

TL;DR
- Look for change, not labels. The critical indicator is deviation from an individual’s established behavioural baseline — not matching symptoms to a diagnosis.
- Quiet withdrawal gets missed most often. Dramatic outbursts attract attention; the colleague who silently stops engaging is the one managers overlook.
- Welfare inquiry before performance management. When work output declines alongside behavioural change, the first conversation should address wellbeing — not targets.
- Managers notice, not diagnose. The role of a line manager or colleague is to observe persistent changes and connect the person with professional support, never to assess clinical conditions.
- Regulatory enforcement is tightening. HSE UK served Notices of Contravention for failure to manage work-related stress in 2025 — psychosocial risk is now a compliance matter, not just a wellbeing initiative.
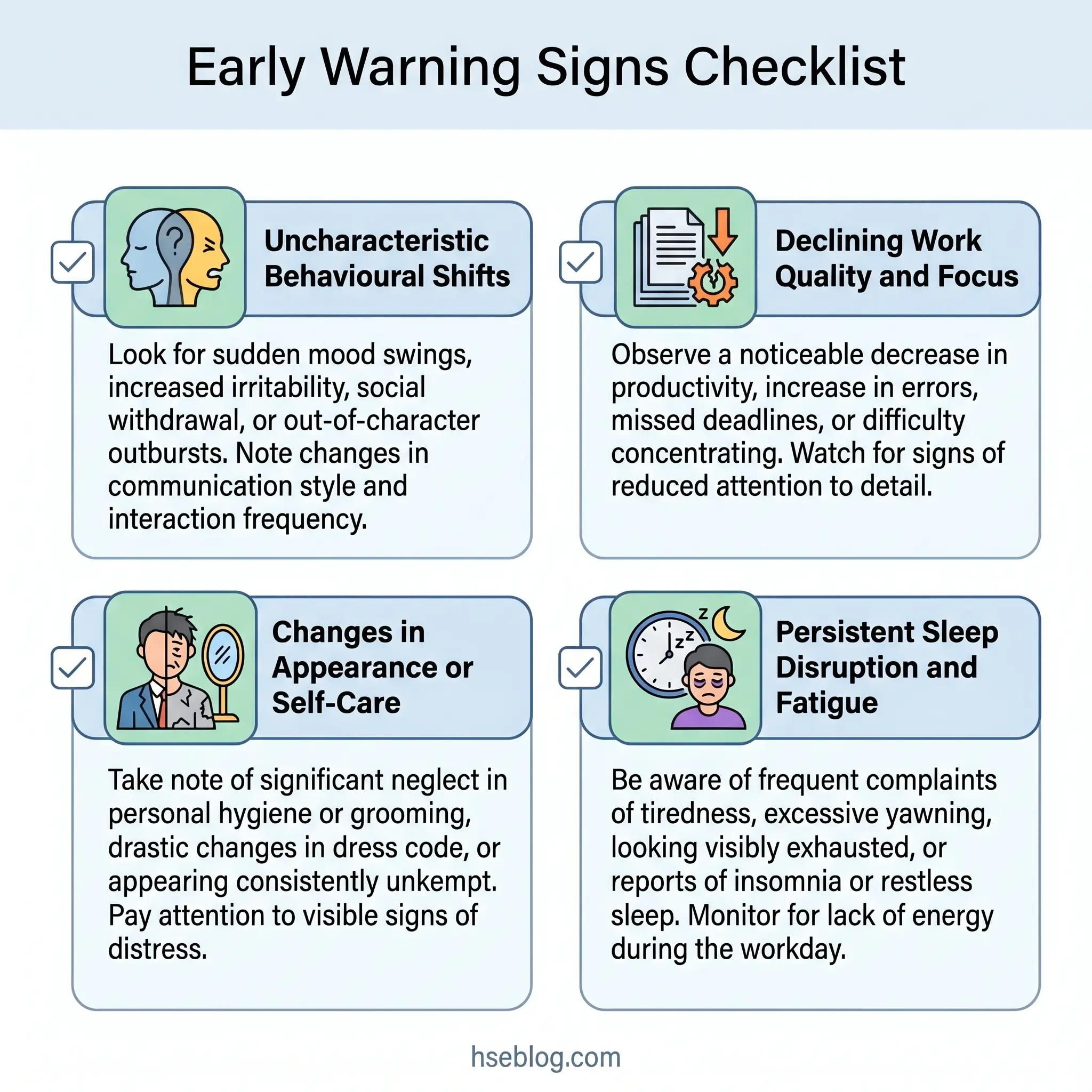
Poor mental health in the workplace typically manifests through observable changes across four domains: behaviour (irritability, mood swings, withdrawal), performance (declining output, increased errors, difficulty concentrating), physical presentation (neglected appearance, fatigue, weight change), and social interaction (isolation, avoiding colleagues, reduced participation). Persistent changes lasting two or more weeks — not a single bad day — are the key indicator.
