

TL;DR — Myth vs Reality
- Myth: Silicosis is a disease of the past, confined to old miners. Reality: Approximately 138,971 new cases were diagnosed globally in 2019 alone — a 64.6% increase from 1990 (Huang et al., 2024). Engineered stone is producing accelerated disease in workers under 35.
- Myth: If you can’t see dust, you’re safe. Reality: Respirable crystalline silica particles are invisible to the naked eye. Dangerous airborne concentrations routinely exist without any visible dust cloud — only air monitoring detects them.
- Myth: Silicosis can be treated and reversed with medication. Reality: There is no cure. Lung fibrosis caused by silica is permanent. Treatment manages symptoms only. Lung transplant is a last resort.
- Myth: A dust mask is enough protection. Reality: Respiratory protective equipment is the last line of defence. Wet cutting, local exhaust ventilation, and HEPA filtration must come first. When RPE is needed, it must be face-fit tested — a loose-fitting mask provides a false sense of security.
Silicosis is an irreversible occupational lung disease caused by inhaling respirable crystalline silica dust — fine particles generated when materials like concrete, sandstone, or engineered stone are cut, ground, or drilled. These particles scar the lungs, progressively destroying breathing capacity. There is no cure. Silicosis is entirely preventable through effective dust controls, exposure monitoring, and respiratory protection.
What Is Silicosis? Understanding the Disease and Why It Matters Now
In 2019, more than 12,900 people died from silicosis worldwide, with 655,700 disability-adjusted life years lost to a disease that is entirely preventable (Global Burden of Disease Study 2019, BMC Pulmonary Medicine, 2022). That figure represents individual workers — stonecutters, tunnellers, countertop fabricators — whose lungs were destroyed by a substance found in ordinary rock, sand, and concrete. Silicosis is not an exotic hazard. It is the consequence of inadequate dust control applied to one of the most common minerals on Earth.
Silicosis is a form of pneumoconiosis — a group of lung diseases caused by inhaling mineral dusts — specifically triggered by respirable crystalline silica (RCS). The three most common crystalline forms are quartz, cristobalite, and tridymite, with quartz being by far the most prevalent in occupational settings. When silica-containing materials are mechanically disturbed — cut, drilled, ground, blasted, or polished — they release fine particles small enough to penetrate deep into the lungs’ alveoli, where gas exchange occurs. There, these particles trigger a destructive immune response that deposits scar tissue in place of functioning lung tissue. The scarring is permanent.
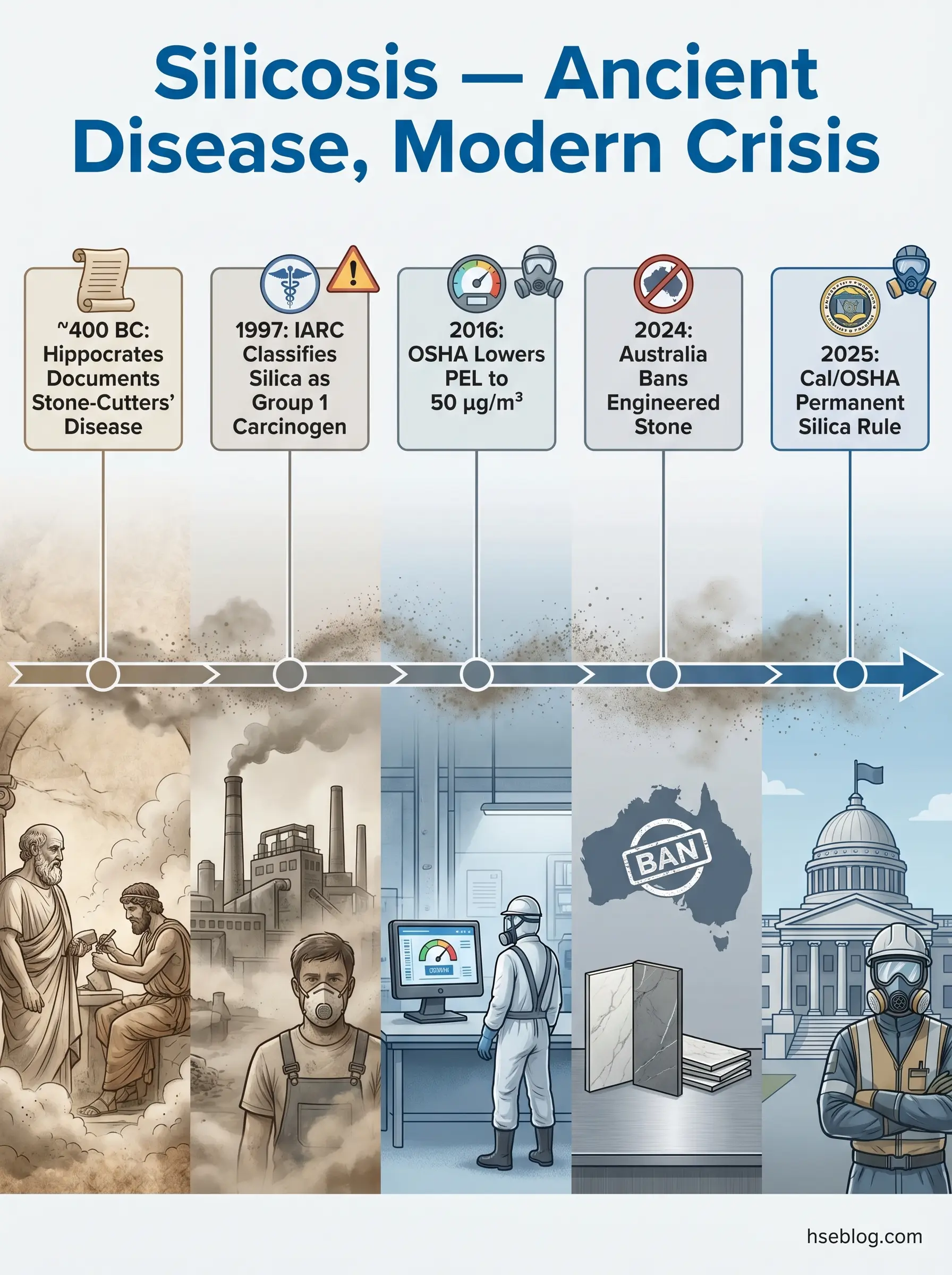
What makes silicosis especially urgent right now is its resurgence in a demographic that traditional occupational health models did not anticipate. The explosion of engineered stone countertops since the early 2000s — products containing over 90% crystalline silica — has produced accelerated silicosis in young fabrication workers, many under 35. Australia responded by becoming the first country in the world to ban engineered stone manufacture, supply, and installation, effective 1 July 2024 (Safe Work Australia, 2024). The International Agency for Research on Cancer (IARC) classifies crystalline silica (in the form of quartz or cristobalite) as a Group 1 carcinogen — carcinogenic to humans. The biggest misconception practitioners encounter is that silicosis belongs to mining’s past. The engineered stone crisis has demonstrated it can emerge rapidly in modern, small-workshop settings where controls are absent.
