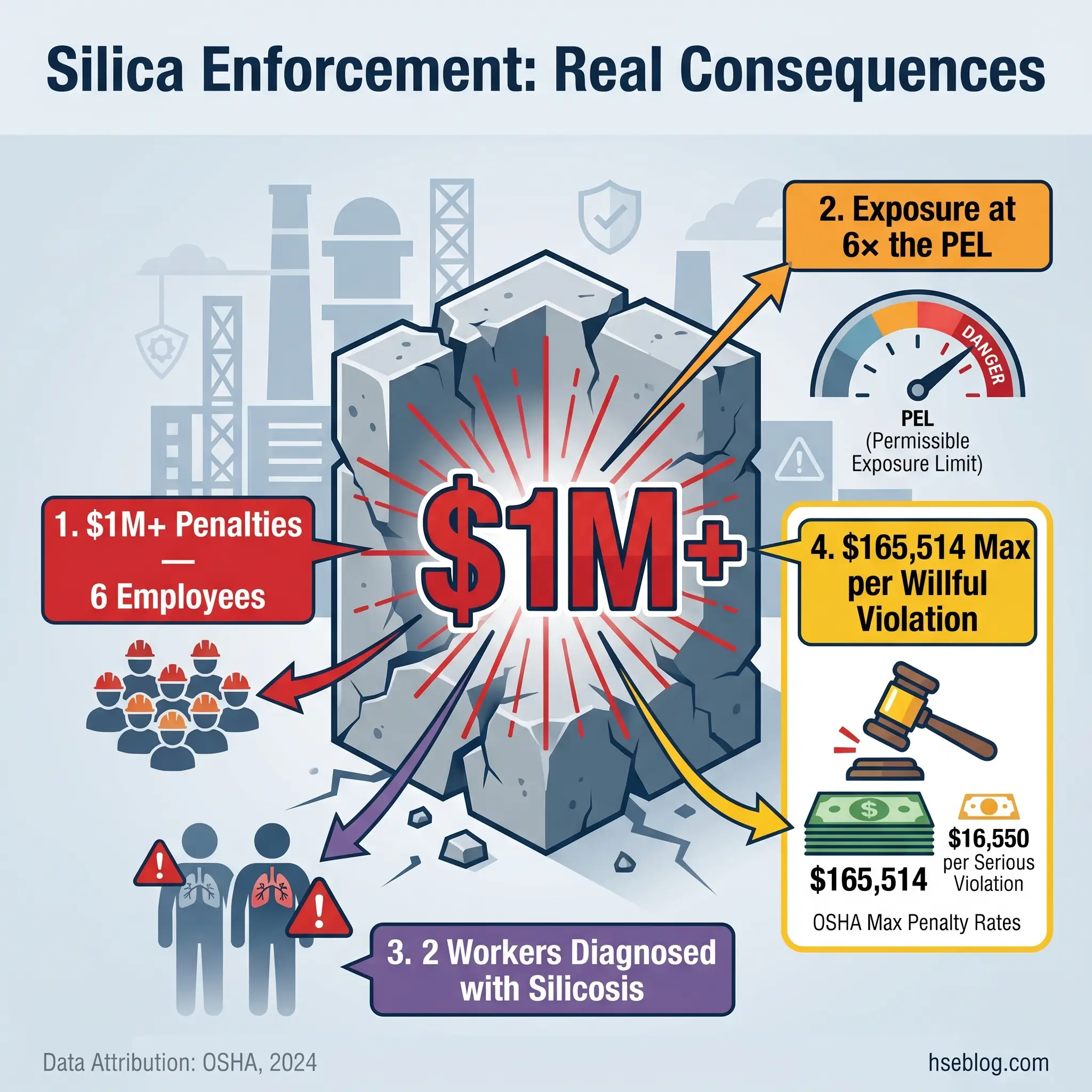
Engineered stone fabrication represents the highest-concentration silica source currently driving regulatory enforcement worldwide. Cutting, grinding, and polishing engineered stone countertops generates extreme respirable silica levels because the material contains up to 90% crystalline silica. Many fabrication shops are small businesses with limited industrial hygiene infrastructure — the exact profile reflected in OSHA’s enforcement data, including the Chicago countertop manufacturer cited in August 2024 with over $1 million in penalties after silica levels were found at nearly six times the PEL at a six-employee facility, where two workers were diagnosed with silicosis requiring lung transplant evaluation (OSHA, 2024).