Why Recognising Poor Mental Health at Work Matters
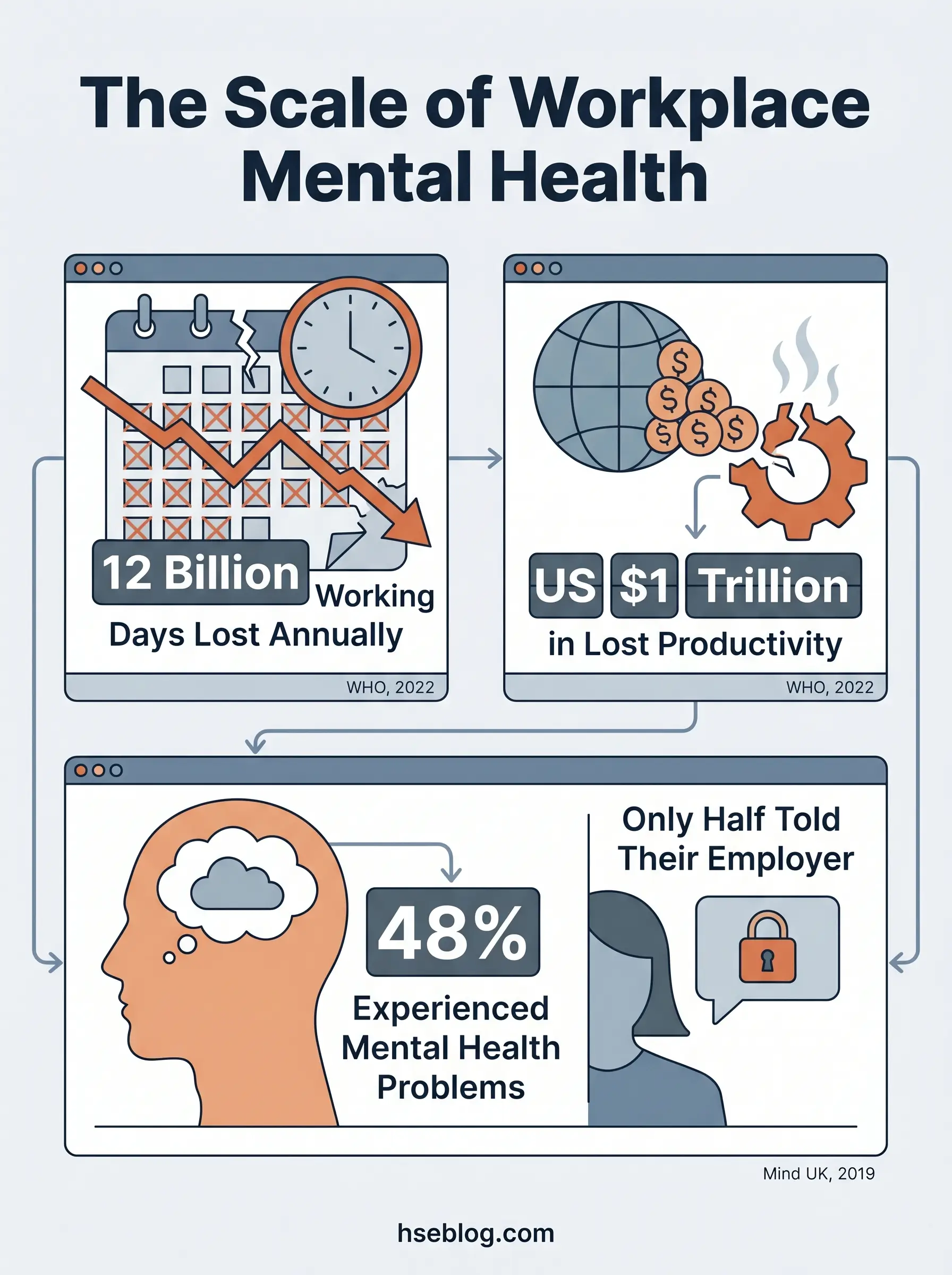
Approximately 12 billion working days are lost annually to depression and anxiety worldwide, costing the global economy roughly US $1 trillion in reduced productivity (World Health Organization, 2022). Behind that number sits a disclosure gap that makes the problem harder to address: in a survey of 44,000 UK workers, 48% had experienced a mental health problem in their current job, yet only half ever told their employer (Mind, 2019).
That gap between prevalence and disclosure is where recognition skills become essential. This article equips managers, colleagues, and HSE practitioners to notice the observable signs that someone may be struggling — and to respond appropriately. It does not equip anyone to diagnose.
This article provides general HSE and occupational health knowledge. It is not a substitute for professional medical or psychological assessment. Workers showing signs described here should be connected with qualified occupational health professionals, an Employee Assistance Programme (EAP), or a mental health practitioner. Nothing in this article constitutes medical advice.
In practice, the most common failure mode is not a lack of caring — it is confusing performance management with welfare concern. When a previously reliable team member starts missing deadlines, the instinct to address the performance gap is natural. The practitioner approach flips the sequence: a private, non-judgmental check-in about wellbeing comes first. The performance conversation, if still needed, comes second.
