

TL;DR
- Heat exhaustion is your body’s distress signal — it means your cooling system is failing and heatstroke is minutes away.
- Core body temperature between 38°C and 40°C triggers heavy sweating, nausea, dizziness, and muscle cramps.
- Dehydration, poor acclimatization, and high workload are the three most common root causes on job sites.
- Immediate shade, active cooling, and oral rehydration can reverse heat exhaustion within 30 minutes if caught early.
- Supervisors miss early symptoms 60% of the time — buddy monitoring and scheduled rest breaks save lives.
I was conducting a heat stress assessment on a pipeline construction project in the Gulf during peak summer. Ambient temperature had climbed past 48°C by 10:30 AM. A welder’s helper sat down on a pipe rack, helmet still on, gloves still on, staring at the ground. His buddy assumed he was resting. Twenty minutes later, a foreman found him semi-conscious, skin clammy, pulse racing. His core temperature read 39.4°C on a tympanic thermometer. He was deep into heat exhaustion — one missed check away from full heatstroke.
That incident changed how I approach thermal health surveillance on every project since. Heat exhaustion is not a minor inconvenience or a sign of poor fitness. It is a medical emergency in progress — the last warning your body gives before thermoregulatory collapse. Every year, thousands of outdoor and industrial workers experience heat exhaustion symptoms, and too many supervisors treat them as fatigue or dehydration alone. This article breaks down exactly what heat exhaustion is, how to recognize every symptom before it escalates, what causes it on real job sites, and how to respond when the signs appear.
What Is Heat Exhaustion and Why Does It Matter?
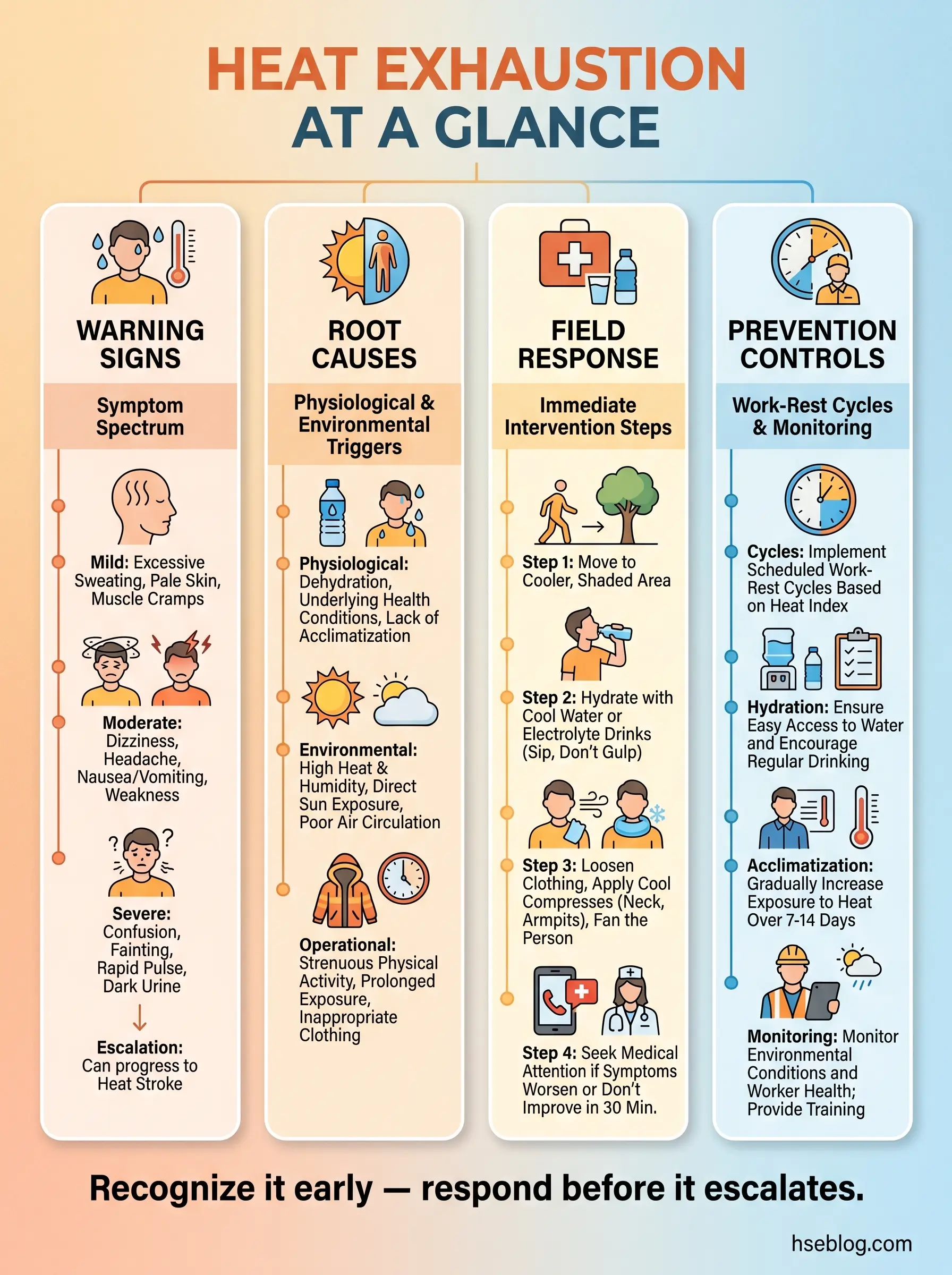
Heat exhaustion is a heat-related illness that occurs when the body cannot dissipate heat fast enough to maintain a safe core temperature. It sits on the heat illness spectrum between heat cramps and heatstroke — and the transition from exhaustion to stroke can happen in under 30 minutes without intervention.