Hydraulic fracturing operations generate silica exposure during sand handling — transporting, transferring, and blending silica sand used as proppant. Maritime abrasive blasting in enclosed spaces is another high-exposure scenario.
Field Test: Exposure often spikes not during the primary silica-generating task, but during secondary activities — dry sweeping after grinding, cleanup without HEPA vacuum, or removing contaminated PPE in the breathing zone. These transition moments are consistently under-controlled and rarely captured by task-based exposure assessments that focus only on the main operation.
How Is Silica Dust Exposure Measured?
Two primary compliance pathways exist for determining whether workers are over-exposed to respirable crystalline silica, and the distinction between them has significant practical consequences.
Personal air sampling is the standard exposure assessment method across all jurisdictions. A cyclone-type sampler is placed in the worker’s breathing zone and collects respirable dust over the full work shift. The sample is then sent to an accredited laboratory for analysis by X-ray diffraction (XRD, per NIOSH Method 7500) or infrared spectrometry (NIOSH Method 7602, OSHA ID-142). The result — a time-weighted average concentration in µg/m³ — is compared against the applicable PEL, WEL, or WES. Under OSHA’s general industry standard (29 CFR 1910.1053), this sampling-based exposure assessment is the only compliance pathway.
OSHA’s Table 1 alternative applies only to construction under 29 CFR 1926.1153. Table 1 lists 18 specific construction tasks alongside the required engineering controls, work practices, and respiratory protection for each. Employers who implement the specified controls exactly as listed are deemed compliant with the PEL without conducting air sampling.
The Table 1 route is attractive for its simplicity, but it becomes a compliance trap when employers treat it as a static checklist rather than a dynamic control verification. A water-suppression system specified in Table 1 that runs dry mid-shift provides zero dust control regardless of what the table says. The obligation is not to list the control — it is to maintain the control throughout the task.
Under both OSHA standards, the action level of 25 µg/m³ is the critical threshold. When exposure at or above this level occurs for 30 or more days per year, the employer must initiate periodic exposure monitoring and medical surveillance. Additional monitoring is required whenever changes in production, process, or controls may increase exposure.
Real-time direct-reading instruments are emerging as supplementary monitoring tools. These devices measure total respirable particulate in near-real-time and provide early warning of exposure spikes. They cannot, however, differentiate crystalline silica from other respirable particles and do not substitute for gravimetric laboratory analysis in any jurisdiction’s compliance framework.
Controlling Silica Dust Exposure: The Hierarchy of Controls Applied
The most common control-hierarchy failure in silica management is the reflex that reaches for respirators first. Distributing half-mask respirators without investing in engineering controls that reduce dust at source inverts the hierarchy entirely and places the full protection burden on the worker — whose actual protection then depends on face-fit seal, filter maintenance, wear compliance, and clean-shaven protocols. All of these degrade in real-world conditions.