What Causes Silicosis? How Silica Dust Damages the Lungs
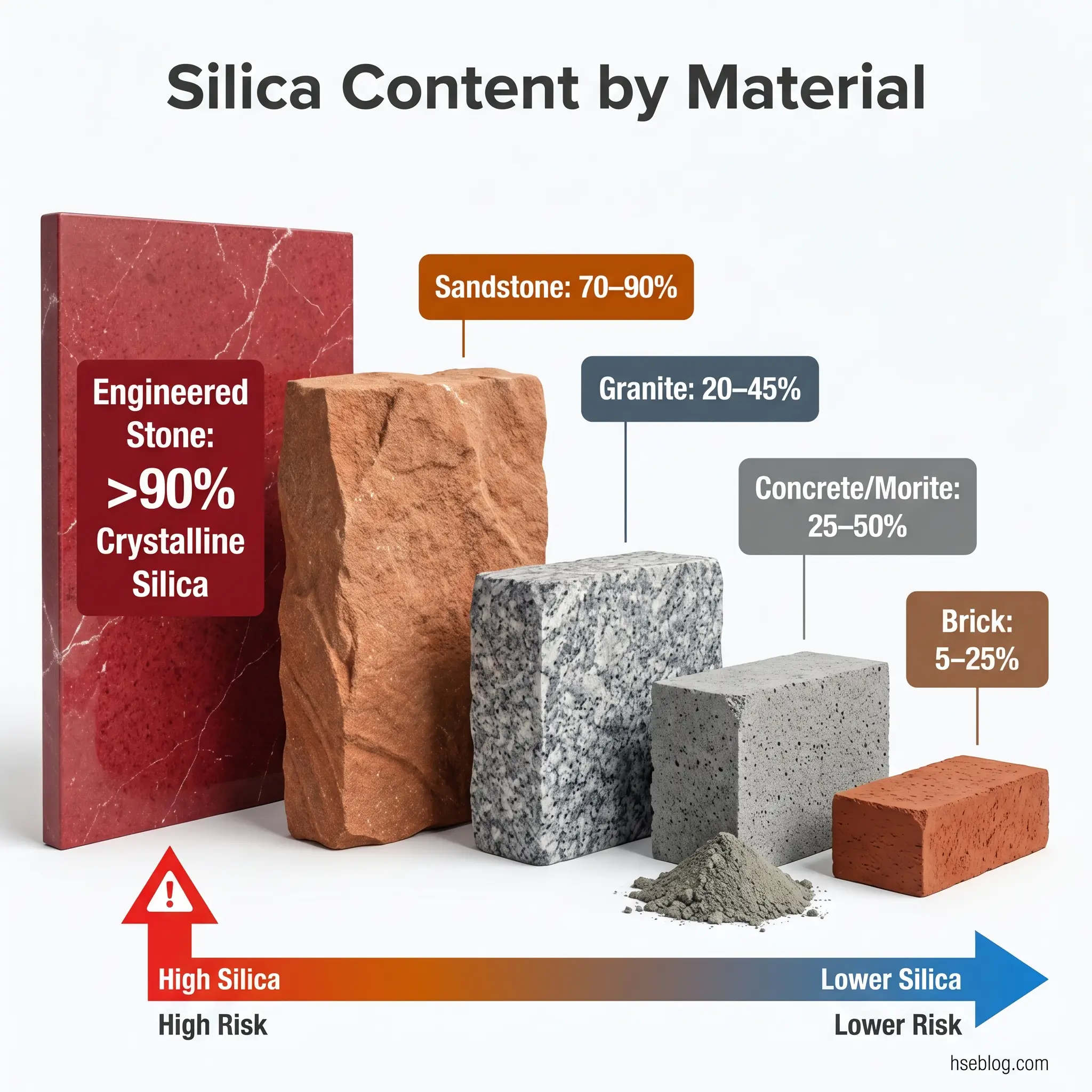
Crystalline silica is the most abundant mineral in the Earth’s crust. It is present in sand, granite, sandstone, slate, concrete, brick, morite, and — at particularly concentrated levels — engineered stone products. In its undisturbed state, silica-containing material poses no inhalation risk. The hazard begins the moment that material is mechanically worked: cut with a saw, drilled, ground with an angle grinder, jackhammered, sandblasted, or polished. These actions fracture the crystalline structure and release respirable particles — fragments smaller than 10 micrometres, with the most damaging fraction below 4 micrometres.
The pathological sequence is specific and well-documented. Inhaled RCS particles small enough to bypass the nose and upper airways travel deep into the terminal bronchioles and alveoli. Alveolar macrophages — the lungs’ frontline immune cells — attempt to engulf and clear the silica particles. Unlike organic debris, crystalline silica is cytotoxic: its surface chemistry destroys the macrophages that ingest it. As these immune cells die, they release inflammatory cytokines and reactive oxygen species, recruiting more immune cells and triggering a chronic inflammatory cascade. Fibroblasts respond to the sustained inflammation by depositing collagen, forming fibrotic nodules — small, hard scars that progressively replace functional lung tissue. These nodules are permanent. The lung does not regenerate the tissue they displace.
A critical distinction that occupational hygienists consistently reinforce: the dose-response relationship is cumulative. Risk depends on the concentration of RCS in the air, the duration and frequency of exposure, and the effectiveness of controls in place. A worker exposed to low concentrations over decades accumulates damage differently from a worker exposed to extreme concentrations over months — but both pathways lead to the same irreversible endpoint. Equally critical is the misconception that visible dust indicates danger while invisible air means safety. Respirable silica particles are invisible to the naked eye. Visible dust clouds represent larger, non-respirable particles. The most dangerous concentrations exist below the threshold of human perception, which is precisely why air monitoring with calibrated sampling equipment is indispensable — not optional.
