TL;DR
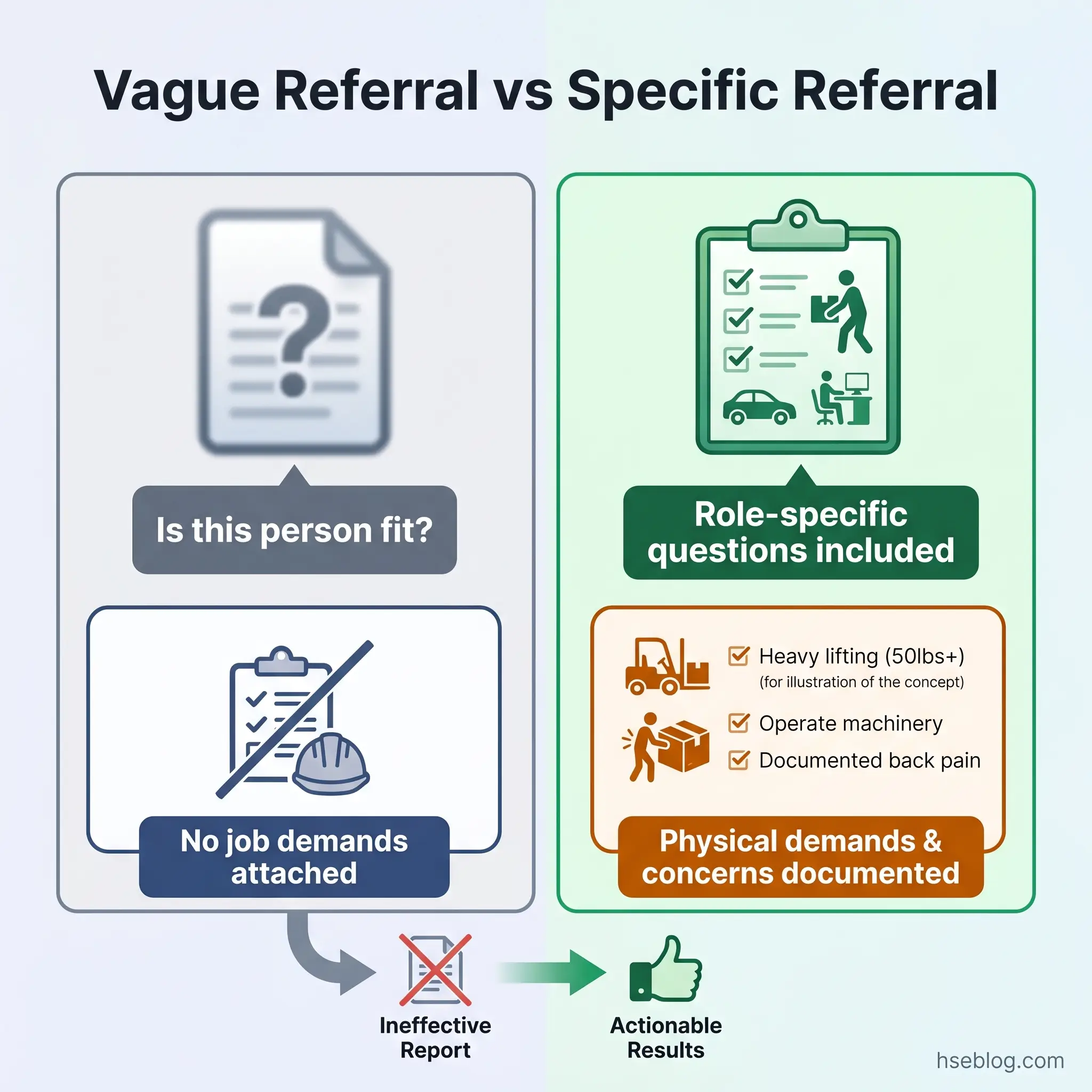
- If your referral says “is this person fit for work?” — you will get back a report too vague to act on. Specify the role’s essential functions, the exact concerns, and the questions you need answered.
