TL;DR — What Every Employer Needs to Know
- Workplace mental health is a legal obligation, not a benefit. Employers in the US, UK, EU, and Australia face enforceable duties to assess and manage psychosocial risks — and regulators are actively enforcing them.
- Organizational interventions come before individual ones. WHO evidence shows that fixing work design, management practices, and job demands reduces distress more effectively than offering apps or resilience training alone.
- Manager training is the highest-leverage single intervention. WHO guidelines identify it as the critical link — yet only about 20% of employees report receiving any mental health training at work (NAMI, 2026).
- Measure outcomes, not activities. Track psychosocial risk scores, stress-related absence, and willingness-to-disclose — not just how many training sessions you ran.
- The ROI is documented. WHO estimates approximately $4 return per $1 invested in treating depression and anxiety at work (WHO, various years).
Workplace mental health refers to the psychological well-being of employees as influenced by work design, organizational practices, management behaviors, and workplace culture. Employers have legal duties across most jurisdictions to assess and manage psychosocial risks — factors like excessive workload, poor job control, bullying, and role ambiguity — that can cause or worsen mental health conditions among workers.
Why Workplace Mental Health Is an Employer Responsibility — Not a Perk
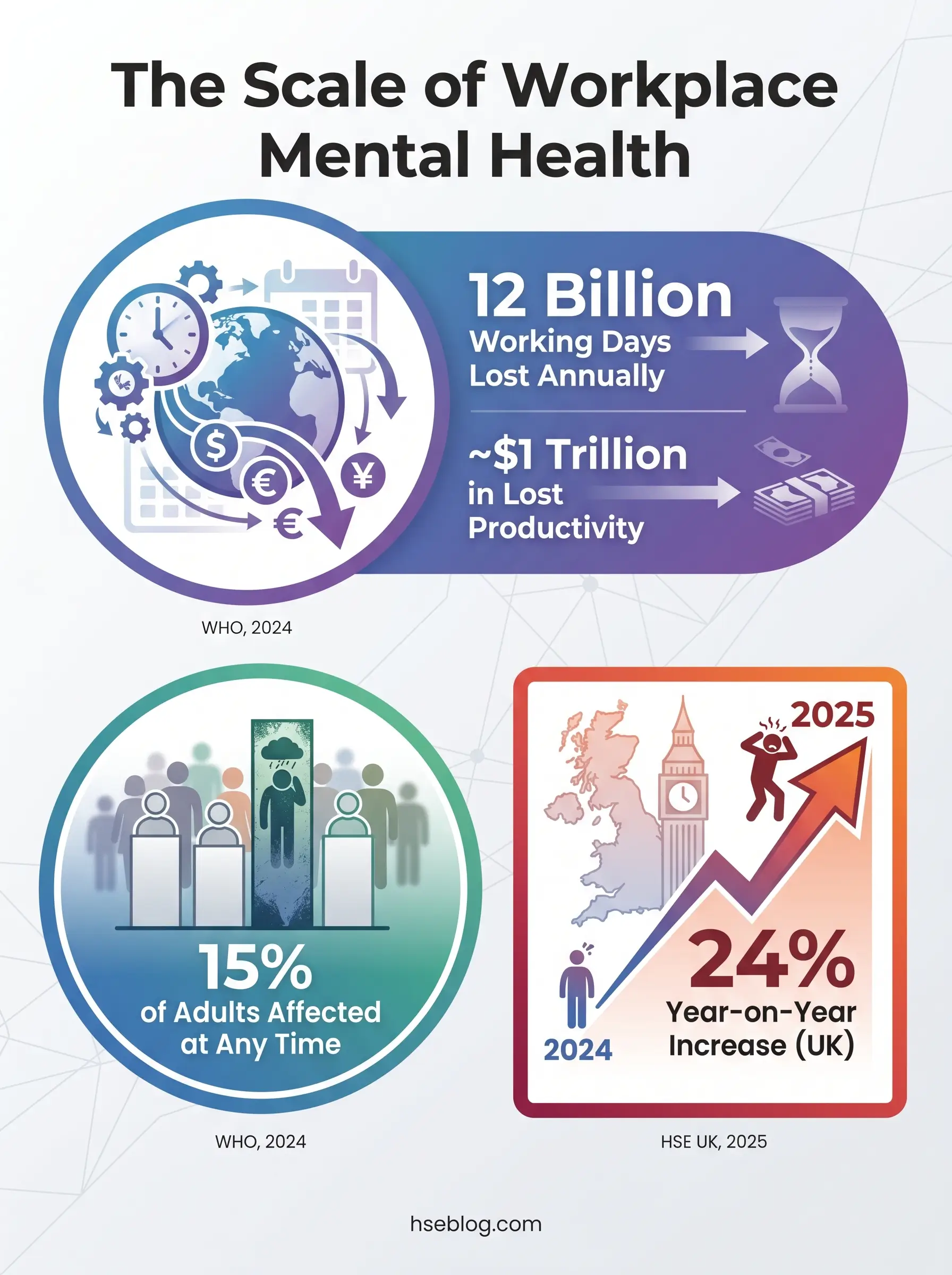
Depression and anxiety alone cost an estimated 12 billion working days and approximately $1 trillion in lost productivity every year globally (WHO, 2024). That figure is not a wellness talking point — it is a measure of organizational failure at scale.
