

TL;DR — Key Numbers
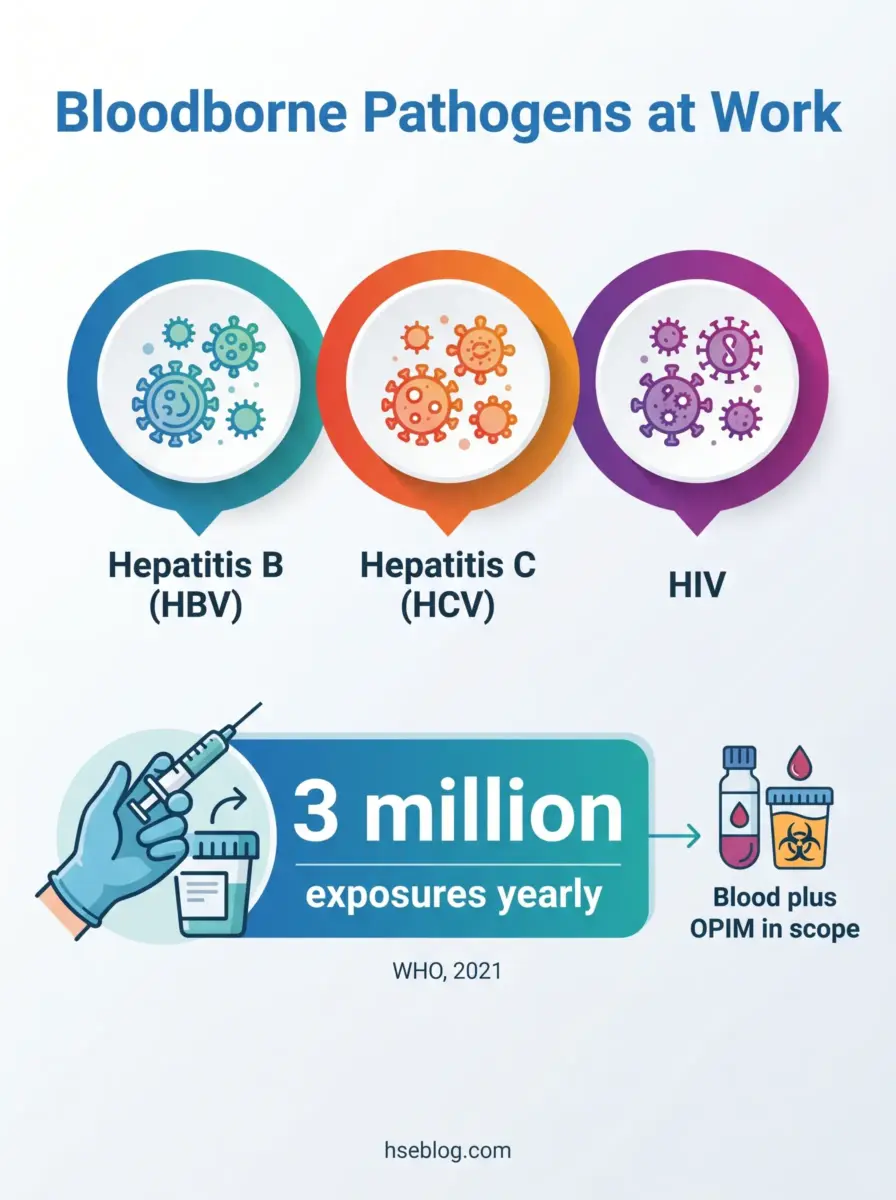
- ~3 million healthcare workers worldwide suffer percutaneous bloodborne-pathogen exposures each year, including roughly 2 million hepatitis B and 170,000 HIV exposures (WHO, cited in BMC Health Services Research, 2021).
- ~385,000 sharps injuries occur annually among US hospital-based staff alone (US CDC, cited in BMC Health Services Research, 2021).
- 31 needlestick or sharp-object injuries were recorded per 100 average daily census across 41 reporting hospitals (EPINet, via OSHA, 2021 data).
- ~95% efficacy is typical for the hepatitis B vaccine series in healthy adults, with protection lasting at least ten years (AMA Journal of Ethics, citing CDC, 2005).
