

TL;DR
- If you exclude a worker on safety grounds without an individualised assessment, you fail both the ADA’s direct-threat test and the Equality Act’s proportionality test simultaneously.
- If you receive an accommodation request and go silent, courts and tribunals treat that delay as a breakdown of the interactive process — liability can attach without a refusal.
- If your policy says “100% healed” or “no medical restrictions” before return to work, the EEOC’s FY2024 enforcement record shows that policy alone is now litigated.
- If you wait for a formal medical disclosure to act, you are likely already in breach — both ADA and Equality Act trigger duties on constructive knowledge.
Employers owe workers with disabilities two parallel duties: protect them from harm under occupational-safety law (the OSH Act in the US; HSWA 1974 in the UK), and protect them from discriminatory exclusion under equality law (the ADA in the US; the Equality Act 2010 in the UK). Discharging both means individualised risk assessment, reasonable accommodation or adjustment, a documented interactive process, and tailored emergency-evacuation planning — never blanket exclusions.
The EEOC received about 29,000 disability-discrimination charges in fiscal year 2024 — a 25-year high — and ADA cases made up roughly 44 percent of merits suits filed by the agency that year (US Equal Employment Opportunity Commission, 2024). Many of those filings were not exotic. They were the same patterns the agency has been litigating for a decade: inflexible qualification standards, blanket return-to-work rules, no-fault attendance policies that point-charge disability-related absences, and refusals to engage with accommodation requests at all.
Workplace safety duty for workers with disabilities is the single most-misapplied corner of HSE compliance, because the safety justification employers reach for is the precise position that triggers equality enforcement when applied without individual evidence. Employer duties for workers with disabilities (safety) are dual obligations — the OSH duty to prevent harm and the equality duty to prevent unlawful exclusion — and they cannot be discharged in isolation. This guide walks through both, in parallel for US and UK jurisdictions, and shows the procedural mechanics that satisfy them at the same time.
Why This Article Frames Employer Duties Across Jurisdictions
The core problem most multinational employers run into is treating disability-safety duty as either a health-and-safety question or a discrimination question. It is both, simultaneously, and the legal regimes police different parts of the same decision. An employer that builds a defensible safety case for excluding a worker can still lose an EEOC charge or an Employment Tribunal claim if the safety case was generic, untested against accommodation, or based on stereotype rather than evidence.
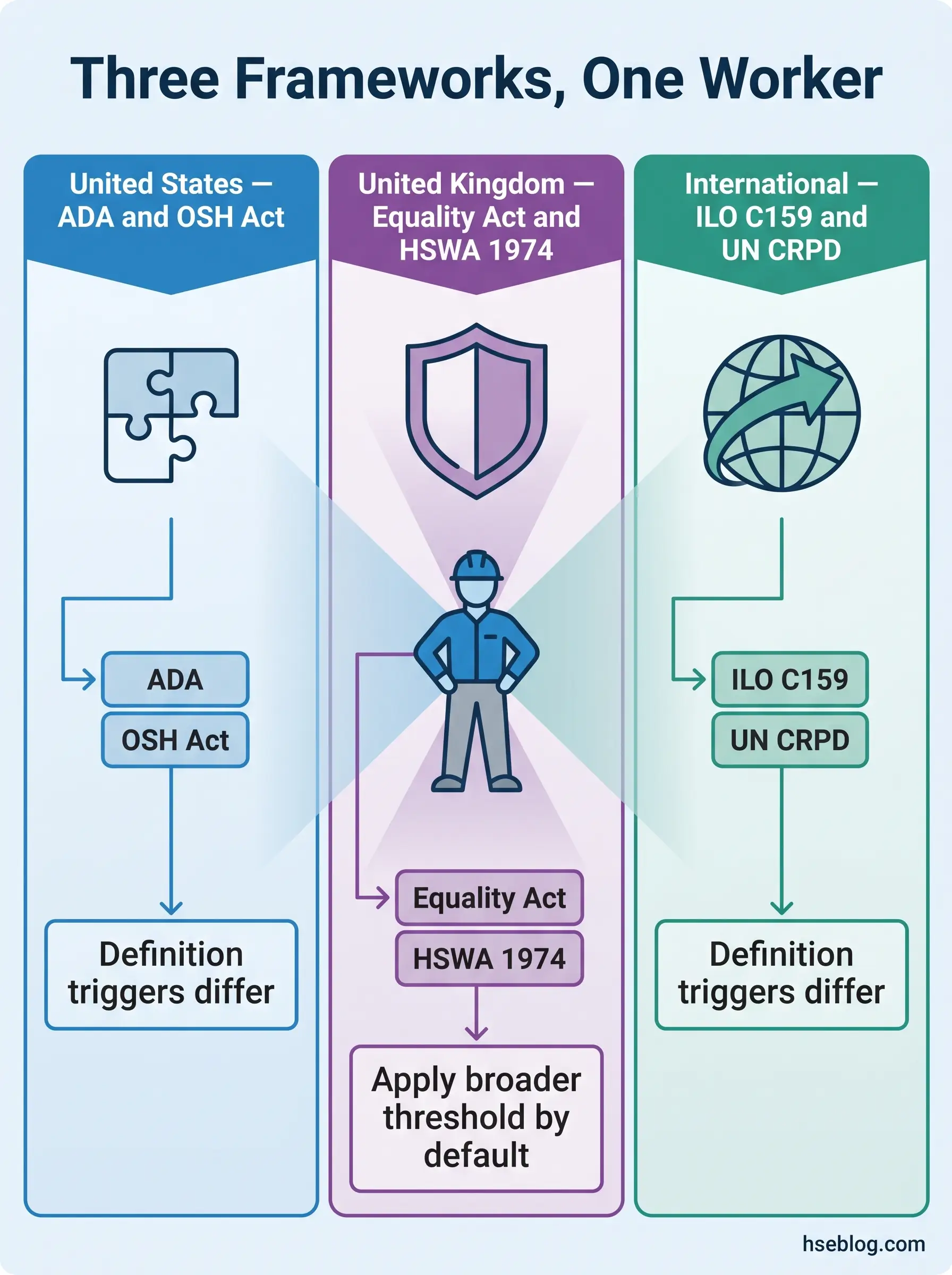
In the United States the controlling instruments are Title I of the ADA (42 U.S.C. § 12101 et seq.) and the OSH Act of 1970 — the first prohibiting discrimination by employers with 15 or more employees, the second imposing the General Duty Clause on every covered employer. In the United Kingdom the parallel pair is the Equality Act 2010 (which covers all employers regardless of size) and HSWA 1974, sitting alongside the Management of Health and Safety at Work Regulations 1999. Above these, the international floor is set by ILO Convention 159 and the 2002 ILO Code of Practice, EU Framework Directive 89/391/EEC, and Article 27 of the UN Convention on the Rights of Persons with Disabilities.
