

TL;DR — The Numbers That Define This Hazard
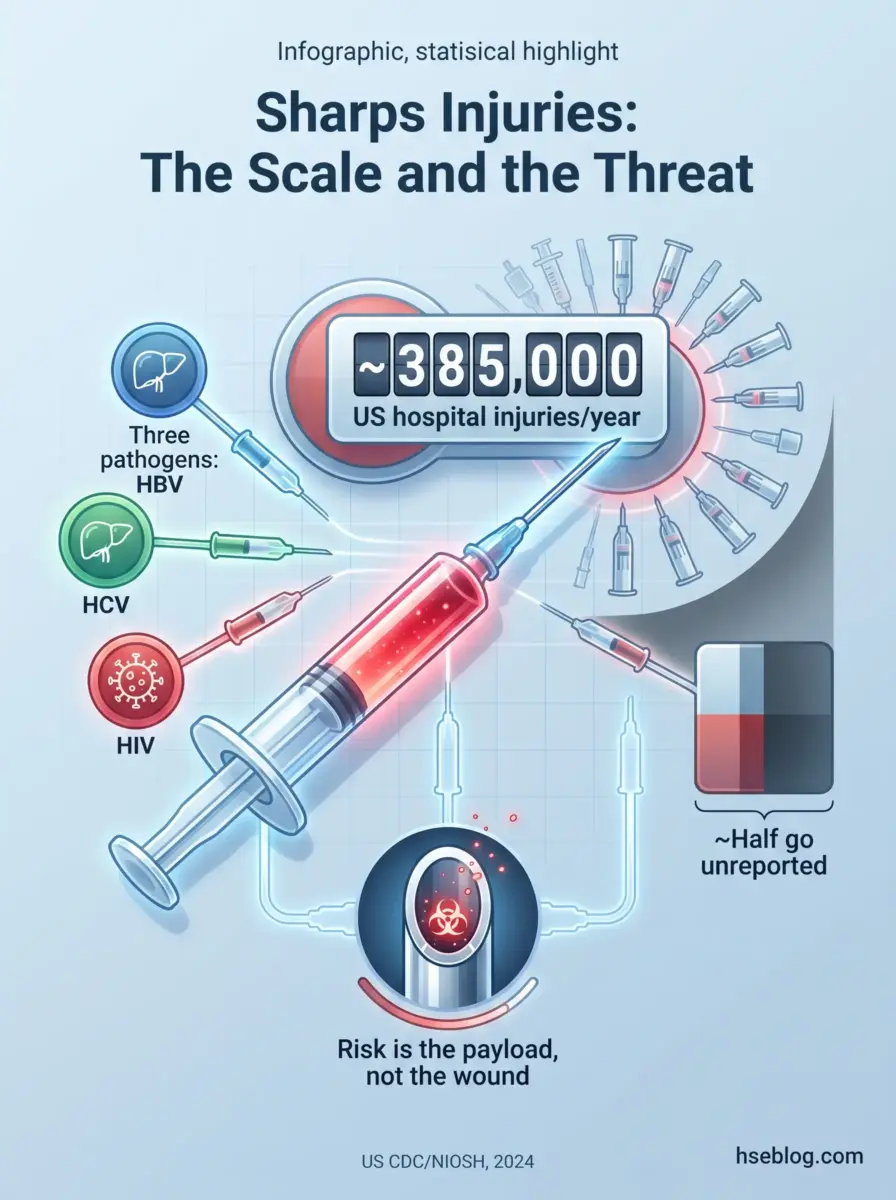
- ~385,000 hospital sharps injuries a year in the US alone, and that figure excludes the unreported ones (US CDC/NIOSH, page updated 2024).
- HIV ~0.3%, HCV ~1.8%, HBV up to ~30% transmission risk per percutaneous exposure to an infected source — the HBV figure applying to an unvaccinated worker exposed to a highly infectious source (US CDC/OSHA).
- 62–88% of sharps injuries are preventable with safer-engineered devices, so most of this harm is a design and training problem, not bad luck (US CDC, cited by OSHA).
- Around half or more go unreported, which means injury logs systematically understate true exposure (US CDC/NIOSH).
- HIV PEP works best started within hours, with a commonly cited outer window of ~72 hours — a clinician-led decision, not a self-administered one.