The body cools itself through two primary mechanisms: sweating (evaporative cooling) and vasodilation (redirecting blood flow to the skin surface). When environmental heat, humidity, physical workload, or clothing barriers overwhelm both mechanisms, internal temperature rises past the body’s safe operating range of 36.5–37.5°C. Once core temperature reaches 38–40°C and the cooling system is struggling, heat exhaustion sets in.
Understanding this physiological tipping point matters because it explains why symptoms appear the way they do. Every symptom of heat exhaustion traces back to the body diverting resources — blood, water, electrolytes — away from normal functions to fight rising temperature. The heart pumps harder. The brain gets less blood. Muscles lose electrolytes. The gut shuts down non-essential digestion. All of these show up as specific, recognizable warning signs.
OSHA’s Technical Manual, Section III, Chapter 4 classifies heat exhaustion as a serious occupational health hazard requiring engineering controls, administrative controls, and medical monitoring in workplaces where WBGT values exceed action limits.
Pro Tip: If you’re running a heat stress program, stop relying solely on ambient temperature. Wet Bulb Globe Temperature (WBGT) accounts for humidity, radiant heat, and air movement — the three variables that actually determine heat load on workers. I’ve seen sites at 35°C ambient with 85% humidity produce more heat casualties than sites at 45°C in dry conditions.
Recognizing Heat Exhaustion Symptoms in the Field
The most dangerous thing about heat exhaustion is not the condition itself — it’s how easily its symptoms get dismissed. I’ve reviewed incident reports where supervisors documented “worker felt dizzy and took a break” with no medical follow-up, no temperature check, no escalation. That worker was exhibiting a textbook heat exhaustion symptom, and the system treated it as a rest issue.
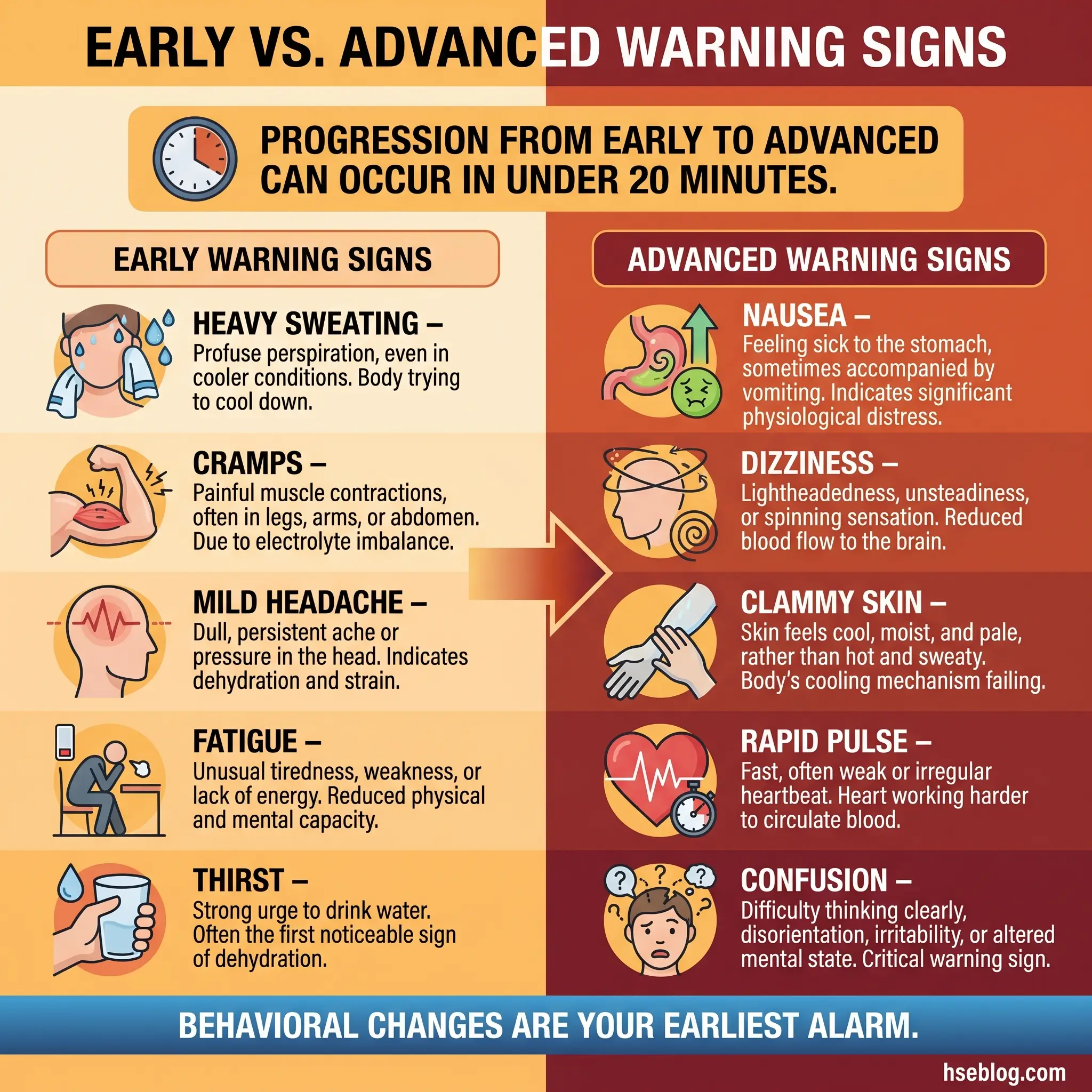
Heat exhaustion symptoms fall into two categories: early warning signs and advanced signs. Knowing both — and training your crew to spot them in each other — is the difference between a 20-minute recovery and an ICU admission.
