
TL;DR — The Numbers That Define the Hazard
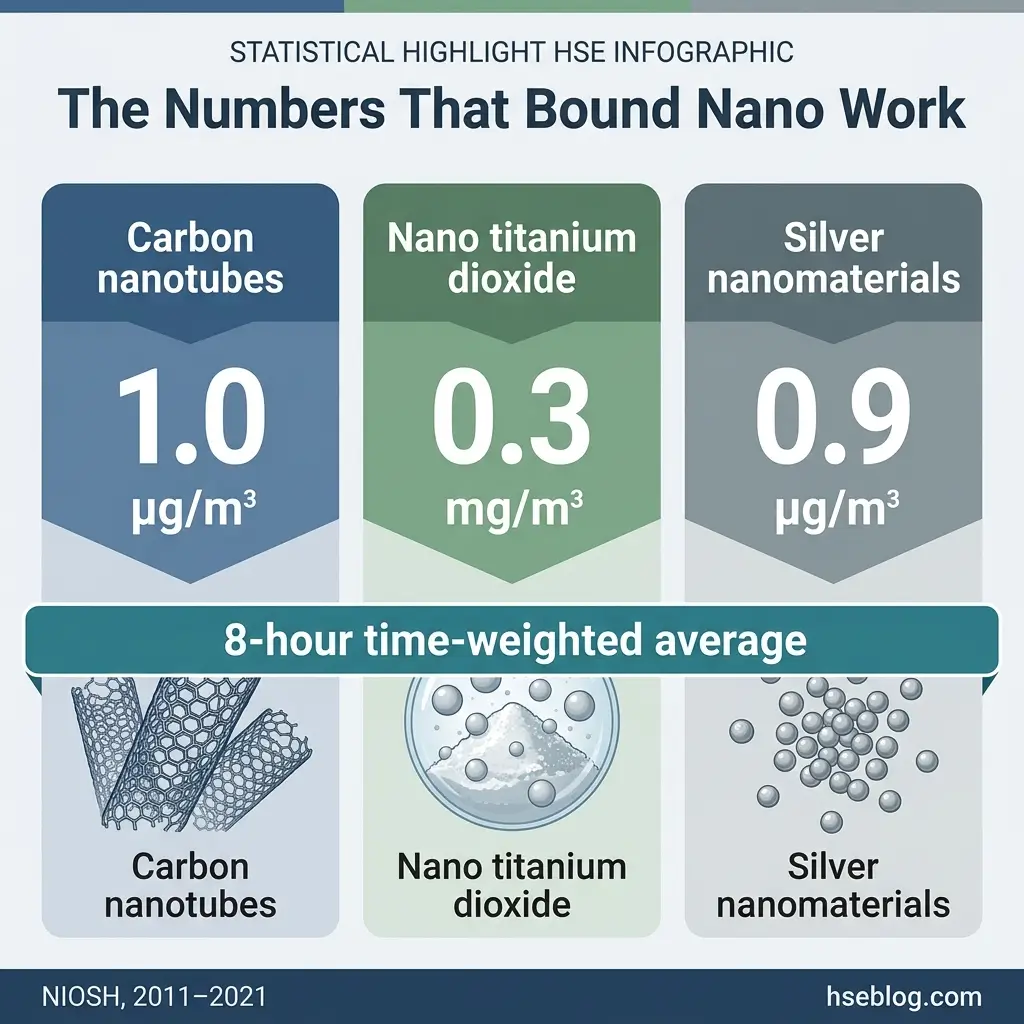
- 1.0 µg/m³ — NIOSH recommended exposure limit for respirable carbon nanotubes and nanofibres, as an 8-hour time-weighted average (NIOSH CIB 65, 2013).
- 0.3 mg/m³ — NIOSH REL for nanoscale titanium dioxide, classed a potential occupational carcinogen; the bulk form sits eight times higher at 2.4 mg/m³ (NIOSH CIB 63, 2011).
- 0.9 µg/m³ — NIOSH REL for silver nanomaterials under 100 nm, far below the 10 µg/m³ limit for total silver (NIOSH CIB 70, 2021).
- Group 2B — IARC classification of one rigid carbon nanotube, MWCNT-7, as possibly carcinogenic to humans (IARC, 2014).