Bloodborne pathogens are infectious microorganisms in human blood — primarily hepatitis B (HBV), hepatitis C (HCV), and HIV — that can cause serious disease. At work, they spread mainly through needlestick or sharps injuries and through blood or infectious fluids contacting the eyes, nose, mouth, or non-intact skin. Intact skin is an effective barrier.
A bloodborne pathogen exposure is one of the few occupational hazards where the wrong response in the first hour can change a worker’s life. The biology is unforgiving, but the controls are well understood and legally mandated. What follows maps the hazard, the four layers of control, the exposure-response sequence, and how employer duties differ across the US, UK, and EU — drawn from the regulatory text and the published surveillance record rather than from generic safety advice.
This article reflects HSE professional understanding, not clinical or legal advice. Where it touches medical management and statutory duty, those caveats appear in full at the relevant sections.
What Are Bloodborne Pathogens?
Bloodborne pathogens are infectious microorganisms carried in human blood — and in certain other body fluids — that can cause disease when they enter another person’s body. That is OSHA’s regulatory framing under 29 CFR 1910.1030 (US), and it is the definition a workplace program should be built around.
Three pathogens drive the occupational concern, but the list is deliberately non-exhaustive:
- Hepatitis B (HBV) — the most readily transmitted of the three through occupational blood contact, and the only one with a protective vaccine.
- Hepatitis C (HCV) — bloodborne, often chronic, with no vaccine and no reliable post-exposure prophylaxis.
- HIV — lower per-contact transmission efficiency than the hepatitis viruses, but severe consequence, with time-critical prophylaxis available.
Others — including syphilis, malaria, brucellosis, and West Nile virus — can also travel through blood. A program that fixes its training entirely on “the big three” misses the reasoning behind the standard, which is to treat the route as the hazard rather than any single organism.
The scope error I see most often sits one level deeper. New workers read “bloodborne” and assume it means blood, full stop — but the standard explicitly extends to other potentially infectious materials (OPIM).
OPIM under 29 CFR 1910.1030 includes:
- Specific body fluids — semen, vaginal secretions, and cerebrospinal, synovial, pleural, pericardial, peritoneal, and amniotic fluid.
- Saliva in dental procedures — not saliva generally, but saliva in the dental context.
- Any fluid visibly contaminated with blood, and any body fluid where it is impossible to distinguish between fluids.
- Unfixed human tissue or organs, and cultures or media containing these pathogens.
What is not OPIM matters just as much for right-sizing controls. Feces, urine, sweat, tears, nasal secretions, vomit, and saliva outside dental work fall outside the standard — unless they contain visible blood. You can read OSHA’s definition of blood and OPIM in full on its bloodborne pathogens hazards page, and it is worth doing so, because this is the precise point where many programs draw the line in the wrong place.
Which Workers Are at Risk of Occupational Exposure?
The at-risk population is far wider than “healthcare workers,” and treating it as a clinical-only problem is exactly how employers under-scope their programs. The governing test is whether exposure is reasonably anticipated in the course of the job — not the job title.
Clinical and laboratory roles
- Direct-care staff — nurses, phlebotomists, physicians, and dental practitioners who handle sharps and bodily fluids routinely.
- Laboratory and research technicians — handling specimens, cultures, and unfixed tissue.
Non-healthcare roles that programs routinely overlook
- First responders and EMS — uncontrolled scenes, sharps in pockets and debris, no clinical setting.
- Custodial, laundry, and waste-handling staff — handling regulated waste and contaminated linens, often the role most wrongly excluded.
- Tattoo and body-art practitioners — repeated skin penetration is the core activity, not an incidental risk.
- Corrections officers, school staff, and mortuary workers — exposure through assaults, first aid, sharps finds, or post-mortem handling.
The pattern worth naming: when an employer drafts its exposure determination too narrowly and leaves maintenance or janitorial roles off the list, those omissions are a frequent driver of citations and, worse, of unprotected sticks during waste handling. The exposure determination is supposed to be made without regard to whether PPE is worn — a detail that catches out employers who reason backward from “they wear gloves anyway.”
