

TL;DR
- Build the team before the outbreak — Name EHS, HR, operations, IT, comms, and continuity leads with written decision triggers, not improvised roles mid-crisis.
- Assess exposure task by task — Classify every role from lower to very high risk; a warehouse picker and a customer-facing cashier need different controls.
- Work the hierarchy top-down — Remote work and ventilation outperform masks and surface cleaning, yet most organizations inverted this and paid for it.
- Know your real legal duty — The US has no permanent OSHA pandemic standard, but the General Duty Clause plus existing respiratory and PPE rules still bind you.
- Test it, don’t shelve it — Review at least annually, drill the plan, and feed frontline observations back into the next version.
A workplace pandemic preparedness plan should include a cross-functional response team, a task-by-task exposure risk assessment, layered controls following the hierarchy of controls, business continuity provisions for critical functions, a communication protocol, and a defined review cadence. In the US, no permanent OSHA standard mandates one, but the General Duty Clause and existing respiratory and PPE standards create the effective duty.
Two employers met the same March 2020 disruption with opposite results. One had a tested infectious disease preparedness and response plan, named roles, and a second qualified supplier for critical PPE; it adjusted within days. The other had a binder nobody had opened since an audit and a single overseas mask vendor; it cascaded into staffing gaps, stockouts, and citations.
The gap between those two outcomes is the real COVID-19 lesson learned in the workplace, and it is not nostalgia. Workplace pandemic preparedness has moved from a one-off 2020 scramble into a standing EHS discipline, sitting inside enterprise risk management alongside cyber and supply-chain risk. This guide maps what a plan must contain, how to apply the hierarchy of controls to airborne disease, and what actually obligates employers now that the emergency standards are gone.
Why COVID-19 Made Workplace Pandemic Preparedness a Standing Requirement, Not a One-Off
A consistent pattern separated the organizations that absorbed COVID-19 from the ones it overran: the resilient ones had already written, tested, and re-tested a plan. Preparedness is now a permanent EHS function, not a 2020 emergency you can declare finished.
Scope and disclaimers. This article is general HSE practitioner reference for organizational preparedness. It is not legal advice; verify requirements against your own jurisdiction. It is also not medical or occupational-health advice — workers with symptoms or specific exposure concerns should consult an occupational physician or qualified medical professional. Clinical infection control inside healthcare settings is a higher-tier topic flagged separately.
