

TL;DR
- Myth: Cold injury only happens below freezing. Reality: Hypothermia, trench foot and chilblains all develop above 0°C in wet, windy conditions.
- Myth: A warming drink helps. Reality: Alcohol speeds heat loss and suppresses shivering; caffeine and nicotine cut blood flow to skin and extremities.
- Myth: When shivering stops, the worker is recovering. Reality: Shivering stopping can signal worsening hypothermia, not improvement.
- Myth: Warm frozen tissue fast. Reality: Rubbing or direct heat destroys frozen tissue; thawing then refreezing causes deeper, often permanent injury.
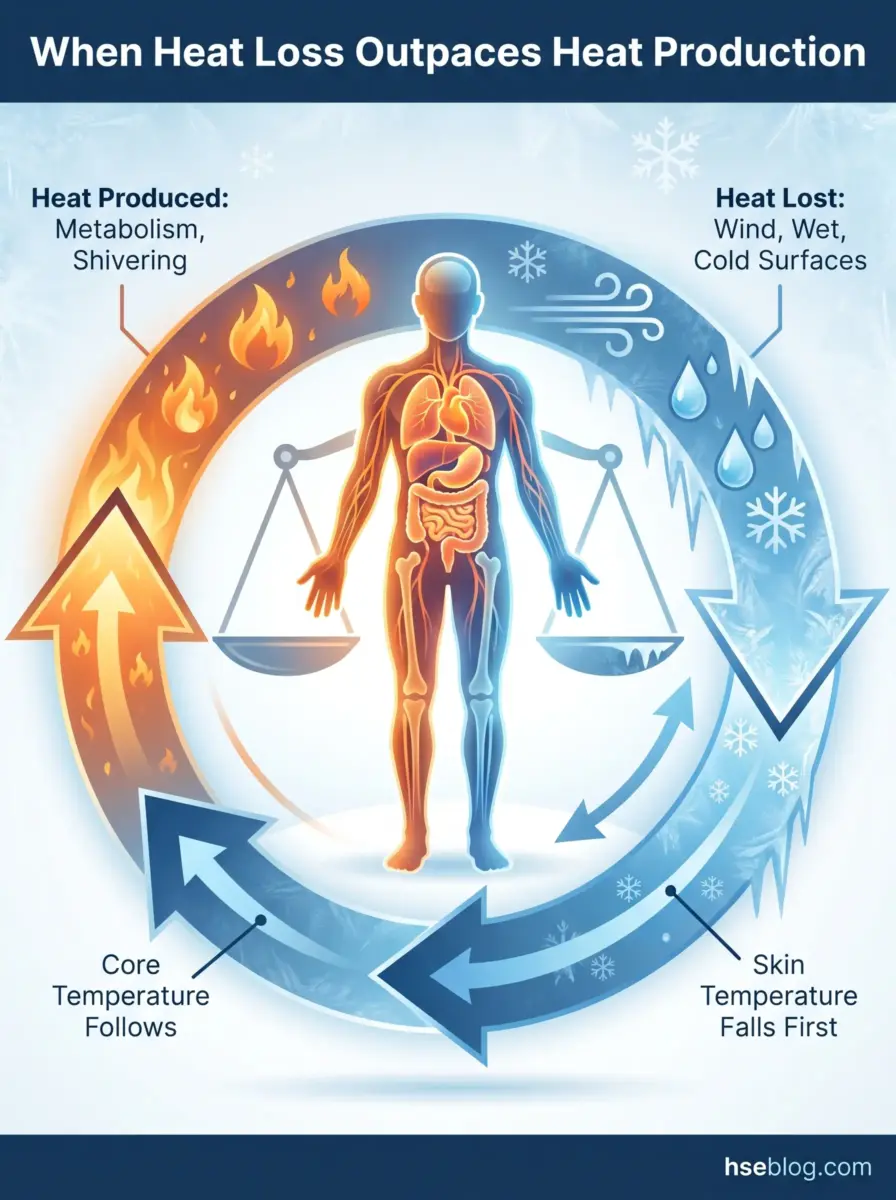
Working in extreme cold becomes dangerous when the body loses heat faster than it can produce it, so no single safe temperature exists — wind, wet clothing and exertion all accelerate heat loss. Near a wind chill of −19°F (−28°C), exposed skin can freeze in roughly 30 minutes (US National Weather Service/NOAA), and frostbite and hypothermia risk climbs sharply below that.