- If you request an assessment without documented objective evidence — you are exposed to disability discrimination claims under the ADA (US) or the Equality Act 2010 (UK), regardless of your safety intentions.
- If the report recommends adjustments and you ignore them — you cannot later defend a dismissal by arguing the employee was unfit. The adjustment pathway must be explored and documented first.
- If you apply one country’s fitness-for-work policy across multiple jurisdictions — you are almost certainly non-compliant somewhere. The ADA and the Equality Act impose different rules at every stage of employment.
A fitness for work assessment is a structured evaluation by an occupational health professional that determines whether an employee can perform the specific physical and psychological demands of their role without unreasonable risk to themselves or others. It is always job-specific, governed by anti-discrimination law in every major jurisdiction, and designed to enable work through adjustments — not to exclude workers through a binary pass/fail gate.
The estimated cost to the UK state from economic inactivity due to ill health now reaches £212 billion annually (Keep Britain Working Review, 2025). In the US, 2.5 million employer-reported injury and illness cases were recorded in private industry in 2024 alone (Bureau of Labor Statistics, 2025). Behind those figures sit individual decisions — made by employers, HR teams, and safety professionals — about when and how to assess whether a worker can safely perform their role. Those decisions, handled well, protect both the worker and the operation. Handled poorly, they generate discrimination claims, regulatory citations, and outcomes that harm the very people they were meant to protect.
Fitness for work assessments sit at the intersection of occupational health, employment law, and operational safety — and that intersection is where most employer errors occur. This article provides a multi-jurisdictional, practitioner-level guide to what these assessments are, when employers can lawfully require them, how the process works, and where the common failure modes lie. The guidance covers both the US framework (ADA, FMLA, OSHA) and the UK framework (Equality Act 2010, HSWA 1974, MHSWR 1999) side by side, because employers operating across borders — or simply searching for best practice — need both.
What Is a Fitness for Work Assessment?
A fitness for work assessment evaluates the match between two variables: an individual worker’s current health status and the specific physical, cognitive, and psychological demands of their role. It is not a general health check-up, a wellness screening, or a blanket medical examination. The assessment is always task-matched — asking whether this person can safely perform this job without unreasonable risk to themselves or others.
The evaluation is conducted by an occupational health professional — typically a physician, occupational health nurse, or occupational psychologist — not by the employer, the line manager, or an HR generalist. The StatPearls clinical reference on fitness for duty provides a comprehensive framework of the assessment criteria used by clinicians. For employers, what matters is understanding the range of possible outcomes.
Those outcomes are not binary. The assessment may determine that a worker is fully fit, fit with specific restrictions or adjustments, temporarily unfit with a projected return timeline, or — in rare cases — permanently unable to meet the role’s essential demands. The most operationally valuable outcome is usually the “fit with adjustments” category. This is where the assessment creates the most benefit for both employer and employee, and it is precisely where employers most frequently fail to act. Treating the process as a pass/fail gate discards the adjustment pathway that anti-discrimination law in every major jurisdiction requires employers to explore.
| Outcome Category | What It Means for the Employer |
|---|---|
| Fit | Employee can perform all essential functions without restriction |
| Fit with adjustments | Employee can perform role with specified modifications — employer must explore feasibility |
| Temporarily unfit | Employee cannot currently perform the role — reassessment recommended at defined interval |
| Permanently unfit for this role | Essential functions cannot be met even with reasonable adjustments — alternative role or separation process begins |
Physical vs Psychological Fitness Assessments
Physical capacity evaluations assess musculoskeletal strength, cardiovascular fitness, sensory function, and the ability to meet specific physical demands — lifting, climbing, standing for extended periods, operating controls. Psychological and mental health assessments evaluate cognitive function, emotional stability, stress tolerance, and the capacity to make safety-critical decisions under pressure.