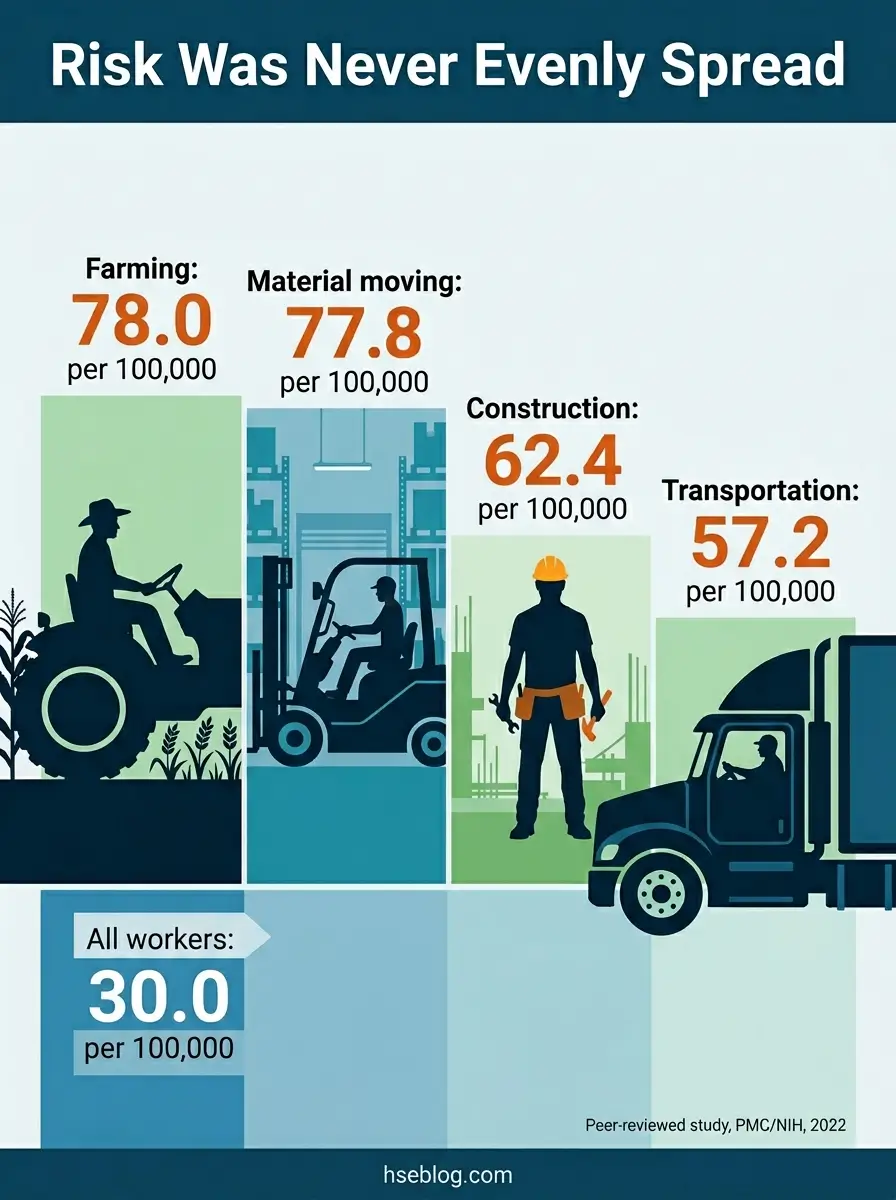
The peer-reviewed record makes the stakes concrete. Among working Californians in 2020, age-adjusted COVID-19 mortality ran at 30.0 per 100,000 workers overall, but reached 78.0 in farming, 77.8 in material-moving, 62.4 in construction, 60.2 in production, and 57.2 in transportation (peer-reviewed study, PMC/NIH, 2022). CDC analysis across 46 US states found mortality varied significantly by industry and occupation in the same period (CDC, 2020–2021 reporting).
What changed since then is structural, not cosmetic:
- Preparedness moved into enterprise risk management — Pandemic risk now sits beside cyber and supply-chain disruption, not in a shelved binder.
- The plan became a living document — Resilient organizations ran quarterly reviews and live drills; the surfaced gaps were usually ones frontline workers saw and management missed.
- The duty outlasted the emergency — Even after the emergency rules expired, the underlying obligation to control a recognized hazard did not.
The failure mode I see most often in the published account is the “set-and-forget binder”: a plan written once, certified for an audit, then never re-tested until it is needed and found stale. The judgment call for any EHS lead is simple to state and hard to fund — a plan that is never drilled is a document, not a control.
What Should a Workplace Pandemic Preparedness Plan Include?
A workplace pandemic preparedness plan needs six working parts: governance, a task-level exposure risk assessment, layered controls, business continuity provisions, communication protocols, and a maintenance cadence. Skip any one and the plan looks complete on paper while failing in use.
Competent-person caveat. This is general guidance. Life-critical decisions — respirator selection, fit-testing, reclassifying a high-exposure task — must be planned and supervised by a competent person with relevant training, jurisdiction-specific authorization, and a site-specific risk assessment. The information here does not replace that.
The structure below follows the components OSHA laid out in its 2020 guidance, OSHA’s guidance on preparing workplaces for COVID-19 (OSHA 3990-03) — useful as a template, but remember it is guidance, not an enforceable standard.
- Governance and named roles. A cross-functional team — EHS, HR, operations, IT, communications, and business continuity — with decision triggers agreed before a crisis, not negotiated during one.
- Task-by-task exposure risk assessment. Classify each role’s exposure rather than the building as a whole.
- Layered, scalable controls. Measures that step up and down with threat severity, not a binary open/closed switch.
- Business continuity provisions. Critical functions, maximum tolerable downtime, and single points of failure identified in advance.