At a wind chill near −19°F (−28°C) — say, 0°F air pushed by a 15 mph wind — exposed skin can freeze in about 30 minutes, and at −40°F frostbite can set in within 10 minutes or less (US National Weather Service/NOAA). For a crew on a winter shutdown or a delivery round, that is less time than a single task takes.
Cold stress rarely announces itself the way a fall or a moving vehicle does — the harm builds quietly, and the first person to miss it is often the casualty whose own judgment is already slipping. This article covers how cold injury develops, how to recognise it early, the threshold systems that actually define “too cold” for working in extreme cold, and the controls and first-aid response that survive an audit.
How Cold Stress Develops: The Path from Cold Stress to Frostbite and Hypothermia
Cold stress develops when the body loses heat faster than it can generate it — skin temperature drops first, and if heat loss continues, core body temperature follows (OSHA framing). That sequence is the foundation everything downstream depends on.
The body defends its vital organs through peripheral vasoconstriction: it narrows blood vessels in the limbs and pulls warm blood toward the core. That self-protective reflex is precisely why fingers, toes, nose, ears and cheeks freeze first — they are sacrificed to keep the heart and brain supplied.
“Cold injury” is not two conditions but a spectrum, and most under-assessment happens because teams only count the bottom two:
- Frostnip — surface cooling with no tissue freezing; reversible, an early warning rather than damage.
- Frostbite — actual freezing of skin and the tissue beneath it; the localised injury most people picture.
- Hypothermia — core temperature below 95°F (35°C); whole-body, not localised, and the one that kills.
- Trench foot — non-freezing injury from prolonged wet and cold; occurs above freezing.
- Chilblains — painful inflammation of small blood vessels after repeated cold exposure; also occurs above freezing.