Both carry equal legal weight. A common misconception is that fitness for work assessments are primarily physical. In practice, psychological fitness assessments are increasingly standard in safety-critical and high-stress roles — emergency services, air traffic control, offshore operations, and healthcare among them. Mental health conditions accounted for 9.8% of UK sickness absences in 2024 (Office for National Statistics, 2025), and the regulatory expectation in both the US and UK is that employers assess psychological fitness with the same rigour applied to physical capacity.
When Should Employers Request a Fitness for Work Assessment?
Knowing when an assessment is warranted — and when it is not — is the single highest-stakes judgment call in this process. A request grounded in documented, objective evidence is lawful and defensible. A request based on subjective impression, assumption, or stereotype is a discrimination claim waiting to file.
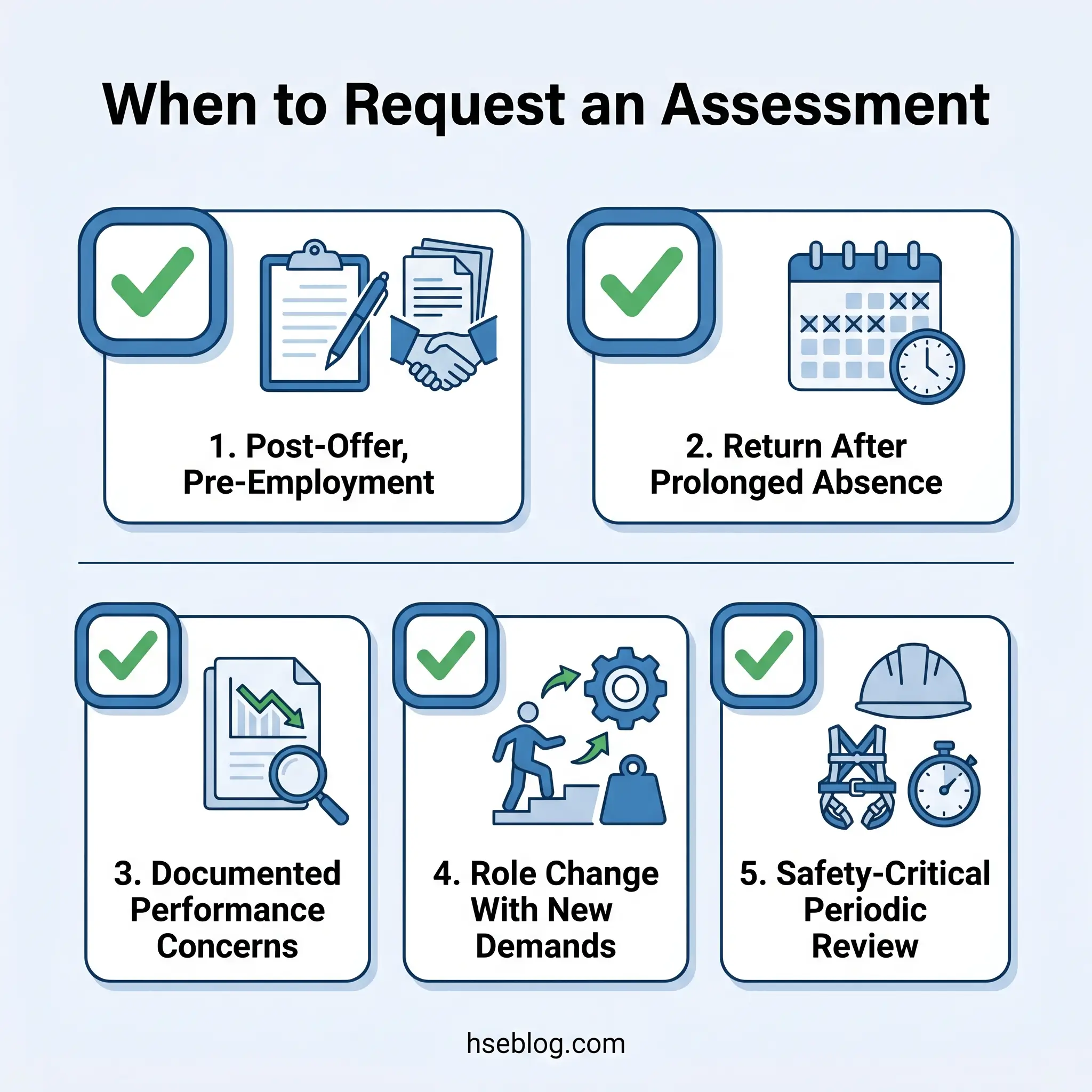
The legitimate trigger scenarios fall into distinct categories, each with its own legal and procedural considerations:
- Pre-employment / post-offer assessments — lawful only after a conditional offer of employment has been extended. Under ADA Section 12112(d) (US), pre-offer medical inquiries are prohibited. Under Equality Act 2010 Section 60 (UK), health questions before a job offer are restricted to narrow exceptions such as determining whether adjustments are needed for the recruitment process itself.