The definitions of “disability” themselves diverge. A short comparison:
| Jurisdiction | Definition trigger | Primary duty source |
|---|---|---|
| United States (ADA, post-ADAAA) | Physical or mental impairment that substantially limits one or more major life activities; “substantially limits” construed broadly. | Title I ADA + 29 C.F.R. Part 1630 |
| United Kingdom (Equality Act 2010) | Physical or mental impairment with a substantial and long-term (12+ months or recurring) adverse effect on day-to-day activities. | Equality Act 2010 ss 13–21, Schedule 8 |
| International (ILO C159 + UN CRPD) | Long-term impairments which, in interaction with barriers, may hinder full and effective participation. | ILO Convention 159; CRPD Article 27 |
The practitioner consequence is straightforward. The same worker may be plainly within scope in one jurisdiction and on the borderline in another. Multinational policy should default to the broader interpretation — typically the post-ADAAA US construction or the deemed-disabilities approach in UK Equality Act Schedule 1 — because compliance with the broader threshold automatically satisfies the narrower one.
What Counts as a “Disability” — and Why the Definition Drives Every Duty
A pattern that runs through EEOC determinations and UK Employment Tribunal decisions is the employer who waits for a formal disclosure or a diagnostic label before acting. The legal duty does not work that way in either jurisdiction. The trigger is knowledge of the impairment — and in many cases, constructive knowledge. A worker who says “my back’s been bad since the surgery” or whose GP letter mentions a recurring condition has put the employer on notice. EEOC enforcement guidance and the UK EHRC Employment Statutory Code of Practice both treat that as enough.
Under the ADA Amendments Act 2008, the definition of disability is to be construed broadly. Episodic conditions and conditions in remission can qualify. Mental-health conditions — long-term anxiety, depression, PTSD, bipolar disorder, autism spectrum conditions — sit on equal legal footing with physical impairments. The Equality Act 2010 reaches the same outcome through different drafting: the “substantial” threshold means more than minor or trivial, and progressive conditions like cancer, multiple sclerosis, and HIV are deemed disabilities from the point of diagnosis under Schedule 1.
Three thresholds practitioners get wrong most often:
- Episodic conditions are covered. A worker with epilepsy, lupus, or major depressive disorder qualifies even when symptom-free at the moment of assessment.
- Hidden disabilities are protected on the same basis as visible ones. There is no “you can see it” requirement in either statute.
- Disclosure can be informal. A request for adjustment, a wheelchair on site, or a third-party communication (occupational health, GP, family member) attaches the duty.
The implication for risk management is direct: the day a worker tells a supervisor about a limitation is the day the employer’s duty starts running, regardless of whether HR has a form on file.