After a needlestick injury, wash the wound with soap and running water and let it bleed gently — never squeeze it. Report the incident immediately and seek medical evaluation within hours, not days. A clinician assesses the source and the exposure and may start HIV post-exposure prophylaxis (PEP) as soon as possible, ideally well inside 72 hours.
The number that should unsettle anyone managing a sharps program is ~385,000 — the sharps injuries sustained by hospital-based healthcare personnel in the US each year (US CDC/NIOSH, page updated 2024). That count only captures hospitals, and only the injuries someone bothered to record. Behind each one sits a worker waiting weeks to learn whether a hollow-bore needle delivered a virus along with a puncture.
Needlestick injuries are dangerous not because of the wound but because of the biological payload it can carry. This article merges what the clinical references, the regulators, and the vendor blogs each cover in isolation: prevention through the hierarchy of controls, the immediate step-by-step protocol after an exposure, post-exposure prophylaxis and medical follow-up reflecting the 2025 US PHS update, and the employer obligations that differ across the US, UK, and EU.
What Is a Needlestick Injury and Why It’s a Serious Occupational Hazard
A needlestick injury is a percutaneous injury — the skin is pierced by a contaminated sharp that may carry bloodborne pathogens. The danger is the inoculation, not the puncture, which is why a trivial-looking prick can be a serious exposure.
The category is broader than the name suggests. It covers any sharp that can breach the skin and transfer blood or body fluids:
- Hollow-bore needles — the highest-risk subtype, because the lumen can retain a larger blood volume.
- Solid sharps — scalpels, suture needles, lancets, trocars.
- Contaminated broken glass — capillary tubes, ampoules, vials.
- Mucocutaneous exposures — blood splashes to the eyes, mouth, or non-intact skin, which sit in the same exposure-incident family even though no sharp is involved.
Who is exposed reaches well past the bedside. Nurses and phlebotomists dominate the data, but the risk follows the device downstream to laboratory staff, dentists, environmental-services and waste-handling teams, and — outside healthcare entirely — sanitation crews and law-enforcement officers who encounter discarded needles.
Reviewing the published incident record, one pattern is consistent enough to treat as a rule: the severity of the outcome is decoupled from the size of the wound. A barely-visible scratch from a hollow-bore needle used on an infectious source outranks a deep, dramatic cut from a clean instrument. That decoupling is exactly what drives the most dangerous behavior — a worker downplays a “tiny prick,” delays reporting, and quietly burns through the window in which post-exposure prophylaxis is most effective.
Which Pathogens Pose the Greatest Risk — and the Actual Transmission Odds
The honest framing is that single-exposure risk is low but non-zero, and the stakes make even low odds unacceptable to leave to chance. Three bloodborne pathogens drive the concern, and a common misconception is worth correcting up front: HIV is not the dominant statistical risk. HBV and HCV are more transmissible per exposure, and HBV in particular is the highest-probability transmission of the three against a non-immune worker.
| Bloodborne pathogen | Approx. risk per percutaneous exposure | Post-exposure pathway |
|---|---|---|
| HBV (hepatitis B) | Up to ~30% (unvaccinated worker, highly infectious source) | Vaccination ± immunoglobulin, by vaccination/responder status |
| HCV (hepatitis C) | ~1.8% | No prophylaxis — monitoring + early antiviral treatment if seroconversion occurs |
| HIV | ~0.3% | Clinician-led PEP, started as soon as possible |
Transmission figures: US CDC/OSHA. Risk varies with source viral load, needle type, blood volume, and injury depth.
Those percentages are averages, not guarantees in either direction. A deep injury from a large-bore device used on a source with a high viral load sits well above the average; a glancing scratch from a solid suture needle sits below it. The practical reading is that the figures justify a fast, structured response rather than reassurance.
How Needlestick Injuries Happen: The Failure Points
Most needlestick injuries are not random — they cluster at three identifiable points in the device’s lifecycle, and each point maps to a control that should have caught it. Mapping injuries to where in the workflow they occur is more useful than listing abstract “causes,” because it tells you which control failed.
- During use — the needle is in motion near the patient and the worker. Awkward patient positioning, sudden movement, and rushing under staffing pressure drive injuries here. The control is procedural: technique, positioning, and not working faster than the task safely allows.
- After use, before disposal — the most under-managed window. The device is now contaminated and exposed, but the worker’s attention has already shifted to the next task. Recapping a used needle belongs here and is a discrete, preventable behavior that regulators specifically target.