- Return-to-work after significant absence — following prolonged illness, surgery, injury, or a mental health episode. The US FMLA framework under 29 CFR §825.312 permits employers to require a fitness-for-duty certification before reinstating an employee returning from FMLA leave, limited to the condition that caused the absence.
- Observable performance or behavioural indicators — when documented, objective evidence suggests a worker’s capacity to perform essential functions has materially changed. This includes attendance patterns, incident frequency, observable impairment, or decline in task performance.
- Role change with materially different demands — transfer or promotion to a position with substantially different physical or psychological requirements.
- Periodic assessments in safety-critical roles — transport, confined space entry, working at height, emergency response, and other roles where fitness directly correlates with survival outcomes.
- For-cause assessments — triggered by a specific incident, near-miss, or behavioural pattern that raises a reasonable, articulable safety concern.
Watch For: The for-cause assessment is the most legally contentious trigger. Employment tribunal complaints in the UK and EEOC charges in the US most frequently originate from employers requesting assessments based on subjective impressions — “she seems off lately” — rather than documented, objective performance evidence. If you cannot point to specific, recorded observations, the request is vulnerable.
Legal Frameworks Governing Fitness for Work Assessments
The regulatory landscape governing fitness for work assessments differs substantially between jurisdictions, and applying one country’s rules across all operations is a reliable way to generate compliance exposure. The US and UK frameworks share a common principle — assessments must not be used to discriminate — but diverge significantly on when assessments are permitted, what information the employer can receive, and how the reasonable adjustment obligation operates.
In the US, the Americans with Disabilities Act structures employer medical inquiries across three stages. Before an offer of employment, disability-related medical inquiries and examinations are prohibited entirely. After a conditional offer but before employment begins, employers may require medical examinations provided they are applied to all entering employees in the same job category. Once employed, medical examinations are permissible only when they are “job-related and consistent with business necessity” — a standard enforced by the EEOC’s detailed guidance on disability-related inquiries. Separately, FMLA Section 825.312 permits employers to require a fitness-for-duty certification for workers returning from FMLA-qualifying leave, but limits the certification to the health condition that caused the absence. OSHA’s General Duty Clause under Section 5(a)(1) imposes an independent obligation to maintain a workplace free from recognised hazards — providing the safety rationale for assessments even where no specific OSHA standard applies.