What Does Poor Mental Health in the Workplace Look Like?
Mental health difficulties rarely announce themselves with a single dramatic event. They emerge subtly, progressively, and across multiple dimensions of a person’s behaviour before becoming unmistakable. The challenge for managers and colleagues is catching the signal early — when intervention is most effective and least intrusive.
Observable changes tend to cluster into four domains:
| Domain | What to Watch For |
|---|---|
| Behavioural | Mood shifts, irritability, emotional volatility, uncharacteristic quietness |
| Performance | Declining output quality, increased errors, difficulty concentrating or deciding |
| Physical / Appearance | Neglected grooming, visible fatigue, weight fluctuation |
| Social / Relational | Withdrawal from colleagues, skipping team activities, reduced meeting participation |
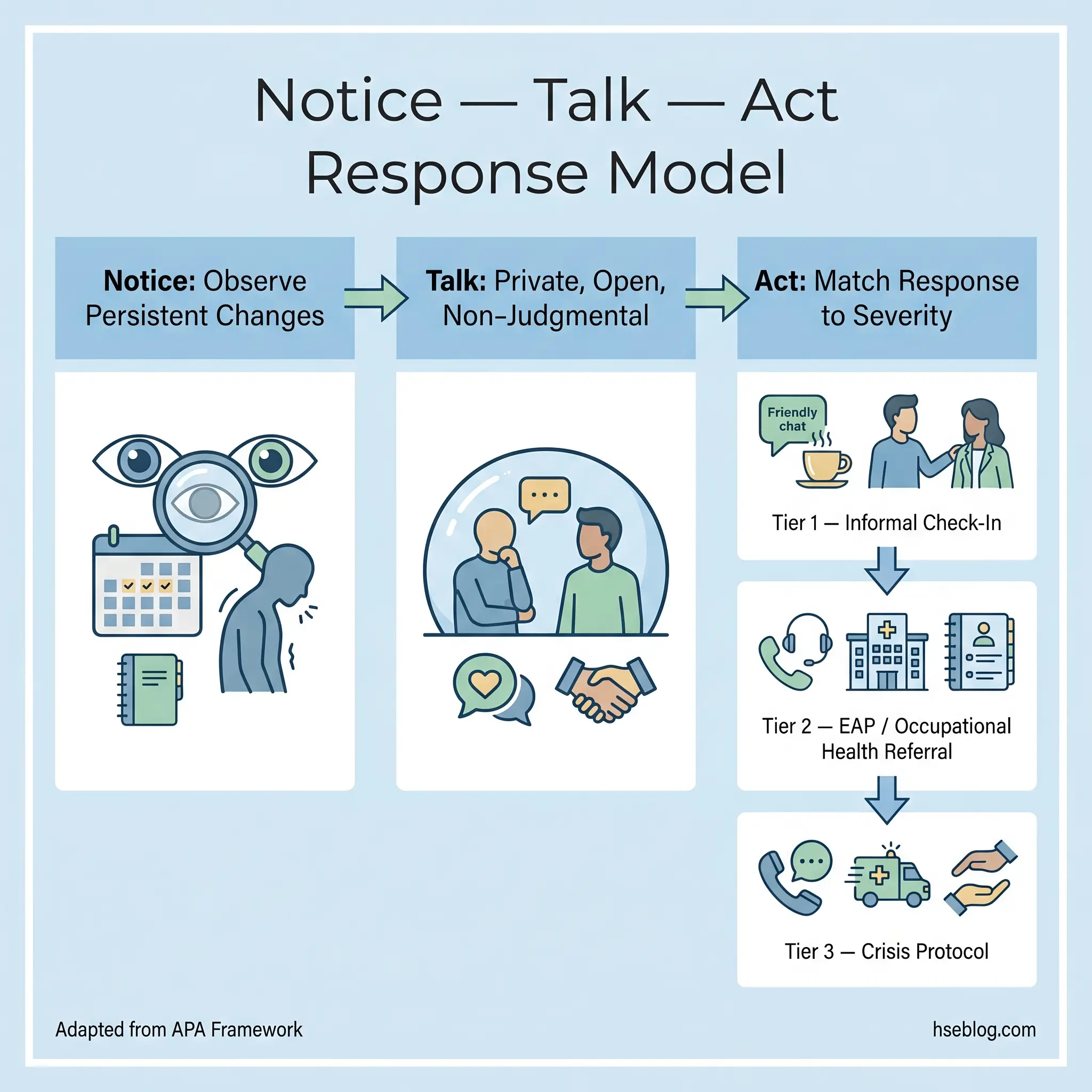
The American Psychological Association’s “Notice. Talk. Act.” framework provides a useful reference model. Notice persistent changes — those sustained over at least two weeks, not a single bad day. Talk by initiating a private, open-ended conversation. Act by connecting the person with appropriate support.