A consistent pattern across cold-injury reporting: crews equate cold injury with sub-zero outdoor work and overlook trench foot and chilblains in damp, just-above-freezing settings — refrigerated logistics, wet groundwork, standing water in trenches. The absence of visible ice reads as “not cold enough to matter,” and the assessment never happens.

Recognising the Warning Signs: Frostbite vs Hypothermia Symptoms
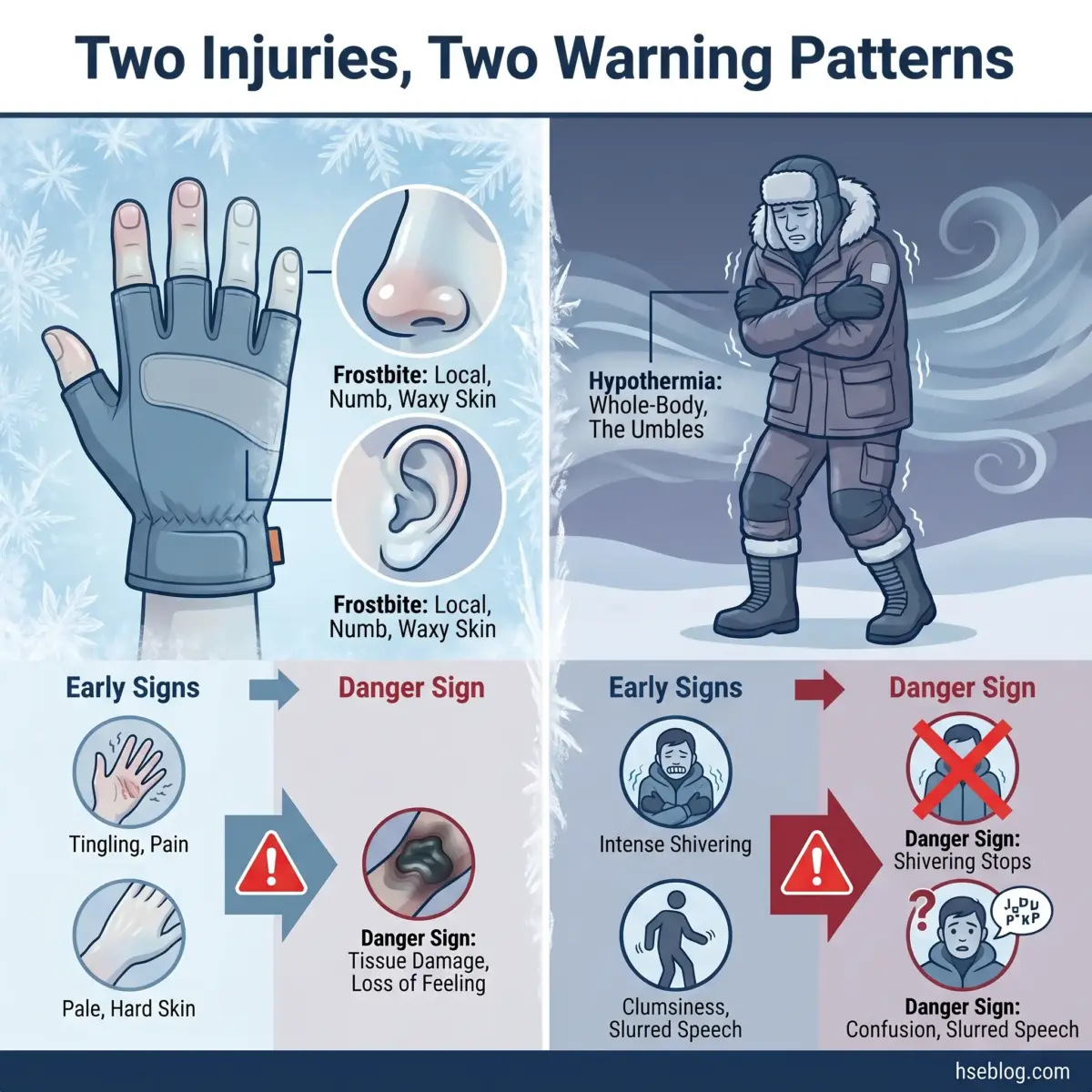
Tell the two apart by what they attack: frostbite is local tissue freezing, while hypothermia is a whole-body core temperature collapse — and the early signs of frostbite and hypothermia in workers are easy to miss on a busy site.
Frostbite advances through stages. It starts as pins-and-needles or throbbing, moves to numbness, then the skin turns firm, pale and waxy; colour then shifts from white or grey-yellow toward reddish-violet and, in severe cases, black, with blistering signalling deeper injury.
Hypothermia announces itself through the “umbles” — stumbles, mumbles, fumbles and grumbles — alongside shivering and clumsiness, then slurred speech and loss of coordination.
| Frostbite | Hypothermia | |
|---|---|---|
| Cause | Localised tissue freezing | Whole-body core heat loss |
| Body area | Fingers, toes, nose, ears, cheeks | Entire body |
| Early signs | Tingling, numbness, pale waxy skin | Shivering, the “umbles,” clumsiness |
| Danger signs | Hard skin, colour shift, blistering | Shivering stops, slurred speech, confusion |
| First response | Protect, don’t rub, prevent refreezing | Move to warmth, insulate, call for help |
The recurring misjudgement here flips the meaning of a symptom. Supervisors read the cessation of shivering as the worker “warming up and being fine,” when stopping can instead mark deterioration — the body has run out of the energy to shiver. Two more late signs catch responders out: confusion that prevents a casualty from recognising their own decline, and paradoxical undressing, a rare late-stage hypothermia behaviour where the casualty removes clothing.
