

TL;DR
- Mental health first aiders are trained workplace responders who recognize signs of mental distress, offer initial support, and guide colleagues toward professional help — they do not diagnose or treat.
- Structured training programs run 1–2 days and cover crisis intervention, active listening, and referral pathways aligned with recognized frameworks such as MHFA England or MHFA Australia.
- ISO 45003:2021 now formalizes psychosocial risk management as part of occupational health and safety systems, making mental health first aid a practical compliance tool.
- Organizations with trained mental health first aiders report measurable reductions in absenteeism and improvements in early intervention rates, though benefits depend on genuine organizational commitment — not token appointments.
A mental health first aider is a trained individual in the workplace who provides initial support to someone experiencing a mental health difficulty or crisis, connecting them with appropriate professional resources. Unlike physical first aiders — whose role is universally understood — mental health first aiders operate in a space where role boundaries, training standards, and organizational expectations vary significantly across jurisdictions, making clear definition and proper implementation essential for both the responder and the person they support.
Depression and anxiety alone cost the global economy an estimated $1 trillion per year in lost productivity (World Health Organization, 2022). That figure represents not an abstract economic indicator but a measure of human suffering that starts at the individual level — workers in distress, unsupported and unrecognized, deteriorating until the consequences become impossible to ignore.
The response across many organizations has been to train designated employees as mental health first aiders. The logic mirrors physical first aid: someone on site, accessible and trained, who can provide an informed initial response before professional support arrives. What separates effective mental health first aid programs from performative ones is the depth of training, the clarity of role boundaries, and whether the organization actually builds a system around the individual. This article examines what the role involves, how training is structured, what the regulatory landscape expects, and where programs commonly fail.
What Is a Mental Health First Aider?
A mental health first aider is a designated, trained employee who serves as the first point of contact when a colleague shows signs of mental health difficulty or is in acute psychological distress. The role mirrors physical first aid in intent — stabilize, support, refer — but differs fundamentally in scope and boundaries.
The distinction matters because misunderstanding the role creates two opposite failure modes.
- Under-definition — the first aider is appointed but given no clear scope, no referral pathways, and no organizational backing. They become a name on a poster.
- Over-definition — the first aider is expected to function as an in-house counselor, absorbing complex cases they are neither trained nor qualified to handle.
What Mental Health First Aiders Do
The core functions are consistent across recognized training frameworks:
- Recognize early warning signs — changes in behavior, withdrawal, concentration difficulties, increased absence, or expressions of hopelessness.
- Approach and offer non-judgmental support — initiate a conversation using trained listening techniques, without diagnosing or advising on treatment.
- Provide initial reassurance — normalize help-seeking and reduce the stigma that prevents many workers from accessing support.
- Guide toward appropriate professional help — connect the individual with Employee Assistance Programs (EAPs), occupational health services, their GP, or crisis services as warranted.
- Maintain confidentiality within defined limits — respect privacy while understanding the duty to escalate where there is risk of serious harm.
What They Do Not Do
This boundary is non-negotiable in every credible training program:
- They do not diagnose mental health conditions.
- They do not provide therapy, counseling, or ongoing treatment.
- They do not replace qualified mental health professionals.
- They do not take on a caseload or become the person’s primary support indefinitely.
In HSE practice, the interpretation of this boundary is where most organizational confusion occurs. A trained first aider who has a helpful conversation with a distressed colleague may be quietly expected to “keep an eye on them” without any formal handover to professional services — an arrangement that serves neither party.