Nanoparticle exposure occurs when particles between 1 and 100 nanometres enter the body — chiefly by inhalation into the deep lung, and secondarily through skin and ingestion. Their small size and large surface area drive oxidative stress, inflammation, and movement to distant organs, producing health effects the bulk form of the same material does not.
Titanium dioxide is an ordinary white pigment, used in paint, paper, and sunscreen and handled in bulk for over a century. Grind the same compound below 100 nanometres and its behaviour changes: the nanoscale form carries enough extra surface reactivity that NIOSH now classifies it as a potential occupational carcinogen by inhalation (NIOSH CIB 63, 2011).
That shift — a familiar substance turning hazardous purely because of particle size — sits at the centre of nanoparticle exposure. This article maps how engineered nanomaterials enter the body, why they spread beyond the point of contact, the health effects recorded across the toxicological literature, and the occupational exposure limits that now bound this work.
What Counts as Nanoparticle Exposure — and Why Size Rewrites the Risk
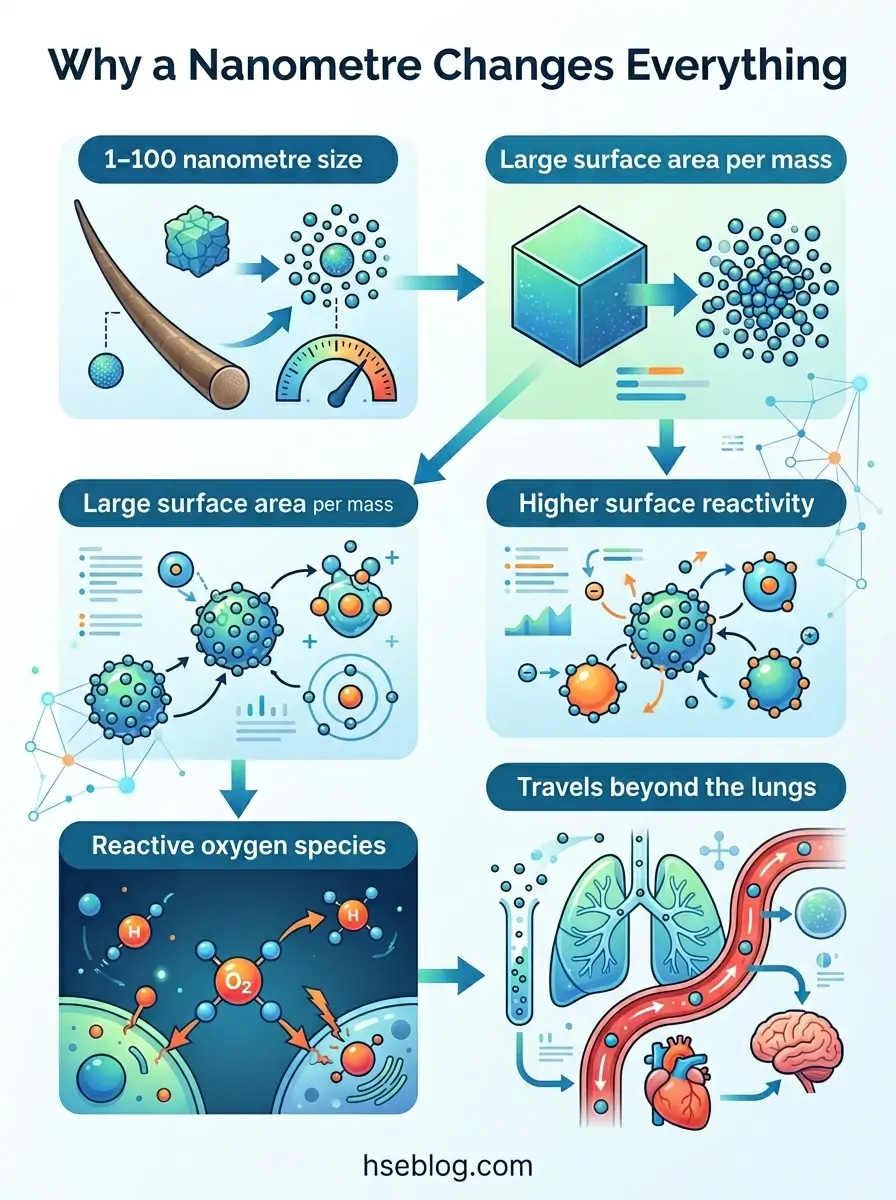
A nanoparticle is any particle with at least one dimension between 1 and 100 nanometres, and at that scale the same chemistry produces a different hazard. The cause is geometry, not novelty.