What Temperature Is Dangerous to Work In? Wind Chill, Exposure Time, and Thresholds
There is no single dangerous temperature, because wind, wet clothing and workload change the answer minute to minute — which is why three different threshold systems exist instead of one magic number. The honest answer to “what temperature is too cold to work outside” is: it depends on heat loss, not the thermometer alone.
- Wind chill freezing time (NWS/NOAA). Near a wind chill of −19°F (−28°C), exposed skin can freeze in roughly 30 minutes; at −40°F, frostbite can occur in 10 minutes or less. This is the wind chill temperature index in its most operational form.
- ACGIH Wind Chill Temperature index and work/warm-up schedule. A consensus guideline pairing exposure with recovery breaks, summarised in CCOHS’s wind chill index and work/warm-up schedule. It recommends cycles, not a hard limit.
- ISO 11079 IREQ and Duration Limited Exposure. This international standard calculates the Required Clothing Insulation (IREQ) for heat balance and a permissible exposure time once insulation is known; its local-cooling criteria say finger temperature should not fall below ~24°C in prolonged exposure (15°C only occasionally).
The 2024 ACGIH TLV/BEI booklet remains the current basis for the Wind Chill Temperature index referenced above, and ISO 11079 is itself under formal revision (committee draft ISO/CD 11079, 2024–2025) — worth flagging for anyone citing the IREQ method as settled.
| System | What it measures | Practical output | Jurisdiction |
|---|---|---|---|
| Wind chill chart (NWS/NOAA) | Wind-driven heat loss on bare skin | Time-to-freeze for exposed skin | US, applied internationally |
| ACGIH WCT + work/warm-up | Combined cold and wind | Recommended exposure/recovery cycles | US-origin consensus, used internationally |
| ISO 11079 (IREQ/DLE) | Clothing insulation vs heat balance | Required insulation and exposure time | International |
The applied failure mode is reading the dry-bulb thermometer and ignoring everything that actually drives heat loss. The worst cold injuries often happen at “not that cold” air temperatures combined with strong wind or soaked clothing — wet skin in wind should be treated as markedly colder than the dry-air reading suggests. Cross-reference OSHA’s cold stress guidance, echoed by NIOSH cold stress materials, when building your own exposure triggers.
Why There Is No Single “Legal” Cold Temperature
OSHA (US) sets no numeric cold limit at all, and the UK sets indoor minimums but no outdoor figure — so every “threshold” above is an assessment tool, not a bright line you can be prosecuted for crossing. The number tells you when to act; it does not absolve you of judgment. That distinction sets up the compliance picture later in this guide.