- During disposal — roughly a third of injuries occur at this stage. Overfilled sharps containers, devices protruding from the opening, and injuries to people who never used the device — waste handlers and housekeeping — concentrate here.
A recurring failure mode deserves naming: teams treat the sharps container as the safety control and quietly ignore the riskier seconds between use and disposal. The container matters, but it only protects against the device once it’s inside. The exposed interval — needle used, hands moving, container a few steps away — is where a large share of injuries actually happen, and no container can reach back in time to cover it.
Human-factors drivers sit underneath all three stages: rushing, understaffing, distraction, and poor point-of-use container placement. These are organizational conditions, not individual carelessness — which is why the durable fixes are systemic.

How to Prevent Needlestick Injuries: The Hierarchy of Controls
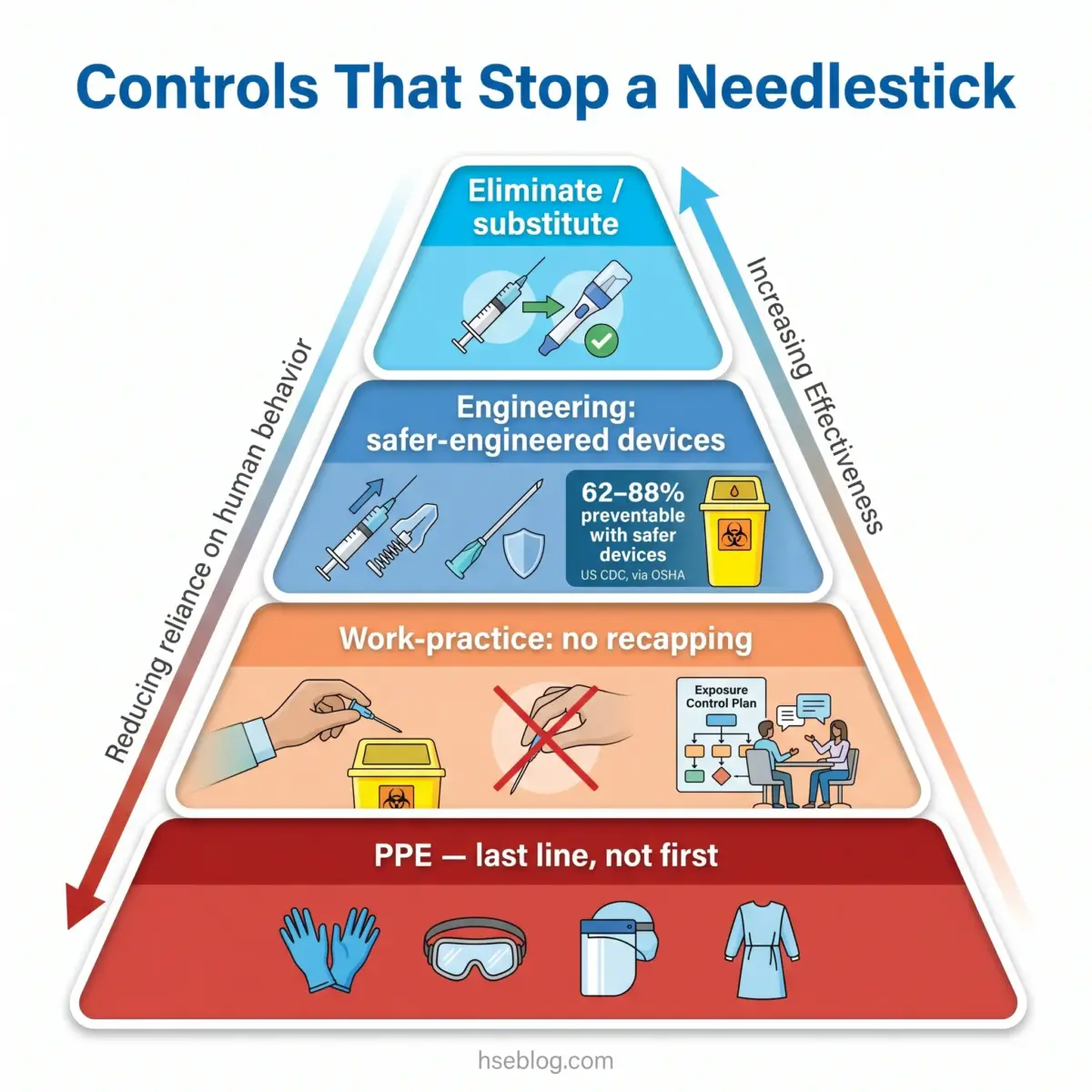
Prevention works when it follows the hierarchy of controls rather than a flat list of tips — because that is the framework the regulators actually enforce. The order matters: the higher up the hierarchy a control sits, the less it depends on a tired human making the right call in the right second.