Early Warning Signs
These symptoms appear first, often while the worker is still on task. They signal that the body’s cooling system is under strain but still functioning.
- Heavy, prolonged sweating: The body is dumping fluid to cool the skin. Sweat production increases dramatically — soaking through clothing, dripping from the hard hat brim. This is the body working overtime, not a sign of good acclimatization.
- Muscle cramps: Especially in the calves, thighs, and abdomen. These result from electrolyte depletion — sodium and potassium lost through sweat faster than they’re replaced.
- Mild headache: Reduced blood flow to the brain as the cardiovascular system prioritizes skin cooling. The headache is typically dull and persistent, not sharp.
- Fatigue and weakness: Muscles receive less oxygenated blood because the heart is redirecting circulation to the skin surface. Workers describe feeling “heavy” or “drained” despite having just started their shift.
- Increased thirst: The body’s signal that fluid volume is dropping. By the time a worker feels genuinely thirsty, they’re already 1–2% dehydrated — enough to impair cognitive function.
Advanced Signs
These symptoms indicate the cooling system is failing. The worker needs immediate removal from heat and active intervention.
- Nausea and vomiting: The gut shuts down as blood is diverted away from the digestive tract. Vomiting compounds the problem by accelerating fluid and electrolyte loss.
- Dizziness and lightheadedness: Blood pressure drops as vessels dilate and fluid volume decreases. Workers may stagger, lose balance, or report tunnel vision.
- Cool, clammy, pale skin: The body is still sweating — this distinguishes heat exhaustion from heatstroke, where sweating often stops. Skin feels wet and cold to the touch despite high environmental temperature.
- Rapid, weak pulse: The heart compensates for low blood volume and vasodilation by beating faster, but with less force per beat. Pulse rates of 100–130 bpm are common.
- Profuse sweating followed by reduced sweating: A critical transition sign. If a worker who was sweating heavily suddenly becomes dry-skinned in a hot environment, they may be progressing toward heatstroke.
- Irritability and confusion: Cognitive impairment from reduced cerebral blood flow. Workers may become uncharacteristically aggressive, make poor decisions, or fail to respond clearly to questions.
Pro Tip: Train your buddy system to watch for behavioral changes, not just physical signs. A worker who stops talking, loses their sense of humor, or starts making unusual mistakes is showing early neurological effects of heat exhaustion. I’ve caught more cases by noticing personality shifts than by checking skin temperature.
Root Causes of Heat Exhaustion on Job Sites
Every heat exhaustion case I’ve investigated traces back to a combination of environmental, physiological, and organizational factors. Rarely is it one thing alone. The welder’s helper I mentioned earlier wasn’t just working in extreme heat — he was dehydrated from the previous day, hadn’t acclimatized to the climate, and was wearing a full FR coverall with no scheduled rest break for three hours.
Understanding the causes of heat exhaustion requires looking at three layers: what the environment does to the body, what the body brings to the situation, and what the work system fails to control.
Environmental Causes
The external heat load on a worker comes from more than just air temperature. These environmental factors drive the thermal burden that overwhelms the body’s cooling capacity.
- High ambient temperature: The most obvious factor, but rarely sufficient on its own. Ambient temperatures above 35°C create conditions where the body struggles to lose heat through convection and radiation.
- High humidity: Humidity above 60% drastically reduces the effectiveness of evaporative cooling. Sweat stays on the skin instead of evaporating, removing little heat despite high sweat rates. This is why tropical and coastal sites produce more heat illness at lower temperatures than dry desert sites.
- Radiant heat sources: Working near furnaces, kilns, hot piping, asphalt, or sun-heated metal surfaces adds a radiant heat load that ambient temperature readings miss entirely.
- Poor air movement: Enclosed or sheltered work areas with minimal wind or ventilation trap heat around the worker. Confined spaces, trenches, and areas behind wind barriers are high-risk zones.