Who Is Most at Risk: Job Roles and Individual Vulnerability Factors
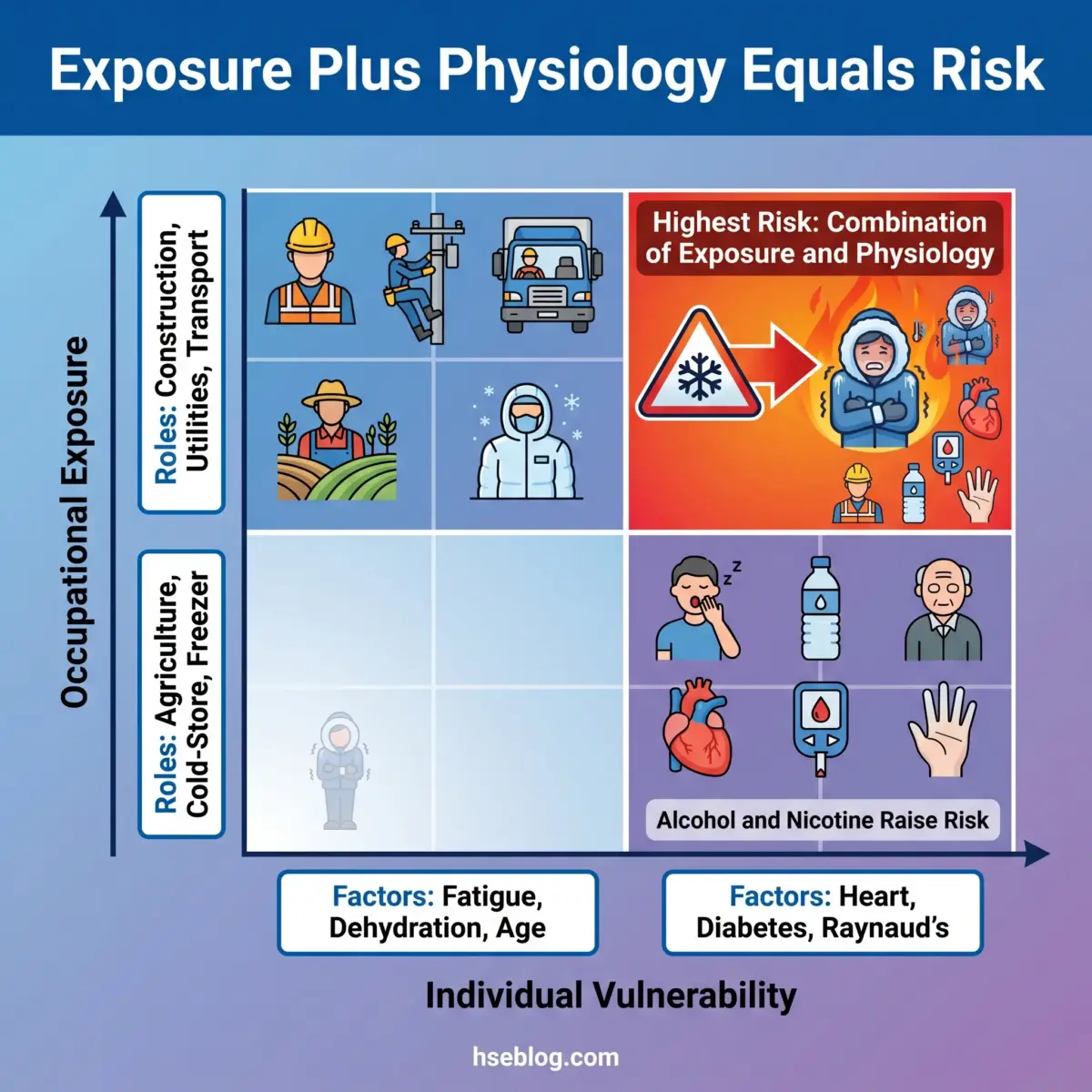
Risk in extreme cold splits into two layers: the job that puts you in the cold, and the physiology that decides how well you tolerate it. Two workers side by side in the same wind chill do not carry the same risk.
This content covering exposure, individual susceptibility and medication effects is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms, conditions or exposure concerns should consult an occupational physician or qualified medical professional.
High-exposure occupational roles include:
- Construction and groundwork — long static exposure, often on wet or frozen ground.
- Utilities and pipeline — fixed outdoor tasks in all weather, frequently wind-exposed.
- Transport and delivery — repeated in-out exposure and time in unheated load areas.
- Agriculture and emergency services — unpredictable duration, limited shelter.
- Cold-store and freezer operatives — sustained sub-zero exposure indoors, easy to underestimate.
Individual factors that raise risk include:
- Fatigue and dehydration — both reduce the body’s capacity to generate and regulate heat.
- Chronic conditions — cardiovascular disease, diabetes and Raynaud’s can impair circulation and thermoregulation.