The Core Employer Duties: Side-by-Side, US and UK
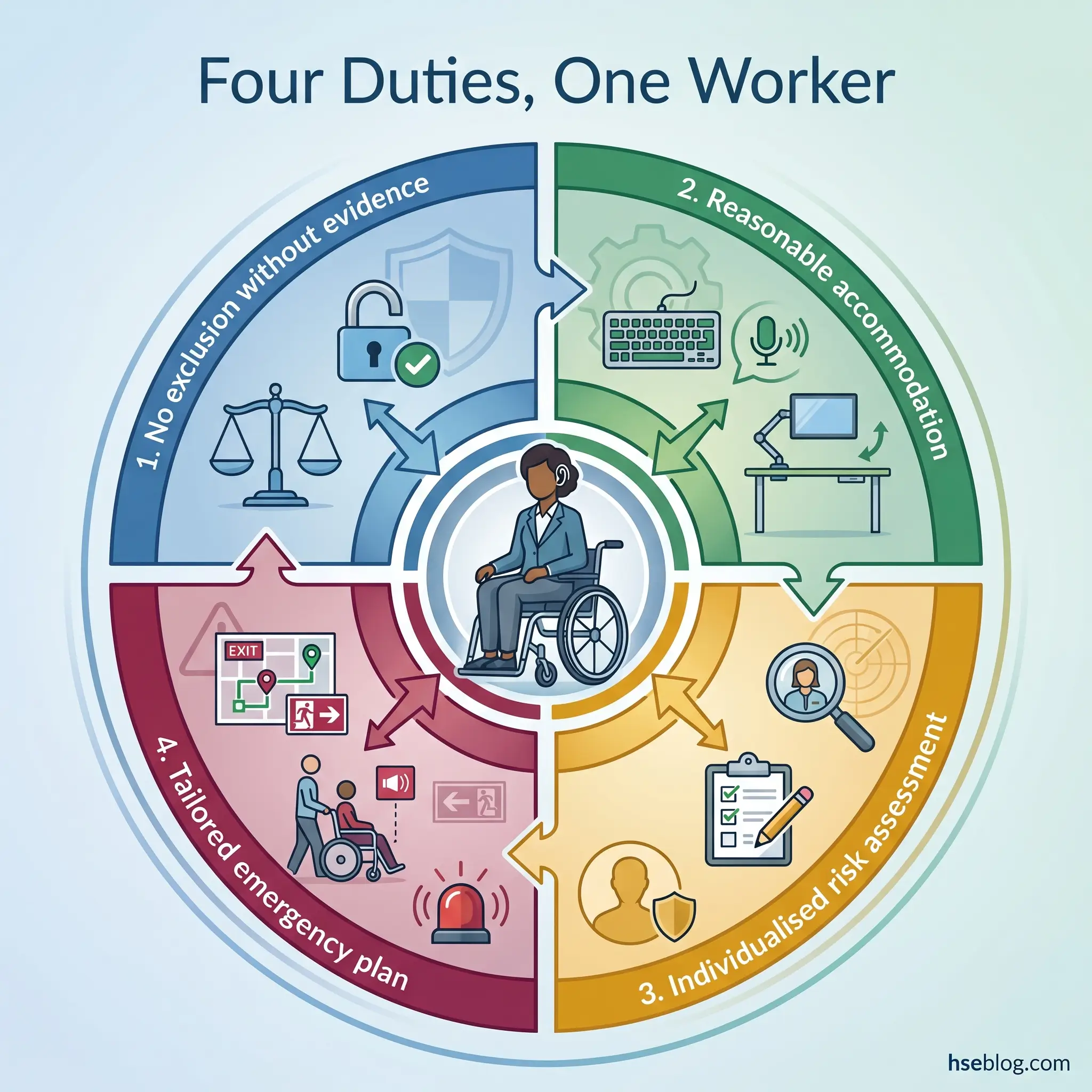
Four operational duties carry the weight of disability-safety compliance. Each has a US source and a UK source that produce equivalent practitioner obligations through different statutory routes. The parallel map below is followed by a subsection on each duty.