- Direct sun exposure: Solar radiation can add 5–10°C to the effective temperature experienced by a worker. Hard hat color, clothing reflectivity, and shade availability all matter.
Physiological Causes
Individual physiology determines how efficiently a worker can cope with heat load. Two workers in identical conditions can respond very differently based on these factors.
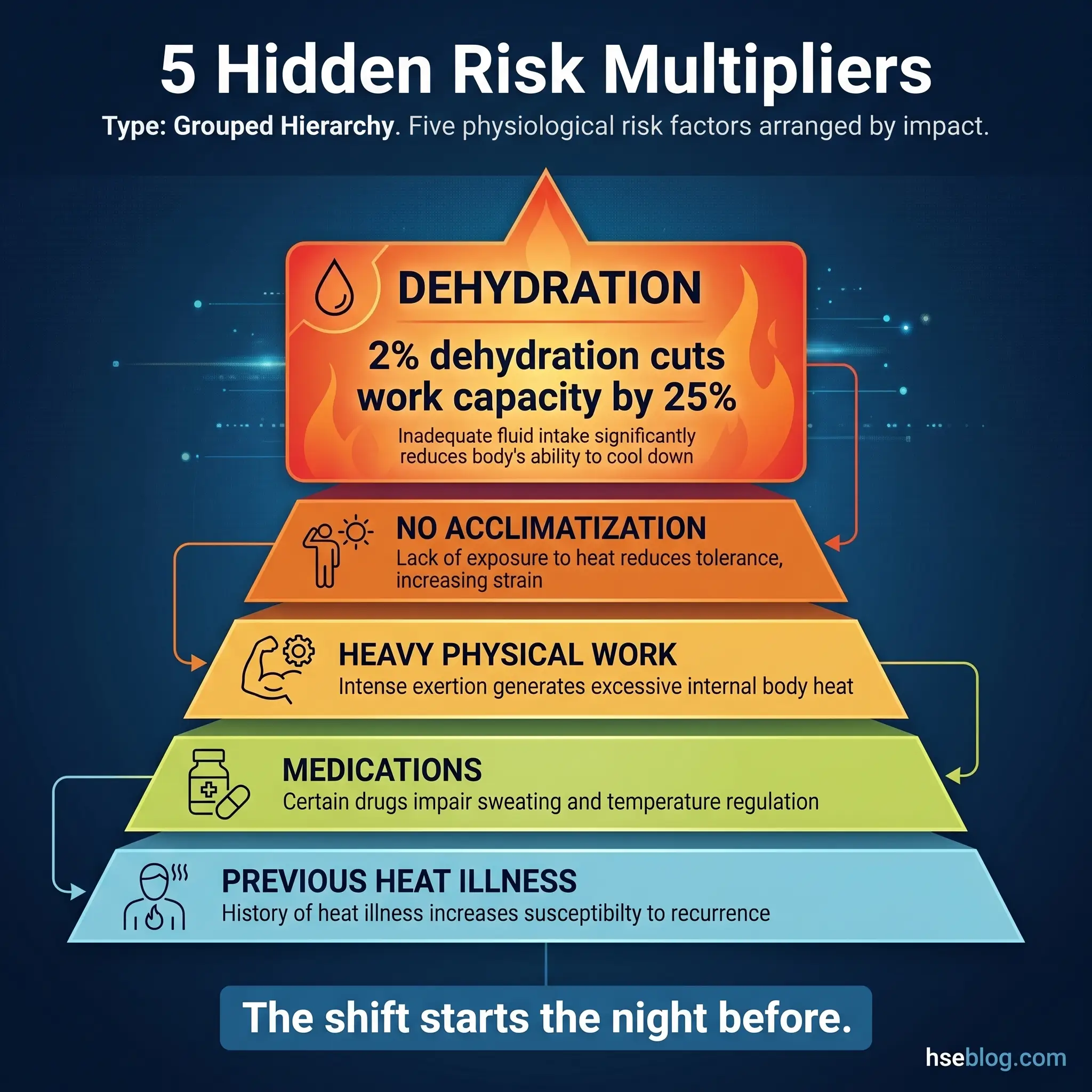
- Dehydration: The single most common physiological contributor. A fluid deficit of just 2% body weight reduces sweat production and impairs cardiovascular function. Workers who arrive on shift already dehydrated from the previous evening — often due to caffeine, alcohol, or simply not drinking enough — are at immediate risk.
- Poor acclimatization: Workers new to hot environments need 7–14 days of gradually increasing heat exposure to develop physiological adaptations — increased sweat rate, lower heart rate, expanded plasma volume. Unacclimatized workers produce less sweat and lose more electrolytes per liter of sweat.
- Physical exertion: Heavy manual work generates internal metabolic heat that compounds the external heat load. A worker performing moderate-to-heavy labor generates 300–500 watts of metabolic heat — equivalent to running a space heater inside their body.
- Obesity: Higher body mass index increases metabolic heat production and reduces the surface-area-to-mass ratio available for heat dissipation. Workers with BMI above 30 are at significantly elevated risk.