- Communication protocol. Cadence, channels, and named spokespeople for both routine updates and uncertainty.
- Maintenance. Review schedule, version control with an audit trail, and a frontline feedback loop.
The recurring error here is copying a generic pandemic plan for businesses and skipping step two. The result reads as a finished plan but cannot distinguish a warehouse picker from a customer-facing cashier in terms of required controls — which is the whole point of a pandemic risk assessment in the workplace.
OSHA 3990 classifies occupational exposure into four tiers. Applied to a non-healthcare employer, it looks like this:
| Exposure level | Typical roles | Control emphasis |
|---|---|---|
| Lower | Remote staff, minimal public or coworker contact | Hygiene, basic administrative controls |
| Medium | Frequent close contact with the public or coworkers | Barriers, improved ventilation, screening |
| High | Some transport, mortuary, healthcare-support roles | Respirators plus engineering controls |
| Very high | Aerosol-generating medical or laboratory procedures | Full respiratory protection and engineering controls |
Conducting the Risk Assessment and Business Impact Analysis
The exposure assessment answers “who is at risk and from what.” The business impact analysis (BIA), drawn from ISO 22301, answers “what breaks if they cannot work.” Run them together.
A workable BIA identifies three things in plain terms:
- Critical functions — the processes the organization cannot pause without serious harm to operations or obligations.
- Maximum tolerable downtime — how long each function can stop before the damage compounds.
- Single points of failure — a sole-source supplier, or one trained person holding a critical role with no backup.
That last item is where most plans are quietly fragile. A function staffed by a single qualified person is a single point of failure long before a pandemic exposes it.

The Hierarchy of Controls Applied to Infectious Disease
Walk onto most sites in 2020 and the spending told the story: budget poured into the bottom of the hierarchy first. The hierarchy of controls ranks measures by reliability, and for an airborne disease that ranking puts PPE last and ventilation far higher — which is precisely the order many employers reversed.
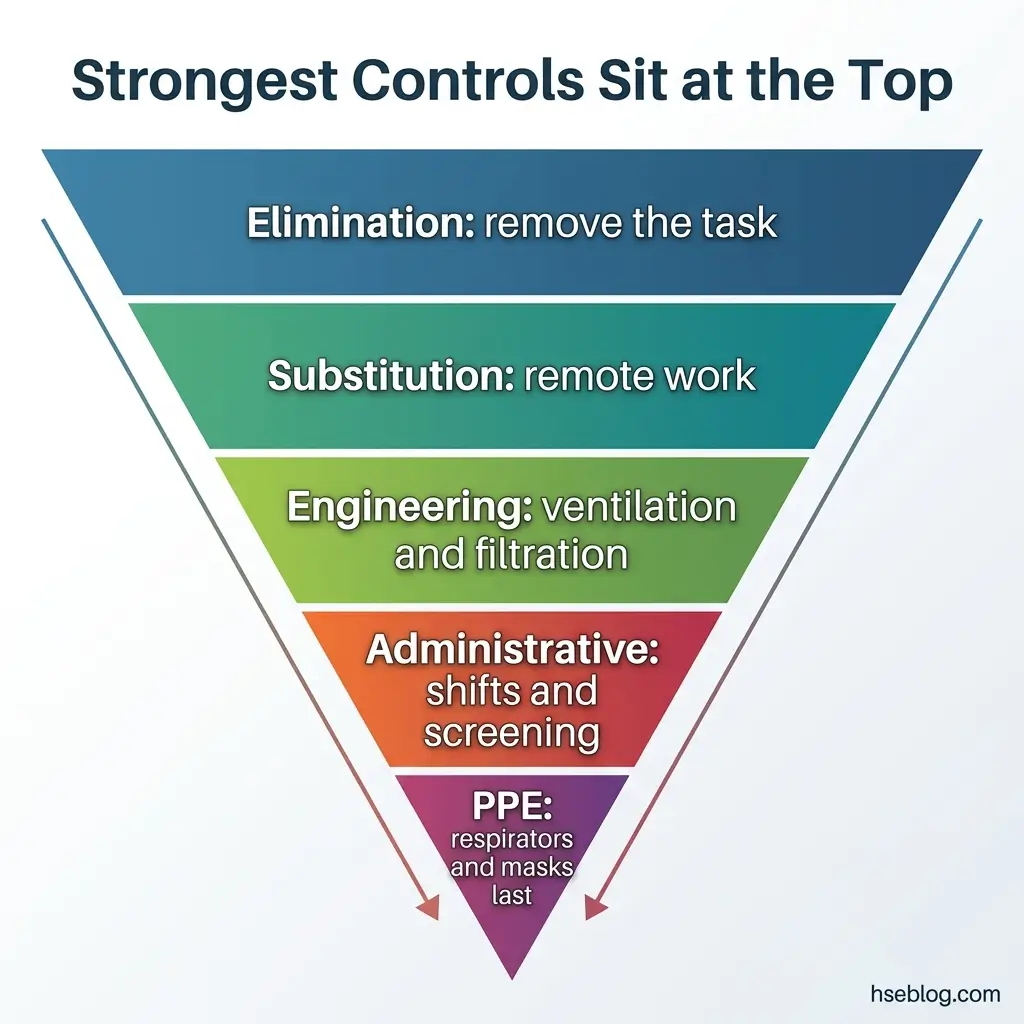
The five-level NIOSH framework translates cleanly to infectious disease. The NIOSH hierarchy of controls reads, from most to least effective:
- Elimination — Remove the exposure entirely. Send a task home; cancel a non-essential in-person gathering.
- Substitution — Replace a high-exposure process with a lower one, such as remote service in place of in-person.
- Engineering controls — Increase outdoor-air exchange, add MERV-rated or HEPA filtration to HVAC systems, install physical barriers, and use negative pressure where aerosol-generating procedures occur.