- Age and prior cold injury — previously damaged tissue is more vulnerable to re-injury.
The “warming drink” belief deserves direct correction. Alcohol triggers vasodilation — blood rushes to the skin, feels warm, and dumps core heat — while also suppressing shivering, the body’s main heat generator; nicotine and caffeine narrow peripheral vessels and reduce blood flow to fingers and toes. Where competitor pages stop at “stay hydrated,” the physiology is the point: dehydration and alcohol specifically degrade cold tolerance, and some prescription medications alter thermoregulation, which is a question for occupational health rather than self-assessment.
A Layered Prevention Strategy: Controls Beyond “Wear a Coat”
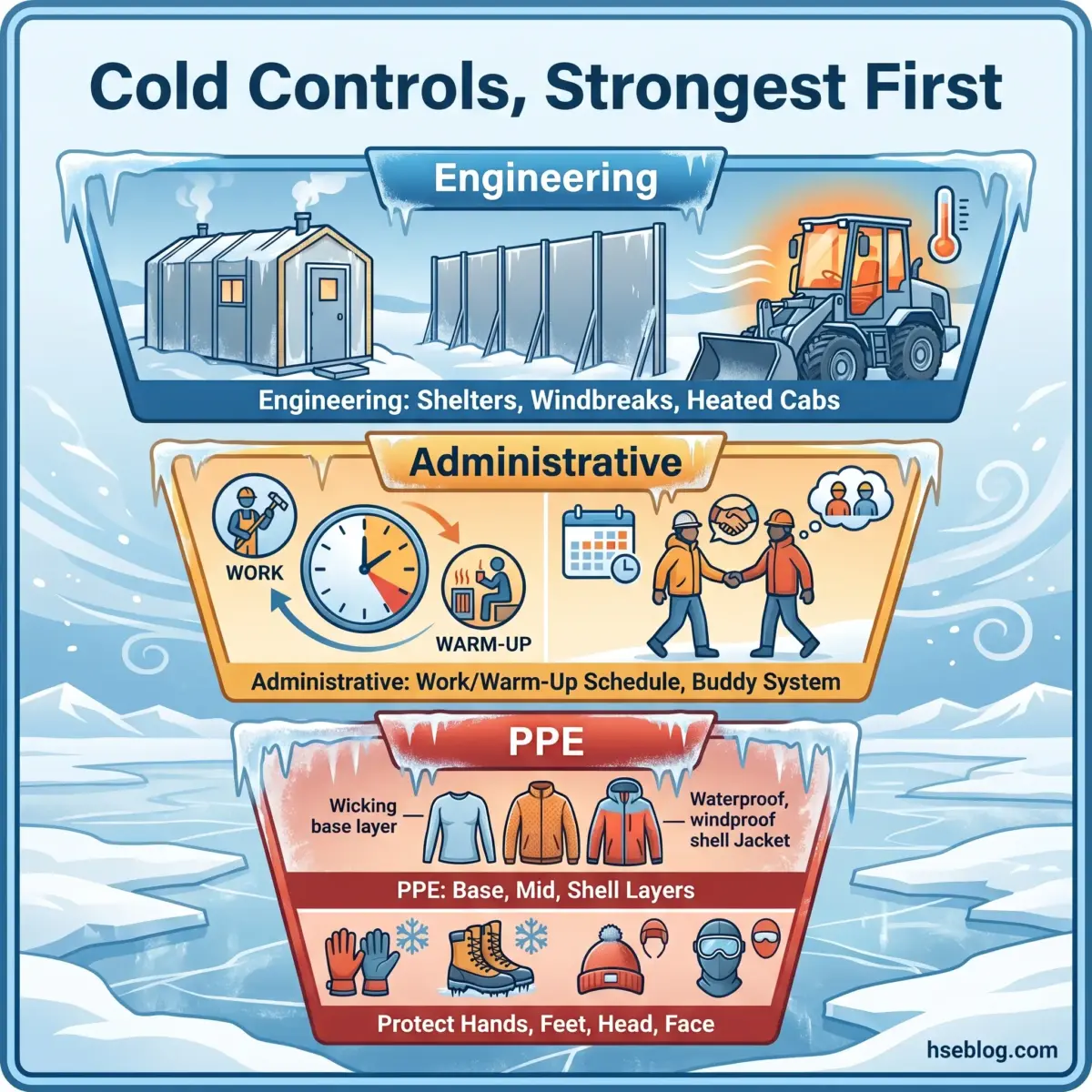
Effective cold stress prevention is a program, not a kit — it works through the hierarchy of controls applied to cold, with PPE as the last line rather than the plan. Reaching straight for a thicker coat skips the controls that do more work for less risk.