- Medications and health conditions: Diuretics, beta-blockers, antihistamines, and stimulants all impair thermoregulation. Cardiovascular disease, diabetes, and previous heat illness episodes also reduce heat tolerance.
- Age: Workers over 50 have reduced sweat gland efficiency and slower cardiovascular adaptation to heat. However, younger workers often take more risks and underestimate their limits.
Organizational Causes
These are the systemic failures that create the conditions for heat exhaustion — the ones management controls and the ones I flag most often in audit findings.
- No acclimatization schedule: Throwing new workers or returning-from-leave workers into full heat exposure on day one. OSHA and NIOSH both recommend starting at 20% workload and increasing by 20% per day over a five-day period.
- Inadequate hydration infrastructure: Water sources too far from work areas. Warm or unpalatable water that workers avoid. No electrolyte replacement available. I’ve audited sites where the nearest water cooler was a 10-minute walk from the work front — effectively guaranteeing dehydration.
- Insufficient rest breaks: Work schedules that don’t account for heat index. Workers pushing through without mandatory cooling breaks because production targets override safety controls.
- Inappropriate PPE for conditions: FR coveralls, chemical suits, and impermeable clothing trap heat against the body. When PPE selection doesn’t factor in thermal burden, workers overheat despite proper task-specific protection.
- Lack of heat illness training: Supervisors and workers who can’t recognize heat exhaustion symptoms, don’t know when to stop work, and have no escalation protocol for thermal emergencies.
Pro Tip: During pre-task briefings in hot conditions, I always ask three screening questions: “Did you drink water last night and this morning?” “Did you sleep at least six hours?” “Are you taking any medication?” These three questions have flagged high-risk individuals before they even started work.