| Duty | US source | US mechanism | UK source | UK mechanism |
|---|---|---|---|---|
| Avoid discriminatory exclusion on safety grounds | ADA Title I; 29 C.F.R. § 1630.2(r) | Direct-threat defence — significant risk of substantial harm based on objective evidence | Equality Act 2010 ss 15 and 19 | Treatment must be a proportionate means of a legitimate aim |
| Provide reasonable accommodation / adjustment | ADA Title I; 29 C.F.R. Part 1630 | Reasonable accommodation absent undue hardship (15+ employees) | Equality Act 2010 ss 20–21, Sch 8 | Reasonable adjustments — all employers, no size threshold |
| Conduct individualised risk assessment | OSH Act § 5(a)(1) | General Duty Clause — recognised hazards, including those affecting at-risk workers | MHSWR 1999 reg 3 + Directive 89/391/EEC | Suitable and sufficient assessment, with vulnerable groups considered |
| Plan emergencies and evacuation | 29 C.F.R. 1910.38(c)(2) | Emergency Action Plan must include procedures for employees needing assistance | RR(FS)O 2005 + HSWA 1974 | PEEPs and GEEPs — the responsible person must ensure all can evacuate safely |
1. Duty to Avoid Discrimination on Safety Grounds
The line that catches the most employers is this: “it’s a safety risk” is not, on its own, a lawful basis to refuse to hire, transfer, or dismiss a disabled worker. Under the ADA, an exclusion must satisfy the direct-threat standard at 29 C.F.R. § 1630.2(r) — a significant risk of substantial harm to the worker or others that cannot be eliminated or reduced to an acceptable level by reasonable accommodation, established by current medical evidence or objective evidence rather than stereotype or generalised fear. Under the Equality Act 2010, exclusion connected to disability must be a proportionate means of achieving a legitimate aim — and the employer must first have considered reasonable adjustments.
Joint research commissioned by HSE and the Disability Rights Commission found that around one in five large UK employers had refused a job to a disabled applicant on health-and-safety grounds, and roughly one in three had dismissed a disabled employee on those grounds (HSE/DRC commissioned research, 2003). That research is now dated, but the pattern of misuse it documented has not changed in the enforcement record — the safety justification remains the single most-litigated employer position. The lesson holds: a generic risk concern, an insurer’s preference, or a customer-facing assumption will not survive scrutiny. Only a specific, evidence-based, individualised assessment will.
2. Duty to Provide Reasonable Accommodations / Adjustments
The ADA requires reasonable accommodation for a qualified individual with a disability, absent undue hardship — and the duty applies in three settings: the application process, performing essential job functions, and equal access to benefits and privileges of employment. The Equality Act 2010 imposes an equivalent duty under sections 20–21 and Schedule 8, but with no employee-number threshold; a four-person bakery owes the same duty as a multinational.
Common categories of accommodation include:
- Physical changes — accessible workstations, height-adjustable benches, ramped access, modified controls.
- Equipment and assistive technology — screen readers, hearing-loop systems, ergonomic input devices.
- Working arrangements — flexible hours, modified breaks, working from home where the essential functions allow.
- Job restructuring — reassigning marginal (non-essential) duties.
- Auxiliary aids and services — sign-language interpretation, accessible documentation, captioning.
About 49.4 percent of accommodations cost the employer nothing, and another 43.3 percent involve only a one-time cost (Job Accommodation Network / US DOL ODEP, 2024). The cost barrier most employers cite is, on the data, largely imagined.
The recurring operational failure is treating accommodations as IT or facilities tickets — assigning them, never closing the loop with the employee, and never reviewing whether the adjustment actually worked. Effective practice runs each accommodation as a small project with a named owner, an agreed trial period, and a scheduled review. That single discipline closes most of the gap between paper compliance and operational compliance.
3. Duty to Conduct an Individualised Risk Assessment
A point that the HSE makes plainly in its employer-duties guidance: there is no requirement for a separate disability risk assessment. The existing risk assessment must be reviewed once the employer becomes aware of the worker’s disability or health condition. Under MHSWR 1999 regulation 3 and EU Framework Directive 89/391/EEC, employers must adapt risk-prevention measures to the worker, with explicit consideration of especially sensitive risk groups. Canadian guidance from CCOHS reaches the same operational standard through different drafting.
The triggers for review include notification of a disability or condition, return from extended absence, change of role, and any material change in workplace layout, equipment, or process. The inputs are the worker’s own knowledge of how their condition affects their work, occupational-health advice where appropriate, and the line manager’s task observation. The output is a documented adjustment, an explicit statement of any residual risk, and a review date.
Watch For: Assessing the condition rather than the interaction between worker, task, and environment. Two workers with the same diagnosis may need entirely different adjustments — or none at all. The assessment must follow the work, not the diagnostic label.
The boundary on information-gathering: the employer cannot demand more medical detail than is necessary to identify the limitation and the accommodation. Under the ADA, that means requesting documentation only where the disability or need for accommodation is not obvious, and limiting the request to functional information. Under the UK GDPR and the Equality Act, health data is a special category requiring explicit safeguards and need-to-know handling.
4. Duty to Plan for Emergencies and Evacuation
In the UK, the Regulatory Reform (Fire Safety) Order 2005 obliges the responsible person to ensure that all relevant persons can safely evacuate the premises. The mechanism is the Personal Emergency Evacuation Plan (PEEP), supplemented where appropriate by a General Emergency Evacuation Plan (GEEP) for visitors and people whose needs are not yet known. In the US, 29 C.F.R. 1910.38(c)(2) requires Emergency Action Plans to address procedures for employees who require assistance during an evacuation; OSHA letters of interpretation confirm this includes employees with disabilities.