High-Risk Occupations and Industries
Approximately 2.3 million workers in the United States alone face occupational silica exposure (US Department of Labor, current estimate). The industries generating the highest exposure vary in obvious ways — mining versus countertop fabrication — but share a common mechanism: mechanical disruption of silica-containing material in conditions where dust is inadequately captured or suppressed.
Construction generates the broadest exposure footprint. Cutting, drilling, and grinding concrete and masonry with handheld tools are among the highest-exposure tasks documented in occupational hygiene literature. Tuckpointing — grinding mortar joints in brickwork — consistently produces some of the highest airborne RCS concentrations measured in any occupation, often exceeding the OSHA PEL by orders of magnitude without engineering controls. Tunnelling and demolition create sustained exposures in enclosed or semi-enclosed environments where dust accumulates.
Mining and quarrying remain significant sources globally, particularly in low- and middle-income countries where mechanisation has reduced but not eliminated manual rock drilling and crushing. Foundry work — where silica sand moulds are used in metal casting — produces exposure during mould preparation, pouring, and shakeout. Glass manufacturing and ceramics involve silica handling at multiple process stages.
The exposure scenario that has reshaped the global regulatory conversation, however, is engineered stone fabrication. Engineered stone — marketed as quartz countertops — typically contains over 90% crystalline silica, compared with 20–45% in natural granite. When fabrication workers cut, grind, and polish these products without wet methods or ventilation, airborne RCS concentrations can reach levels that produce accelerated silicosis within a decade or less. This is the material and process behind Australia’s world-first ban and a surge of enforcement activity in the United States.
The Three Types of Silicosis and Their Symptom Timelines
Silicosis is not a single uniform disease. It manifests in three clinically distinct forms, differentiated by exposure intensity, latency period, and rate of progression. Understanding these types matters operationally because each implies different control failures and different windows for intervention.
Chronic silicosis is the most common form and the one most associated with traditional mining and construction exposure. It develops after 10 to 20 or more years of exposure to relatively low-to-moderate RCS concentrations. In early stages, it is often entirely asymptomatic — detectable only through routine chest imaging that reveals small rounded opacities, predominantly in the upper lobes. A worker can have chronic silicosis and be unaware of it, which is why health surveillance catches what symptoms do not.
Accelerated silicosis follows heavier exposure over a shorter period — typically 5 to 10 years. Radiographically, it resembles chronic silicosis but progresses faster and carries a worse prognosis. This is the form increasingly diagnosed in engineered stone workers, many of them under 35 — a demographic pattern that challenges the long-standing assumption that silicosis is a disease of older workers with decades of cumulative exposure. The engineered stone crisis has made accelerated silicosis a defining occupational health issue of the 2020s.
Acute silicosis, also termed silicoproteinosis, is the rarest and most devastating form. It develops within weeks to a few years following massive, overwhelming exposure — the kind produced by sandblasting in an enclosed space, for example, or uncontrolled dry cutting of high-silica materials. The alveoli fill with proteinaceous fluid rather than forming nodules, producing a clinical picture that resembles pulmonary oedema. Acute silicosis is rapidly fatal.
All three forms share a defining characteristic: irreversibility. Fibrotic scarring does not resolve when exposure stops. In chronic and accelerated forms, Progressive Massive Fibrosis (PMF) can develop — large confluent fibrotic masses that severely impair breathing and dramatically worsen prognosis. Disease progression after cessation of exposure is well-documented, particularly the transition from simple silicosis to PMF.
| Type | Exposure Level | Latency Period | Prognosis |
|---|---|---|---|
| Chronic | Low to moderate | 10–20+ years | Slowly progressive; may develop PMF |
| Accelerated | Higher concentration | 5–10 years | Faster progression; PMF risk elevated |
| Acute (Silicoproteinosis) | Massive, overwhelming | Weeks to few years | Rapidly fatal |
Recognising the Symptoms of Silicosis: From Early Warning Signs to Advanced Disease
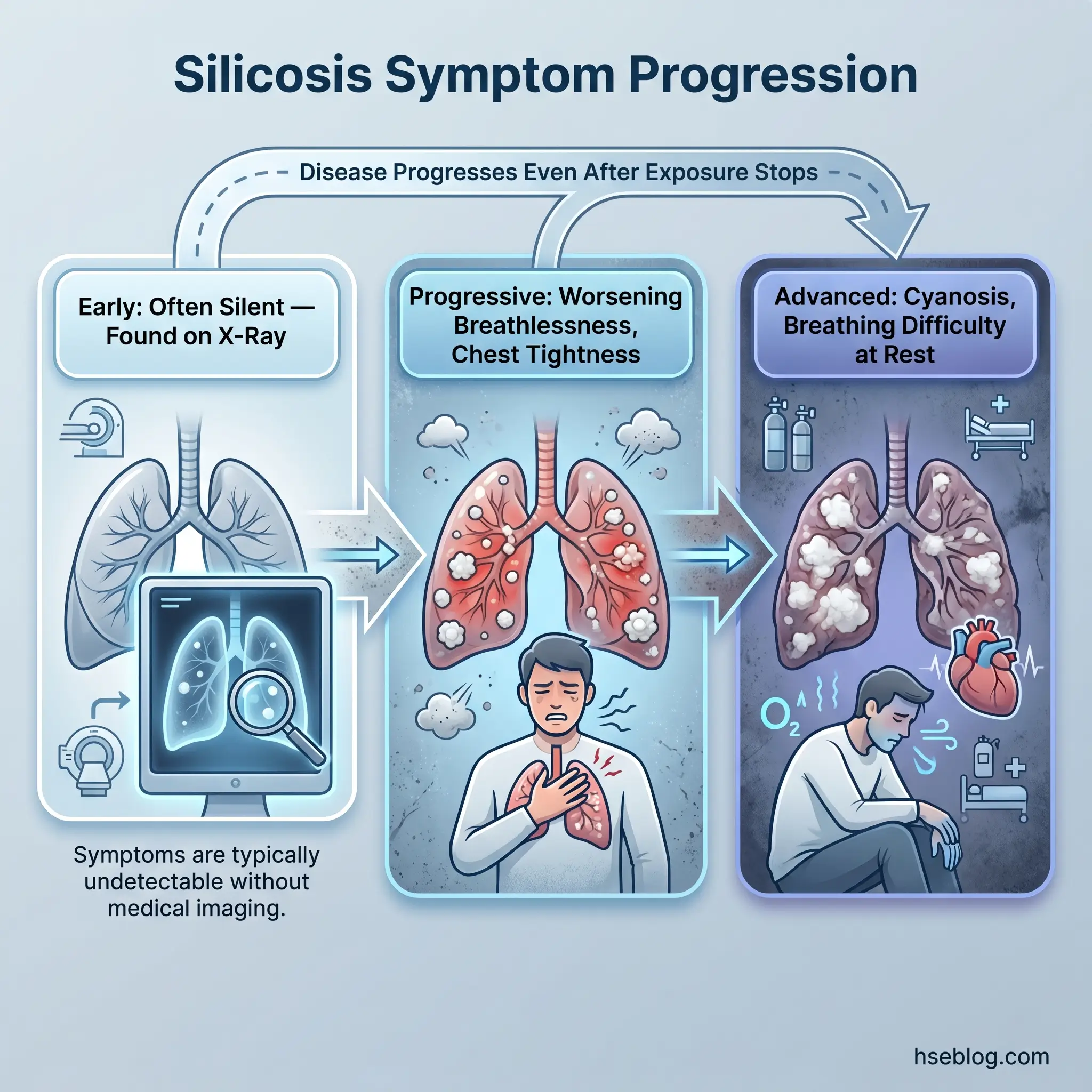
The most dangerous feature of silicosis from a clinical surveillance perspective is its silence in early stages. By the time a worker notices symptoms, significant and irreversible lung damage has already occurred. This is not a disease that announces itself early — it is discovered through monitoring or, too often, through late presentation.