The most commonly missed signals are not the dramatic ones. A previously sociable colleague who starts eating lunch alone, a team member who stops volunteering in meetings, someone who quietly reduces their presence rather than visibly breaking down — these quiet withdrawals are the indicators that pass unnoticed until the situation has deteriorated significantly.
Sign 1: Uncharacteristic Behavioural Changes
The critical word is uncharacteristic. What matters is not absolute behaviour but deviation from an individual’s established baseline.
A naturally reserved person who becomes quieter is a subtler signal than a gregarious person who suddenly falls silent — but both represent meaningful change from their norm.
- Mood swings or emotional flatness. Unpredictable shifts between irritability and withdrawal, or a persistent emotional numbness replacing the person’s usual engagement.
- Uncharacteristic anger or tearfulness. Reactions disproportionate to the triggering situation.
- Gendered presentation differences. Research consistently shows that men experiencing depression more commonly express it through irritability or anger rather than sadness — a pattern that leads to under-recognition.
A common pattern in workplace settings: managers dismiss irritability as an “attitude problem” and route it through performance channels. The practitioner lens asks a different question first — has something changed for this person? Addressing the behavioural surface without investigating the wellbeing underneath misses the actual issue.
Sign 2: Decline in Work Performance and Concentration
Depression reduces cognitive performance approximately 35% of the time (CDC, cited in Purdue University, 2021). That statistic translates into specific, observable workplace effects: slower task completion, increased errors, missed deadlines, and difficulty with decisions that previously came easily.
The distinction that matters is declining quality, not just quantity. A worker may still meet output targets while producing work that requires significantly more checking, rework, or supervision.
What This Looks Like Operationally
- Increased errors, near-misses, or rework. Tasks that were previously completed competently now require correction.
- Decision paralysis. The individual repeatedly defers decisions, seeks excessive reassurance, or avoids committing to a course of action.
- Difficulty prioritising. Work that requires sequencing multiple tasks becomes overwhelming; low-priority items receive attention while critical deadlines pass.
The judgment call for managers is recognising when performance decline is a competence issue versus a wellbeing signal. The differentiator is usually trajectory — a previously competent employee whose output quality drops over weeks is showing a pattern inconsistent with a skills gap. The practitioner standard: welfare inquiry before performance escalation.
Sign 3: Changes in Physical Appearance or Self-Care
When someone stops maintaining grooming or dress standards they previously upheld, the change often reflects a loss of capacity for routine self-care — a recognised feature of depression, severe anxiety, and substance use disorders.
- Neglected personal grooming that represents a departure from the individual’s norm.
- Visible fatigue — persistent dark circles, pallor, or a general appearance of exhaustion.
- Notable weight change in either direction over a short period.
This sign creates discomfort for many managers because commenting on someone’s appearance feels intrusive. The practitioner approach sidesteps the appearance observation entirely and focuses on the wellbeing question: “You don’t seem yourself lately — is everything alright?” The goal is the check-in, not a grooming critique.
Sign 4: Sleep Disruption and Fatigue
Persistent sleep disruption is one of the strongest predictors of mental health deterioration. It appears as a diagnostic criterion in both major depressive disorder and generalised anxiety disorder, and it functions as both a symptom and an accelerant — poor sleep worsens the condition that caused it.
Both extremes matter:
- Insomnia — difficulty falling or staying asleep, leading to exhaustion during working hours.
- Hypersomnia — excessive sleeping that the person cannot seem to recover from.
- Unrestorative sleep — sleeping adequate hours but waking unrefreshed.
Workplace cultures that valorise sleep deprivation — treating late-night emails as commitment, wearing tiredness as a badge — actively mask genuine warning signs. When everyone jokes about being exhausted, the person who is exhausted because of clinical depression blends into the background.