How Heat Exhaustion Differs from Heat Stroke
Confusing heat exhaustion with heatstroke — or worse, treating heatstroke as heat exhaustion — kills workers. I’ve seen emergency response teams lose critical minutes because the initial assessment was wrong. The distinction is clinical, and every supervisor on a hot-weather site needs to know it cold.
The key differentiators between these two conditions are clear when you know what to look for. This comparison covers the clinical markers that separate a recoverable condition from a life-threatening emergency.
| Clinical Marker | Heat Exhaustion | Heat Stroke |
|---|---|---|
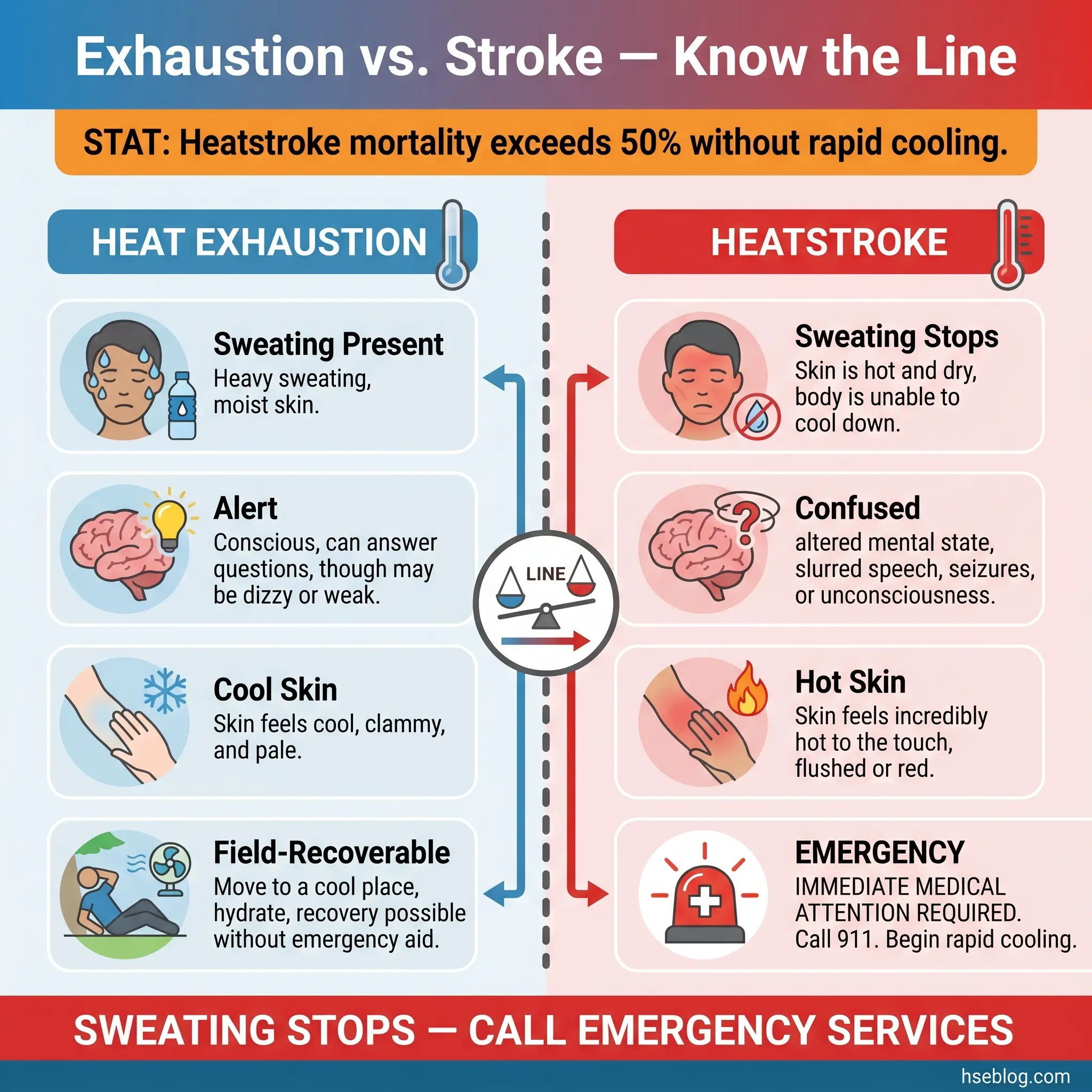
| Core body temperature | 38°C – 40°C | Above 40°C |
| Sweating | Present — often profuse | Absent or minimal (dry, hot skin) |
| Mental status | Alert but fatigued; mild confusion possible | Altered consciousness, seizures, delirium |
| Skin appearance | Cool, pale, clammy | Hot, red, dry |
| Pulse | Rapid and weak | Rapid and strong |
| Reversibility | Reversible with rest, cooling, fluids | Medical emergency — organ damage possible |
| Response required | Remove from heat, cool, rehydrate, monitor | Call emergency services immediately, aggressive cooling |
The moment a worker stops sweating in a hot environment and becomes confused or combative, you are dealing with heatstroke — not exhaustion. Treat it as a medical emergency with zero delay.
This distinction matters because the response protocols are fundamentally different. Heat exhaustion allows for supervised field recovery. Heatstroke demands emergency medical services, aggressive whole-body cooling, and hospital transport. Getting the assessment right in the first 60 seconds determines the outcome.
Immediate Field Response to Heat Exhaustion
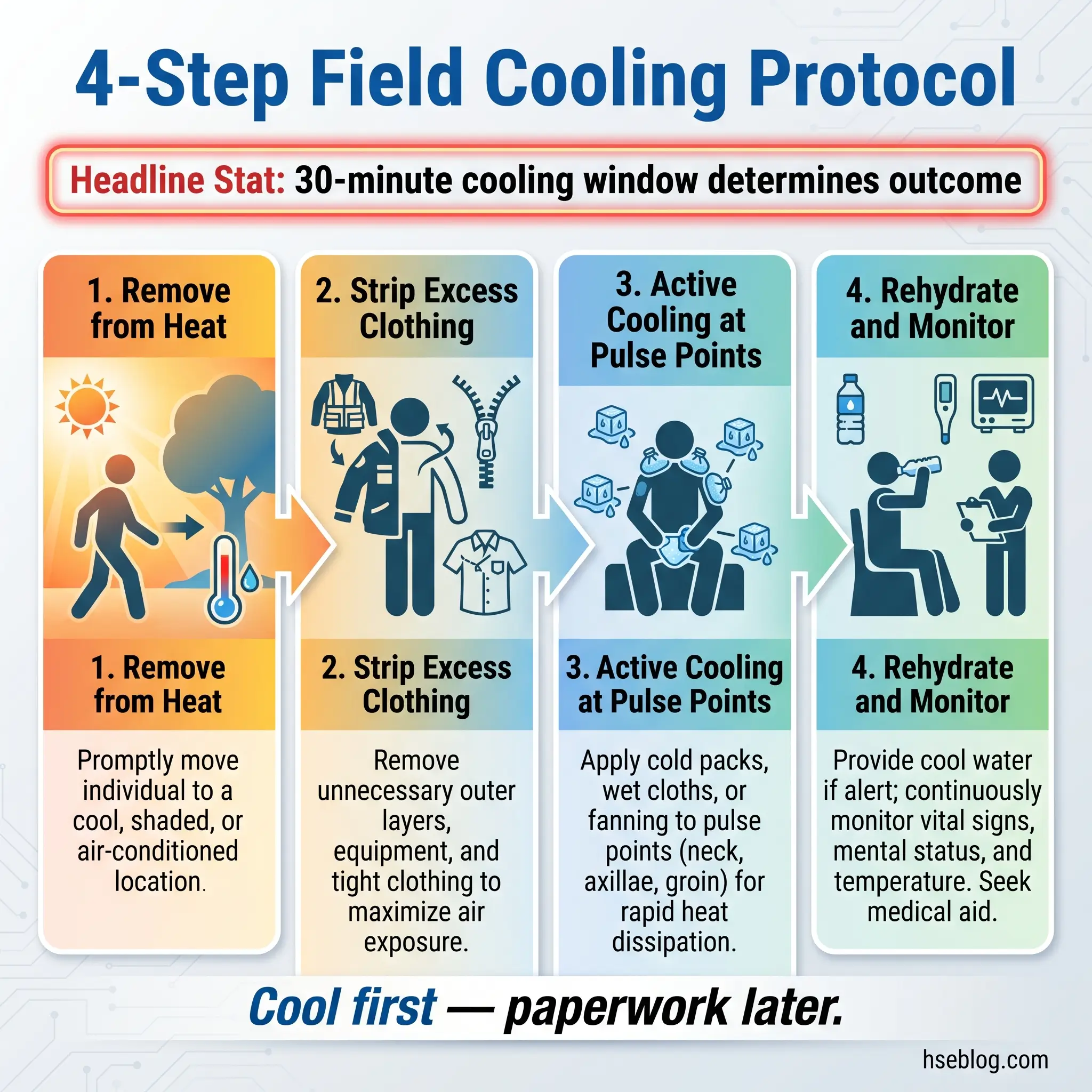
When I train site medical teams and supervisors on heat illness response, I tell them: you have a 30-minute window. Within that window, heat exhaustion is reversible. Beyond it, you’re gambling with organ function.