Early symptoms, when they appear, are non-specific: a persistent dry cough that does not resolve, mild shortness of breath during physical exertion, and unexplained fatigue. These are easy to dismiss or attribute to other causes — ageing, fitness, smoking, a lingering cold. Workers in physically demanding jobs often normalise breathlessness as part of the work rather than recognising it as a clinical signal.
As fibrosis progresses, symptoms become more pronounced and harder to ignore. Shortness of breath worsens and occurs with less exertion. Chest tightness develops. Wheezing may appear. Exercise tolerance declines noticeably. Workers may find themselves unable to perform tasks they handled without difficulty a year prior.
In advanced disease, the clinical picture is severe. Cyanosis — a bluish discolouration of the skin and lips — indicates chronic oxygen deprivation. Breathing difficulty occurs at rest. Cor pulmonale — right-sided heart failure caused by chronic pulmonary hypertension — develops as the heart struggles against increased resistance in scarred, stiffened lungs. Weight loss and profound fatigue mark the terminal stages.
A further diagnostic complication: silicosis symptoms overlap significantly with tuberculosis, chronic obstructive pulmonary disease, and pneumonia. Misdiagnosis is common, especially when the clinician does not take a thorough occupational exposure history. The clinical pattern observed across occupational health practice is that early silicosis is most reliably detected incidentally — on routine chest X-rays during scheduled health surveillance — reinforcing that medical monitoring is not an administrative formality but a critical early-detection mechanism.
Watch For: Symptoms can continue to progress even after all silica exposure has stopped. A worker removed from exposure is not “cured” — they require ongoing medical follow-up.
How Is Silicosis Diagnosed?
A thorough occupational exposure history is the cornerstone of silicosis diagnosis — and the point where diagnosis is most often won or lost. Clinicians who ask only about current employment miss the workers who left silica-exposure jobs years or decades ago but are only now presenting with respiratory symptoms. The lag between exposure and symptomatic disease means that the relevant occupational history may stretch back 15 or 20 years, across multiple employers and industries.
Once a silica exposure history is established, imaging is the primary diagnostic tool. A standard posteroanterior chest X-ray reveals the characteristic bilateral small rounded opacities concentrated in the upper lung zones. Occupational health physicians read these films using the International Labour Organization (ILO) Classification of Radiographs of Pneumoconioses — a standardised system that grades the profusion and distribution of opacities to ensure consistent interpretation across practitioners. Computed tomography (CT) scanning is more sensitive than plain X-ray, detecting smaller nodules and mediastinal lymphadenopathy that X-ray may miss. High-resolution CT is particularly valuable for early disease.
Pulmonary function testing — primarily spirometry — measures the functional impact. Silicosis typically produces a restrictive pattern: reduced total lung capacity with relatively preserved airflow rates in early disease. Mixed restrictive-obstructive patterns occur, especially when silica exposure has also caused airways disease. Serial spirometry over time tracks the rate of functional decline.
Because silicosis significantly increases tuberculosis risk, TB screening is a standard component of the diagnostic workup. Tuberculin skin testing or interferon-gamma release assays are used to detect latent TB infection. Lung biopsy is rarely necessary but is definitive when the diagnosis is uncertain — histopathology reveals the pathognomonic silicotic nodule with its characteristic concentric layers of collagen. Bronchoalveolar lavage can support the diagnosis and help rule out competing conditions.
The judgment call for occupational health practitioners is recognising when to pursue silicosis as a differential diagnosis even in the absence of classic imaging findings. Early disease may present with subtle imaging changes that do not yet meet the ILO threshold for formal classification, but the exposure history and clinical trajectory warrant close follow-up and repeat imaging.
Complications and Associated Health Risks of Silica Exposure
Treating silicosis as a standalone lung disease understates the breadth of harm. Crystalline silica exposure and the fibrotic disease it produces are associated with a range of complications that extend well beyond pulmonary fibrosis — a dimension that many general references underserve.
The tuberculosis–silicosis interaction is the most clinically significant and historically documented complication. Silica exposure impairs alveolar macrophage bactericidal function — the same immune cells that silica destroys are the primary defence against Mycobacterium tuberculosis. Published data shows silicosis increases TB risk by a factor of 2 to 30, depending on exposure intensity and the prevalence of TB in the worker’s environment. This interaction is widely recognised in mining medicine but underestimated in non-mining settings. Construction HSE teams rarely incorporate TB screening into their silica health surveillance programmes, even though the immunological mechanism operates identically regardless of industry.
Lung cancer risk is elevated by silica exposure independently of silicosis, though the risk increases further in workers who have developed silicotic fibrosis. IARC’s Group 1 classification of crystalline silica as carcinogenic to humans is based on sufficient evidence of lung cancer causation in exposed workers. The risk is compounded in workers who also smoke — the combined effect of silica exposure and tobacco smoke on lung cancer risk is multiplicative rather than merely additive.