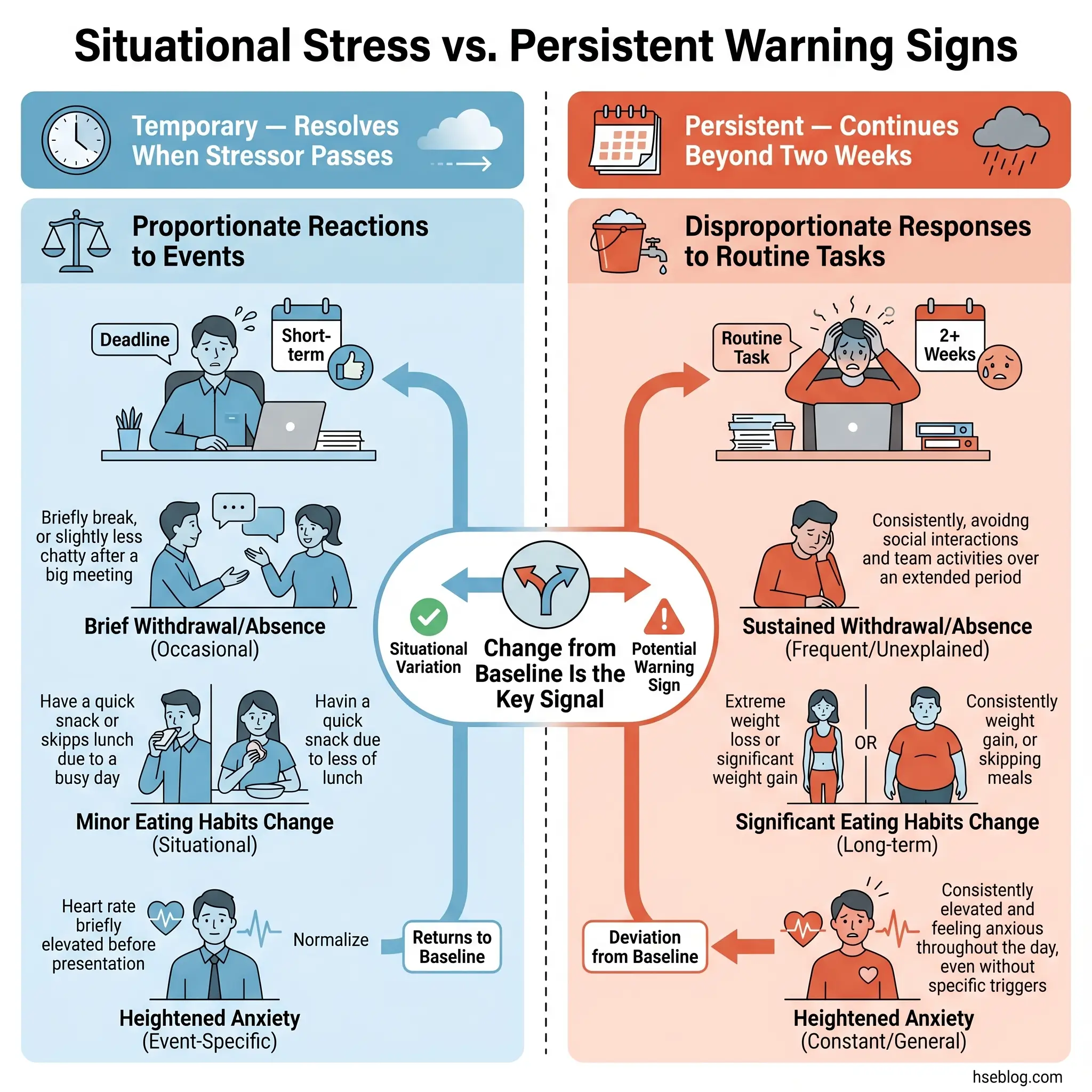
The differentiator is persistence. Project-related tiredness during a deadline push is situational and resolves. Fatigue that stretches across weeks, regardless of workload, and combines with other signs on this list warrants a conversation.
Sign 5: Withdrawal from Colleagues and Social Isolation
Of all the signs on this list, withdrawal is the one most frequently overlooked — precisely because it is quiet. The person is not creating disruption; they are simply receding.
Social support from colleagues is a documented protective factor for workplace mental health. When someone cuts themselves off from that support network, they lose one of the most effective natural buffers against deteriorating mental health.
Observable Indicators
- Avoiding informal interactions — skipping coffee breaks, eating lunch alone, declining after-work invitations when they previously accepted.
- Reduced verbal contribution — speaking less in meetings, offering monosyllabic responses, stopping the small talk that previously characterised their interactions.
- Physical withdrawal cues — working with the door closed, wearing headphones constantly, choosing isolated workstations.
In remote and hybrid environments, the digital equivalents are equally significant: cameras consistently off, monosyllabic chat messages, declining optional video calls, and disappearing from channels where the person previously contributed. These patterns are harder to detect because the baseline for digital interaction is already more distant — which makes intentional monitoring more important, not less.
Sign 6: Increased Absenteeism or Erratic Attendance
In the UK, 22.1 million working days were lost to work-related stress, depression, or anxiety in 2024/25 (HSE, 2025). That figure represents the single largest category of work-related ill health.
Absence patterns linked to mental health conditions tend to differ from other causes. EU-OSHA data indicates that mental-health-related absences are typically longer in duration than those from other conditions. But the pattern that often precedes a long absence is more telling:
- Frequent short-notice absences — particularly recurring patterns tied to specific days of the week.
- Arriving late and leaving early — a compression of the working day that may indicate difficulty getting started or sustaining effort.
- Unexplained disappearances — stepping away from the desk or worksite for extended periods during the day.
Equally important is presenteeism — the employee who is physically present but functionally absent. They appear at their desk, but their output, engagement, and responsiveness are markedly reduced. Research suggests that presenteeism from mental health conditions costs employers more in lost productivity than outright absenteeism, because it persists longer and is harder to detect.
The practitioner pattern to watch: the employee who uses all their sick leave in small increments rather than taking one longer absence. This often indicates someone managing symptoms day-to-day rather than accessing proper support.