In the UK, the Equality Act 2010 Section 60 prohibits pre-offer health questions except in narrow circumstances. The Health and Safety at Work etc. Act 1974 Section 2 establishes the employer’s duty to ensure the health, safety, and welfare of employees — the foundational basis for requiring fitness assessments. The Management of Health and Safety at Work Regulations 1999 Regulation 6 requires health surveillance where risk assessment identifies the need, though health surveillance and fitness-for-work assessments serve different purposes and are governed by different regulatory provisions. The UK fit note system, which certifies an employee’s fitness status during illness absence, is currently under reform following the Keep Britain Working Review (2025).
| Assessment Stage | US (ADA / FMLA) | UK (Equality Act / HSWA) |
|---|---|---|
| Pre-offer | Medical inquiries prohibited | Health questions restricted (Section 60) |
| Post-offer, pre-employment | Permitted if applied uniformly | Permitted; must not discriminate |
| During employment | Only if job-related and business necessity | Permitted under duty of care; must be proportionate |
| Return-to-work | FMLA fitness-for-duty certification permitted | OH referral standard practice; fit note required for absence evidence |
| Confidentiality | Medical records stored separately; supervisors receive restrictions only | GDPR applies; employer receives work-related outcomes only |
| Adjustment obligation | Reasonable accommodation under ADA | Reasonable adjustments under Equality Act 2010 |
A practical reality that multi-site and multinational employers must confront: fitness-for-work policies cannot be templated from one jurisdiction and applied globally. The ADA’s three-stage framework does not map onto the UK’s Section 60 restrictions, and the FMLA fitness-for-duty certification mechanism has no direct UK equivalent. Policies must be localised.
The “Job-Related and Consistent with Business Necessity” Standard
This ADA threshold is the single most litigated element of fitness-for-duty practice in the United States. The standard requires the employer to demonstrate that the medical examination is genuinely connected to the employee’s ability to perform the essential functions of their position and that there is a legitimate business reason for requiring it.
What constitutes sufficient “objective evidence” is narrower than many employers assume. Documented performance deficiencies, recorded attendance patterns, specific incident reports, and direct observations of impaired function have been upheld. Generalised concerns, co-worker rumours, or assumptions based on known diagnoses have not. The Tenth Circuit’s 2025 decision in Baker v. Alliance for Sustainable Energy reinforced that the employer’s evidence must be particularised and contemporaneous — historic performance issues that have since resolved do not satisfy the threshold for a current examination.
Jurisdiction Note: In the UK, the legal threshold for requesting an occupational health referral is less prescriptively defined than the ADA’s “business necessity” test, but the Equality Act 2010 still requires the request to be proportionate and non-discriminatory. An employer who repeatedly refers a disabled employee for assessments without clear justification risks a harassment claim.
How the Fitness for Work Assessment Process Works
The procedural quality of the assessment process determines whether the outcome is operationally useful or legally vulnerable. Each stage matters, and each is a point where employer errors commonly occur.
Step 1 — Document the objective evidence. Before making any referral, the employer must record the specific, observable basis for the assessment. This includes performance records, absence data, incident reports, and contemporaneous notes of observed behaviour. General impressions are not documentation. The record must be specific enough that a third party could review it and agree the concern is reasonable.
Step 2 — Prepare a role-specific referral. The referral to the occupational health provider is the single most influential input in the entire process. A referral that asks “is this person fit for work?” will produce a report too vague to act on. Effective referrals specify the role’s essential functions, describe the physical and cognitive demands, explain the specific concerns prompting the referral, and pose targeted questions about the employee’s capacity to meet those demands. Attaching the job description and a physical demands analysis is standard best practice.
The Fix That Works: Frame referral questions around the job, not the diagnosis. Instead of “does this employee’s condition prevent them from working?”, ask “can this employee safely perform confined space entry, including climbing vertical ladders, wearing SCBA, and maintaining communication with the standby person, given the concerns documented in this referral?”
Step 3 — Communicate with the employee. Explain the purpose of the assessment, the employee’s rights, what information will and will not be shared with the employer, and the confidentiality protections in place. Most refusals stem from fear or misunderstanding, not obstruction. Transparent communication at this stage prevents escalation later.
Step 4 — The assessment itself. Conducted by the qualified occupational health professional, typically lasting 30–60 minutes. It may include a clinical interview, physical examination, functional capacity testing, and — where relevant — psychometric or cognitive evaluation. The scope is determined by the referral questions and the role’s demands, not by a generic template.