- Administrative controls — Stagger shifts, set vaccination and sick-leave policy, run screening, and discipline communication.
- PPE — Respirators, surgical masks, and face coverings, used to fill the residual gap the higher controls leave.
PPE sits at the bottom for a reason. It protects one person, only while worn correctly, and depends on continuous compliance — whereas a well-filtered, well-ventilated room protects everyone in it without anyone remembering to do anything.
Respirator selection is also where a control quietly becomes a legal obligation. The moment respirators are necessary rather than optional, the field procedure most aligned with 29 CFR 1910.134 (US, OSHA) kicks in: a written respiratory protection program, fit testing, and a medical evaluation before use. A half-mask handed out without that program is not compliance — it is exposure with paperwork attached.
The inversion error is the pattern worth naming. Many organizations spent heavily on surface cleaning and face coverings — the bottom of the hierarchy — while leaving ventilation, an engineering control sitting much higher, untouched. The reason is human, not technical: cleaning is visible and reassuring, while a recalibrated air-handling unit is invisible. The hierarchy of controls for infectious disease only works when you fund the parts no one can see.
The Regulatory Reality After the ETS: What Actually Obligates Employers Now
As of 2025, no permanent OSHA standard requires US general-industry employers to hold a pandemic preparedness plan. The duty is real anyway — it runs through the General Duty Clause, Section 5(a)(1) (US, OSH Act), which requires a workplace free of recognized hazards likely to cause death or serious harm, backed by existing PPE and respiratory standards.
Jurisdictions diverge sharply on whether a prospective written plan is mandatory. Where an employer operates across several, the defensible move is to plan to the strictest applicable jurisdiction:
| Jurisdiction | Prospective written plan required? | Primary legal instrument |
|---|---|---|
| US federal (general industry) | No standing mandate | General Duty Clause 5(a)(1) + 29 CFR 1910.134, .132, .1030 |
| California | Yes, for covered employers | Cal/OSHA Aerosol Transmissible Diseases, Title 8 §5199 |
| New York | Yes, for designated outbreaks | HERO Act, Labor Law §218-b |
| United Kingdom | Ongoing biological-agent risk assessment | COSHH 2002 under HSWA 1974 |
| European Union | Ongoing biological-agent risk assessment | Biological Agents Directive 2000/54/EC |
The US baseline confuses people in two opposite directions. Some employers assume a specific “OSHA COVID rule” still binds them and build to a standard that no longer exists; others assume that because the emergency rule is gone, no duty remains. Both misread the General Duty Clause, which never went anywhere.