A defensible PEEP contains the following elements:
- The named individual and the specific limitation it addresses.
- The route from each work location to a safe place — including refuges where used.
- Identified assistants, with cover for absence, holiday, and shift changes.
- Equipment required (evacuation chair, communication device) and where it is stored.
- Communication arrangements for the individual during an alarm — visual, vibration, or other signal as needed.
- Explicit instructions on lift use — most passenger lifts must not be used in fire; only designated evacuation lifts may be relied on.
- Drill schedule and review date — tested in real drills, not on paper.
Three predictable PEEP failures sit behind most evacuation incidents involving disabled workers: PEEPs written without the individual’s input, plans that assume a passenger lift will work in a fire, and named-assistant arrangements with no cover. All three are cheap to fix at design stage and expensive to fix after an incident.
How to Run a Defensible Interactive / Adjustment Process — Step by Step
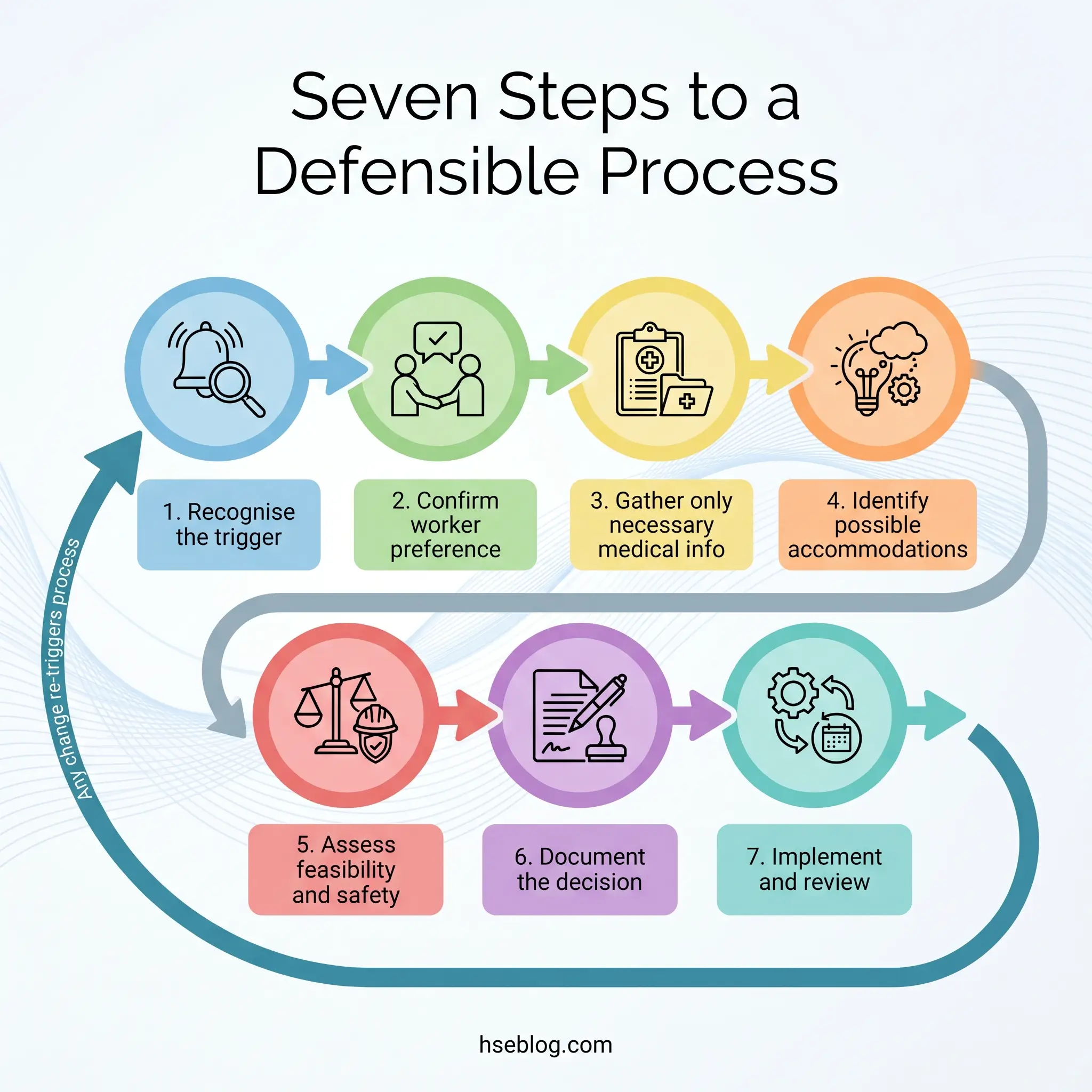
Most failed-to-accommodate determinations turn on procedure rather than substance. The employer often had a reasonable answer available and simply did not run a clean process to reach it. A documented sequence — applicable in either jurisdiction with minor terminology shifts — looks like this:
- Recognise the trigger. A request, a return-to-work flag, an occupational-health observation, a manager’s notice of difficulty, or a third-party communication. The trigger does not need to use the words “reasonable accommodation” or “reasonable adjustment.”