One clarification keeps the section honest. The risk here is strictly occupational; most community transmission of HBV, HCV, and HIV happens through routes — sexual contact, shared injection equipment — that sit entirely outside this standard’s scope.
How Are Bloodborne Pathogens Transmitted at Work?
Occupational transmission happens through two main routes, and the highest-efficiency one is percutaneous — a needlestick or sharps injury that breaches the skin. Blood or OPIM reaching a mucous membrane or non-intact skin is the second route. Intact skin, importantly, is an effective barrier.
| Route | How it happens | Relative efficiency |
|---|---|---|
| Percutaneous | Needlestick, scalpel cut, broken glass, sharps puncture | Highest occupational route |
| Mucocutaneous | Splash of blood/OPIM to eyes, nose, or mouth | Lower, but real with volume or force |
| Non-intact skin | Contact via cuts, abrasions, dermatitis, or open lesions | Lower, route-dependent |
| Intact skin | Surface contact only | Not a transmission route on its own |
Per-contact transmission risk also differs by pathogen. The well-established ranking is HBV highest, then HCV, then HIV — and I deliberately give that as a ranking rather than precise percentages, because the figures circulating online are frequently mis-cited. For any program document, the seroconversion estimates should be pulled from a current CDC or US Public Health Service primary page, not a statistics aggregator.
The timing of injuries tells you where complacency lives. A large share of sticks happen after the clinical task is finished — during recapping, disposal, or cleanup — when the device is already contaminated and attention has dropped.
That post-use window is the part most training underplays:
- Recapping a used needle reintroduces the hand into the danger zone the device was designed to remove it from.
- Reaching into an overfilled or mis-sited sharps container converts a routine disposal into a puncture.
- Cleanup and linen handling expose downstream workers who never performed the original procedure.

The Hierarchy of Controls for Bloodborne Pathogens
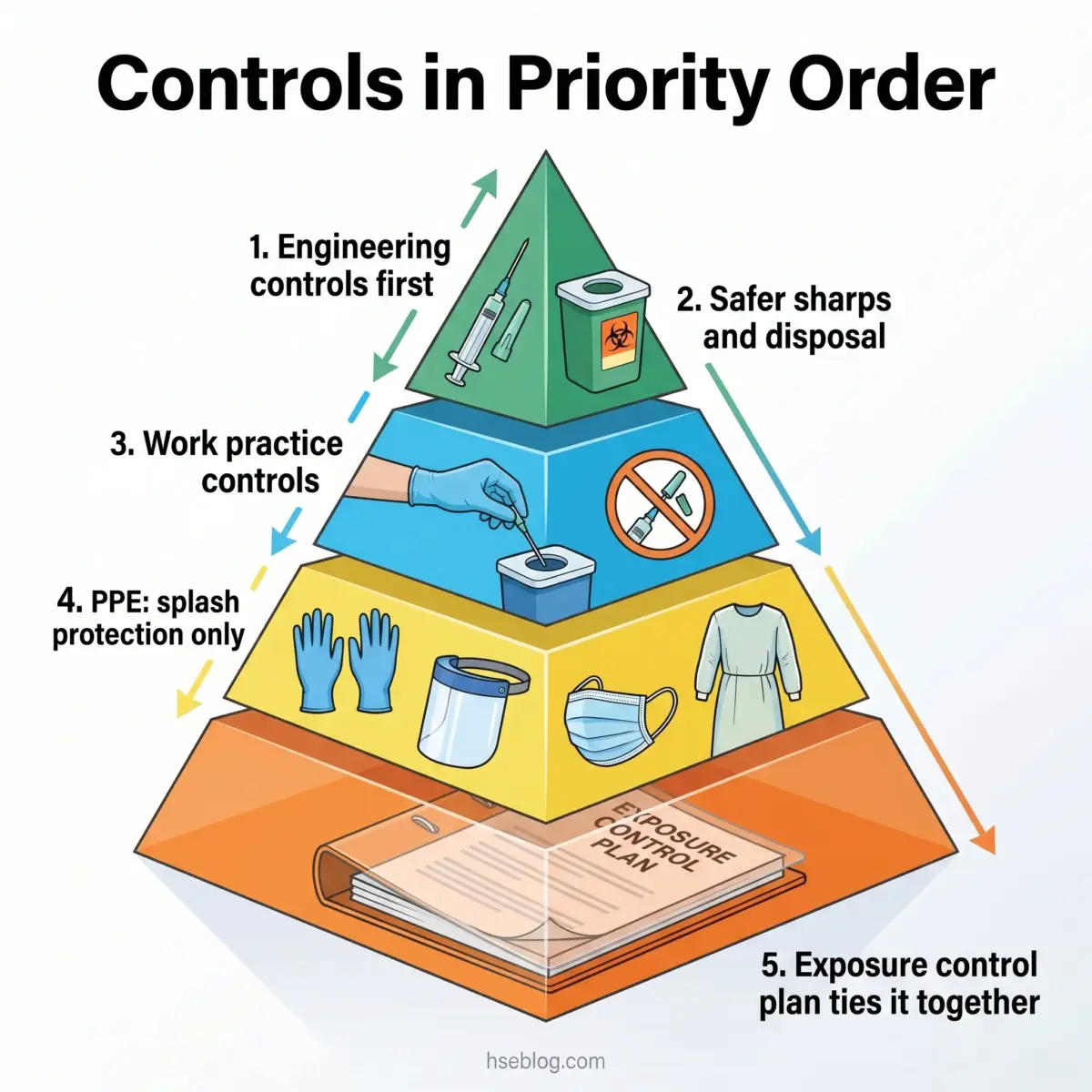
Every safety procedure for bloodborne pathogens belongs to a layered hierarchy, and the order is what competitors usually get wrong: engineering controls first, work practices next, then PPE, with the written program holding it all together. PPE is the last line of defense, not the first.