The verified anchor for the whole approach is that 62–88% of sharps injuries are preventable with safer medical devices (US CDC, cited by OSHA). That single range reframes prevention from awareness campaigns to engineering and procurement decisions.
Elimination and Substitution
- Remove unnecessary injections and sharps where a needle-free route or an alternative delivery method exists.
- Substitute safer-engineered sharps — the most effective tier short of removing the device entirely.
Engineering Controls
- Self-sheathing and retractable needles that cover or withdraw the point immediately after use.
- Blunt-tip suture needles in surgical settings where they are clinically appropriate.
- Sharps containers at the point of use, so the exposed interval between use and disposal shrinks to seconds.
Work-Practice and Administrative Controls
- No recapping of used needles, except in the rare cases where a one-handed technique is genuinely required.
- Immediate disposal into a point-of-use container.
- A written exposure control plan, reviewed at least annually for new safer technology.
- Frontline-worker input into device selection — the people using the device know which “safety” feature is unusable in practice.
PPE — the Last Line, Not the First
Gloves and eye protection reduce the consequence of some exposures, but a glove does not stop a hollow-bore needle. PPE is the final layer precisely because it depends entirely on the device already having failed.
A recurring gap undermines all of this in the field: facilities buy safety-engineered devices but never confirm that staff actually activate the safety feature. Procurement gets logged as compliance, while the human step that makes the device safe — sliding the shield, triggering the retraction — goes untrained and unaudited. A safety device with its mechanism unused is just a regular needle with a higher invoice. The CDC sharps injury prevention program workbook is a useful reference for building the program around that reality rather than around the purchase order.
The Role of Hepatitis B Vaccination in Prevention
HBV vaccination is a pre-exposure control, and in the US the employer must offer it free of charge to workers with occupational exposure. It targets the pathogen with the highest per-exposure transmission risk, which makes it the single most efficient prevention investment against the three concerns.
Two points carry into the response phase. Vaccination status matters at the moment of exposure, and so does responder status — whether the worker mounted a protective antibody response. A documented responder needs no HBV post-exposure treatment; a known non-responder or a worker of unknown status changes the post-exposure decision entirely, which is why this information belongs in the occupational-health record before an injury ever happens.
What to Do Immediately After a Needlestick Injury: Step-by-Step Protocol
Act in this order: first aid, then report, then medical evaluation within hours — not days. The sequence is what protects the worker, because reporting is the step that starts the clinical clock for time-sensitive prophylaxis.
Medical disclaimer: This section is for HSE practitioner reference. It is not medical advice. A worker with a specific exposure should be assessed by an occupational physician or qualified medical professional, who makes all PEP and treatment decisions.