- Confirm the worker’s preference. Ask what the worker thinks will help. The EEOC’s enforcement guidance on reasonable accommodation gives primary consideration to the employee’s preferred accommodation; the employer retains the ability to choose between effective options where more than one exists. UK practice operates on the same balance.
- Gather only the medical information necessary. Functional limitations — what the worker can and cannot do — not diagnoses. Confidentiality is mandatory under the ADA and is special-category processing under UK GDPR.
- Identify possible accommodations. Use the Job Accommodation Network’s Situations and Solutions Finder for US scenarios; HSE employer-duties guidance and the UK Access to Work scheme are the equivalent UK starting points.
- Assess feasibility and safety. Consider effectiveness, cost, operational impact, and any genuine safety implications. Cost should be weighed against the undue-hardship threshold (US) or the reasonableness factors (UK), and grant schemes such as Access to Work in the UK and tax incentives in the US should be factored in before a “too expensive” conclusion.
- Document the decision. Record the request, the options considered, the option selected, and the reasoning — including any rejected options and why. This is the file the EEOC investigator or tribunal will read.
- Implement and review. Set a defined review date and re-open the process on any material change in role, condition, equipment, or workplace.
Audit Point: The single biggest source of failed-to-accommodate findings is silence. The employer received the request, considered it internally, and never came back with an answer. Both EEOC determinations and UK Employment Tribunal jurisprudence treat protracted delay or “going dark” as a breakdown of the interactive process — and that breakdown alone, without a refusal, can establish liability.
When Safety Genuinely Justifies Restriction: The “Direct Threat” Test
The exclusion that does survive challenge is the one built on the four-factor direct-threat analysis at 29 C.F.R. § 1630.2(r) — itself underpinned by the US Supreme Court decision in Chevron U.S.A. v. Echazabal (2002), which permits the direct-threat-to-self defence as well as direct-threat-to-others. The four factors are:
- Duration of the risk — is the limitation temporary, episodic, or persistent?
- Nature and severity of potential harm — what would actually happen?
- Likelihood of occurrence — established on objective evidence, not worst-case speculation.
- Imminence — how soon could harm materialise on this job?
The standard’s UK counterpart sits in the Equality Act 2010’s section 15 (discrimination arising from disability) and section 19 (indirect discrimination). Treatment must be a proportionate means of achieving a legitimate aim — and the employer must have considered reasonable adjustments first. The drafting differs, but the operational outcome aligns: a generic concern is not enough; an evidence-based, individualised, post-adjustment analysis can be.
A worked illustration. A person with a current, uncontrolled seizure disorder applying for a role in which loss of consciousness would create immediate harm — a crane operator, a sole driver of a passenger vehicle in service, a worker on an unguarded platform — can be lawfully restricted from that role on the duration-and-imminence factors, where no adjustment removes the risk. The same person, medically controlled and cleared, in a different role, generally cannot be restricted on the basis of historical diagnosis.
Employers reach for “direct threat” or “health and safety” most often when the real concern is discomfort, customer reaction, or insurance assumption. None of those meet the legal threshold under either framework. The defence requires current, objective, individualised medical evidence — not stereotype, not speculation, not a diagnosis from years ago.
Confidentiality, Documentation, and Records
Records are where good practice and bad practice diverge. The ADA requires medical information obtained from an employee to be kept in separate, confidential medical files — physically or logically separate from the personnel file. The Equality Act, supplemented by UK GDPR, treats health data as a special category requiring an additional lawful basis (typically employment-law obligations under Article 9(2)(b)) and need-to-know handling.
Disclosure is permitted in narrow channels: to supervisors and managers who need to know about restrictions or accommodations, to first-aid and emergency responders where the condition could affect emergency response, to compliance investigators on lawful request, and to workers’ compensation administrators in the US where claims are active. Disclosure to colleagues, to clients, or to general HR staff outside the accommodation chain is not permitted.
A documentation pattern that survives scrutiny on both sides looks like this: a one-page accommodation record that names the limitation in functional terms — “cannot lift more than 10 kg from floor to waist,” “requires a 15-minute break every two hours,” “needs a quiet workspace away from open-plan distractions” — rather than diagnostic terms. That phrasing satisfies the safety-management need (the supervisor can implement it), contains nothing the supervisor does not need (the diagnosis stays with occupational health), and respects the employee’s privacy.