This article provides general HSE knowledge. Life-critical work involving sharps and potential bloodborne pathogen exposure must be planned and supervised by a competent person with relevant training, jurisdiction-specific authorization, and a site-specific risk assessment. The information here does not replace that. Recognized training pathways — NEBOSH, IOSH, OSHA outreach, or the regional equivalent — are the route to that competence.
Engineering Controls
These remove or isolate the hazard at the source, and under OSHA they are the primary required control, not an optional upgrade.
- Needleless systems — eliminating the sharp where the clinical task allows.
- Sharps with engineered sharps-injury protection (SESIP) — self-sheathing or retracting needles that shield the point after use.
- Blunt-tip suture needles where surgically appropriate.
- Puncture-resistant sharps containers, sited at the point of use, upright, and replaced before they overfill.
Work Practice Controls
These change how a task is performed so the residual hazard is managed:
- No recapping of used needles by hand, and no two-handed techniques.
- No eating, drinking, smoking, or applying cosmetics in areas of reasonably anticipated exposure.
- Hand hygiene immediately after glove removal and any contact.
- Safe specimen handling — leak-proof, labeled containers, no mouth pipetting.
Personal Protective Equipment (PPE)
PPE for bloodborne pathogens is splash and contact protection, and this is where a damaging conflation creeps in. Gloves, fluid-resistant gowns or aprons, face shields, and goggles protect against blood and OPIM reaching skin or mucous membranes.
What PPE for this hazard is not is respiratory protection. Bloodborne pathogens are not an airborne hazard, so an N95 respirator — the right tool for tuberculosis or aerosolized agents — is the wrong reference point here, and treating the two interchangeably signals a program that has copied language without understanding it.
Administrative Controls and the Exposure Control Plan
The written Exposure Control Plan (ECP) is the backbone that holds the other three layers together. Under 29 CFR 1910.1030 it must include the exposure determination, the methods of compliance, and evidence that front-line workers were involved in selecting safer devices — and it must be reviewed at least annually and whenever tasks change.
The dominant failure mode is treating the ECP as a one-time binder rather than a live document. When I audit a program, the tell is simple: I look for whether non-managerial staff were genuinely consulted on device selection, because that consultation is both a legal requirement and the practical difference between a safer device being adopted and the same device sitting unused in a storeroom.