Approximately 15% of working-age adults have a mental disorder at any point in time (WHO, 2024). In Great Britain, the 2024/25 Labour Force Survey found 964,000 workers reporting work-related stress, depression, or anxiety — a 24% increase from the prior year’s 776,000 — accounting for 52% of all work-related ill health (HSE UK, 2025).
The instinct many employers follow is to treat mental health as a benefits-line-item: purchase an Employee Assistance Program, promote a meditation app, run a wellness week. The evidence points in a different direction entirely.
The WHO guidelines on mental health at work and ISO 45003:2021 both frame mental health as an occupational hazard management problem. The intervention model that works is the same one used for physical hazards:
- Identify the hazard at its source — work design, management behavior, organizational culture
- Assess the risk using structured tools and worker consultation
- Control the hazard through organizational change before defaulting to individual coping strategies
What Is Psychosocial Risk and Why Should Employers Manage It?
Psychosocial risk refers to workplace factors — arising from how work is designed, organized, managed, and socially structured — that increase the probability of work-related stress and psychological or physical harm. ISO 45003:2021 defines these hazards as distinct from physical workplace hazards but requiring the same systematic assessment and control.
The confusion most employers face is conflating psychosocial risk with “stress.” Work-related stress is the outcome — the symptom an employee experiences. Psychosocial hazards are the causes, embedded in the organization itself.
The Six Domains That Drive Psychosocial Risk
The UK’s HSE Management Standards for work-related stress provide the most practical taxonomy available. Six domains cover the full spectrum of organizational factors:
| Domain | What It Covers | Warning Indicators |
|---|---|---|
| Demands | Workload, work pace, work patterns, work environment | Sustained overtime, unachievable deadlines, emotional labor without support |
| Control | Autonomy over how work is done | Micromanagement, no input into scheduling, rigid process with no discretion |
| Support | Resources, management support, peer support | No regular supervision, inadequate tools, isolated working |
| Relationships | Conflict, bullying, harassment | Unresolved grievances, patterns of interpersonal conflict, harassment reports |
| Role | Role clarity, absence of conflicting demands | Contradictory instructions, unclear reporting lines, scope creep without discussion |
| Change | How organizational change is communicated and managed | Restructures without consultation, rumor replacing communication |
The WHO’s list of psychosocial risk factors aligns closely: excessive workloads, low job control, bullying, harassment, job insecurity, poor communication, and role ambiguity all appear across both frameworks.
One dimension that gets overlooked is how psychosocial hazards interact with physical hazards. Fatigue from excessive hours does not merely affect mental health — it directly increases injury risk. Cognitive impairment from chronic stress degrades hazard recognition. The two categories are not separate management problems.
The corrective for employers is to apply the hierarchy of controls to psychosocial hazards. Eliminate or redesign the hazard at its organizational source before defaulting to individual coping strategies — training workers to be “resilient” against a badly designed job is the equivalent of issuing earplugs instead of enclosing a noisy machine.
Legal Obligations Employers Must Know Across Jurisdictions
Employer obligations around psychosocial risk are not aspirational — they carry enforcement consequences. The specific requirements vary by jurisdiction, but the direction of travel is uniform: regulators are moving toward explicit psychosocial hazard management duties.
United States
US employers face a patchwork of overlapping statutes:
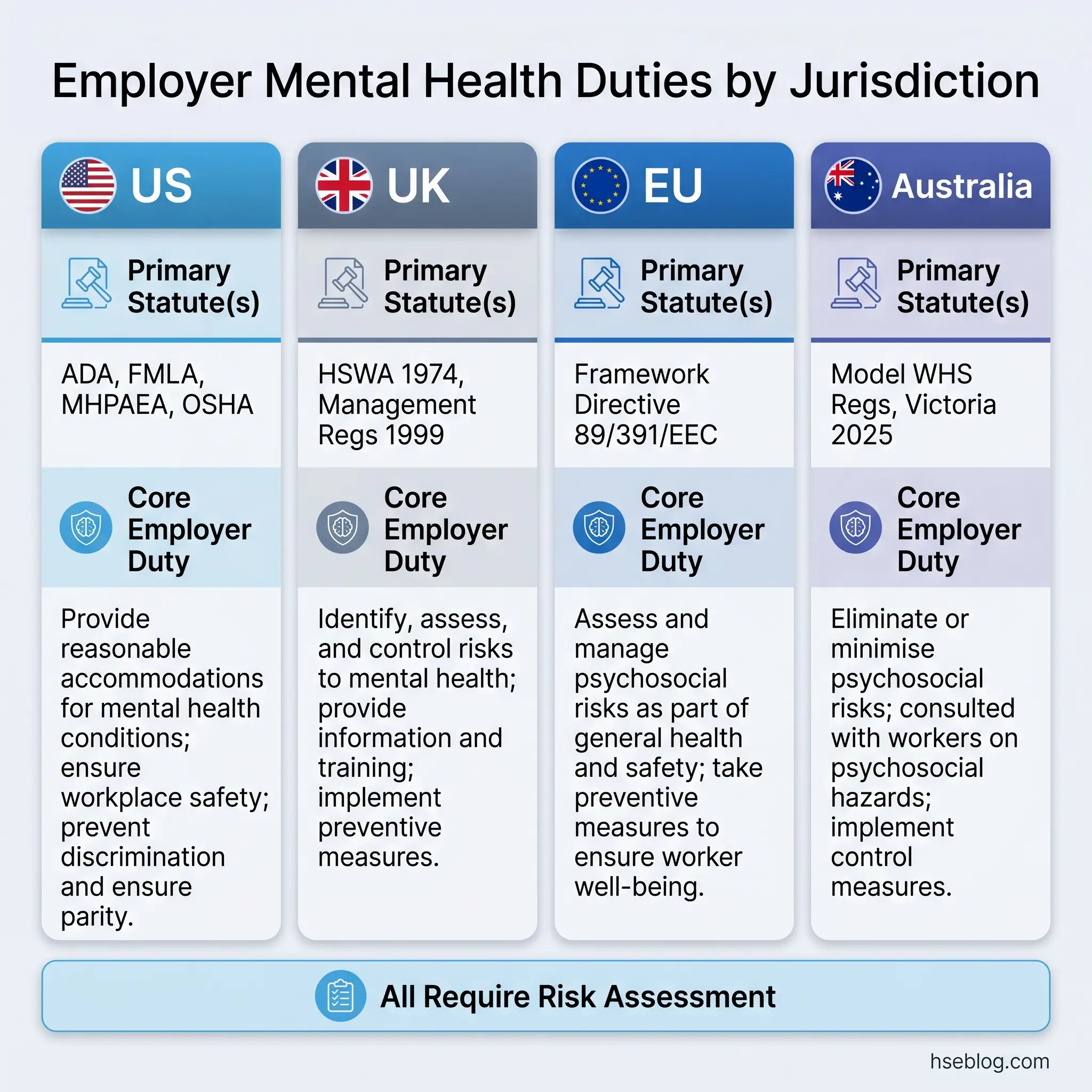