Beyond the lungs, silica exposure is associated with chronic kidney disease through mechanisms that are still being characterised but likely involve systemic inflammatory and autoimmune pathways. Autoimmune disorders — including scleroderma, rheumatoid arthritis (Caplan syndrome when it occurs in the context of pneumoconiosis), and systemic lupus erythematosus — appear at elevated rates in silica-exposed populations. Cor pulmonale, right-sided heart failure secondary to chronic pulmonary hypertension, develops as the heart works against increasing vascular resistance in fibrosed lung tissue.
Treatment and Management of Silicosis
This article provides general HSE knowledge. Clinical management of silicosis must be directed by a qualified occupational physician or respiratory specialist. The information here does not replace individual medical assessment and treatment planning.
There is no curative treatment for silicosis. This is not a qualification or a hedge — it is the clinical reality that shapes every management decision. Fibrotic scarring in the lungs cannot be reversed by any currently available therapy. Treatment focuses entirely on managing symptoms, slowing disease progression where possible, and preventing complications.
The first and most critical clinical intervention is cessation of all further silica exposure. This decision — seemingly straightforward — is often the most contested, because it carries immediate economic consequences for the worker and the employer. Occupational health teams must navigate this tension directly, because continued exposure accelerates a disease that is already progressing. The clinical imperative overrides operational convenience.
Symptomatic management includes bronchodilators to relax airway smooth muscle and reduce breathlessness, and inhaled corticosteroids to manage inflammation and mucus production. Supplemental oxygen therapy becomes necessary in advanced cases where blood oxygen saturation drops below sustainable levels. Pulmonary rehabilitation — structured exercise and breathing technique programmes — can improve functional capacity and quality of life even though it does not alter the underlying fibrosis.
Lung transplantation exists as a last-resort intervention for end-stage silicosis, but it is rare, carries significant surgical risk, and requires lifelong immunosuppression. Smoking cessation is essential for any worker with silicosis — tobacco smoke compounds the inflammatory burden on already-damaged lungs and further elevates lung cancer risk. Vaccinations against influenza and pneumococcal disease are recommended to reduce the risk of respiratory infections in lungs with compromised defence.
Regular medical follow-up is non-negotiable: monitoring for disease progression, screening for TB and lung cancer, and tracking pulmonary function decline over time. The American Lung Association’s silicosis resources provide additional patient-facing guidance for workers navigating their diagnosis.
How to Prevent Silicosis: Workplace Controls and Regulatory Requirements
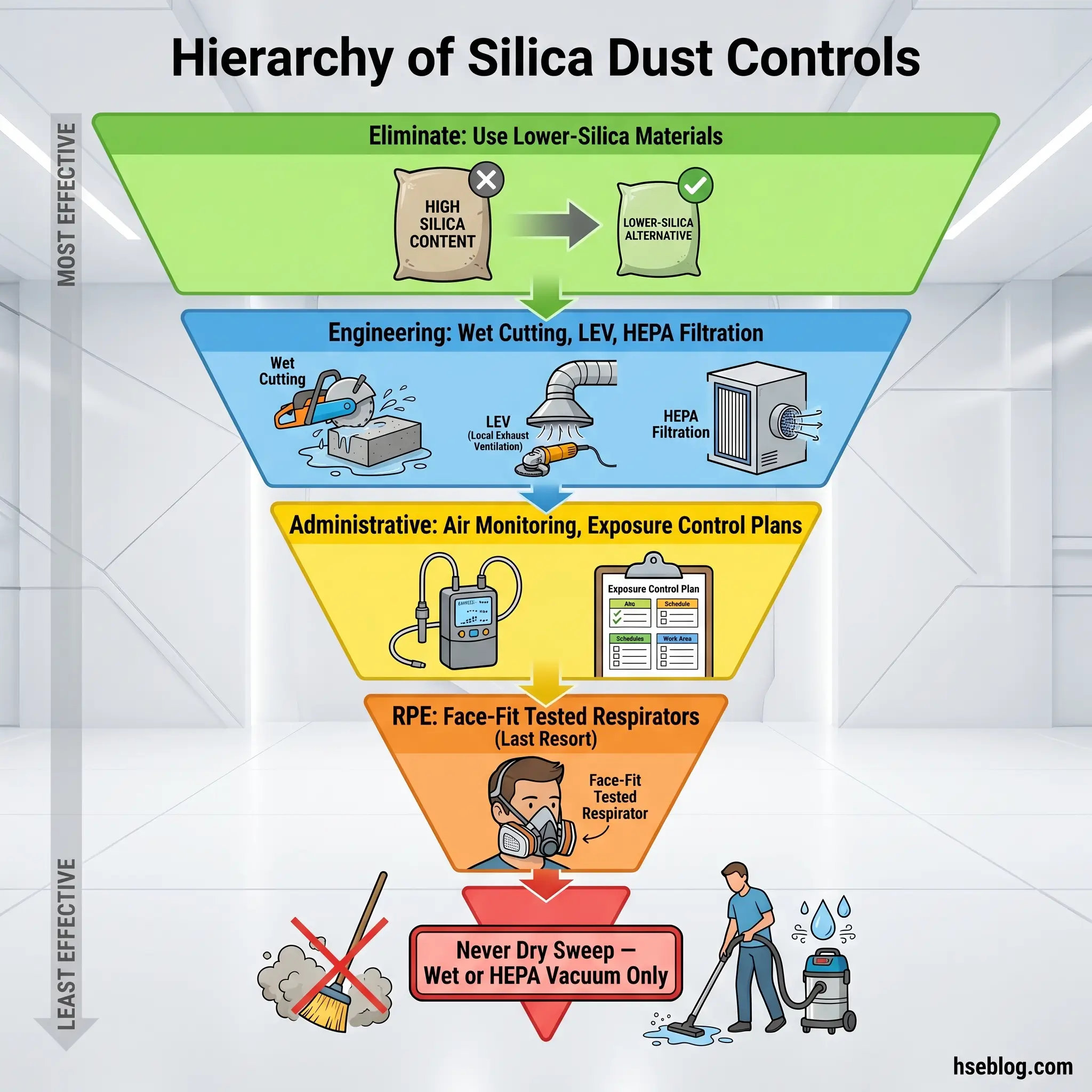
Prevention is the only effective response to silicosis, because treatment cannot undo the damage. The hierarchy of controls — the organising principle for hazard management in every major regulatory jurisdiction — provides the structure for building a silica dust control programme that actually works. The common failure mode observed across sites is not the absence of controls at initial setup but the degradation of controls over time: water feed rates drop below effective suppression levels, HEPA filters clog without scheduled replacement, RPE fit-testing lapses after the initial round. Prevention demands a maintenance culture, not just an equipment purchase order.