Universal Precautions vs Standard Precautions
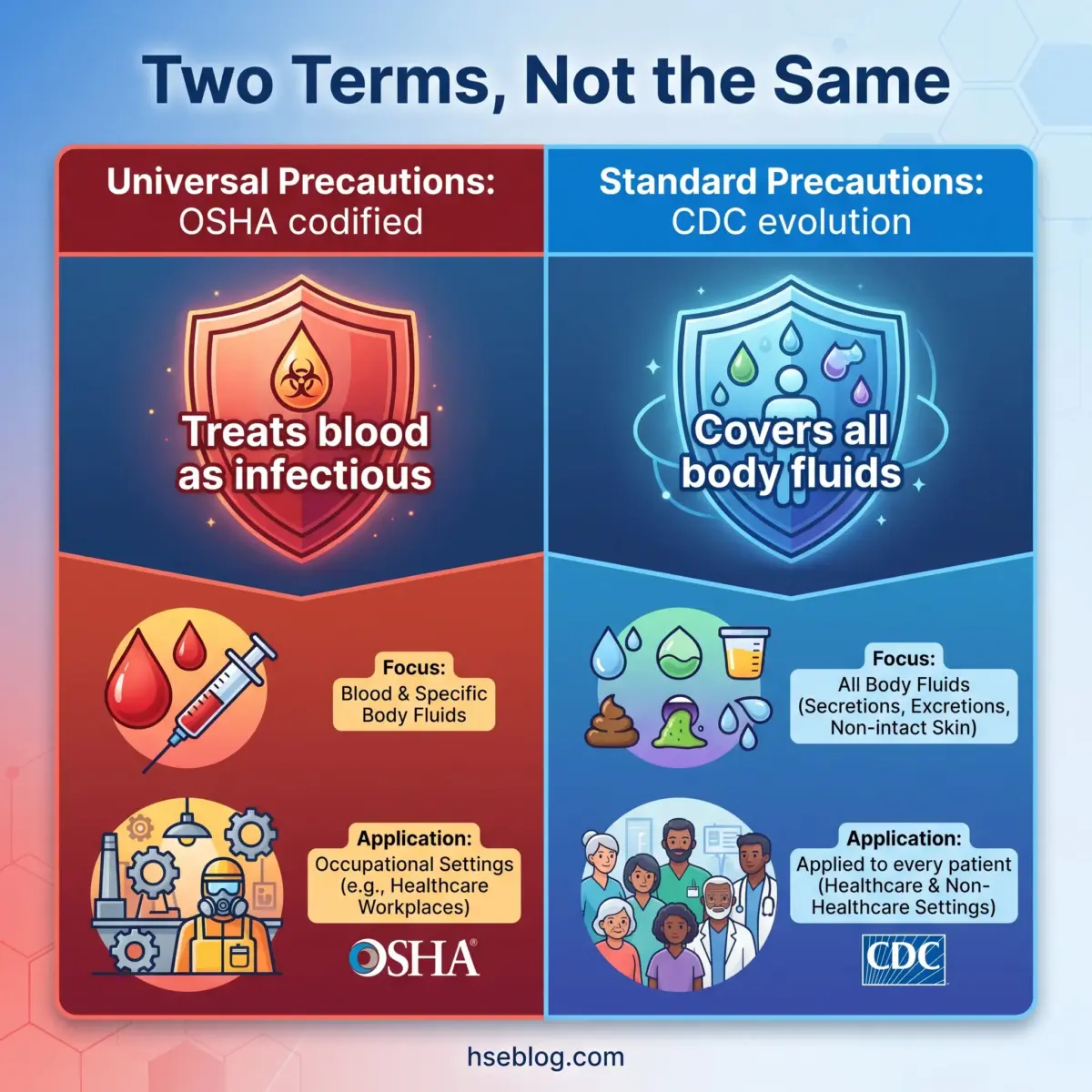
These two terms are used interchangeably on most sites, but they are not identical — and OSHA’s standard is written around Universal Precautions specifically. Getting this right is a small thing that signals whether a program understands its own legal basis.
| Universal Precautions | Standard Precautions | |
|---|---|---|
| Originating body | Codified in OSHA 1910.1030 (US) | Evolved by the CDC |
| What’s treated as infectious | All human blood and certain body fluids | All blood, body fluids, secretions, excretions (except sweat), non-intact skin, and mucous membranes |
| Scope | Bloodborne-pathogen exposure control | Broader infection control for all patient contact |
| Practical reading | The OSHA compliance baseline | The wider clinical infection-prevention framework |
The cleanest way to hold the relationship in mind: Standard Precautions absorbed Universal Precautions and added body-substance isolation, applying the combined approach to every patient regardless of known status. When you are writing or auditing an OSHA-aligned program, use “Universal Precautions” because that is the term the legal text uses; when describing day-to-day clinical infection control, “Standard Precautions” is the accurate term.