- ADA (42 U.S.C. § 12101 et seq.) — Prohibits discrimination against employees with mental health conditions and requires reasonable accommodations unless the employer can demonstrate undue hardship. The EEOC guidance on mental health conditions and workplace rights specifies that conditions like major depression, PTSD, bipolar disorder, and anxiety disorders qualify as disabilities under the ADA Amendments Act 2008.
- FMLA (29 U.S.C. § 2601 et seq.) — Provides up to 12 weeks of job-protected unpaid leave for serious health conditions, including mental health conditions requiring inpatient care or continuing treatment.
- MHPAEA (2024 final rules) — Health plans covering mental health benefits cannot impose more restrictive limitations than on comparable medical/surgical benefits. The 2024 final rules strengthened enforcement by requiring plans to demonstrate parity through outcomes data, not just plan design.
- OSHA General Duty Clause — The obligation to maintain a workplace free from recognized hazards extends, in interpretation, to psychosocial factors — though OSHA has not yet issued a standalone psychosocial standard.
United Kingdom
The UK framework is more direct on psychosocial obligations:
- Health and Safety at Work Act 1974 (UK) — The employer’s duty to ensure, so far as is reasonably practicable, the health, safety, and welfare of employees includes psychological health. Courts have consistently interpreted this to cover work-related stress.
- Management of Health and Safety at Work Regulations 1999, Regulations 3, 4, and 5 (UK) — Require suitable and sufficient risk assessment of all risks, including psychosocial risks, and the application of principles of prevention.
- Equality Act 2010 (UK) — Mental health conditions that substantially affect day-to-day activities qualify as disabilities, triggering duties for reasonable adjustments.
European Union
The EU Framework Directive 89/391/EEC places a broad obligation on employers to assess and manage all workplace risks, which EU-OSHA guidance explicitly extends to psychosocial hazards. Member states implement this through national legislation with varying specificity.
Australia
Australia has moved furthest, fastest. Model WHS Regulations now include psychosocial hazard provisions (Regulations 55A–55F) requiring persons conducting a business or undertaking to identify psychosocial hazards, eliminate risks so far as reasonably practicable, and maintain and review control measures. Victoria’s Occupational Health and Safety (Psychological Health) Regulations 2025, effective 1 December 2025, go further — requiring employers to apply a hierarchy of controls specifically to psychosocial risks and strengthening consultation requirements with health and safety representatives.
Enforcement Is Real: What Happens When Employers Fail
The assumption that psychosocial duties are soft obligations — present in law but never enforced — collapses under recent enforcement data. Three cases illustrate the range:
- HSE UK — East of England Ambulance Service (April 2025). HSE served a Notice of Contravention specifically for failure to manage work-related stress, citing material breaches of Regulations 3, 4, and 5 of the Management of Health and Safety at Work Regulations 1999 (UK). The regulator did not require proof that stress had been eliminated — it required documented risk assessment, active controls, and evidence of monitoring. The organization had none.
- Australia — Elisha v Vision Australia Limited. The employer was ordered to pay A$1.4 million in damages for psychiatric injury caused by breaching its own grievance procedures. The court found that the employer’s failure to follow its own documented processes directly caused foreseeable psychological harm.
- US — EEOC enforcement. The EEOC continues to pursue ADA violations where employers refuse or fail to provide reasonable accommodations for mental health conditions, including cases involving denial of leave, failure to engage in the interactive accommodation process, and retaliatory termination following disclosure.
The pattern across all three jurisdictions is consistent: regulators do not require employers to eliminate stress entirely. They require documented risk assessment, active controls, and evidence of monitoring. Organizations that face enforcement typically had no documented psychosocial risk assessment at all.