Step 5 — Receive and interpret the report. The employer receives fitness-for-work advice and adjustment recommendations. The employer does not receive the diagnosis, detailed clinical history, or treatment information. The report should address each question posed in the referral with a clear, actionable answer.
Step 6 — Act on the recommendations. Implement the recommended adjustments, plan a phased return, or — if adjustments are not feasible — begin the interactive process (US) or reasonable-adjustment exploration (UK) with full documentation. Ignoring recommendations without recorded justification creates significant liability.
Medical Confidentiality and Data Handling
Confidentiality failures in fitness-for-work processes rarely involve dramatic data breaches. They occur through informal channels — a manager receiving clinical details by phone, a poorly redacted report left in an inbox, or a verbal briefing that discloses the diagnosis rather than the work restrictions alone.
Under ADA requirements (US), medical records generated through fitness assessments must be stored in files separate from the employee’s personnel record. Access must be strictly limited. Supervisors and managers receive only the information necessary to implement work restrictions or accommodations — never the underlying diagnosis or treatment details. In the UK, assessment data falls under GDPR, medical ethics obligations, and Equality Act protections. The occupational health provider shares work-related outcomes with the employer; clinical details remain confidential between the practitioner and the employee.
The operational risk is not just formal storage. It is the informal information flow. When a line manager learns — through a casual conversation, an overheard phone call, or a report that should have been redacted — that an employee has a particular diagnosis, that knowledge influences subsequent management decisions whether the manager intends it to or not. Effective confidentiality policies must address these informal channels explicitly. The standard to set is clear: managers know what the employee can and cannot do, and what adjustments to implement. They do not know why.
Fitness for Work in Safety-Critical and High-Risk Roles
In sectors where worker fitness directly determines whether people live or die, the assessment framework is more prescriptive, more frequent, and carries higher operational stakes.
US Department of Transportation regulations under 49 CFR §391.41 require commercial motor vehicle drivers to undergo biennial medical examinations by a certified medical examiner. The physical qualification standards are specific: vision, hearing, blood pressure, cardiovascular fitness, musculoskeletal function, and absence of conditions likely to cause loss of consciousness. These are not discretionary employer decisions — they are federally mandated, and driving without valid medical certification is a violation that can shut down an operation.
In the UK, safety-critical roles in rail, aviation, and offshore oil and gas operate under industry-specific medical standards that often exceed general employment law requirements. Workers performing confined space entry, working at height, or involved in LOTO-controlled maintenance must be assessed against the specific physical and cognitive demands of those tasks — not against a generic fitness standard.
The judgment call that matters most in safety-critical sectors is understanding that medical clearance is a point-in-time snapshot, not a permanent status. A worker certified fit in January may develop a condition by March that changes their risk profile. Fitness is dynamic, and the gap between assessment cycles is where risk accumulates. This is why periodic reassessment, combined with a reporting culture where workers can disclose health changes without fear of automatic exclusion, produces better safety outcomes than rigid pass/fail gatekeeping alone.
Audit Point: Review whether your periodic medical assessments for safety-critical roles include the specific functional demands of the role — or whether they default to a generic health screen that misses the task-specific risks.
Functional capacity evaluations (FCEs) deserve particular mention. Unlike standard medical assessments, FCEs involve task-specific physical testing — can this worker actually lift this load, climb this ladder, sustain this posture for this duration? For physically demanding roles, an FCE provides data that a clinical interview alone cannot.
What Happens If an Employee Refuses a Fitness for Work Assessment?
Employee refusals generate anxiety on both sides. The employer fears losing control of the process. The employee fears the result will be used against them. Both responses lead to errors.
If the employer’s request is lawfully grounded — based on documented objective evidence, tied to a legitimate business necessity, and proportionate to the concern — refusal can carry consequences. In the US, where a fitness-for-duty examination meets the ADA’s “job-related and consistent with business necessity” standard, an employee who refuses without justification may face disciplinary action. Under FMLA, an employer can delay reinstatement if the returning employee refuses to provide the required fitness-for-duty certification.