What can and cannot be shared, in summary:
- Can be shared with line management: functional limitations, work restrictions, accommodation in place, review date, emergency-response considerations relevant to that role.
- Cannot be shared with line management: diagnosis, prognosis, treatment, full medical history, or content of medical reports beyond what is needed to implement restrictions.
Returning to Work After Injury or Acquired Disability
The scenario where most employers slip is the existing employee who acquires a disability — through workplace injury, illness, surgery, or a mental-health condition. After the ADA Amendments Act in the US and the Equality Act in the UK, many common workplace injuries clear the disability threshold: significant back injuries, repetitive strain, post-surgical limitations, and stress-linked anxiety or depressive disorders.
The interaction with workers’ compensation (US) or industrial-injury and statutory sick-pay regimes (UK) can mask the underlying disability duty. Workers’ comp settles the medical and wage-replacement question; it does not displace the ADA. An SSP or industrial-injury claim in the UK does not extinguish Equality Act duties. The duty to consider reasonable accommodation or adjustment — including modified duties, phased return, and reassignment to a vacant position as a last resort — runs in parallel.
A specific failure mode shows up at the handover between occupational health and line management. OH writes a clear restriction; the line manager either over-applies it (taking the worker off too many tasks, accelerating deconditioning and prolonging absence) or under-applies it (treating the restriction as advisory and pushing the worker into tasks the OH report excluded). A short joint meeting — OH, manager, worker — at the point of hand-back, not before, closes most of these gaps and produces a return-to-work plan all three parties have signed up to.
Common Pitfalls That Lead to Enforcement Action
EEOC FY2024 enforcement data shows ADA cases at roughly 44 percent of merits suits filed (US Equal Employment Opportunity Commission, 2024) — and the recurring fact patterns are not novel. They sit in policy manuals more often than in any individual manager’s intent. The patterns most likely to produce enforcement action:
- “100% healed” or “no medical restrictions” return-to-work rules. A blanket policy that an employee must be fully recovered before return — explicitly named in the EEOC’s Strategic Enforcement Plan 2024–2028 as a target for litigation.
- No-fault attendance policies that point-charge disability-related absences. A policy that triggers discipline at a fixed number of absences without any disability exception fails the reasonable-accommodation test on its face.
- Blanket bans on entire conditions — “no one with epilepsy can do X,” “no one with a back injury can return to manual work” — without individualised assessment. Both ADA and Equality Act prohibit this.
- Going silent on a request. Receiving an accommodation request and not responding, or responding only after a three-month internal discussion, is treated as a breakdown of the interactive process.
- Denying an accommodation before exploring alternatives. A “no” without a documented analysis of effective alternatives — including ones the employee did not propose — usually loses on review.
- Using cost as a sole reason without testing the threshold. Undue hardship in the US is a high bar; the UK reasonableness test is similar in effect; and grant schemes (Access to Work) and tax credits should be factored in before the cost argument is made.
- Treating the safety justification as a trump card without evidence. “It’s a safety risk” without the four-factor direct-threat analysis or proportionality assessment will not survive a charge.