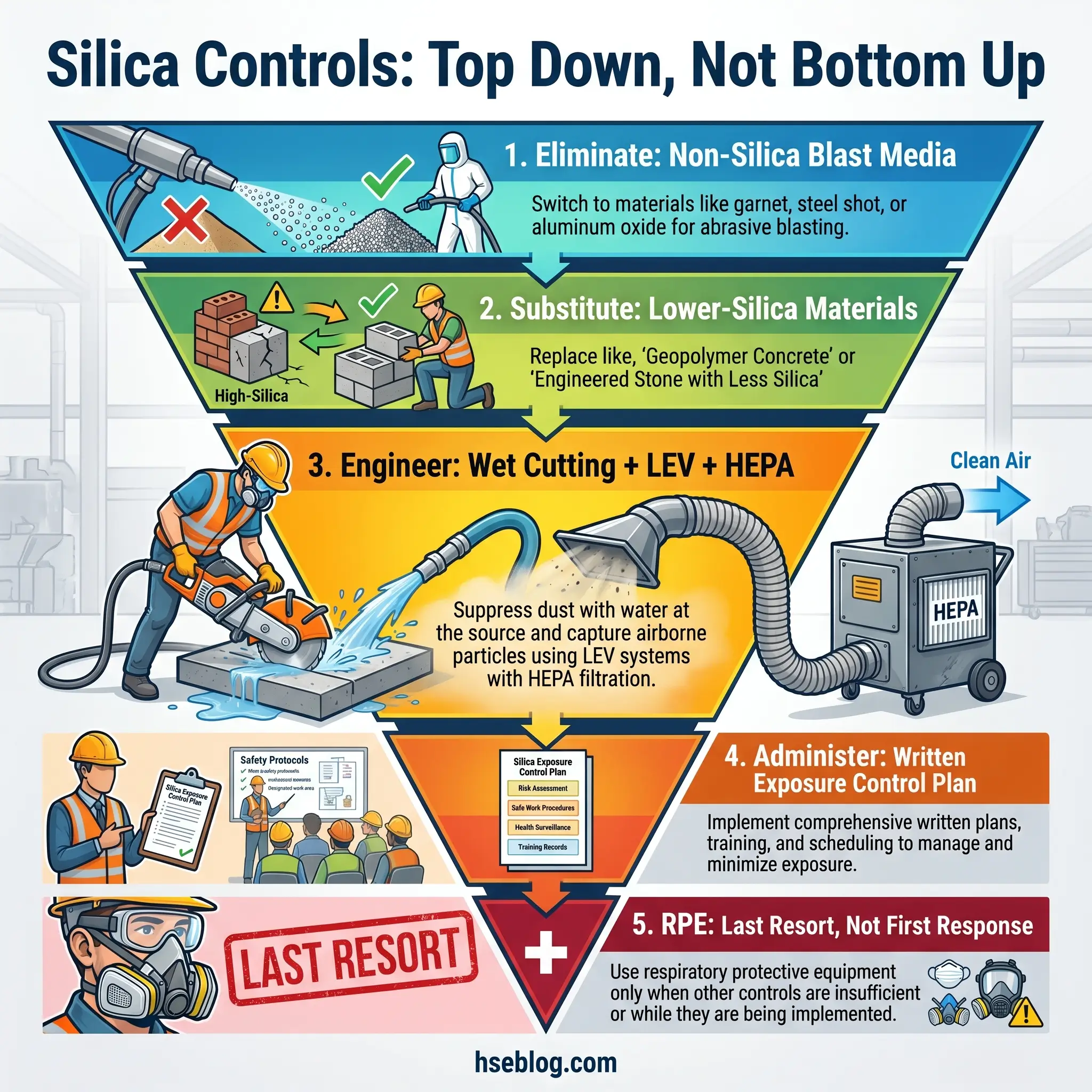
The hierarchy of controls applied to silica exposure demands working from the top down.
Elimination removes silica-containing material from the process entirely. Substituting non-silica abrasive media for sandblasting — using steel grit, garnet, or crusite instead of silica sand — eliminates the silica exposure source. Several jurisdictions now prohibit silica sand as a blasting abrasive outright.
Substitution reduces silica content rather than eliminating it. Switching from engineered stone (up to 90% silica) to porcelain or sintered stone alternatives with substantially lower silica content reduces the exposure source. Substitution decisions must be verified with material safety data — the replacement material’s silica content needs to be confirmed, not assumed.