When a fixed mass of material is divided into ever-smaller particles, a far greater share of its atoms ends up on the surface. That surface is where chemical and biological reactions happen.
The surface-area effect
A larger reactive surface per unit mass means more catalytic activity and more generation of reactive oxygen species inside cells. This oxidative stress is a recurring driver of inflammation and cellular damage across the nanotoxicology literature.
The properties that make engineered nanomaterials commercially useful are the same ones that make them biologically active:
- High surface-area-to-mass ratio — more reactive surface per gram, so a tiny mass can carry large biological potency.
- Particle shape — fibres, tubes, and plates behave differently from compact spheres, and shape strongly influences toxicity.
- Biopersistence — durable particles that resist dissolution and clearance stay in tissue and keep provoking a response.
- Surface chemistry — coatings and functional groups change how a particle interacts with cells and whether it clumps or stays dispersed.
Why bulk exposure limits don’t transfer
The most important practical point is one that OSHA states plainly: existing exposure limits for a substance may not protect against the nanoparticle form of that same substance, because the nanoscale particles can be more hazardous (OSHA, 2013). Treating a nanomaterial as if the dust limit for its bulk powder applies is one of the more common and dangerous assumptions I see in early-stage risk assessments.
The Four Routes of Entry: How Nanoparticles Reach the Body
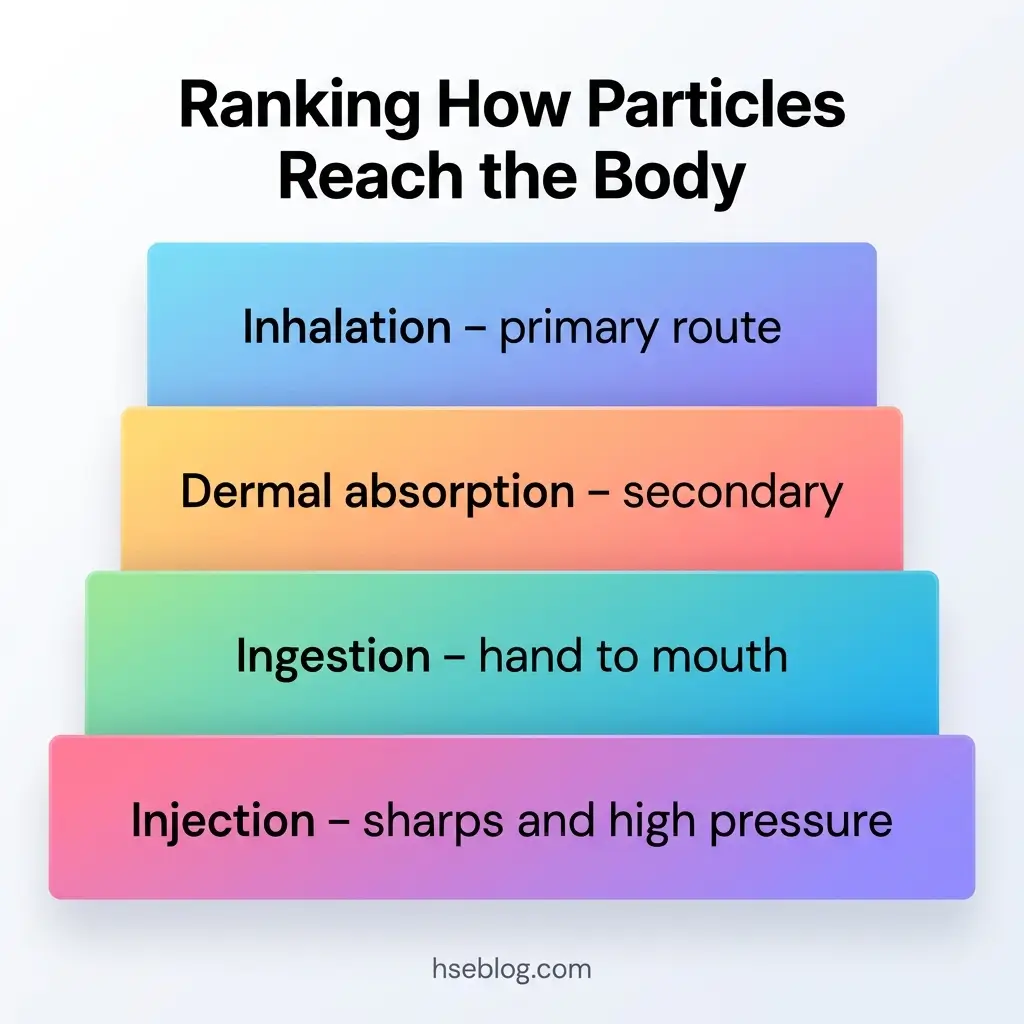
Inhalation dominates occupational nanoparticle exposure, with skin absorption and ingestion as secondary routes and injection a niche risk (Health Canada, 2026). Mapping the route matters because the route determines which organs receive the dose first and which controls actually work.