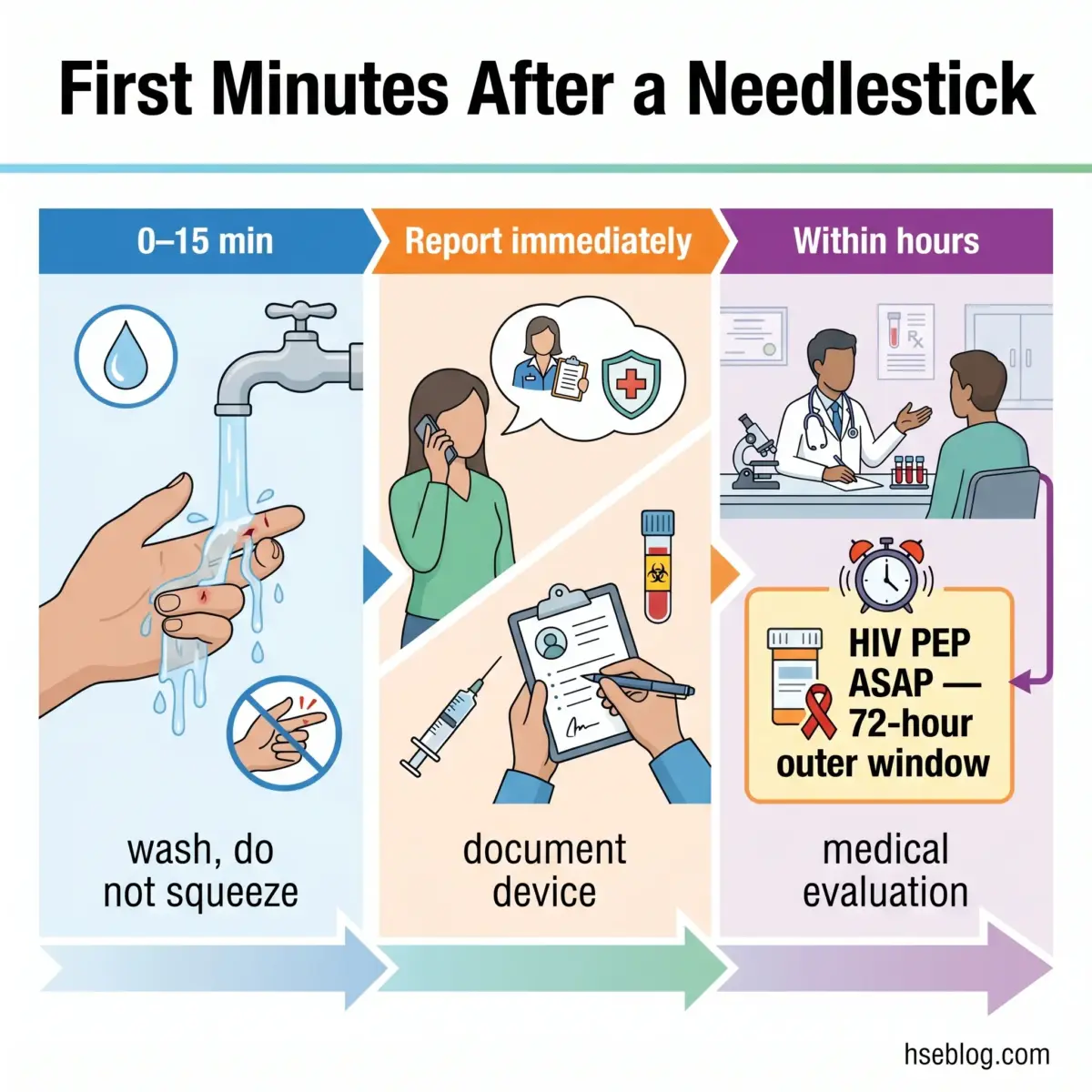
0–15 minutes — first aid
- Wash the wound with soap and running water. Let it bleed gently under the running water.
- Do not squeeze or “milk” the wound. Squeezing has no proven benefit and may worsen tissue trauma, potentially driving contaminant deeper rather than expelling it.
- For splashes, irrigate the eyes with water or saline and flush exposed mucous membranes thoroughly.
Within minutes — report and document
- Report immediately to the supervisor and occupational health. Reporting is not paperwork-after-the-fact; it is the trigger that starts the assessment and the PEP decision window.
- Document the incident details — the device involved, how the injury happened, and the source patient identity where known.
Within hours — medical evaluation
- Seek evaluation urgently. A clinician assesses the source patient and the exposure, draws baseline serology from the worker (HBV/HCV/HIV), and determines whether prophylaxis is indicated.
- HIV PEP, if indicated, starts as soon as possible. Effectiveness falls sharply with delay; the outer window commonly cited for HIV PEP is up to 72 hours, but “as soon as possible” is the operative instruction, not “within three days.”
The single most mishandled real-world step is the instinct to squeeze the wound to force blood out — a folk remedy with no evidence behind it. The second is treating reporting as optional. A worker who waits until the end of shift, or until tomorrow, to mention a “small” stick is not being stoic; they are running down the clock on the one intervention that is genuinely time-critical.