Elimination and substitution sit at the top of the hierarchy and offer the most reliable protection. Where feasible, specifying materials with lower crystalline silica content removes the hazard at the design stage. Australia’s engineered stone ban represents the most aggressive application of elimination — removing a material from the market entirely because it could not be worked safely under typical fabrication conditions.
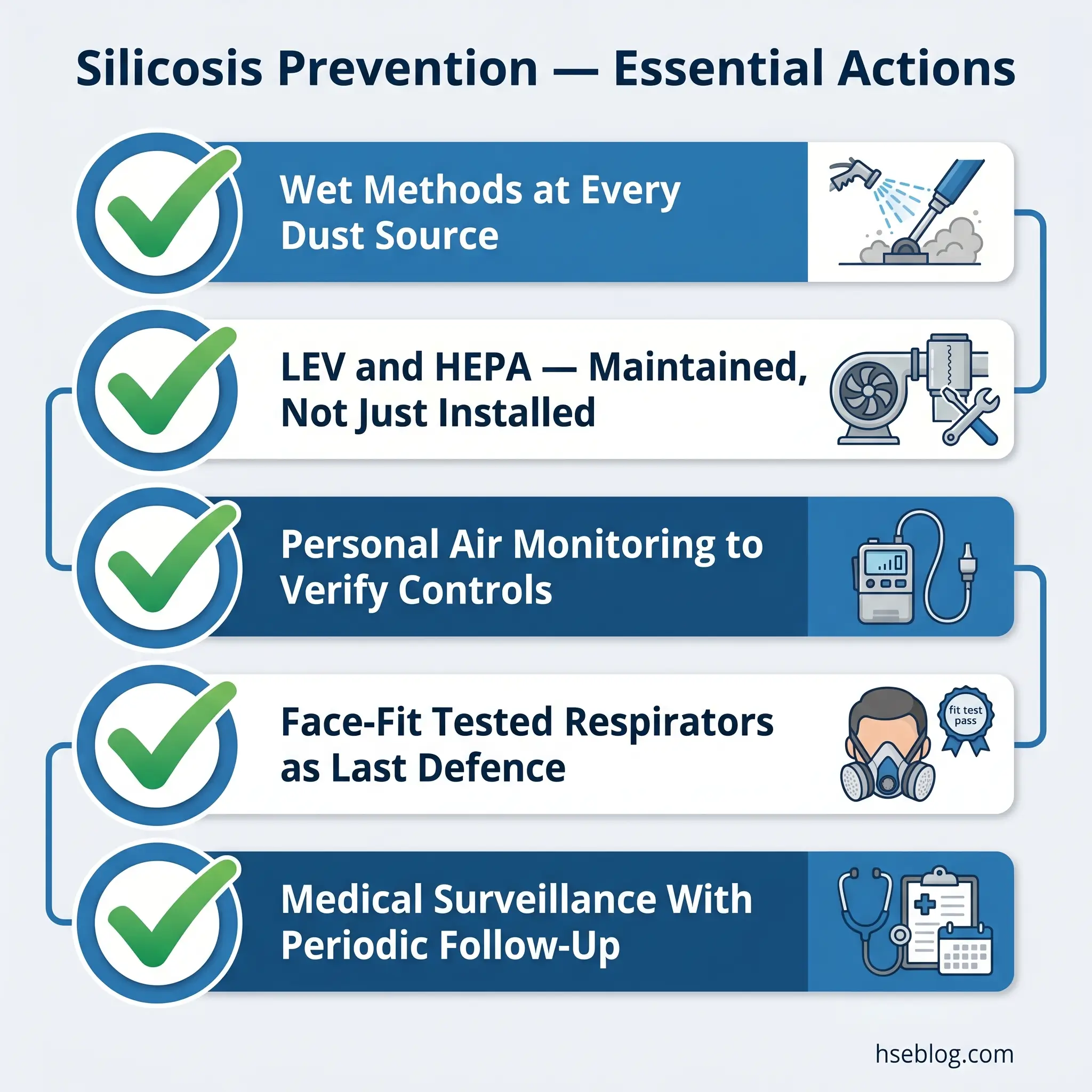
Engineering controls are the primary defence for operations where silica-containing materials must be worked. Wet cutting and drilling suppress dust at the point of generation by binding airborne particles to water — but the water supply must be continuous and at sufficient flow rate, not a trickle from a bottle. Local exhaust ventilation (LEV) with HEPA filtration captures dust at the source before it disperses into the breathing zone. Enclosed operator cabs and process booths isolate the worker from the dust-generating activity. Dust collection systems with properly maintained filters complete the engineering picture. NIOSH’s safe work practices for silica provide detailed engineering control guidance for specific operations.
Administrative controls complement engineering measures. Exposure monitoring — personal air sampling with gravimetric analysis — quantifies actual worker exposure against regulatory limits and verifies that engineering controls are performing as intended. Written exposure control plans document the controls in place, assign responsibilities, and schedule monitoring and maintenance. Job rotation to limit individual cumulative exposure has a role, though it is worth noting that California’s 2025 permanent silica regulation under Cal/OSHA §5204 has explicitly prohibited rotation as a sole control method — rotation may supplement engineering controls but cannot substitute for them. Restricted access zones prevent unprotected workers from entering high-exposure areas.
Respiratory protective equipment (RPE) is the last line of defence — not the first. When engineering and administrative controls cannot reduce exposure below the applicable limit, RPE bridges the gap. For brief, low-concentration tasks, a minimum of N95 (US) or FFP2 (EU/UK) particulate filtering facepiece is required. For sustained exposure or higher concentrations, a half-mask respirator with P3 particulate filters (assigned protection factor of 20) or a powered air-purifying respirator (PAPR, APF 40+) provides the necessary protection level. Cal/OSHA’s 2025 permanent rule mandates PAPR as the minimum for engineered stone fabrication. Every respirator must be face-fit tested to the individual wearer — an improperly fitted respirator provides significantly less protection than its rated APF.