The following response sequence has been field-validated across multiple projects in hot climates. Every step is deliberate and sequenced for maximum cooling efficiency.
- Stop work and remove the worker from the heat source. Move them to the nearest shaded or air-conditioned area. If no shade exists, create it — a vehicle cab with AC running, a tarp shelter, or an emergency cooling tent.
- Loosen or remove restrictive clothing. Unzip FR coveralls, remove hard hat, open collars. Every layer trapping heat against the skin delays cooling.
- Position the worker semi-reclined with feet slightly elevated if they’re lightheaded. If nauseated, position on their side to protect the airway.
- Begin active cooling immediately. Apply cold wet towels to the neck, armpits, and groin — high blood-flow areas where cooling transfers fastest. Use fan-assisted evaporative cooling if available. Misting the skin with water while fanning accelerates heat loss.
- Begin oral rehydration with cool water or electrolyte solution. Small, frequent sips — not large gulps. If the worker is vomiting, do not force fluids orally; this requires medical evaluation for IV rehydration.
- Monitor core temperature every 10 minutes using a tympanic or temporal artery thermometer. Target: core temperature below 38°C within 30 minutes.
- Assess mental status continuously. If confusion worsens, speech becomes slurred, or the worker loses consciousness, escalate immediately to a heatstroke protocol and activate emergency medical services.
- Do not allow the worker to return to heat exposure on the same shift. Even after symptom resolution, the thermoregulatory system remains compromised for 24–48 hours.
Pro Tip: Keep pre-mixed cold towels in insulated coolers at work fronts during hot-weather operations. I started this practice after watching a medic waste four minutes looking for towels and a water source during a real incident. Four minutes of uncontrolled core temperature rise is the difference between recovery and hospitalization.
Preventing Heat Exhaustion on the Job Site
Prevention outperforms response every single time. The most effective heat illness programs I’ve seen — and helped design — treat prevention as an engineering and administrative control problem, not a worker behavior issue. Blaming workers for “not drinking enough water” while scheduling six-hour shifts with no rest break in 45°C heat is a management failure, not a hydration failure.
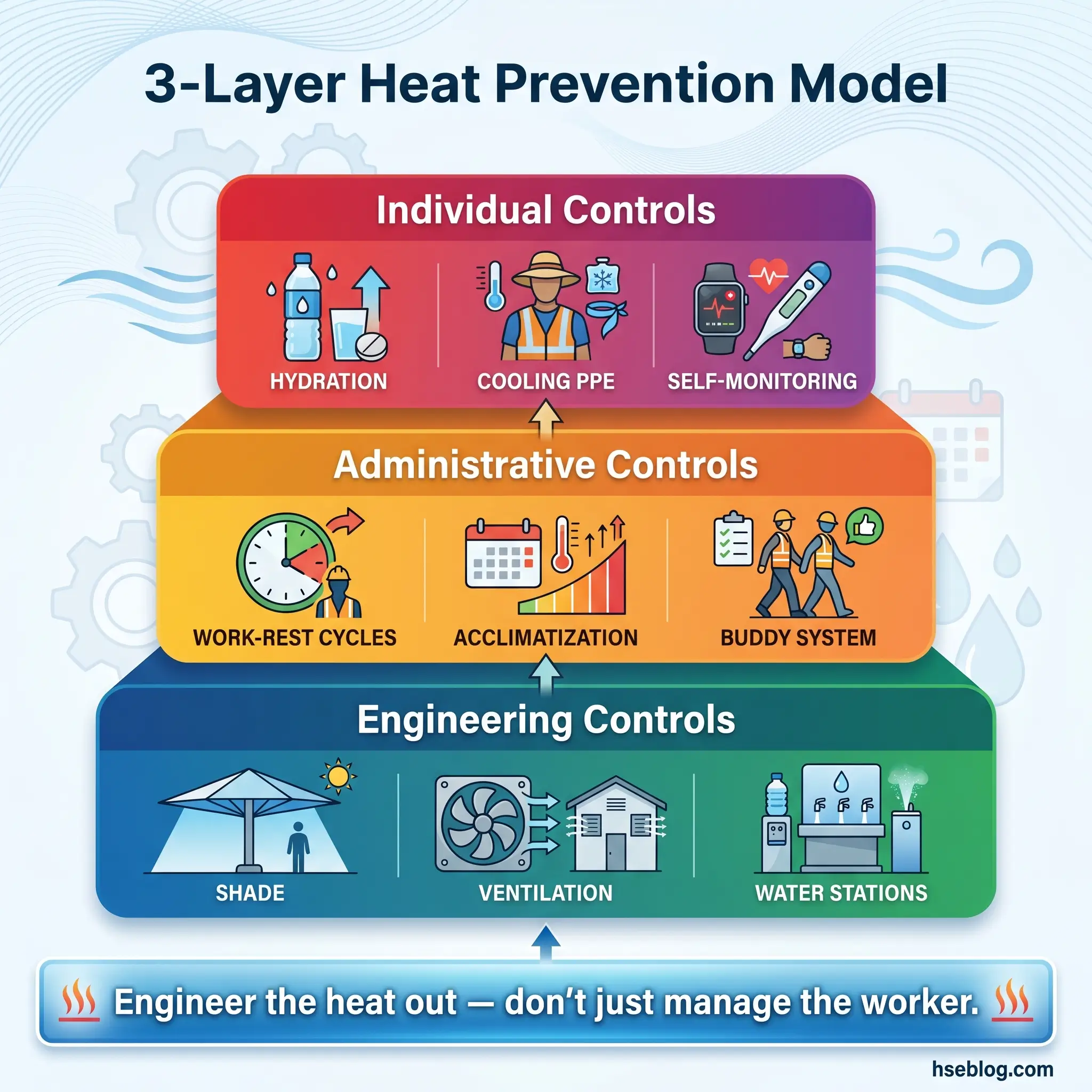
Effective prevention requires controls at three levels: engineering the environment, managing the work schedule, and supporting the individual worker.
Engineering Controls
These modify the work environment to reduce the heat load reaching the worker.
- Shade structures and sun barriers: Fixed or portable canopies over static work areas, reflective barriers near radiant heat sources, and shaded rest stations within two minutes’ walk of every work front.
- Mechanical ventilation and air movement: Industrial fans, forced-air blowers in enclosed areas, and air-conditioned break trailers positioned near high-heat tasks.
- Radiant heat shielding: Reflective curtains around furnaces, hot piping insulation, and heat-reflective coatings on surfaces workers contact.