How to Build a Workplace Mental Health Strategy: A Framework for Employers
The single most important sequencing decision in any employer mental health program is this: organizational-level interventions must come before individual-level interventions. WHO evidence shows that organizational interventions — changing work design, management practices, and job demands — reduce emotional distress and improve work-related outcomes. Individual interventions alone are insufficient.
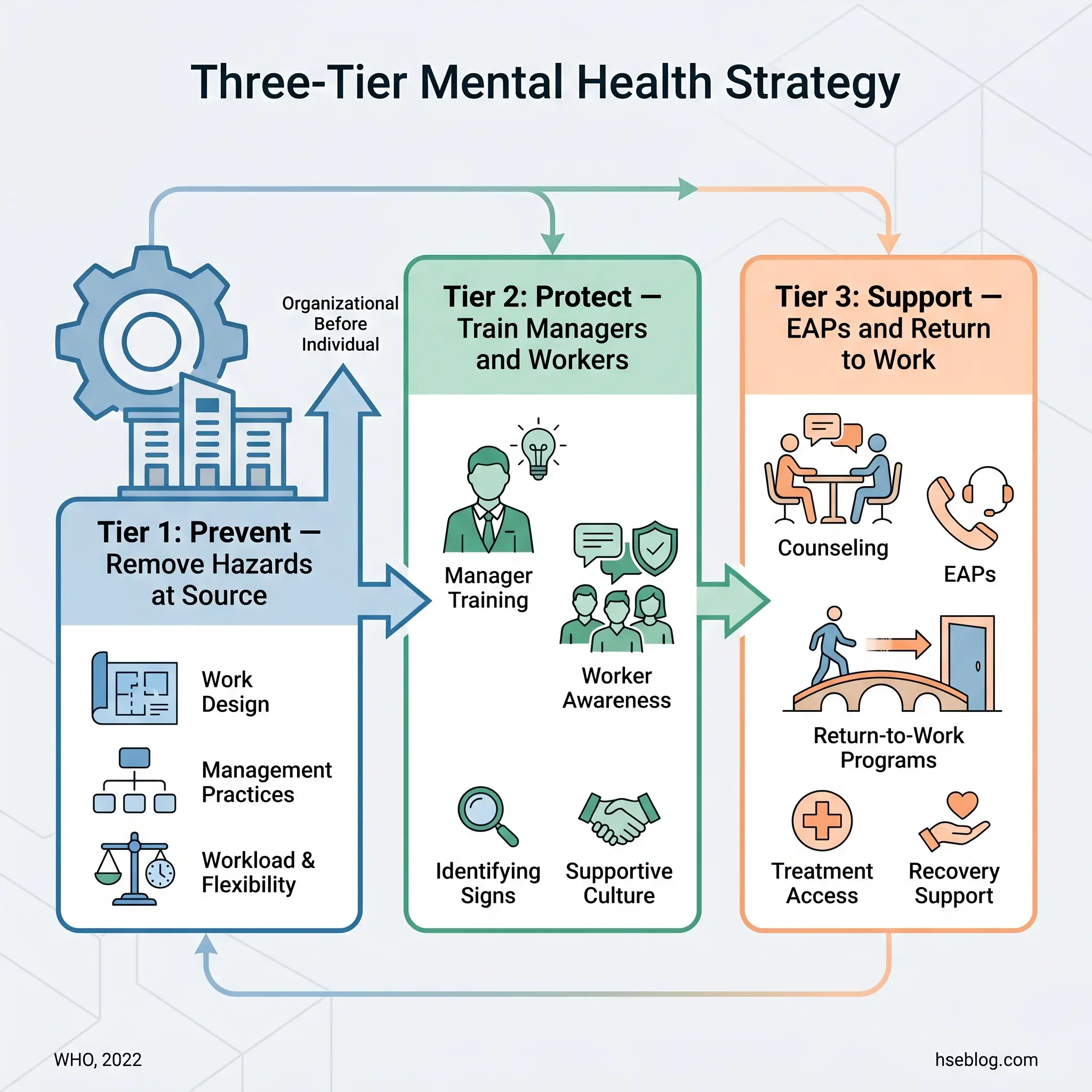
The practical framework draws on WHO’s three-tier model and integrates with ISO 45003’s Plan-Do-Check-Act cycle:
Tier 1 — Prevent: Eliminate or Reduce Psychosocial Hazards at Source
This is the organizational intervention layer. Before purchasing any wellness platform or launching any training, employers must assess what hazards their own systems are generating.
- Conduct a baseline psychosocial risk assessment. Use structured tools — the HSE Indicator Tool is freely available and validated. Supplement with absence data analysis, exit interview patterns, and EAP utilization trends.
- Identify the top three to five hazard domains scoring poorly. Prioritize by severity and number of workers affected.
- Design organizational controls. Workload redistribution, role clarification, improved change communication, management accountability for team wellbeing indicators.
Tier 2 — Protect and Promote: Build Capability Across the Organization
Once the organizational hazards are being addressed, build the human infrastructure:
- Manager training on recognizing distress, having supportive conversations, understanding accommodation obligations, and knowing referral pathways (addressed in detail in the next section).
- Worker awareness — ensuring every employee knows what resources exist, how to access them, and that doing so carries no career penalty.
- Anti-stigma initiatives grounded in operational language, not slogans. Normalize discussing workload, fatigue, and pressure as operational risks.