| Route of entry | How it happens | First targets | Practical relevance |
|---|---|---|---|
| Inhalation | Airborne particles drawn into the airways during weighing, mixing, sonication, or cleanup | Nasal passages, airways, alveoli | The primary occupational route; deep enough to deposit in gas-exchange tissue |
| Dermal absorption | Contact with powders, sprays, or suspensions; entry via skin and eyes, easier through broken skin | Skin, eyes | Underestimated, and the dominant route for nano-enabled personal-care products |
| Ingestion | Hand-to-mouth transfer from contaminated hands, surfaces, food, or drink | Gastrointestinal tract | Driven by hygiene failures; controllable with handwashing and clean-eating-area discipline |
| Injection | Accidental needle-stick or high-pressure equipment forcing material through skin | Bloodstream directly | Rare, but bypasses every external barrier in one step |
The headline is that inhalation reaches the part of the lung built for absorption. The human lung presents a vast internal surface area to the outside air, which makes it both the main gateway and the primary target organ for inhaled nanoparticles.
A point auditors increasingly test: the dermal route is real, not theoretical. For nano-enabled cosmetics and coatings, skin contact is the leading exposure pathway, which is why glove selection and splash protection belong in the assessment alongside respiratory controls.
Why Nanoparticles Don’t Stay Put: Translocation Through the Body
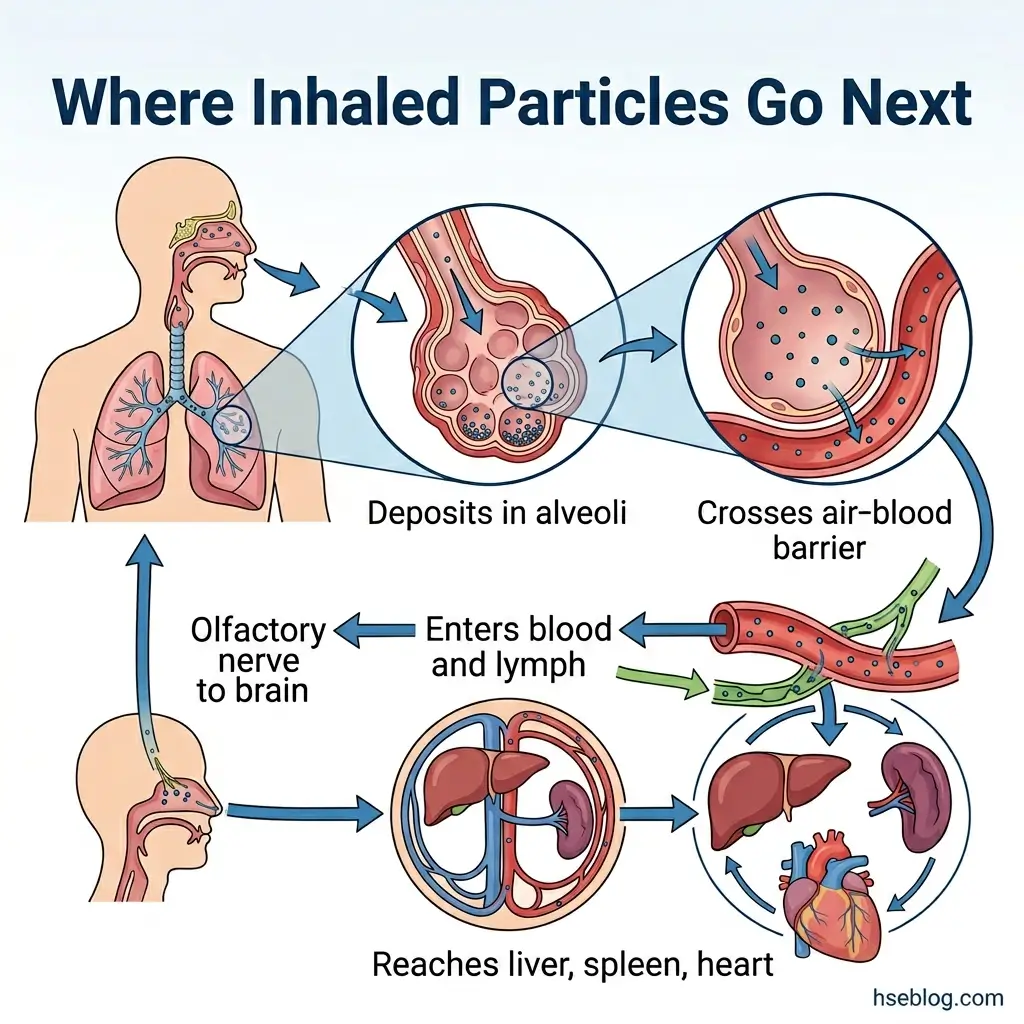
The lung is the entry point, not the destination — and that is what separates nanoparticle exposure from ordinary dust exposure. Once particles deposit in the alveoli, their size lets them cross barriers that stop larger particles.
From the deep lung, nanoparticles can move into the circulatory and lymphatic systems and reach tissues and organs throughout the body (NIOSH, 2009). This biodistribution is the mechanism behind effects seen far from the site of contact.