The Fix That Works: A policy review that surfaces and rewrites the institutional clauses — return-to-work language, attendance policy, qualification standards, fitness-for-work statements — removes most of the institutional risk in a single pass. Individual manager training is necessary but not sufficient; the policy is where the systemic risk lives.
Building an Inclusive Safety Culture — Beyond the Minimum
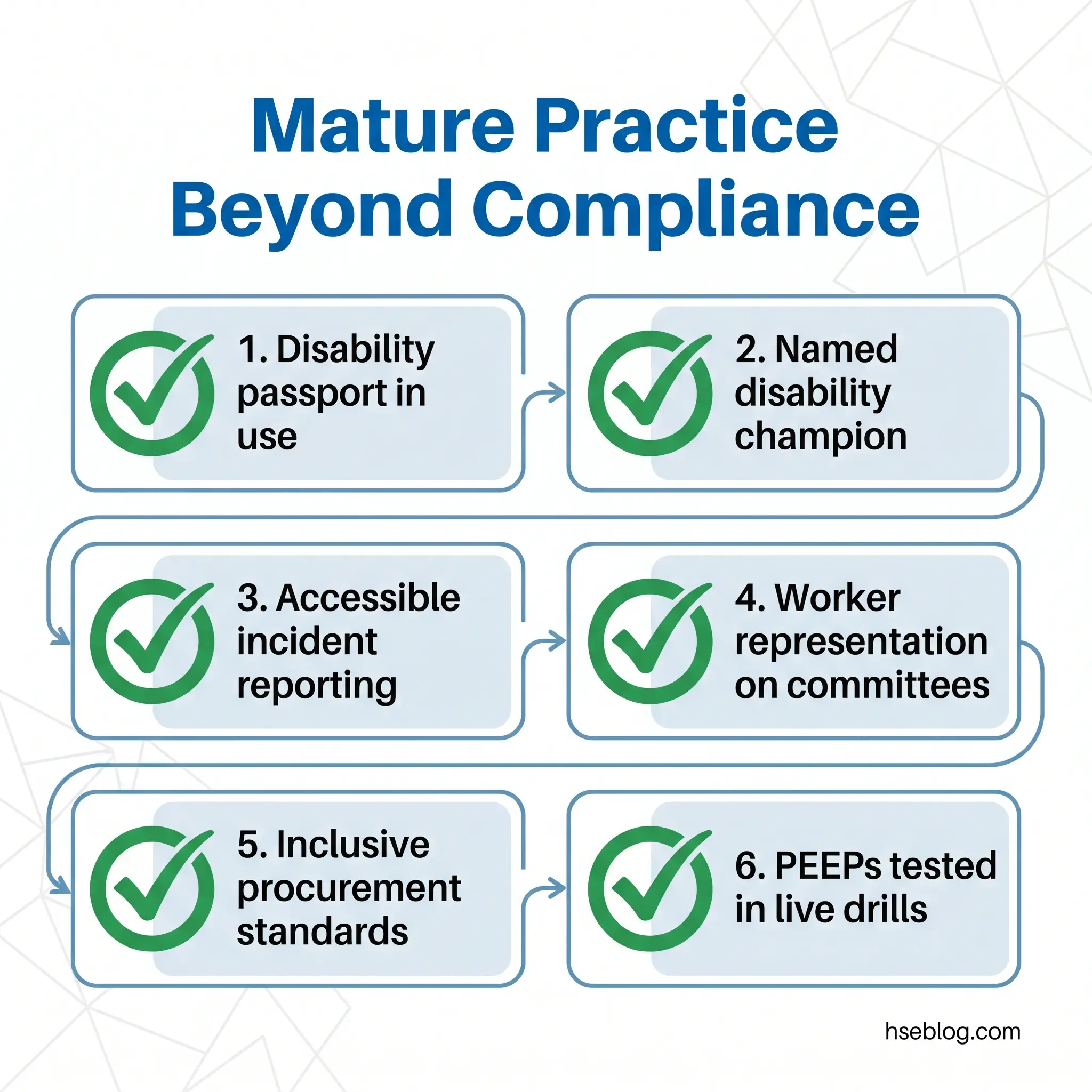
Compliance is the floor; mature practice goes further. The pattern across employers who outperform on both injury rates and dispute rates includes a small set of observable practices:
- A disability passport — a portable adjustment record that travels with the worker between roles, departments, and managers, so the same conversation does not have to be re-run every time the line manager changes.
- A named disability champion in HSE and HR functions, with the authority to escalate stalled accommodation processes.
- An accessible incident-reporting system — visual, audio, multi-language, and physically accessible — so that disabled workers can report hazards on equal footing.
- Disabled workers represented on safety committees, particularly when emergency procedures, layout changes, or new equipment are being assessed.
- Procurement standards that require assistive-tech compatibility in new IT systems and accessibility in physical works — preventing the next round of retrofits.
- PEEP testing in real drills, not on paper. A PEEP that has not been walked through with the named individual and assistants is unfinished.
These map directly to the ILO Code of Practice on Managing Disability in the Workplace (2002) — the international good-practice benchmark and a useful policy reference where local law is silent. None of these practices is required by statute. All of them sharply reduce both injury rates and dispute rates, and most of them cost very little to implement.
Frequently Asked Questions
Conclusion
Discharging employer duties for workers with disabilities (safety) cleanly comes down to four operational decisions taken together. Treat occupational-safety duty and equality duty as one obligation, not two separate compliance lanes. Run the interactive or adjustment process every time the trigger fires — a request, a return-to-work flag, a new role, a changed condition — and document the steps taken, the options considered, and the reason for the choice. Build any safety-based restriction on the four-factor direct-threat analysis or a proportionality test, with current individualised evidence, and only after reasonable adjustments have been examined.
The data is clear about where the risk concentrates. The EEOC’s FY2024 enforcement record points consistently to inflexible policies, “100% healed” return-to-work rules, no-fault attendance, and silence in the face of accommodation requests (US Equal Employment Opportunity Commission, 2024). Most of those failure modes sit in policy text, not in any individual manager’s intent. A policy review surfaces them faster and more reliably than manager training alone — and a one-page functional accommodation record, kept separately from the personnel file, removes most of the documentation risk.
The standard to aim for is operational, not aspirational. Every disabled worker on site has an assessment that follows the work rather than the diagnosis, an accommodation that has been implemented and reviewed, an emergency plan that has been tested in a real drill, and a route to re-open any of the above without HR drama. That is the pattern that satisfies both legal regimes simultaneously — and it is the pattern that protects the worker, which is the duty everything else exists to serve.