Tier 3 — Support: Individual Interventions and Return to Work
This is where EAPs, counseling access, digital mental health tools, mental health first aid training, and return-to-work programs sit. These are essential — but they cannot substitute for Tiers 1 and 2.
The judgment call for employers is resisting the temptation to start at Tier 3 because it is fastest to procure. An EAP is a purchase order. Redesigning job demands requires organizational change. The sequence matters because workers will not trust or use Tier 3 resources if Tier 1 hazards remain unaddressed.
Writing a Mental Health Policy That Actually Works
A workplace mental health policy is the governance document that holds the strategy together. The most common policy failure is a document that lists aspirational values but contains no named responsible person, no defined review cycle, and no connection to risk assessment findings. A policy that cannot be audited cannot be enforced internally.
Essential elements for an operationally credible policy:
- Purpose and scope — applies to all workers including remote, hybrid, contract, and part-time
- Legal obligations referenced — cite the specific statutes applicable to the organization’s jurisdiction
- Psychosocial hazard definitions aligned with ISO 45003 and/or HSE Management Standards
- Roles and responsibilities — named individuals or role-holders accountable for each element
- Confidentiality protections — explicit limits on who has access to health information
- Complaint and reporting procedures — accessible, documented, and non-retaliatory
- Anti-discrimination commitments — linked to ADA (US), Equality Act (UK), or equivalent
- Review schedule — annual minimum, triggered by organizational change or incident data
Manager Training: The Critical Intervention Most Employers Get Wrong
WHO guidelines identify manager mental health training as a core recommended intervention — and the evidence supports the emphasis. Effective manager training improves mental health-related knowledge, attitudes, and skills among managers, and increases help-seeking behavior among workers they supervise.
The gap is enormous. The 2026 NAMI-Ipsos Workplace Mental Health Poll found that only about 20% of respondents receive training about mental health conditions or symptoms (NAMI, 2026). Most organizations have not equipped the people with the most direct influence over daily work conditions to recognize distress, respond appropriately, or refer effectively.
What Effective Training Covers — and Where the Line Falls
The content of manager training must be carefully bounded. Managers are not clinicians, and training that blurs that boundary generates liability and undermines trust.
What training should include:
- Recognition — observable changes in behavior, performance, attendance, or engagement that may indicate distress
- Conversation skills — how to open a supportive, non-diagnostic conversation that focuses on wellbeing and work performance
- Legal literacy — understanding accommodation obligations, confidentiality requirements, and anti-discrimination duties specific to the organization’s jurisdiction
- Referral pathways — when and how to connect employees with EAP, occupational health, or HR resources
What training must explicitly exclude:
- Diagnosis — managers should never be positioned to identify specific conditions
- Therapeutic intervention — supportive conversation is not counseling
- Pressure to disclose — employees have the right to keep diagnoses private; managers must focus on functional needs, not labels
Effective vs. Ineffective Approaches
The common failure mode is the one-off awareness session. A two-hour webinar during Mental Health Awareness Week generates temporary enthusiasm and zero sustained behavioral change. The misconception is that awareness equals capability — knowing that mental health matters is not the same as knowing what to do when an employee is struggling.
Effective programs embed mental health into ongoing management development. They include role-play or scenario-based practice, refresh annually at minimum, and evaluate managers on wellbeing indicators — not just productivity targets. The difference is between a calendar event and a management competency.
Employee Assistance Programs and Mental Health Benefits: What Works
EAPs remain the most widely deployed employer mental health resource, typically costing $12–$40 per employee per year. WHO estimates approximately $4 return per $1 invested in treating depression and anxiety in the workplace (WHO, various years). Deloitte’s research corroborates that ROI improves when programs span the full spectrum — from promotion to prevention to intervention to care — rather than offering only reactive services.
The utilization problem, however, is persistent and widely misunderstood.