The published toxicology shows a consistent pattern of spread:
- Into the bloodstream and lymph — particles cross the air–blood barrier and circulate, with controlled human inhalation studies confirming that inhaled nanoparticles can enter the circulation.
- Into solid organs — animal inhalation studies of silver nanomaterials found raised silver concentrations in every organ tested, evidence that distribution is body-wide, not lung-limited (NIOSH CIB 70, 2021).
- Along the olfactory nerve to the brain — in two-year inhalation studies, rigid carbon nanotubes were recovered from the olfactory bulb and brain, a nose-to-brain route that sidesteps the bloodstream entirely (published rat inhalation studies, peer-reviewed).
- Into the pleural space — fibre-shaped nanomaterials can migrate from the alveoli to the lining of the lung, the tissue central to asbestos disease.
The judgment point for a practitioner is that “contained to the lungs” is the wrong mental model. Where a material is biopersistent, the relevant question is not only what the airway can tolerate, but what the liver, heart, and pleura accumulate over a working lifetime.
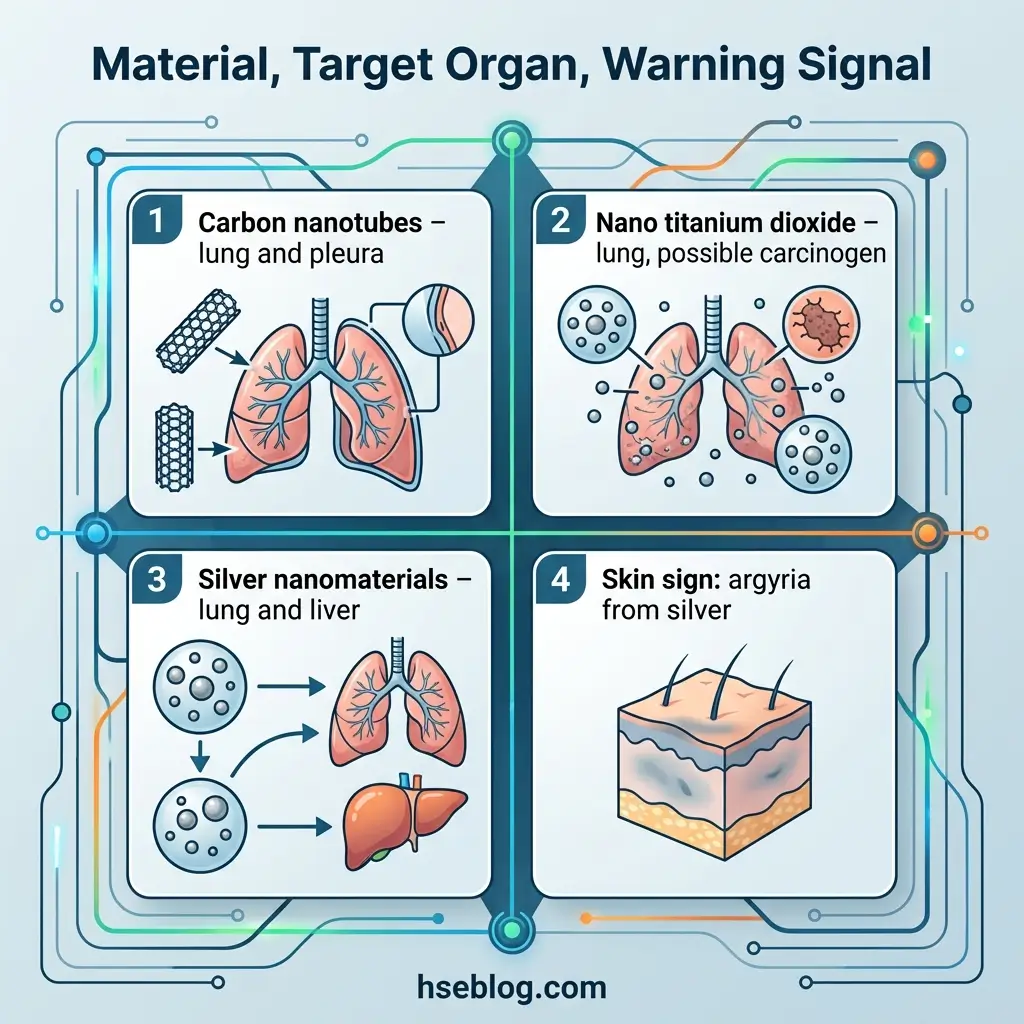
Health Effects of Nanoparticle Exposure, by Material and Target Organ
The recorded health effects track the material and the route rather than a single “nano” syndrome — carbon nanotubes, titanium dioxide, and silver each carry their own signal. The strongest evidence comes from animal and cellular studies, with human epidemiology still limited because workplace nano exposure is hard to separate from background ultrafine particles.
This content covering nanoparticle exposure and health effects is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms or exposure concerns should consult an occupational physician or qualified medical professional.
Respiratory effects: inflammation, fibrosis, and the fibre question