The history clarifies it. OSHA issued a COVID-19 healthcare Emergency Temporary Standard (29 CFR 1910.502) in June 2021, withdrew its non-recordkeeping provisions in December 2021, and formally terminated the rulemaking on January 15, 2025 — and in mid-2025 proposed removing the remaining COVID-19 recordkeeping provisions as well (OSHA / Federal Register, 2025). You can confirm the closure directly through OSHA’s termination of the COVID-19 healthcare rulemaking. The net effect: the US has no permanent infectious-disease standard for general industry.
A point worth stating flatly, because it is a frequent compliance error: the bloodborne pathogens standard, 29 CFR 1910.1030 (US), does not cover airborne or droplet transmission. It governs blood and other potentially infectious materials. Treating it as your COVID-19 hook leaves the actual transmission route uncontrolled.
Internationally, the duty is broader and older. The UK carries ongoing biological-agent obligations through COSHH 2002 within the HSWA 1974 framework, regardless of whether a pandemic is declared. The EU added SARS-CoV-2 to the classified-agent list under Directive 2000/54/EC. And the wider trend points one way: the World Health Assembly adopted the WHO Pandemic Agreement in 2025, with annex negotiations continuing into 2026 (World Health Organization, 2025) — a signal that prospective preparedness obligations are tightening, not loosening.
Legal disclaimer and regulatory currency note. This regulatory content reflects general HSE professional understanding of the cited jurisdictions’ requirements as of 2025. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.

Lessons COVID-19 Taught About Continuity, Equity, and Communication
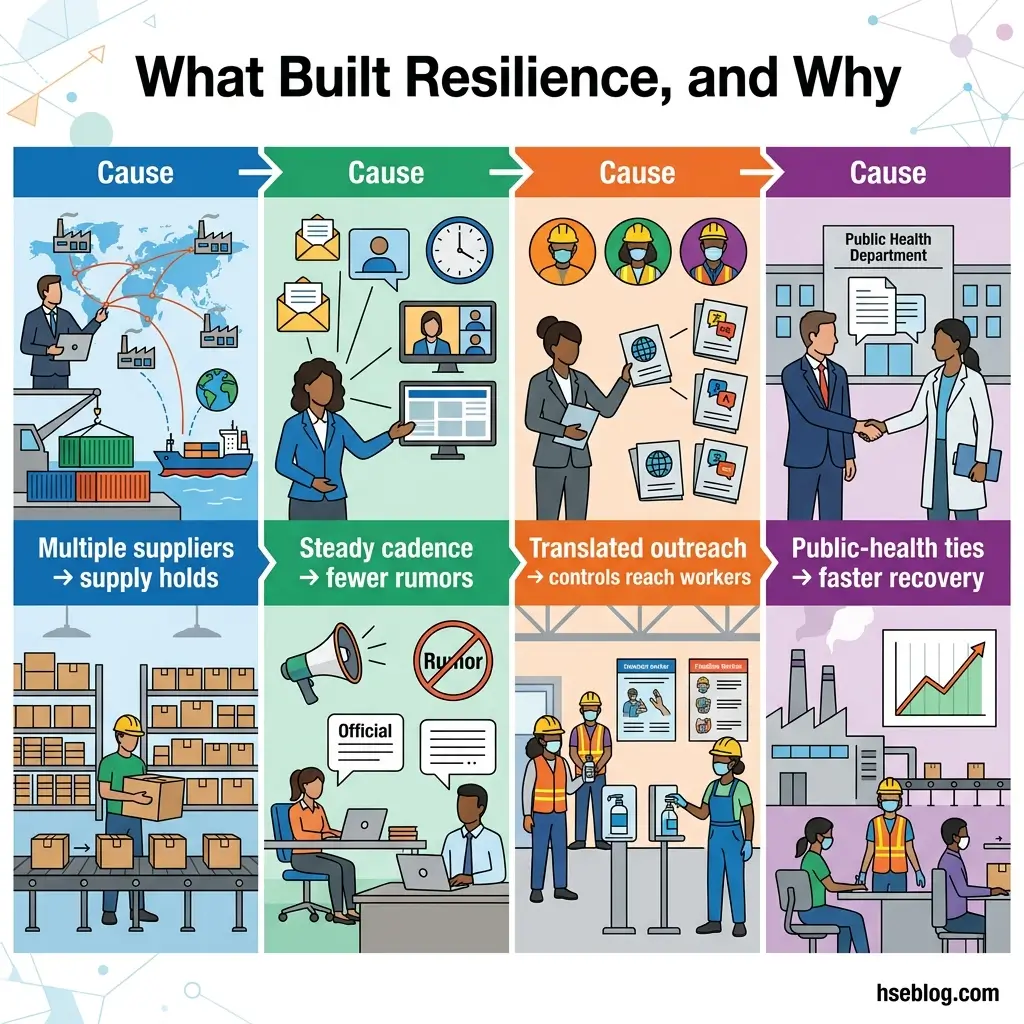
Supply chains broke first, and the break was rarely random — it traced back to single-source dependence. The applied lesson across continuity, communication, and equity is the same: resilience comes from redundancy and relationships built before the crisis, never during it.
Supply-chain redundancy. The PPE and semiconductor shortages of 2020 punished concentration.
- Qualify a second supplier for every critical item before you need it.