Sign 7: Changes in Eating Habits
Skipping meals, avoiding communal eating, overeating, or notable weight change can all signal stress, anxiety, depression, or more complex conditions. The observer’s role is to notice a pattern change — never to comment on someone’s food choices or body.
- Skipping lunch or refusing to eat with colleagues when they previously did.
- Eating at irregular times or visibly different quantities.
- Weight change in either direction over a relatively short period.
The differentiator is change from baseline. Someone who always ate alone is not signalling a problem. Someone who suddenly starts eating alone — especially alongside other signs on this list — may be.
This sign is commonly dismissed as personal preference, which is exactly why it goes unnoticed until more obvious indicators emerge.
Sign 8: Heightened Anxiety, Paranoia, or Irrational Fears
Persistent, disproportionate anxiety is distinct from the normal nervousness that accompanies a challenging project or a difficult meeting. The distinction lies in proportionality and duration.
Recognising the Pattern
- Excessive worry disproportionate to actual risk. Catastrophising about routine tasks or outcomes. Repeated “what if” spirals about unlikely scenarios.
- Paranoid or suspicious thinking. Interpreting neutral management decisions as personal threats. Believing colleagues are conspiring against them without evidence.
- Physical anxiety manifestations. Sweating, trembling, rapid breathing, or difficulty speaking in meetings — particularly when these are new behaviours.
A common anxiety pattern that is rarely flagged as a mental health indicator: the employee who repeatedly seeks reassurance about decisions already made. This “checking loop” — returning to confirmed answers multiple times — reflects an inability to tolerate uncertainty rather than a lack of understanding. Managers who interpret it as a competence gap miss the underlying condition.
The judgment call: situational stress resolves when the stressor passes. Anxiety that persists beyond the triggering event, or that attaches itself to new situations as soon as the previous one is resolved, warrants a wellbeing conversation.
Sign 9: Increased Substance Use or Reliance on Coping Mechanisms
Self-medication with alcohol, drugs, or other substances is a common response to untreated mental health conditions. It creates a compound problem: the underlying condition remains unaddressed while the substance use introduces its own health and safety risks.
Observable indicators include:
- Smelling of alcohol during working hours or on arrival.
- Impaired functioning — slurred speech, unsteady movement, slowed reactions — particularly when intermittent rather than constant.
- References to heavy consumption — casual mentions of heavy weekend drinking, increased caffeine or energy drink reliance, or jokes about “needing a drink to get through the day.”
The safety dimension is unavoidable. Impairment at work creates risk for the individual and everyone around them, particularly in operational environments. Under the ADA (US), current illegal drug use is not a protected condition, though substance use disorder itself may qualify as a disability. Employers are not required to tolerate impairment on the job regardless of disability status.
The practitioner challenge is separating the welfare response from the disciplinary response. Both may be necessary, but sequencing matters. Leading with safeguarding — “I’m concerned about you, and I want to make sure you get the right support” — before any sanction improves outcomes for the individual and the organisation. The disciplinary process, if required, remains available. But starting there closes the door that the welfare conversation might have opened.
Sign 10: Expressing Hopelessness or Making Concerning Statements
This is the highest-severity indicator on this list. Statements expressing hopelessness, feeling trapped, or referencing self-harm require immediate, calm, direct action — not monitoring over time.
Phrases that should always be taken seriously:
- “What’s the point?”
- “Everyone would be better off without me.”
- “I just can’t do this anymore.”
- Dark humour about death that is persistent or escalating.
- Any explicit reference to suicide or self-harm.
Every other sign on this list can escalate to this point if left unaddressed. The APA’s guidance — that persistent changes of at least two weeks warrant attention — does not apply here. Explicit concerning statements warrant immediate response regardless of how long they have been occurring.
What to Do
- Do not leave the person alone. Stay with them or ensure someone trusted stays with them.
- Ask directly and calmly. Evidence consistently shows that asking someone if they are thinking about suicide does not put the idea in their head. Asking directly is protective, not provocative.
- Follow your organisation’s safeguarding protocol. If none exists, connect the person with crisis services immediately.
- Do not promise confidentiality you cannot keep. You may need to involve others to keep the person safe.
Crisis Resources:
- US: 988 Suicide & Crisis Lifeline — call or text 988
- UK: Samaritans — call 116 123 (free, 24/7)
- International: Find your local crisis line at findahelpline.com
Many managers fear that raising the subject of suicidal thoughts will make things worse. The published evidence is clear and consistent on this point: asking directly, in a private setting, with calm concern, is one of the most protective actions a non-clinical person can take.
What Causes Poor Mental Health in the Workplace?