Certain inhaled nanoparticles deposit in the respiratory tract and cause inflammation and damage to lung cells; carbon nanotubes and nanofibres specifically can produce pulmonary inflammation and fibrosis (OSHA, 2013). Fibrosis is scarring that permanently stiffens lung tissue and reduces gas exchange.
The more serious concern attaches to high-aspect-ratio nanomaterials — long, thin, rigid, durable fibres such as some carbon nanotubes. Decades of asbestos research produced the fibre pathogenicity paradigm, which holds that length, thinness, rigidity, and biopersistence determine whether an inhaled fibre causes pleural disease, including mesothelioma.
That paradigm now extends to nanotubes. When a fibre is too long and rigid for a macrophage to engulf, the cell undergoes “frustrated phagocytosis,” sustaining chronic inflammation while the fibre persists at the pleura. On this evidence, IARC classified the rigid nanotube MWCNT-7 as possibly carcinogenic to humans (Group 2B) in 2014, while leaving other nanotube types unclassified for want of sufficient evidence (IARC, 2014). The interpretation that matters operationally: not all carbon nanotubes are equal, and shape and rigidity — not chemistry alone — should drive how tightly a given product is controlled.
Systemic and organ effects
Because nanoparticles distribute body-wide, effects appear beyond the lung:
- Liver — inhaled silver nanomaterials produced bile duct hyperplasia alongside early lung inflammation in rats (NIOSH CIB 70, 2021).
- Cardiovascular system — circulating ultrafine and nanoscale particles are associated in the broader literature with cardiovascular stress, with particle size strongly influencing the response.
- Cell and DNA damage — in human-cell studies, silver nanomaterials caused size-dependent cytotoxicity and DNA damage (NIOSH CIB 70, 2021).
Skin: the argyria example
Silver nanomaterials illustrate that not every effect is hidden internally. Prolonged silver exposure can cause argyria, a permanent blue-grey discolouration of the skin and eyes — a visible, irreversible marker that exposure controls have failed over time.