- Cooled water stations: Insulated water dispensers stocked with cool (10–15°C) water and electrolyte supplements, positioned so no worker walks more than 100 meters to access hydration.
Administrative Controls
These manage the exposure duration and work intensity to keep workers within safe thermal limits.
- WBGT-based work-rest schedules: Match work-rest ratios to measured WBGT values and workload categories. At WBGT 30°C with moderate workload, ACGIH TLVs recommend 25% rest per hour.
- Acclimatization protocols: New workers and those returning from seven or more days’ absence start at 20% workload, increasing 20% per day. Full acclimatization takes 7–14 days.
- Shift scheduling: Schedule heavy tasks during cooler hours. On Gulf projects, I’ve implemented split shifts — work from 5:00–10:00 AM and 3:00–6:00 PM — eliminating the peak heat window entirely.
- Buddy monitoring systems: Pair workers and train them to observe each other for heat exhaustion symptoms. A buddy who notices behavioral changes acts faster than any environmental monitor.
- Pre-shift health screening: Brief check-in questions covering hydration status, sleep quality, medication use, and prior-day heat exposure. Flag and reassign high-risk individuals.
Individual Worker Controls
These support the worker’s ability to self-regulate and respond to their own body.
- Hydration discipline: Drink 200–250 ml of water every 15–20 minutes during heat exposure — before thirst signals appear. Electrolyte replacement after the first hour of heavy sweating.
- Cooling PPE where feasible: Evaporative cooling vests, neck wraps, and moisture-wicking base layers that enhance the body’s cooling efficiency without compromising task-specific PPE requirements.
- Self-monitoring awareness: Workers trained to recognize their own early symptoms — headache, cramps, unusual fatigue — and empowered to stop work without penalty through a robust stop-work authority culture.
- Off-shift recovery: Adequate sleep, rehydration before next shift, avoidance of alcohol and excessive caffeine. The recovery that happens between shifts is as critical as the controls during the shift.
Conclusion
Heat exhaustion is a preventable condition that becomes a medical emergency only when organizations and individuals fail to act on clearly visible warning signs. Every case I’ve investigated shares the same pattern: environmental heat plus physiological vulnerability plus organizational gaps. Remove any one of those three, and the worker goes home safe.
The symptoms of heat exhaustion — heavy sweating, cramps, nausea, dizziness, rapid pulse, confusion — are not subtle. They follow a predictable progression that gives supervisors, buddies, and the worker themselves a window to intervene. The causes — dehydration, poor acclimatization, excessive workload, inadequate rest, and environmental extremes — are well understood and entirely controllable through engineering, administrative, and individual measures.
No production target, no project deadline, and no shift schedule is worth a worker’s thermoregulatory collapse. Heat exhaustion tells you the body is losing a fight it cannot win alone. Your job — whether you’re the safety officer, the supervisor, or the worker standing next to someone who looks unwell — is to answer that signal before the body stops sending it.