Engineering controls
These remove or reduce the cold at source, before it reaches the worker:
- Thermal shelters and warming areas sited within easy reach of the work.
- Windbreaks and draft reduction to cut the wind component of heat loss.
- Heated cabs and enclosures for plant operators and fixed posts.
- Insulating mats between workers and cold ground or steel surfaces.
Administrative controls
These shape how and when the work happens:
- Work/warm-up schedule — paired exposure and recovery cycles, the practical core of cold stress prevention.
- Scheduling to the warmest daylight hours and rotating workers through colder tasks.
- Buddy system so deteriorating judgment is spotted by someone else.
- Training on early signs, because acclimatisation cannot be relied on (see below).
PPE and the layered clothing system
The layered clothing system is dynamic, not a fixed outfit, and it works in a specific order:
- Base layer — moisture-wicking, to move sweat off the skin.
- Mid layer — insulating, to trap warm air.
- Shell layer — windproof and waterproof, to block wind and wet.
Add extremity protection — insulated gloves, boots, headwear and face protection — and remember the governing principle of cold weather PPE: wet insulation fails. Warm fluids and adequate calories are physiological controls too, not comforts.
The set-and-forget failure mode is the one I see most often in the published record and in audits: a cold-weather PPE kit issued at season start and never reassessed as tasks, conditions and exertion change. The most common real-world error is over-dressing for heavy work, sweating into the base layer, then chilling fast during a break — which is why layering has to be adjusted through the shift, not at the start of it.
Does Cold Acclimatisation Work Like Heat Acclimatisation?
No — and this is a dangerous assumption to build a control around. Humans acclimatise to cold far less, and far more slowly, than to heat, so “they’ll get used to it” is not a control measure. Plan for the cold tolerance workers have now, not the toughening-up you are hoping for.
Cold-Weather First Aid: Responding to Frostbite and Hypothermia
The right cold stress first aid is usually to recognise, protect and transport — not to rewarm aggressively on site — because several “obvious” warming actions cause serious harm. Get the response wrong and you can deepen the injury you are trying to treat.
This article provides general HSE knowledge. Life-critical work such as cold-injury first aid and casualty rewarming must be planned and supervised by a competent person with relevant training, jurisdiction-specific authorisation, and site-specific risk assessment. The information here does not replace that. Train responders through recognised pathways such as NEBOSH, IOSH, OSHA outreach, or an accredited first-aid certification, and defer to trained responders and EMS for treatment.
For hypothermia:
- Move the casualty to warmth and shelter as gently as possible — rough handling can trigger a dangerous afterdrop.
- Remove wet clothing and insulate the whole body, including the head and ground beneath them.
- Warm the core gradually; do not plunge the casualty into heat.
- Call emergency services for any moderate-to-severe case, and monitor breathing continuously.
For frostbite:
- Do not rub or massage the area — friction destroys frozen tissue.
- Do not rewarm if there is any chance of refreezing, because thaw-then-refreeze causes worse, often permanent damage.
- If rewarming is appropriate and medical care is delayed, use lukewarm — not hot — water, around 99–104°F (37–40°C); never apply direct or dry heat to frozen tissue.