Housekeeping is the control most often neglected and most consequential when it fails. Settled silica dust is a secondary exposure source — any disturbance re-aerosolises it. Wet sweeping or HEPA-filtered vacuum cleaning are the only acceptable methods. Dry sweeping and compressed air blowdown are prohibited in every major regulatory jurisdiction because they generate airborne concentrations that can exceed the PEL within seconds.
Audit Point: During site audits, the most revealing test of a silica control programme is not the presence of equipment but its condition. Check water flow rates, LEV capture velocity at the hood face, HEPA filter change logs, and RPE fit-test records. Controls that existed on the purchase order but have degraded since installation are functionally absent.
Exposure Limits: OSHA, HSE UK, and International Standards Compared
Regulatory exposure limits for respirable crystalline silica vary by jurisdiction, and the differences are not merely numerical — they reflect different regulatory philosophies that produce different compliance outcomes in practice.
| Jurisdiction | Standard | Limit (8-hr TWA) | Key Note |
|---|---|---|---|
| US (OSHA) | 29 CFR 1926.1153 / 1910.1053 | 50 µg/m³ PEL; 25 µg/m³ Action Level | Triggers medical surveillance and controls at Action Level |
| UK (HSE) | EH40/2005 under COSHH | 100 µg/m³ WEL | ALARP duty requires reduction below WEL as far as practicable |
| ACGIH | TLV | 25 µg/m³ | Strictest commonly referenced limit |
| EU | Directive 2017/2398 | 50 µg/m³ (indicative OEL) | Member states may adopt stricter limits |
The UK WEL of 100 µg/m³ is numerically double the US OSHA PEL of 50 µg/m³, which might suggest less stringent protection. The practical interpretation is more nuanced. Under the Control of Substances Hazardous to Health Regulations 2002, UK employers have an explicit duty to reduce exposure as low as reasonably practicable (ALARP) — not merely to comply with the WEL as a ceiling. RCS is classified under EH40 as capable of causing cancer and heritable genetic damage, which tightens the ALARP obligation further. A UK employer who achieves 99 µg/m³ and considers that “compliant” misreads the legal framework.
The ACGIH Threshold Limit Value of 25 µg/m³ is the strictest commonly referenced standard and represents the science-driven recommendation unencumbered by economic feasibility considerations that shape regulatory PELs. Where practitioners have the latitude to specify a target, the ACGIH TLV is the benchmark that provides the greatest margin of safety.
The operational recommendation across jurisdictions: identify the strictest applicable limit for the reader’s regulatory environment and treat it as a target, not a ceiling. Exposure should be driven as far below any limit as controls can achieve.
Medical Surveillance and Health Monitoring
Exposure limits and engineering controls prevent disease. Medical surveillance detects it early enough to intervene before irreversible damage progresses to disability or death. Both sides of the equation must function — controls without surveillance leave early disease undetected; surveillance without controls amounts to documenting avoidable harm.
Under OSHA 29 CFR 1926.1153 and 1910.1053, employers must provide medical examinations — including chest X-ray and spirometry — within 30 days of initial assignment and every three years thereafter for workers exposed above the Action Level or required to wear respirators for 30 or more days per year. The examination must include a medical and work history emphasising past silica,ite, and dust exposures.
UK requirements under COSHH mandate health surveillance for workers exposed to RCS above levels where disease is reasonably foreseeable. This typically includes respiratory symptom questionnaires, spirometry, and chest X-rays at intervals determined by the occupational health provider, with reference to HSE guidance on COSHH health surveillance.
Australia, post-2024, has implemented enhanced requirements. Silica Risk Control Plans are mandatory for all work involving materials containing 1% or more crystalline silica. Air monitoring and health monitoring — including chest X-rays and spirometry — are required for all workers carrying out crystalline silica tasks.
Cal/OSHA’s 2025 permanent regulation under Title 8 CCR §5204 introduced 24-hour mandatory reporting of confirmed silicosis cases by employers, initial and periodic medical examinations, and authorised immediate Orders Prohibiting Use (stop-work orders) where violations create imminent silicosis risk.
Medical surveillance programmes only deliver value when they are actually completed. The consistent failure mode is conducting baseline screening when a worker is first assigned to silica work but neglecting the periodic follow-up examinations that detect early disease progression. A baseline with no follow-up is a legal record, not a health protection programme.
Jurisdiction Note: Medical surveillance trigger points and examination intervals vary across OSHA, HSE UK, and Australian standards. Multinational operations must comply with the specific requirements of each jurisdiction in which workers are exposed — defaulting to the most conservative schedule is the most defensible approach.
What Is the Engineered Stone Silicosis Crisis?
Engineered stone — also marketed as artificial quartz, composite stone, or reconstituted stone — entered the residential and commercial construction market aggressively from the early 2000s, promoted for its uniform appearance, durability, and competitive pricing against natural granite and marble. The material is manufactured by binding crushed quartz with polymer resins, producing a product that typically contains more than 90% crystalline silica — roughly double to quadruple the silica concentration of natural granite.
The health consequences emerged on a timeline that occupational health professionals recognise from previous industrial disease outbreaks: a new material achieves widespread commercial adoption before its occupational health risk profile is characterised or controlled, and by the time the clinical and epidemiological evidence mounts, a generation of workers has already accumulated damaging exposure. Engineered stone fabrication workers — cutting, grinding, edge-profiling, and polishing countertops — were exposed to airborne RCS concentrations that, in the absence of wet methods and ventilation, routinely exceeded regulatory limits by multiples.
The Australian experience crystallised the crisis. Clusters of accelerated silicosis began appearing in young engineered stone fabrication workers — many under 35, many from immigrant and linguistically diverse communities. The cases were severe, rapidly progressive, and occurring after fewer than 10 years of exposure. Safe Work Australia determined that engineered stone could not be safely fabricated under typical workplace conditions and implemented the world’s first national ban on the manufacture, supply, processing, and installation of engineered stone benchtops, panels, and slabs, effective 1 July 2024, with an import ban from 1 January 2025. Enhanced regulations for all work with materials containing 1% or more crystalline silica came into force 1 September 2024.