Hepatitis B Vaccination: A Required Safeguard
The employer’s duty here is specific and time-bound: under 29 CFR 1910.1030, the hepatitis B vaccine series must be offered free of charge, within 10 working days of a worker’s assignment to duties with reasonably anticipated exposure. Vaccination is the rare instance where a single control closes off one of the three primary pathogens almost entirely.
The core duties:
- No-cost offer of the full HBV vaccine series before exposure work begins.
- Right to decline in writing — but a worker who declines may opt in later at any point while still covered by the standard.
- No equivalent for HCV or HIV — no vaccine exists for either, which is why prevention and post-exposure response carry the entire defensive load for those two.
The vaccine earns its place in the program on the evidence: efficacy in healthy adults runs around 95%, with protection lasting at least ten years (AMA Journal of Ethics, citing CDC, 2005).
The quiet gap I see in otherwise compliant programs is the declination form treated as a closed door. Forms get collected at orientation, filed, and never revisited — yet the standard explicitly preserves the worker’s right to be vaccinated later, and a program that never re-offers is leaving protection on the table.
The hepatitis B vaccination and exposure-management content here is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms, immunization questions, or exposure concerns should consult an occupational physician or qualified medical professional.
What to Do After a Bloodborne Pathogen Exposure
Act immediately — the response to a bloodborne pathogen exposure is time-sensitive, and delay narrows or closes the window for effective prophylaxis. The sequence below puts physical first aid before reporting, but both must happen fast.
This section is not a substitute for medical advice. After any exposure, seek immediate occupational-health or emergency medical evaluation. Post-exposure decisions — including whether prophylaxis is needed and which regimen applies — are made by a treating clinician, not from a webpage.
Immediate steps after a needlestick or splash:
- Wash the wound with soap and running water; flood the area generously. Do not scrub harshly and do not apply caustic agents.
- Flush mucous membranes — eyes, nose, mouth — with water or sterile saline if blood or OPIM has splashed.
- Report immediately to your supervisor and occupational health, before leaving the site if at all possible.
- Enable source-patient assessment so the clinician can perform a timely risk evaluation.
- Attend the confidential medical evaluation and follow-up the employer must provide at no cost.
- Document the incident — including device, circumstances, and the post-use moment if relevant — for the employer’s records and the sharps injury log.
Why the speed matters: prophylaxis effectiveness is time-dependent, particularly for HIV, where post-exposure prophylaxis (PEP) should start as soon as possible after exposure. The clinical detail belongs to the treating physician, and current US practice is set out in the 2025 US Public Health Service guidelines for occupational HIV exposure — the first major revision since 2013, which updated preferred antiretroviral regimens, shortened the follow-up HIV testing period, and removed routine drug-toxicity labs (US PHS, 2025).
The wider prevention toolkit has also moved on. The 2025 FDA approval of lenacapavir as a twice-yearly injectable pre-exposure option illustrates how far PEP and PrEP have advanced beyond the regimens baked into older training decks — a reason to check that exposure-response training reflects current clinical guidance rather than a decade-old protocol.
The failure pattern that undoes all of this is underreporting. A meaningful share of sticks go unreported because the worker judges the paperwork a hassle or fears stigma — and an unreported exposure cannot receive time-critical prophylaxis. Programs that make reporting fast, accessible around the clock, and explicitly blame-free consistently see better reporting and better outcomes.