Post-Exposure Prophylaxis (PEP) and Medical Follow-Up
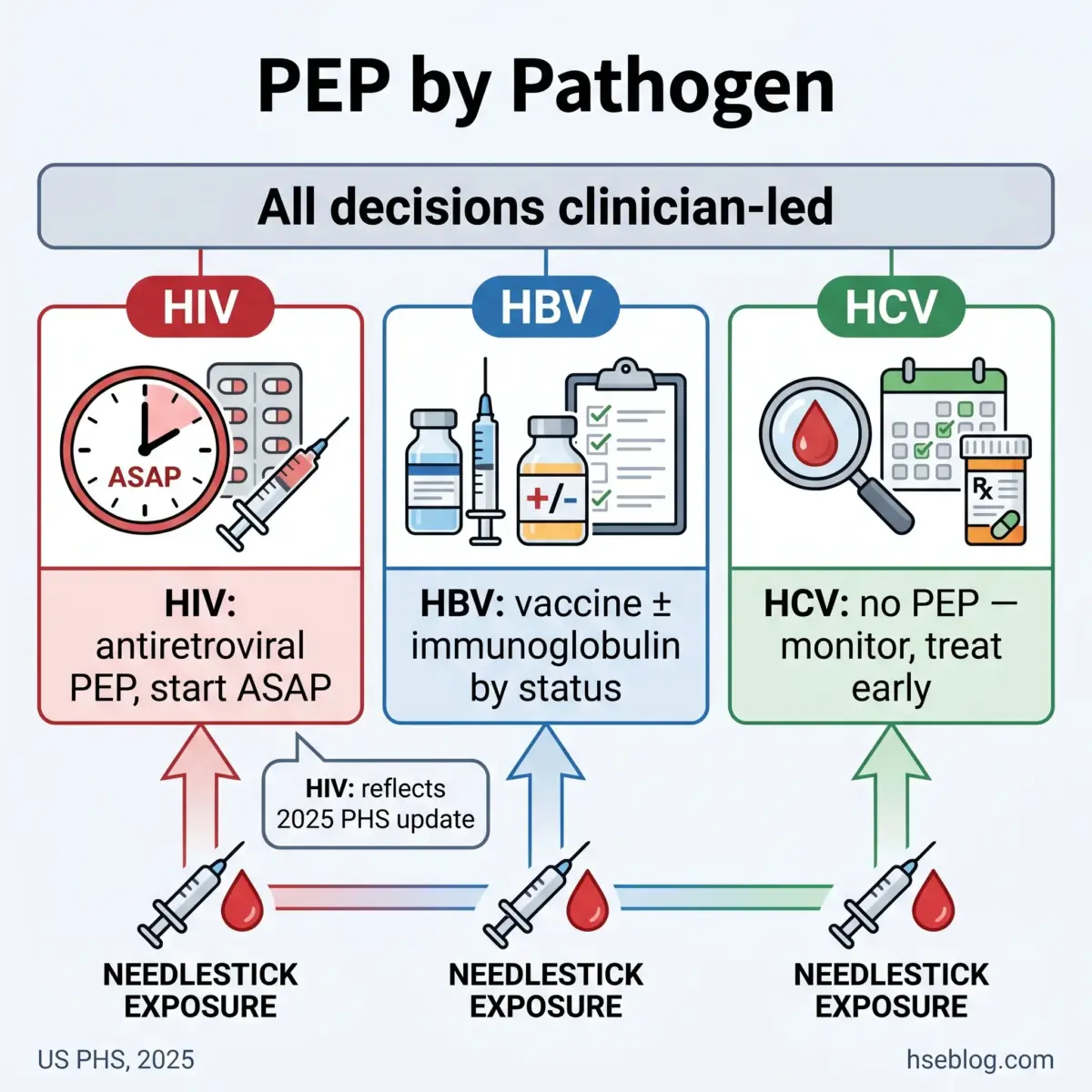
PEP differs by pathogen: HIV has a time-critical antiretroviral course, HBV is managed by vaccination status, and HCV has no prophylaxis at all. Every decision below is clinician-led — this section informs the practitioner; it does not prescribe.
A note on currency matters here. The US Public Health Service released updated occupational HIV exposure and PEP guidelines in 2025 — the first revision since 2013 — and most older web content still describes the 2013 regimen. The 2025 US PHS PEP guidelines introduce updated antiretroviral regimens, a shortened HIV follow-up testing period, elimination of routine ARV-toxicity labs, explicit consideration of source patients with undetectable viral loads, and — notably — inclusion of the exposed worker in the PEP decision rather than treating it as a purely clinician-imposed step.
HIV — Time-Critical Prophylaxis
- Start as soon as possible after exposure; the benefit erodes with every hour of delay.
- A clinician determines the regimen, typically running about a 28-day course.