The Awareness Gap
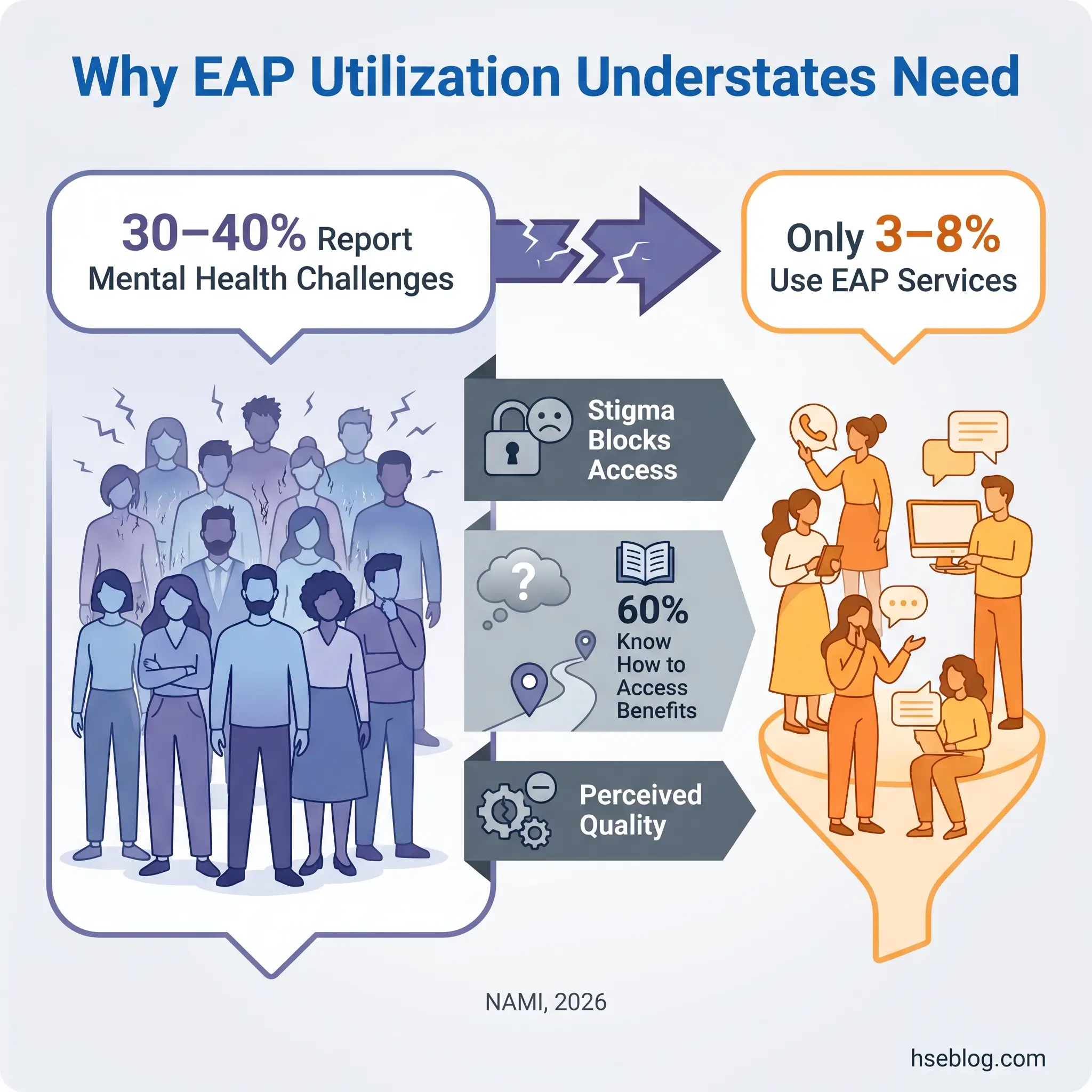
The 2026 NAMI-Ipsos Workplace Mental Health Poll found that only six in ten employees know how to access mental health care through their employer-sponsored health insurance (NAMI, 2026). The same poll found that 57% of employees report receiving no training about workplace mental health resources.
Low EAP utilization — typically 3–8% of the workforce in any given year — is frequently interpreted by employers as evidence of low need. That interpretation is almost always wrong. Self-reported mental health challenges typically affect 30–40% of a workforce. The gap between reported need and service engagement reflects stigma, lack of awareness, and perceived quality concerns — not an absence of demand.
Insurance Parity: MHPAEA Requirements (US)
Sites operating under US jurisdiction must comply with the Mental Health Parity and Addiction Equity Act. The requirement is straightforward: health plans cannot impose more restrictive limitations on mental health and substance use disorder benefits than on comparable medical/surgical benefits. The 2024 final rules strengthened this by requiring plans to demonstrate parity through outcomes data.
Emerging Tools
Digital CBT platforms, peer support networks, and mental health first aid training programs are expanding the intervention landscape beyond traditional EAP models. These tools are most effective when integrated into a broader strategy — not deployed as standalone substitutes.
| Intervention Tier | Examples | Cost Range | Best Used When |
|---|---|---|---|
| Promotion | Anti-stigma campaigns, awareness training | Low | Building organizational culture |
| Prevention | Psychosocial risk assessment, job redesign | Medium | Addressing root causes |
| Early Intervention | Manager referral, digital CBT, peer support | Low–Medium | Early signs of distress |
| Treatment | EAP, counseling, clinical referral | Medium–High | Diagnosable conditions |
Measuring the Impact: KPIs for Workplace Mental Health Programs
The trap employers fall into is measuring activity rather than outcomes. Counting the number of training sessions delivered, the number of EAP referrals made, or the number of wellness events hosted creates a false sense of progress. These are output metrics — they tell you what you did, not whether it worked.
Effective measurement distinguishes between leading and lagging indicators, tracks them at appropriate frequencies, and ties them back to baseline data established before program launch.
Leading vs. Lagging Indicators
| Indicator Type | Metric | Measurement Tool | Frequency |
|---|---|---|---|
| Leading | Psychosocial risk survey scores | HSE Indicator Tool or equivalent | Annually minimum |
| Leading | Manager training completion + competency | Post-training assessment | After each cohort |
| Leading | Policy awareness rates | Employee survey | Annually |
| Leading | Willingness-to-disclose scores | Confidential survey | Annually |
| Lagging | Stress-related sickness absence | HR absence data | Quarterly |
| Lagging | EAP utilization + outcome data | EAP provider reports | Quarterly |
| Lagging | Presenteeism measures | Validated scale (e.g., SPS-6) | Annually |
| Lagging | Turnover attributed to wellbeing | Exit interview analysis | Quarterly |
| Lagging | Workers’ compensation claims — psychological injury | Claims data | Annually |
Frequency and Baseline
Annual psychosocial risk surveys are the minimum. Quarterly reviews of absence and EAP utilization data catch emerging trends before they become entrenched. During periods of organizational change — restructures, mergers, redundancy programs — real-time pulse checks are warranted.