In the UK, refusal to attend an occupational health assessment is not automatically misconduct. However, the employer can draw reasonable inferences from the refusal when making subsequent management decisions — and employment tribunals have upheld this position where the employer’s request was demonstrably justified and the employee was informed of the consequences.
The practical failure modes run in two directions. Some employers back down entirely after a refusal, establishing a precedent that assessments are optional and undermining the programme for every future case. Others escalate immediately to formal disciplinary action, triggering a grievance or discrimination claim that could have been avoided. The approach that works — and the one that withstands tribunal scrutiny — is re-engagement: explaining the purpose of the assessment again, clarifying the confidentiality protections, acknowledging the employee’s concerns, and documenting each step of the process. Most refusals resolve when fear is addressed.
How Are Fitness for Work Assessments Changing?
The regulatory and operational landscape is shifting in both major jurisdictions, and employers relying on policies drafted three or five years ago are already behind.
In the UK, the Keep Britain Working Review published in November 2025 proposed a Workplace Health Provision model built around structured Stay-in-Work and Return-to-Work Plans that may eventually replace or supplement the current fit note system. A three-year Vanguard Phase (2026–2029) is underway. Separately, UK Statutory Sick Pay reforms effective 6 April 2026 — enacted under the Employment Rights Act 2025 — removed the three-day waiting period and the Lower Earnings Limit threshold, making SSP payable from day one and expanding eligibility to lower-paid workers. These changes increase employer payroll exposure and heighten the business case for effective fitness-for-work programmes that support early return.
The UK has also expanded the range of professionals authorised to issue fit notes beyond GPs — since July 2022, nurses, physiotherapists, occupational therapists, and pharmacists can certify fitness status. This change is designed to reduce bottlenecks and improve the quality of fitness advice, as these professionals often have more direct knowledge of the patient’s functional capacity than a GP working under ten-minute appointment constraints.
In the US, appellate case law continues to refine the boundaries of the “job-related and consistent with business necessity” standard. The Tenth Circuit’s 2025 decision in Baker v. Alliance for Sustainable Energy narrowed the circumstances under which employers can rely on historical performance concerns to justify a current fitness-for-duty examination, reinforcing the requirement for contemporaneous, particularised evidence.
Across both jurisdictions, the direction of travel is consistent: toward earlier intervention, structured stay-in-work support, and a model that treats fitness for work as an ongoing, dynamic management process rather than a reactive gatekeeping exercise. Employers who build their programmes around this trajectory — prevention, adjustment, and supported return — will find themselves aligned with where regulators, case law, and occupational health practice are all heading.
Frequently Asked Questions
Conclusion
The regulatory trajectory across both the US and UK points in the same direction: fitness for work assessments are evolving from reactive gatekeeping tools into components of a broader, prevention-oriented occupational health model. The Keep Britain Working Review’s Workplace Health Provision framework, the UK’s day-one SSP reforms, and the narrowing of the ADA’s business-necessity threshold in recent appellate decisions all signal that employers will face increasing scrutiny on how they manage fitness for work — not just whether they do it.
For employers building or reviewing their fitness for work assessment programmes now, three priorities stand above the rest. First, anchor every assessment request in documented, role-specific, objective evidence — because this is where most discrimination complaints originate. Second, invest in referral quality — because a referral that specifies the job’s demands and asks targeted questions produces a report the employer can actually use. Third, treat the “fit with adjustments” outcome as the default working assumption rather than an inconvenient middle ground — because this is where the most operational value lies, and it is what regulators and tribunals expect to see explored before any adverse decision.
Fitness for work is not a binary verdict. It is an ongoing, dynamic process of matching worker capacity to role demands — and the employers who understand that distinction will manage both their legal exposure and their people more effectively than those still operating a pass/fail gate.