Engineering controls are the operational backbone of silica exposure management and the layer where the most impactful reductions occur:
- Wet cutting methods — Continuous water flow at the point of dust generation suppresses airborne respirable particles during cutting, drilling, and grinding. Water must be applied at the point of contact, not sprayed generally. Intermittent wetting or wetting after dust is already airborne is far less effective.
- Local exhaust ventilation (LEV) — Capture hoods, tool-integrated dust shrouds, and vacuum attachments connected to HEPA-filtered extraction systems remove dust at the source before it enters the breathing zone.
- Enclosed operator cabs — Positive-pressure cabs with HEPA-filtered air supply protect operators of drilling rigs, crushers, and heavy equipment.
- HEPA vacuum systems — Required for housekeeping under both OSHA silica standards. Dry sweeping and compressed air blowdown are explicitly prohibited unless combined with capture ventilation.
Administrative controls supplement engineering measures but cannot replace them. A written exposure control plan is required under OSHA’s construction standard (1926.1153(g)) and general industry standard (1910.1053(f)). Worker rotation limits cumulative exposure but does not reduce airborne concentrations. Restricted access zones prevent bystander exposure. Signage and hazard communication inform workers of silica-generating areas.
Respiratory protective equipment (RPE) is the last layer. Respirator selection must be based on the measured or anticipated exposure level and the respirator’s assigned protection factor (APF). For silica exposures at or below 10 times the PEL (500 µg/m³ under OSHA), a minimum N95 filtering facepiece or half-mask with P100 filters is required. For sustained high-exposure tasks — particularly in engineered stone fabrication — powered air-purifying respirators (PAPRs) with APFs of 25 or higher provide more reliable protection. Face-fit testing is mandatory under OSHA (29 CFR 1910.134), COSHH (UK), and Safe Work Australia requirements. NIOSH’s safe work practices for silica provides detailed engineering and RPE selection guidance.
Audit Point: During site audits, test the engineering controls while the silica-generating task is running. Verify water flow rates, check LEV capture velocities at the hood face, inspect HEPA filters for loading, and confirm that vacuum attachments maintain seal at the tool interface. Paper documentation of controls that are not functioning during the task has zero protective value.
Written Exposure Control Plan Requirements
Both OSHA silica standards mandate a written exposure control plan. Under 29 CFR 1926.1153(g) for construction and 29 CFR 1910.1053(f) for general industry, the plan must describe the engineering controls, work practices, and respiratory protection measures used for each silica-generating task on site.
The plan must also describe housekeeping measures — specifying HEPA vacuum or wet methods and confirming that dry sweeping and compressed air are prohibited except with capture ventilation. OSHA requires the plan to be reviewed and updated at least annually, or whenever there is a change in production processes, equipment, or controls that could affect silica exposure levels.
Critically, the plan must be accessible. It must be available to workers, their designated representatives, and OSHA compliance officers upon request. A plan stored exclusively on a corporate server that site workers have never seen fails both the regulatory and the operational intent. Under COSHH in the UK, the equivalent obligation is the COSHH risk assessment — which must similarly identify controls, assign responsibilities, and be reviewed regularly.
Medical Surveillance and Health Monitoring for Silica-Exposed Workers
OSHA requires medical surveillance for workers exposed at or above the action level of 25 µg/m³ for 30 or more days per year. The surveillance program includes a baseline examination (within 30 days of initial assignment or as soon as possible thereafter), with periodic examinations every three years. The examination covers a medical and work history, physical examination, chest X-ray read according to the ILO International Classification of Radiographs of Pneumoconioses, and pulmonary function testing (spirometry).
The physician provides a written medical opinion to the employer, but its content is limited by design — only fitness-for-duty determination and any recommended limitations are disclosed. Specific diagnoses and clinical findings remain between the physician and the worker, a privacy protection built into both OSHA standards.
In the UK, COSHH requires health surveillance for employees significantly exposed to respirable crystalline silica. This typically includes a respiratory health questionnaire and lung function testing. Australia’s framework requires health monitoring before a worker begins silica-exposed work, with periodic monitoring at least every three years — or annually for workers in high-risk roles such as engineered stone fabrication.