- Source viral load now informs the decision. Under the 2025 guidance, an undetectable source viral load is a consideration in the PEP judgment — but this is a clinician-led assessment, never a blanket “no PEP needed” rule a worker should apply themselves.
HBV — Managed by Status
- Depends on the worker’s vaccination and responder status and on the source’s status.
- HBIG (hepatitis B immunoglobulin) may be indicated alongside vaccination for a non-immune worker exposed to an infectious source.
- A documented responder generally needs no further HBV action — which is why that record should exist before an injury.
HCV — Monitor, Don’t Prophylax
- No prophylaxis exists. Management is baseline and follow-up testing.
- Early antiviral treatment is the pathway if seroconversion is detected, and modern HCV therapy makes early detection genuinely consequential.
Two practitioner realities round this out. First, PEP non-adherence is a recurring breakdown — workers stop the course early because of side effects, undermining the protection the protocol was built to provide, so anticipating and supporting adherence is part of a competent program. Second, the follow-up testing window carries a heavy psychological load that clinical checklists routinely ignore; weeks of waiting to learn whether you seroconverted is a real occupational-health burden, and it deserves explicit support rather than silence.
Regulatory and Employer Obligations Across Jurisdictions
Employer duties around sharps converge on the same goals — prevent, protect, respond, record — but the specific legal instruments and reporting rules differ by jurisdiction. The table below places the three frameworks side by side; the narrative then flags where they actually diverge.
Legal disclaimer: This content reflects general HSE professional understanding of US, UK, and EU requirements as of 2025. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction. Regulatory content here was reviewed for currency in 2025; confirm against the primary sources at the date of use.
| Duty | US (OSHA) | UK (HSE) | EU |
|---|---|---|---|
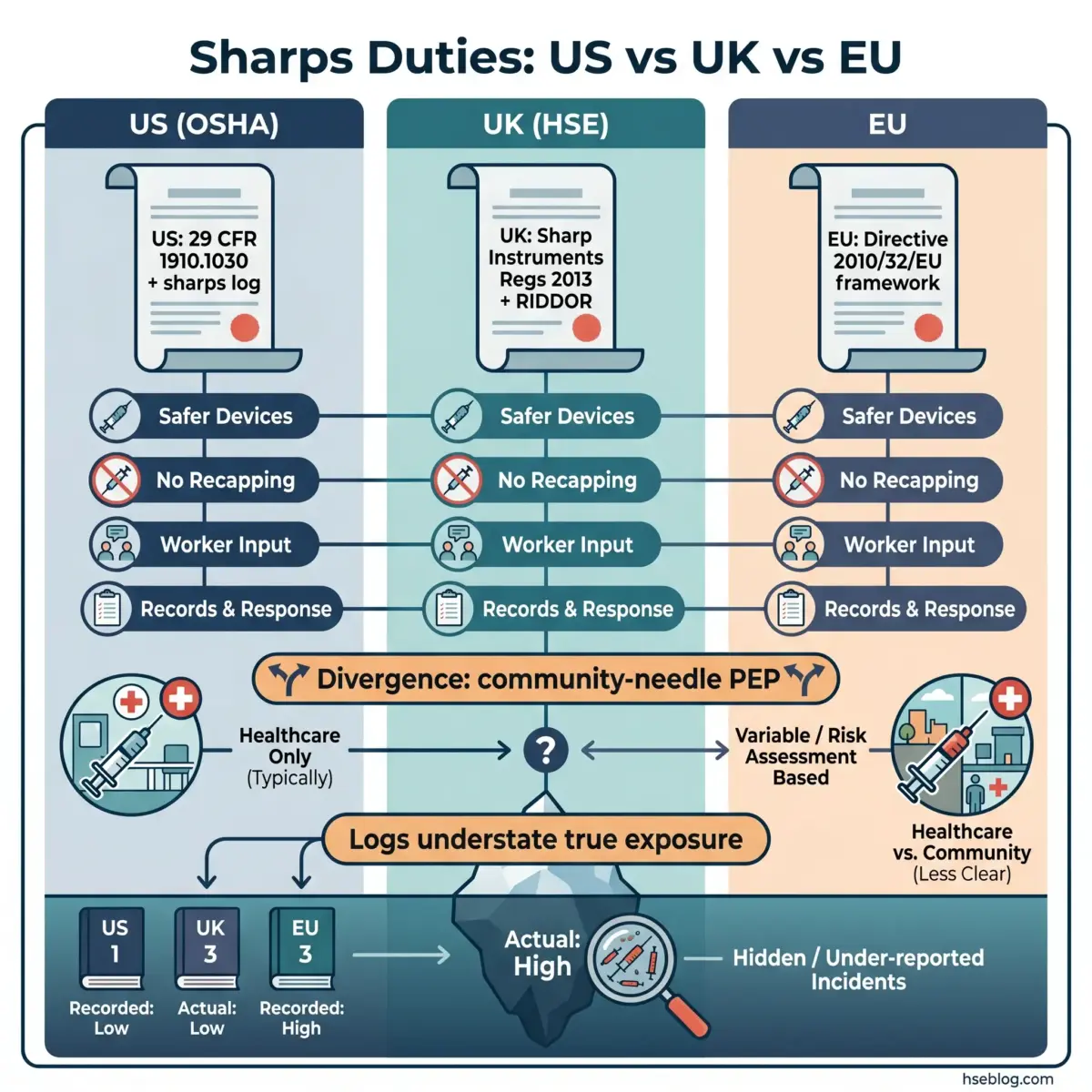
| Governing instrument | Bloodborne Pathogens Standard, 29 CFR 1910.1030 + Needlestick Safety and Prevention Act | Health and Safety (Sharp Instruments in Healthcare) Regulations 2013 (SI 2013/645) | Council Directive 2010/32/EU (the Sharps Directive) |
| Safer devices | Use/evaluate safer-engineered devices; annual review for new technology | Substitute safer-engineered sharps where reasonably practicable | Framework requiring member-state laws to mandate prevention |
| Recapping | Prohibited unless required by a specific procedure | Banned unless a one-handed technique is required | Addressed via member-state transposition |
| Worker input | Documented input from non-managerial frontline workers in device selection | Risk assessment and consultation duties | Built on the HOSPEEM–EPSU framework agreement |
| Records / response | Exposure control plan; separate sharps injury log; post-exposure follow-up | Clear injury-response procedures; interacts with RIDDOR reporting | Basis for national recording and response rules |