Compliance Requirements Across Jurisdictions (US, UK, EU)
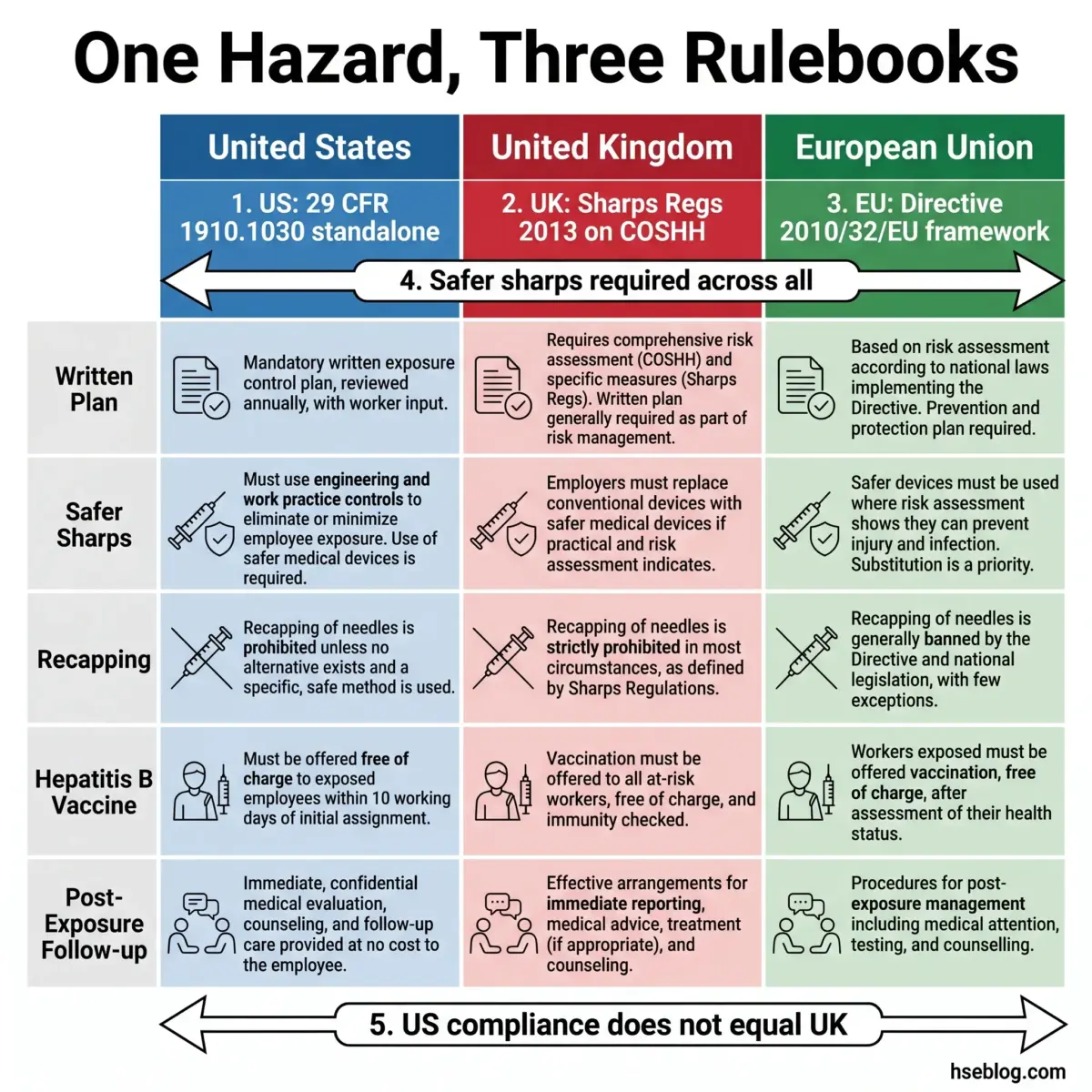
The control philosophy converges across the US, UK, and EU, but the legal architecture differs sharply — and that structural difference is what trips up multinational employers. In the US the duties sit in one prescriptive standalone standard; in the UK and EU they layer specific sharps requirements onto general risk-assessment law.