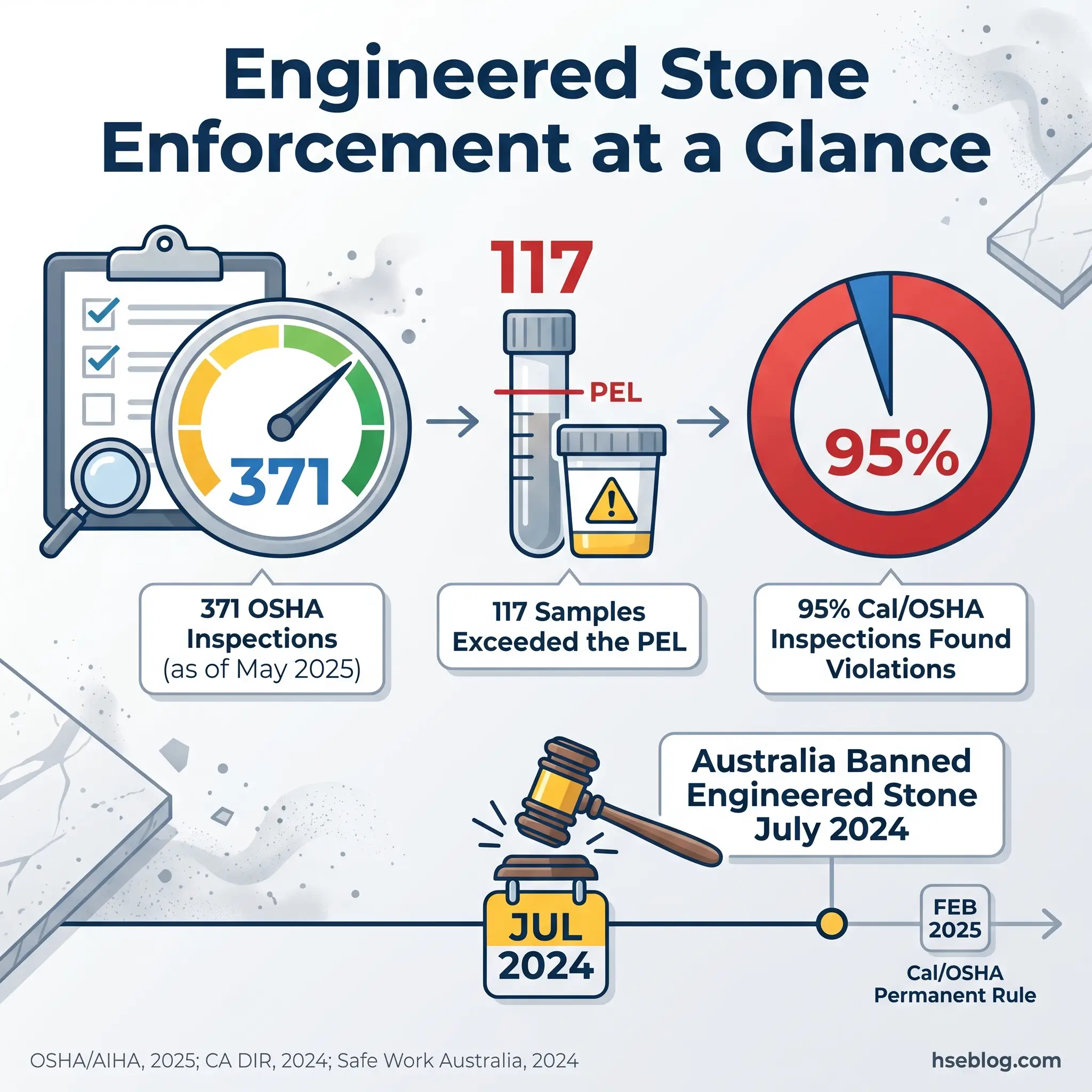
In the United States, federal OSHA launched a focused enforcement initiative targeting engineered stone fabrication shops in September 2023. As of May 2025, this initiative had conducted 371 inspections and collected 574 silica air samples. Of those samples, 117 exceeded the PEL — including 22 at five times the PEL and 6 at ten times the PEL (OSHA Office of Health Enforcement, AIHA Connect 2025). An estimated 3,600 to 7,300 new silicosis cases are recognised annually in the US (Silica-Safe.org), though significant underreporting is acknowledged.
California moved further and faster than federal OSHA. Cal/OSHA adopted a permanent respirable crystalline silica regulation (Title 8 CCR §5204, effective February 2025) that prohibits dry fabrication of engineered stone, mandates 24-hour reporting of confirmed silicosis cases, requires Silica Risk Control Plans, and authorises immediate stop-work orders. Enforcement has been aggressive: 95% of Cal/OSHA’s closed silica inspections resulted in violations — 53 of 56 inspections over the first 12 months (California Department of Industrial Relations, 2024).
The engineered stone crisis illustrates a pattern recognisable across the history of occupational disease: commercial adoption outpaces hazard characterisation, regulation responds reactively, and a generation of workers pays the price in the interval. Whether it justifies the label “the asbestos of the 2020s” — as the Australian construction union has described it — depends on the regulatory response’s speed. The bans and enforcement escalations of 2024–2025 represent a faster regulatory response than the decades-long asbestos delay, but for the workers already diagnosed, the distinction is academic.
Frequently Asked Questions
Conclusion
Silicosis is not a relic of industrial history. It is a present-tense disease — killing more than 12,900 people globally in 2019, disabling young countertop fabricators who had no idea what they were breathing, and prompting the first national material ban of this century. The lungs do not recover from silica scarring. Every case diagnosed is a case that should have been prevented.
The clinical reality of silicosis — irreversible, progressive, untreatable — makes prevention the only strategy that matters. Not prevention in the abstract, as a word on a policy document, but prevention as a daily operational discipline: water flowing at the cutting point, LEV systems capturing dust at the hood face, HEPA filters changed on schedule, air monitoring confirming that what the engineering controls promise is what the worker’s breathing zone actually receives, and medical surveillance programmes that follow through on periodic examinations rather than stopping after baseline. The gap between equipment purchased and equipment maintained is the gap where silicosis cases are created.
For every HSE professional reading this, the question is specific: do you know what your workers’ actual RCS exposure is today — measured, not estimated? If the answer is uncertain, the first action is personal air sampling with a cyclone sampler and gravimetric analysis against the strictest applicable limit for your jurisdiction. Everything that follows — controls selection, RPE specification, medical surveillance scheduling — depends on that number. Silicosis is a disease of known cause, known mechanism, and known prevention. The knowledge exists. The obligation is to apply it.