- Avoid walking on frostbitten feet unless unavoidable, and cover the area loosely for transport.
Do not: rub frozen tissue, use a vehicle heater vent or chemical warmer on frostbite, or rewarm when refreezing is possible.
The field tension responders most often get wrong is the instinct to “warm it up fast” — hot water, heater vents, chemical warmers — which runs straight into the refreeze and burn risks above. Where both injuries are present, treat the life-threatening hypothermia first; for early recognition framing, MedlinePlus frostbite and hypothermia guidance backs the “protect and seek medical help” posture.

Employer Legal Duties and Compliance Across Jurisdictions
No major jurisdiction gives you a single outdoor cold temperature to obey — the duty is to assess and control a recognised hazard, and that duty exists whether or not a number does. Here is how the obligations differ, framed as general HSE understanding rather than legal advice.
Regulatory content here reflects general HSE professional understanding of US and UK requirements as of 2026. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction. Regulatory content reviewed 2026.
United States. OSHA has no specific standard for working in cold environments. Instead, the General Duty Clause — OSH Act Section 5(a)(1), US, 1970 — requires employers to provide a workplace free of recognised hazards likely to cause death or serious physical harm, and it is citable when basic cold controls are absent. OSHA’s Winter Weather guidance then supplies the expected practices: training, appropriate clothing, engineering controls and warm breaks.
United Kingdom. The Workplace (Health, Safety and Welfare) Regulations 1992, Reg 7, with its Approved Code of Practice (UK), requires a “reasonable” indoor temperature, normally at least 16°C, or 13°C where much of the work is physically strenuous — but sets no statutory outdoor or maximum limit. The overarching duty sits in the Health and Safety at Work etc. Act 1974 (UK). HSE’s 2024 cold-weather guidance now directs employers to specific British and ISO standards — BS EN ISO 11079, ISO 15743, ISO 13732-3 and BS 7915 — as routes to demonstrate compliance, set out in HSE’s cold stress guidance for employers.
International consensus tools. ISO 11079 (IREQ) and ISO 15743 (cold-workplace risk assessment), alongside ACGIH TLVs, give a defensible quantitative basis where no national number exists. The conflict here is not contradictory limits but parallel frameworks; where a defensible numeric basis is needed, the stronger combination is ISO 11079 IREQ/Duration Limited Exposure cross-checked against the ACGIH work/warm-up schedule — rather than treating the absence of an OSHA number as a safe harbour.
A documented cold-stress program should contain, at minimum:
- Risk assessment specific to the tasks, sites and seasons involved.
- Monitoring of temperature, wind and wet conditions, with records.
- PPE specification and selection criteria tied to the assessment.
- Training records covering recognition and response.
- Emergency response arrangements, written down.
The audit-trail gap is where competent employers still get caught: they run the controls but cannot evidence them. The difference between a defensible position and a citation is frequently documentation — wind-chill logs, training records, PPE selection criteria — not the controls themselves.
Frequently Asked Questions
Conclusion
The recurring failure in working in extreme cold is not ignorance of the danger — it is under-reading it. Crews judge risk by the dry thermometer, miss the wind and the wet, and treat the end of shivering as recovery rather than decline.
The single highest-impact change is to stop hunting for one “safe” temperature and instead assess against wind chill, clothing insulation and workload — the ACGIH work/warm-up schedule cross-checked against ISO 11079’s IREQ method. Then document it: wind-chill logs, PPE selection criteria and training records are what separate a defensible position from a citation, in both US and UK enforcement.
Cold injury is slow, quiet and almost entirely preventable, which is exactly why it gets normalised until someone loses a finger or a life. The competent response is rarely dramatic — it is the warm-up shelter that actually gets used, the soaked base layer that gets changed at the break, and the discipline to protect and transport instead of rewarming a frozen hand in a truck cab.