Occupational Exposure Limits for Nanomaterials: Reading the Numbers
NIOSH has issued material-specific recommended exposure limits (RELs) for the most studied engineered nanomaterials, and the figures sit far below the limits for the bulk forms. These RELs are the practical backbone of nanoparticle exposure assessment in the United States.
| Nanomaterial | NIOSH REL | Averaging basis | Source / jurisdiction |
|---|---|---|---|
| Carbon nanotubes & nanofibres | 1.0 µg/m³ (respirable elemental carbon) | 8-hour TWA | NIOSH CIB 65, 2013 — US |
| Titanium dioxide (nanoscale, <100 nm) | 0.3 mg/m³ — potential occupational carcinogen | 8-hour TWA | NIOSH CIB 63, 2011 — US |
| Titanium dioxide (fine, >100 nm) | 2.4 mg/m³ | 8-hour TWA | NIOSH CIB 63, 2011 — US |
| Silver nanomaterials (<100 nm) | 0.9 µg/m³ (respirable) | 8-hour TWA | NIOSH CIB 70, 2021 — US |
| Total silver (dust, fume, soluble) | 10 µg/m³ | 8-hour TWA | NIOSH — US |
Two things in this table carry the lesson. The nanoscale titanium dioxide limit is set eight times tighter than the bulk limit for the identical compound, and the silver-nanomaterial limit is roughly eleven times tighter than the total-silver limit.
A jurisdictional distinction matters here. NIOSH RELs are recommendations, not law, whereas OSHA permissible exposure limits are enforceable — and OSHA has not set a nano-specific PEL, instead recommending employers follow the NIOSH figures and relying on the General Duty Clause, Section 5(a)(1), to require a safe workplace (OSHA, 2013).
The European Union takes a different route — exposure-limit-light but registration-heavy. Since 1 January 2020, amended REACH annexes require companies that manufacture or import nanoforms to submit nanoform-specific hazard and characterisation data to ECHA, and the EU revised its formal definition of a nanomaterial in 2022 (ECHA, 2020).
There is also a measurement trap built into these limits. NIOSH itself flagged in CIB 65 that a mass-based sampling method may miss nanostructures present at very low mass — meaning a reassuring milligram reading can coincide with a high particle count. The applied reading is that mass alone is an incomplete metric, and surface-area or particle-number monitoring is often the more honest measure of nanoparticle exposure.
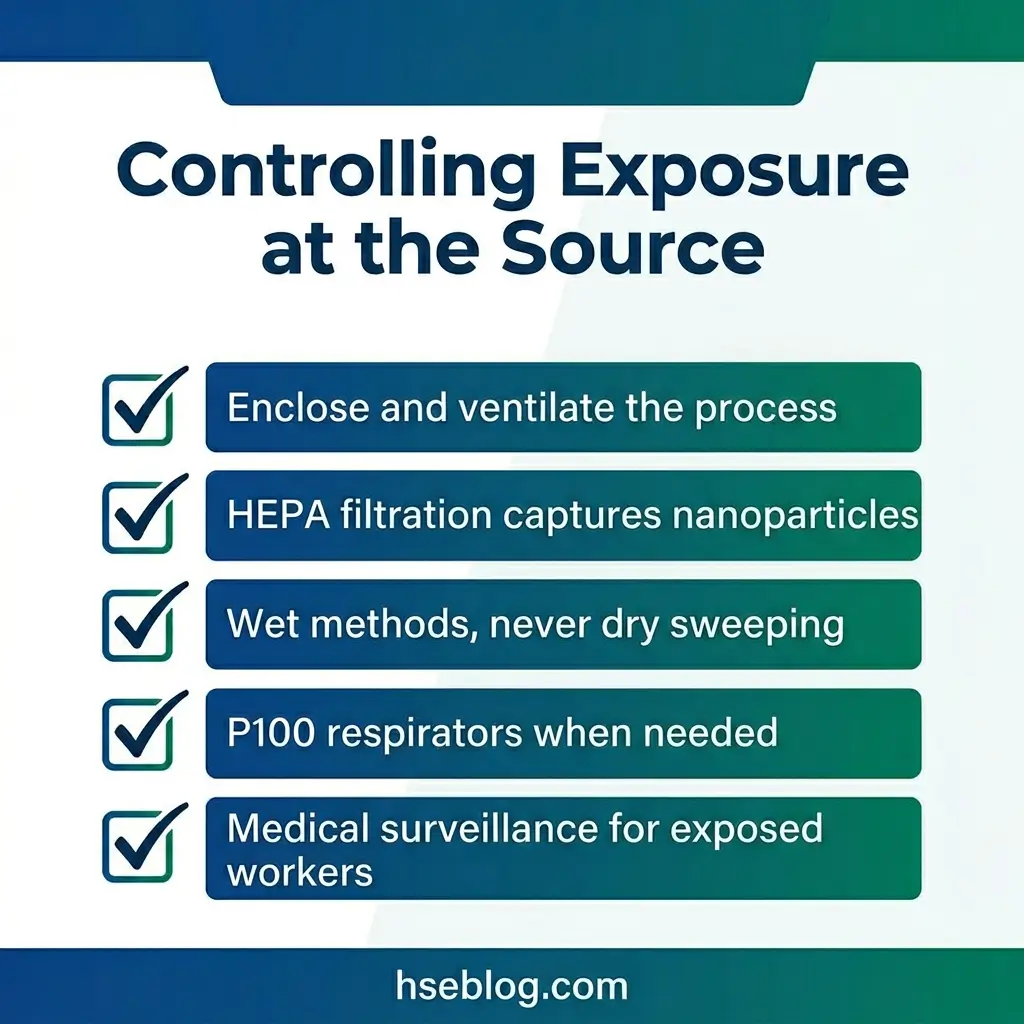
Controlling Nanoparticle Exposure on Site
Controlling nanoparticle exposure begins with keeping the material out of the air and off the worker, in that order. The good news from the engineering side is that conventional high-grade filtration works: HEPA media traps at least 99.97% of 0.3-micrometre particles, and NIOSH research indicates such filters effectively remove nanoparticles too (OSHA, 2013).
A defensible control programme runs roughly in this sequence:
- Enclose the process. Handle nanomaterials in ventilated enclosures such as glove boxes, fume hoods, or process chambers fitted with HEPA filtration, so the particles never reach the breathing zone.