In the US, the legal backbone is the OSHA Bloodborne Pathogens Standard (29 CFR 1910.1030), reinforced by the Needlestick Safety and Prevention Act. Together they require a written exposure control plan, free HBV vaccination, post-exposure evaluation and follow-up, a separate sharps injury log, and — a point employers often overlook — documented input from frontline workers when selecting safer devices.
For the UK, the practical reference is the HSE guidance on the Sharp Instruments in Healthcare Regulations 2013. Those regulations implement EU Directive 2010/32/EU and require avoiding unnecessary sharps, substituting safer devices where reasonably practicable, banning recapping unless required, providing point-of-use disposal, and having clear response procedures. UK injury reporting then interacts with RIDDOR, which is reportable where the exposure results in infection or meets specified criteria.
Two divergences matter operationally. US occupational guidance frames HIV PEP consideration as standard for healthcare exposures, whereas UK national guidance generally does not recommend HIV PEP for community discarded-needle injuries — so the same puncture can trigger different protocols depending on where and how it happened. And the sharps injury log, while a legal requirement in the US, is a structurally weak standalone metric: because around half or more of injuries go unreported (US CDC/NIOSH), the log systematically understates true exposure and should never be read as a clean measure of program success.
Frequently Asked Questions
Conclusion
The industry’s recurring mistake with needlestick injuries is treating them as a wound-management problem when they are an exposure-management problem. The size of the prick tells you almost nothing; the source, the device, and the speed of response tell you everything. That single reframing — severity is decoupled from the wound — is what separates a program that protects workers from one that just stocks sharps containers and files logs.
If there is one highest-impact change, it is closing the “tiny prick → delayed report → missed window” cascade. Most of these injuries are preventable at the device level — 62–88% with safer-engineered devices (US CDC, cited by OSHA) — but the ones that still occur are only survivable as a clinical problem if the worker reports immediately and reaches evaluation within hours. Build the culture where a same-minute report is normal, audit whether staff actually activate the safety feature they were issued, and keep your protocol current with the 2025 PHS PEP changes.
The work is unglamorous: procurement that prioritizes the right device, training that covers the human step, an exposure control plan that gets read rather than shelved, and an occupational-health pathway that treats the weeks-long testing window as a real burden rather than a formality. Done together, those reduce both how often needlestick injuries happen and how badly they end.