Regulatory content here reflects general HSE professional understanding of US, UK, and EU requirements as of 2025. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.
| Element | US — OSHA 1910.1030 | UK — Sharps Regs 2013 (HSIS7) | EU — Directive 2010/32/EU |
|---|---|---|---|
| Legal structure | Standalone prescriptive standard | Sits atop COSHH and HSWA | Framework agreement, transposed by states |
| Written plan / risk assessment | Written Exposure Control Plan, reviewed annually | Risk assessment under COSHH | Risk assessment required |
| Safer sharps | Required; device input from staff | Required where reasonably practicable | Safety-engineered devices required |
| Recapping | Prohibited as a work practice | Prohibited | Prohibited |
| HBV vaccine offer | Free, within 10 working days | Provided as part of health protection | Vaccination offered |
| Sharps injury log | Required (employers with 11+ employees) | Records via RIDDOR where applicable | Incident recording required |
| Post-exposure follow-up | Confidential, employer-funded | Medical advice and treatment arranged | Incident response required |
A few practitioner notes on reading the table:
- US: The duties flow from a single source — OSHA’s Bloodborne Pathogens Standard, 29 CFR 1910.1030 — strengthened by the Needlestick Safety and Prevention Act (2000), which mandated the sharps injury log and front-line input on device selection.
- UK: The Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 require safer sharps where reasonably practicable and prohibit recapping, but they operate inside the broader COSHH and Health and Safety at Work Act framework rather than as a self-contained code. HSE’s sharps guidance is the Tier 1 reference.
- EU: Council Directive 2010/32/EU implemented the HOSPEEM/EPSU framework agreement and drove member-state sharps legislation, requiring risk assessment, elimination of unnecessary sharps, safety-engineered devices, training, and incident response across the healthcare sector.
The trap to name plainly: an OSHA-compliant program does not automatically satisfy UK or EU duties. Because the UK and EU requirements attach to separate risk-assessment law, a multinational employer that lifts its US ECP wholesale will still have gaps under COSHH or the relevant national transposition — and assuming otherwise is the structural error behind a lot of cross-border non-compliance.
Bloodborne Pathogens Training Requirements
Training is a legal duty tied to exposure, not a box-ticking purchase — and under OSHA it must happen before a worker is assigned to exposure duties and at least annually thereafter. It is also triggered again whenever new tasks or procedures change the exposure profile.
The core content the training must cover:
- The standard itself — a copy and explanation of 29 CFR 1910.1030 and the workplace’s Exposure Control Plan.
- Transmission and recognition — how bloodborne pathogens spread and how to identify tasks with exposure risk.
- The control hierarchy — engineering controls, work practices, and PPE, including correct selection, use, and removal.
- The hepatitis B vaccine — its benefits, efficacy, and the no-cost offer.
- Exposure response — the immediate steps, reporting route, and the post-exposure evaluation and follow-up.
Retraining triggers worth flagging in any program document:
- A new device, procedure, or task that alters exposure risk.
- A role change that brings a previously out-of-scope worker into exposure duties.
- The annual cycle, which is a floor, not a ceiling.
The equivalent duty exists across jurisdictions even where the wording differs. UK employers must provide information, instruction, and training under the Sharps Regulations 2013 and COSHH, and EU member states carry training obligations transposed from Directive 2010/32/EU — so a workforce spread across regions needs training mapped to each jurisdiction, not a single US module applied everywhere.
Frequently Asked Questions
Conclusion
The industry tends to over-engineer its bloodborne pathogens documentation and under-engineer the two moments that actually decide outcomes: the post-use disposal window where most sticks happen, and the first hour after an exposure where time-critical prophylaxis is won or lost. A binder reviewed once and filed does nothing for either. A live exposure control program — with safer sharps chosen by the people using them, fast and blame-free reporting, and a workforce that knows the response cold — does.
If there is a single highest-impact change, it is to design the system so reporting is effortless and stigma-free, because an unreported exposure cannot be treated, and treatment is where the science still has the most to offer. The 2025 US PHS revision and newer prevention options have widened that clinical window; the failure point is almost always organizational, not pharmacological. The other quiet win is correctness — knowing that PPE here is splash protection, that Universal Precautions is the term OSHA actually uses, and that an OSHA-compliant program does not carry over to the UK or EU.
For any HSE professional building or auditing a bloodborne pathogens program, the uncomfortable question is worth asking directly: if a worker on your site took a needlestick during disposal tonight, would they know exactly what to do, and would the system reward them for reporting it within the hour? If the answer is anything short of yes, that is where the work is.