- Capture at the source. Where full enclosure is impossible, install local exhaust ventilation with a capture hood at the exact point of generation or release.
- Eliminate dust-raising cleanup. Prohibit dry sweeping and compressed air, which re-aerosolise settled particles; use wet wiping and HEPA-filtered vacuums instead.
- Use the right respiratory protection. Where airborne exposure remains, use HEPA-filter air-purifying respirators — the N100, R100, or P100 class — selected and fit-tested under a respiratory protection programme to 29 CFR 1910.134 (US).
- Protect skin and eyes. Provide appropriate gloves and protective clothing for the dermal and ocular routes, which are easy to overlook once respiratory controls feel handled.
- Run exposure assessment and medical surveillance. Characterise tasks, sample the air with a metric suited to nanoparticles, and make established medical surveillance available to potentially exposed workers.
The freshest direction in this field is methodological. As the NIOSH Nanotechnology Research Centre marked its twentieth anniversary, NIOSH described continuing work on grouping and hazard-banding schemes — sorting nanomaterials by solubility, biopersistence, surface reactivity, and aspect ratio so that controls can be set even where a material-specific REL does not yet exist (NIOSH Science Blog, June 2024). For sites handling materials without a published limit, that banding logic is the most practical interim basis for deciding how tightly to contain.
Frequently Asked Questions
What the Industry Still Gets Wrong
The persistent error in nanoparticle exposure management is treating the nanoform like the bulk material. A compound that has been handled safely as a powder for decades can become a different hazard once it drops below 100 nanometres, with a tighter exposure limit, a deeper reach into the lung, and the capacity to travel to organs the dust never touched.
If there is one change with the highest payoff, it is this: stop assuming the dust limit protects against the nanoparticle, and start treating particle shape, biopersistence, and surface area as primary risk variables rather than footnotes. The fibre pathogenicity paradigm earned through asbestos research is the clearest warning — long, rigid, durable fibres deserve the strictest containment, whatever they are made of, and the cost of getting that judgement wrong is measured in decades-latency disease, not lost time.
The materials will keep arriving on site faster than dedicated limits can be written. Sound practice is to contain aggressively where the data is thin, measure with a metric that actually sees nanoparticles, and let the hazard-banding logic stand in until a specific number exists — because the worker handling tomorrow’s nanomaterial is, as NIOSH puts it, among the first to be exposed to it.