- Hold a buffer inventory of essential PPE sized to your real burn rate, not a token shelf.
- Map sub-tier dependence — a “diversified” supplier base is fragile if every vendor draws from one factory.
Communication discipline. A communication vacuum does not stay empty; misinformation fills it.
- Keep a regular cadence even when there is no new information to share.
- State uncertainty openly rather than projecting false certainty.
- Route messages through channels frontline and shift workers actually use, not just email.
Equity as a control, not a courtesy. Controls only work if they reach the people most exposed.
- Translate materials for the languages your workforce actually speaks.
- Account for shift-worker schedules so updates and protections reach off-hours staff.
- Recognize that frontline roles carried higher exposure — the mortality data earlier in this article is that point in numbers.
One pattern stands out in the published account of recovery. Organizations that already had working relationships with local public-health authorities restored continuity faster, because those relationships function as an early-warning and coordination channel. They cannot be assembled mid-crisis. This is the practical edge of the One Health view — workforce health, public health, and operational continuity are one system, not three.
Embedding Pandemic Readiness Into Standing EHS and Continuity Systems
Preparedness survives only when it has a budget line and a place in an existing management system. A plan that lives as a standalone document dies in the first tight budget cycle, because it was never owned by anything that gets reviewed.
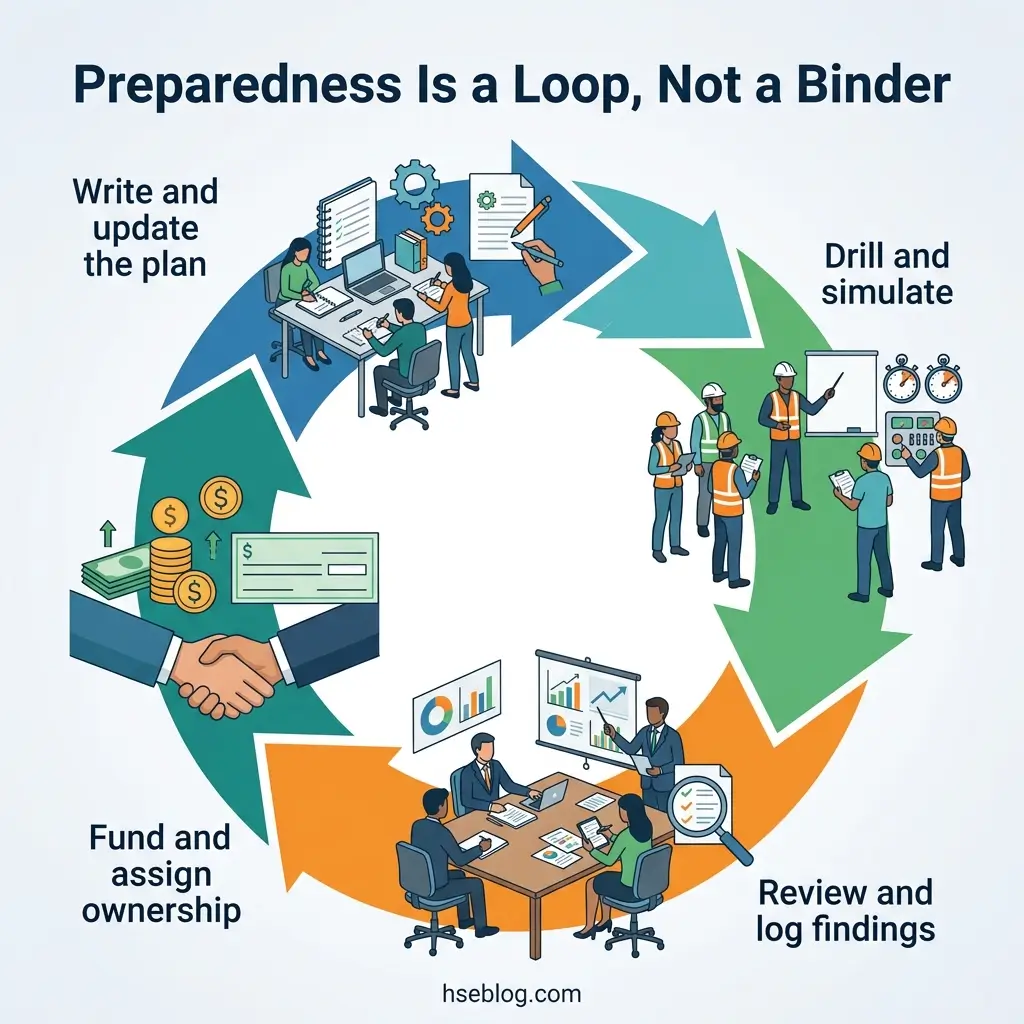
The integration sequence is short and concrete:
- Fold it into your BCMS. Attach the pandemic plan to your ISO 22301 business continuity framework so it inherits the same review, audit, and impact-analysis machinery. The ISO 22301 business continuity standard already accounts for epidemics and pandemics as disruption scenarios.
- Tie controls into the OH&S management system. Exposure assessment and the hierarchy of controls belong with your existing occupational health and safety processes, not in a separate silo.