Deloitte’s research reinforces that performance measurement is often the most overlooked element: companies that track baseline data and measure incrementally achieve greater program ROI than those that deploy interventions without establishing what they are measuring against.
The judgment call for most organizations is whether to invest in rigorous baseline measurement before launching interventions, or to start interventions immediately and measure retrospectively. The evidence favors establishing a baseline first. Without it, you cannot distinguish program impact from regression to the mean.
What Does a Psychologically Safe Return-to-Work Process Look Like?
The most damaging return-to-work failure is the “cliff edge” return — an employee goes from full absence to full duties overnight with no transition plan, no management check-in, and implicit pressure to perform at pre-absence levels immediately. This drives relapse and repeat absence, which is worse for the employee and more costly for the organization than a properly graduated return.
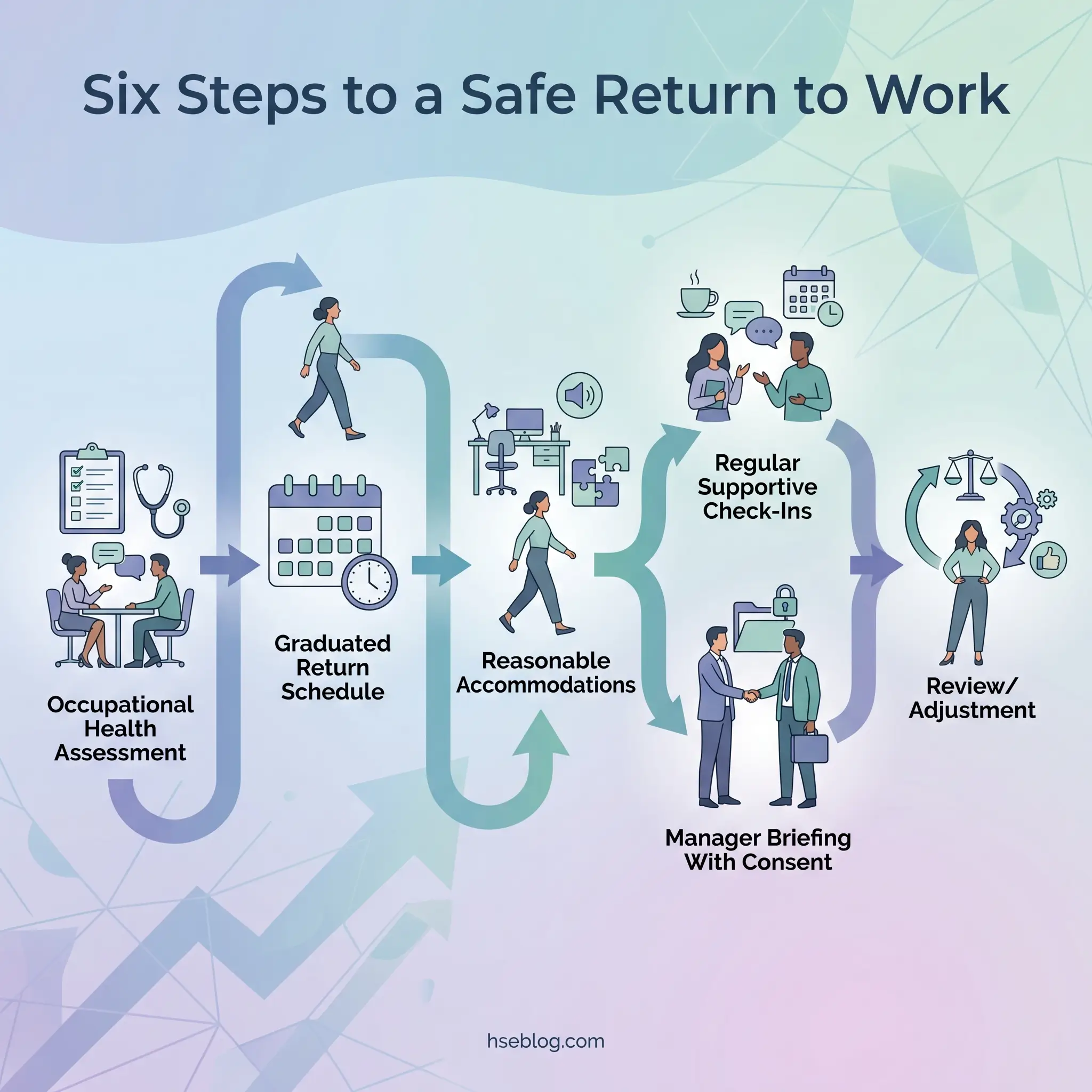
WHO identifies return-to-work programs as multi-component interventions requiring coordination between healthcare providers, employers, and employees. The key elements form a sequence, not a checklist:
- Pre-return occupational health assessment. Establish functional capabilities and any needed adjustments. This is a functional assessment, not a diagnostic interrogation — the employer does not need (and in most jurisdictions cannot demand) the employee’s diagnosis.
- Graduated return schedule. Phased hours and modified duties over a defined period, agreed in writing between the employee, their manager, and HR or occupational health.
- Reasonable accommodations. Based on functional limitations, not diagnostic labels. Under ADA (US), employers must engage in an interactive process to identify effective accommodations. Under the Equality Act 2010 (UK), the duty to make reasonable adjustments applies to mental health conditions qualifying as disabilities.