The sensitivity gap between screening methods is a critical practitioner concern. Standard chest X-ray, while sufficient for regulatory compliance in most jurisdictions, has limited sensitivity for detecting early silicotic nodules. By the time radiographic opacities reach ILO category 1/1 on chest X-ray, the disease has already progressed substantially. High-resolution computed tomography (HRCT) is significantly more sensitive for identifying early-stage nodular disease. Cal/OSHA’s 2024/2025 permanent standard for engineered stone workers now requires HRCT rather than chest X-ray — an acknowledgment that the regulatory minimum screening tool may be insufficient for the highest-risk populations.
Occupational health programs that rely solely on the minimum regulatory screening schedule are likely to miss early-stage disease in high-exposure populations. The judgment call for HSE professionals managing silica-exposed workforces is whether to adopt more frequent screening and more sensitive imaging than the regulation requires — particularly for workers in fabrication, mining, and other sectors with sustained high-exposure potential.
What Are the Penalties for Non-Compliance with Silica Standards?
Enforcement actions in silica are increasingly pursued as willful violations rather than serious violations, reflecting a regulatory posture shift. Regulators in multiple jurisdictions now take the view that comprehensive guidance on silica hazards and controls has been available for years, and continued non-compliance constitutes a deliberate choice rather than an information gap.
Under OSHA’s penalty structure (as of January 2025), a serious violation carries a maximum penalty of $16,550. A willful or repeated violation can reach $165,514 per instance. OSHA’s instance-by-instance citation policy means each affected worker or each day of violation can constitute a separate penalty — a multiplier that rapidly escalates the total.
The August 2024 enforcement action against a Chicago countertop manufacturer illustrates the stakes concretely. OSHA cited the six-employee facility with over $1 million in combined penalties after inspection found silica exposure levels at nearly six times the PEL. Two workers at the facility had been diagnosed with silicosis, one requiring evaluation for a double-lung transplant (OSHA, 2024). The citations included willful violations — the highest classification, indicating the employer either knew of the hazard and failed to act or showed reckless disregard for worker safety.
HSE UK enforces silica compliance through COSHH, with no statutory maximum on fines and the possibility of imprisonment for serious breaches. HSE actively inspects stone fabrication and construction operations for silica compliance. In Australia, penalties under the Work Health and Safety Act extend to both the PCBU (person conducting a business or undertaking) and individual officers, and the engineered stone ban carries separate offences for non-compliance.
The Fix That Works: The organizations that avoid enforcement exposure share one characteristic — they treat the ACGIH TLV of 25 µg/m³ as their operational target, not the PEL. When your internal standard is already at the most protective benchmark, regulatory changes like the MSHA 2024 rule require operational adjustment rather than operational overhaul.
Frequently Asked Questions
Conclusion
Every jurisdiction covered in this article — OSHA, HSE UK, the EU, Australia, MSHA — has strengthened its stance on silica exposure within the past two years. Australia banned the highest-risk source material outright. MSHA halved its PEL. OSHA intensified enforcement in the sector generating the most alarming disease data. The regulatory trajectory is unambiguous: exposure limits will tighten further, enforcement will expand, and the organizations that treat current limits as aspirational targets rather than operational baselines will face compounding compliance, legal, and human costs.
The engineered stone silicosis crisis is not an anomaly — it is a case study in what happens when a high-silica material enters an industry sector with inadequate industrial hygiene infrastructure. Young workers developing irreversible lung disease after five to seven years of exposure, needing lung transplants in their twenties and thirties, represents a failure that no penalty structure can undo. The controls to prevent this — wet cutting, local exhaust ventilation, exposure monitoring, medical surveillance — are not novel technologies. They are established, proven, and required by law in every major jurisdiction.
The judgment call for HSE professionals is not whether silica controls are necessary. It is whether the controls you have in place are actually functioning — not on paper, not in the exposure control plan stored on a server, but at the point where the blade meets the stone and the dust enters the air.