- Drill it on a schedule. Run tabletop exercises and at least one live simulation a year, and document the outcomes — the gaps you find are the deliverable.
- Line-item the budget. Treat preparedness as a recurring expense, the way you treat fire-system maintenance, so it is not the first thing cut.
A quick integration check:
- Owner named — a specific role accountable for the plan year-round.
- Review cadence set — at least annual, with version control and an audit trail.
- Drill scheduled — dated, with findings logged back into the plan.
- Budget assigned — a standing line, not a one-time grant.
The under-resourcing pattern is the one to guard against. Preparedness that depends on a single enthusiastic manager and no budget code lasts until that person moves on. For the people building this capability, recognized training pathways — NEBOSH and IOSH qualifications, OSHA outreach training, or the equivalent regional certification — give the function the standing it needs to hold a budget line.
Frequently Asked Questions
Test the Plan Before the Next Pathogen Does
Here is the uncomfortable question worth taking back to your own site: if a new pathogen reached emergency status next month, would your plan tell a warehouse picker and a customer-facing cashier two different things — and has anyone actually drilled it in the last year? If the honest answer is no, you have a document, not workplace pandemic preparedness.
The organizations that came through COVID-19 intact were not lucky. They had named the team, assessed exposure task by task, funded the invisible engineering controls, understood that the General Duty Clause bound them whether or not an emergency standard existed, and built supplier and public-health relationships before they were needed. None of that survives a tight budget cycle unless it sits inside a standing system with an owner and a line item.
Pull your plan this week and run it against the six components and the jurisdiction table above. The gap between a binder and a control is measured in drills — and the next time the gap matters, you will not have a month to close it.