- Regular supportive check-ins. Scheduled, not ad hoc. Focused on workload manageability and adjustment effectiveness — not on the employee’s medical status.
- Manager briefing with employee consent. The employee controls what information their manager receives. Confidentiality must be strictly maintained — limit knowledge of absence reasons to the smallest number of people operationally necessary.
- Review and adjustment. The return plan is a living document. If the graduated schedule is too fast or too slow, it should be adjusted without penalty.
The legal requirement across jurisdictions is consistent: employers must not require disclosure of diagnosis, and accommodations must be based on what the employee needs to perform their job, not on a clinical label. EEOC guidance (US) specifies what employers may and may not ask, and erring on the side of asking less is always the safer position.
Frequently Asked Questions
Conclusion
The central lesson from the evidence, the regulation, and the enforcement record is that workplace mental health is a systems problem requiring a systems response. Organizations that treat it as a benefits-line-item — an EAP here, a wellness week there — consistently underperform on both employee outcomes and financial return compared to those that treat psychosocial hazards with the same rigor as physical ones.
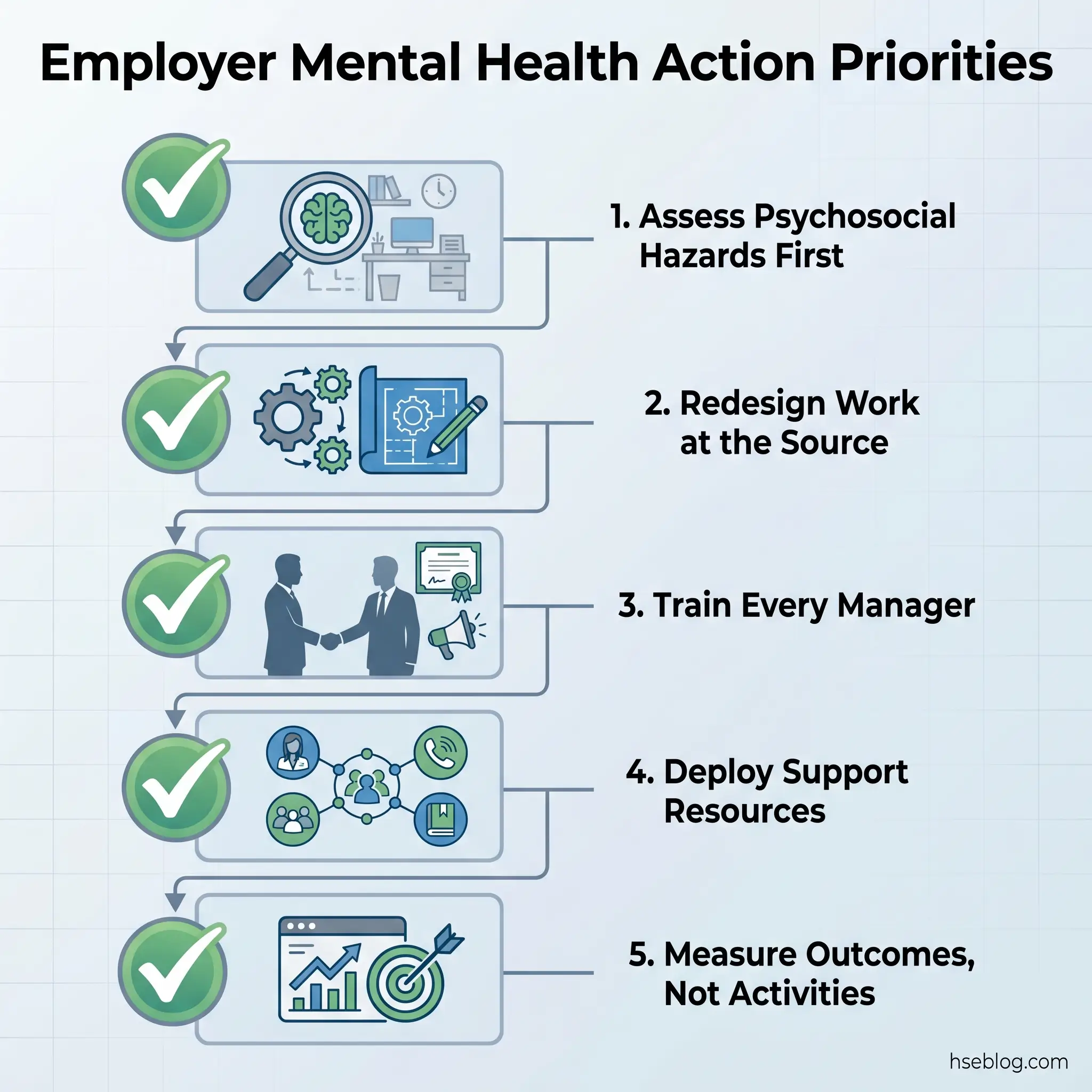
The single highest-impact change most employers can make is sequencing their interventions correctly. Assess organizational hazards first, redesign work and management practices second, then layer on individual support programs. WHO, ISO 45003, and the published evidence all point in the same direction — and regulators in the UK, Australia, the EU, and increasingly the US are enforcing that direction with real consequences.
Every employer reading this can start with one action: conduct a baseline psychosocial risk assessment using a validated tool, and let the findings — not assumptions about what employees need — drive the strategy that follows.