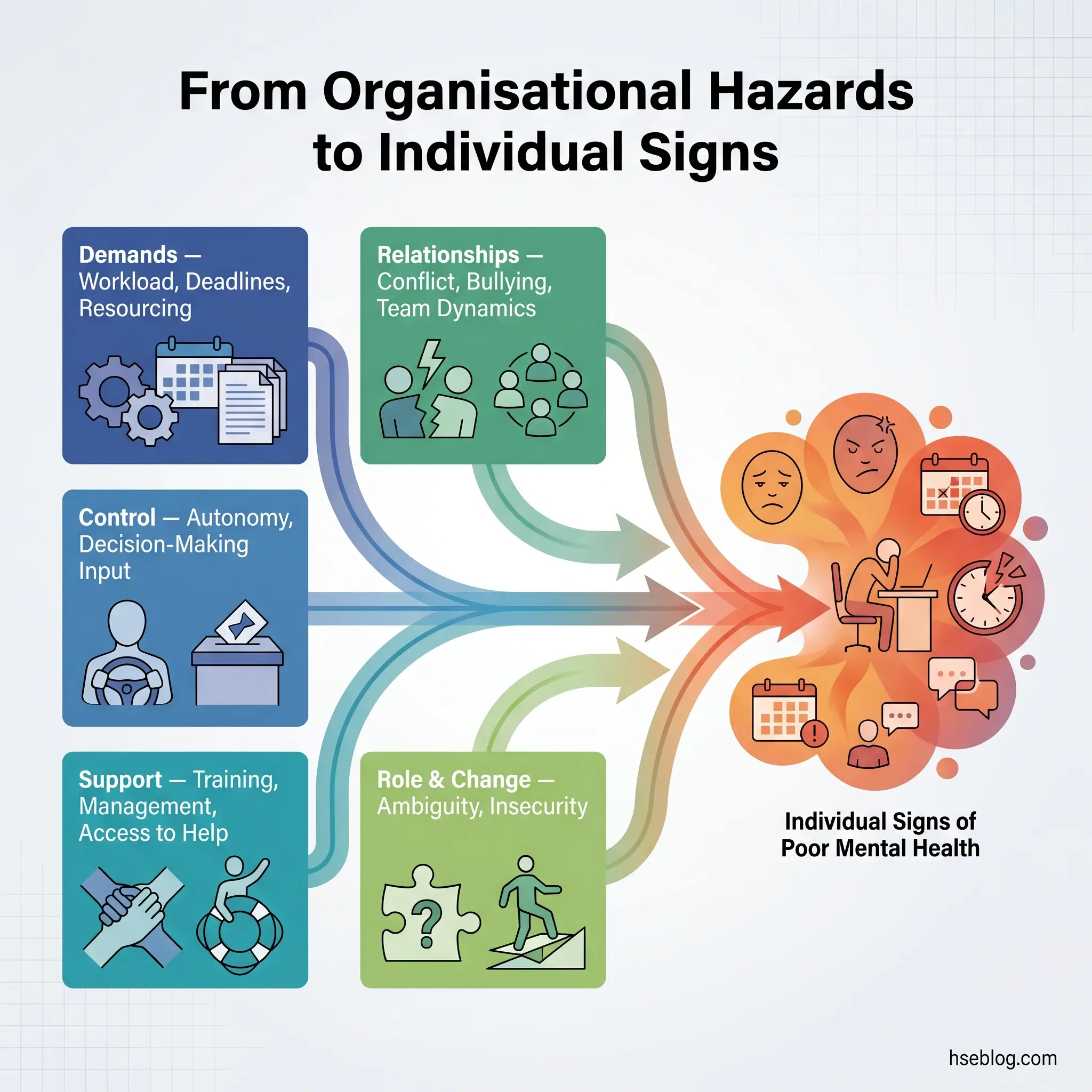
Individual signs do not emerge in a vacuum. They develop within organisational conditions — and those conditions are identifiable, assessable, and manageable using the same risk-management approach applied to any other workplace hazard.
The HSE Management Standards for work-related stress (UK) define six domains that, when poorly managed, generate psychosocial risk:
| HSE Management Standard Domain | Example Workplace Condition |
|---|---|
| Demands | Unmanageable workloads, unrealistic deadlines, inadequate resourcing |
| Control | Low autonomy, no input into how work is done, rigid micromanagement |
| Support | Insufficient training, absent management, no access to EAP or occupational health |
| Relationships | Bullying, harassment, unresolved interpersonal conflict, poor team dynamics |
| Role | Role ambiguity, conflicting responsibilities, unclear expectations |
| Change | Poorly communicated restructures, job insecurity, inadequate consultation |
ISO 45003:2021 — the global voluntary standard for psychological health and safety at work — organises psychosocial hazards into three categories: work organisation, social factors at work, and work environment. The WHO’s 2022 Guidelines on Mental Health at Work identify overlapping risk factors including excessive workloads, low job control, job insecurity, workplace violence, and discrimination (WHO fact sheet on mental health at work).
A common organisational blind spot: many employers address individual symptoms — offering EAP referrals, mental health awareness days, resilience training — while leaving the root psychosocial hazards untouched. This treats consequences rather than causes. If the demands domain is generating chronic overwork across a department, no amount of individual counselling will resolve the pattern. The hazard itself must be assessed and controlled.
How to Respond When You Notice These Signs
The graduated response — from informal check-in to crisis intervention — is what separates an effective response from a well-intentioned but unhelpful one. Not every sign on this list requires the same action.
Step 1: Notice
Observe persistent changes across the four domains. Document what you observe factually — behaviour, attendance, performance patterns — not your interpretation of the cause.
Persistence matters. The APA’s two-week threshold is a useful calibration point: sustained change over at least two weeks, not a single difficult day, is the trigger for action.
Step 2: Talk
Choose a private, uninterrupted setting. Not a corridor. Not a rushed five minutes before a meeting.
- Ask open questions: “How are things going for you?” or “I’ve noticed you seem a bit different lately — is there anything I can do?”
- Listen without judgement. Do not attempt to diagnose or explain what you think is wrong.
- Accept that the person may not be ready to talk. Acknowledge that, and leave the door open.
The most common manager error is having this conversation in a rushed, semi-public setting. The practitioner standard is a scheduled, private, uninterrupted conversation — and acceptance that one conversation may not be enough.
Step 3: Act
Signpost to appropriate support based on the severity and context:
- Informal check-in level — the person acknowledges difficulty but is functioning. Offer to adjust workload, flag the EAP, check in again.
- EAP / occupational health referral — signs are persistent, affecting work, or the person requests support. Connect them with the organisation’s EAP or refer to occupational health.
- Crisis response — concerning statements about self-harm or hopelessness. Follow the organisation’s safeguarding protocol immediately. Use crisis resources listed under Sign 10.
The legal boundary is clear: managers should focus on observable behaviour and work performance. Attempting to diagnose a condition crosses into territory that both the ADA (US) and the Equality Act 2010 (UK) restrict. The appropriate question is about wellbeing and work, not about medical conditions.
Reasonable accommodations — flexible scheduling, modified duties, adjusted workload, phased return from absence, quiet workspace — are available under the ADA (US) and Equality Act 2010 (UK), provided they do not cause undue hardship to the employer. Each case is assessed individually.
Employer Legal Duties for Workplace Mental Health
This section provides general orientation on legal frameworks. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.
Regulatory enforcement on psychosocial risk management is tightening across jurisdictions. Organisations treating mental health solely as a wellbeing initiative — rather than a compliance obligation — face increasing exposure.
United Kingdom
The Health and Safety at Work etc. Act 1974 and the Management of Health and Safety at Work Regulations 1999 (Regulations 3, 4, and 5) create an enforceable duty to assess and manage all workplace risks, including psychosocial hazards. The HSE Management Standards provide the compliance framework.
Enforcement is no longer theoretical. In 2025, HSE UK served Notices of Contravention for failure to manage work-related stress on the East of England Ambulance Service (April 2025) and the University of Birmingham (December 2025) — marking a significant escalation in regulatory action on psychosocial risk (HSE / Clyde & Co, 2025). In 2024/25, 964,000 workers in Great Britain reported work-related stress, depression, or anxiety (HSE, 2025).
United States
OSHA’s General Duty Clause — Section 5(a)(1) — requires employers to provide a workplace free from recognised hazards causing or likely to cause death or serious physical harm. Application to psychosocial hazards is emerging but no specific federal standard yet exists. The ADA requires employers with 15 or more employees to provide reasonable accommodations for qualified individuals with mental health conditions, unless doing so causes undue hardship.
European Union
The Framework Directive 89/391/EEC requires employers to assess and manage all workplace risks, including psychosocial risks. This is supported by social partners’ framework agreements on work-related stress (2004) and harassment and violence at work (2007).
Global Framework
ISO 45003:2021 provides a voluntary but authoritative management framework for psychosocial risk within occupational health and safety management systems based on ISO 45001. While not legally binding, it represents the current international consensus on what good practice looks like.
Regulatory currency note: The legal content in this section reflects general HSE professional understanding of requirements as of 2025. Regulatory frameworks evolve. Verify current requirements with qualified legal counsel in the applicable jurisdiction.
Frequently Asked Questions
Conclusion
The gap the industry has not closed is the space between noticing and acting. Most managers and colleagues can sense when something is wrong. Where the system breaks down is in what happens next — or, more commonly, what doesn’t happen. Signs get attributed to personality, to laziness, to bad attitude, to personal problems that are “not the company’s business.” By the time the organisation responds, the opportunity for early intervention has passed and the situation has escalated into crisis, long-term absence, or both.
The highest-impact change most organisations can make is not another awareness poster or a mental health day. It is training line managers to have one conversation — a private, calm, non-judgmental welfare check-in — when they notice persistent change. That single capability, embedded as a standard management practice rather than an optional extra, intercepts the majority of escalations before they reach the point where professional intervention becomes urgent.
Recognising the signs of poor mental health in the workplace is not a clinical skill. It is an observation skill backed by the willingness to act. The ten signs covered here are observable, documentable, and — most importantly — respondable. What turns observation into impact is the conversation that follows.