Core Responsibilities in Practice
The practical responsibilities of a mental health first aider extend beyond the initial conversation. Reviewing published guidance from MHFA England and comparable frameworks, a consistent pattern of operational responsibilities emerges.
During a Mental Health Crisis
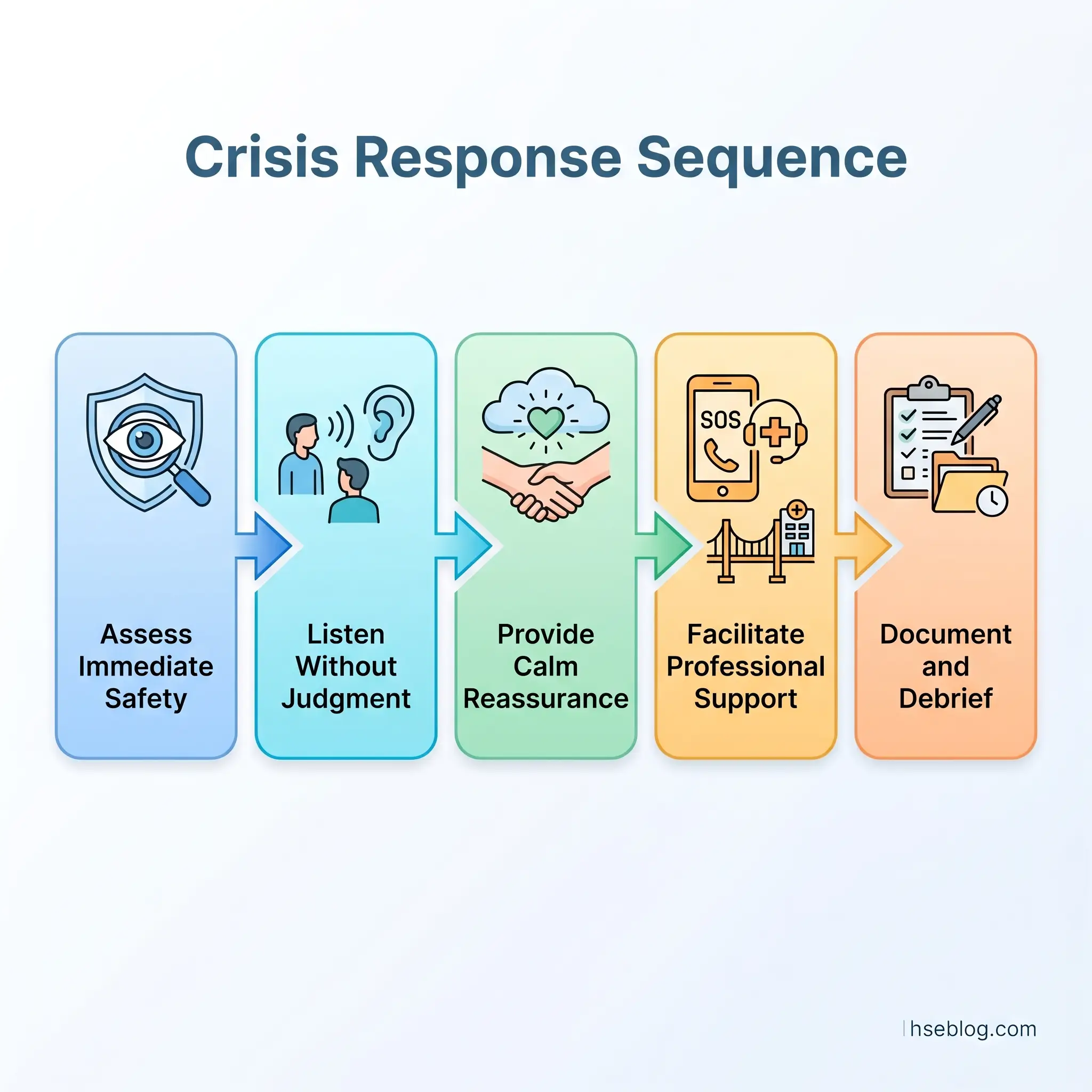
When someone is in acute distress — a panic attack, suicidal ideation disclosed in conversation, or a severe emotional breakdown at work — the first aider’s responsibility follows a specific sequence:
- Assess the situation for immediate safety — is the person at risk of self-harm or harm to others?
- Listen without judgment — allow the person to express what they are experiencing without interruption, advice-giving, or minimization.
- Provide calm reassurance — presence and steadiness matter more than words. Avoid phrases like “just think positive” or “others have it worse.”
- Facilitate access to crisis support — if risk of self-harm is present, support the person in contacting emergency services or a crisis helpline. Do not leave them alone if risk is immediate.
- Document and debrief — record the interaction (within confidentiality limits) and debrief with a manager or occupational health professional.
Between Crises: The Ongoing Role
The day-to-day function is less dramatic but equally important:
- Visibility and accessibility — colleagues know who they are and that they are approachable.
- Normalizing conversations about mental health — their presence signals organizational permission to talk about psychological wellbeing.
- Feeding back patterns (not names) — alerting management to systemic stressors such as excessive workload, bullying, or organizational change causing widespread anxiety, without breaching individual confidentiality.
How Mental Health First Aid Training Works
Recognized mental health first aid training programs follow structured curricula developed by accredited bodies. The two most widely adopted frameworks globally are MHFA England (used across the UK and adapted internationally) and MHFA Australia (the original program, developed in 2000).
Training is typically delivered over one to two days, either in-person or through a blended format combining online learning with facilitated group sessions.
What Training Covers
The curriculum across accredited programs consistently includes:
- Mental health literacy — understanding the spectrum of mental health conditions including depression, anxiety disorders, psychosis, substance use disorders, and eating disorders.
- Risk factors and warning signs — behavioral, emotional, and physical indicators that a colleague may be struggling.
- The ALGEE action plan (used in MHFA Australia-derived programs):
- A — Approach, assess, and assist with any crisis
- L — Listen and communicate non-judgmentally
- G — Give support and information
- E — Encourage appropriate professional help
- E — Encourage other supports (social, community, self-help)
- Crisis first aid skills — responding to suicidal thoughts, self-harm, panic attacks, traumatic events, and acute psychotic episodes.
- Referral pathways — knowing what services exist, how to access them, and how to support someone through the process.
- Self-care for the first aider — recognizing compassion fatigue and maintaining personal boundaries.
Training Standards and Accreditation
The judgment call for organizations is which training program to select. Not all “mental health awareness” courses are equivalent.
| Criterion | Accredited MHFA Program | Generic Awareness Course |
|---|---|---|
| Duration | 1–2 full days (12–16 hours) | Often 2–4 hours |
| Crisis skills | Included with practice scenarios | Usually absent |
| Certification | Nationally recognized, time-limited | Variable or none |
| Refresher requirement | Typically every 3 years | Rarely specified |
| Evidence base | Peer-reviewed outcome studies | Limited |
A half-day awareness session has value for general workforce education, but it does not produce a competent mental health first aider. Organizations that conflate the two create risk — an employee titled “mental health first aider” who lacks the training depth to handle what the title implies.
Legal and Regulatory Context
No jurisdiction currently mandates mental health first aiders in the same way physical first aiders are required. However, the regulatory trajectory is clear, and existing legal duties already encompass psychosocial risk.
UK — Health and Safety at Work Act 1974
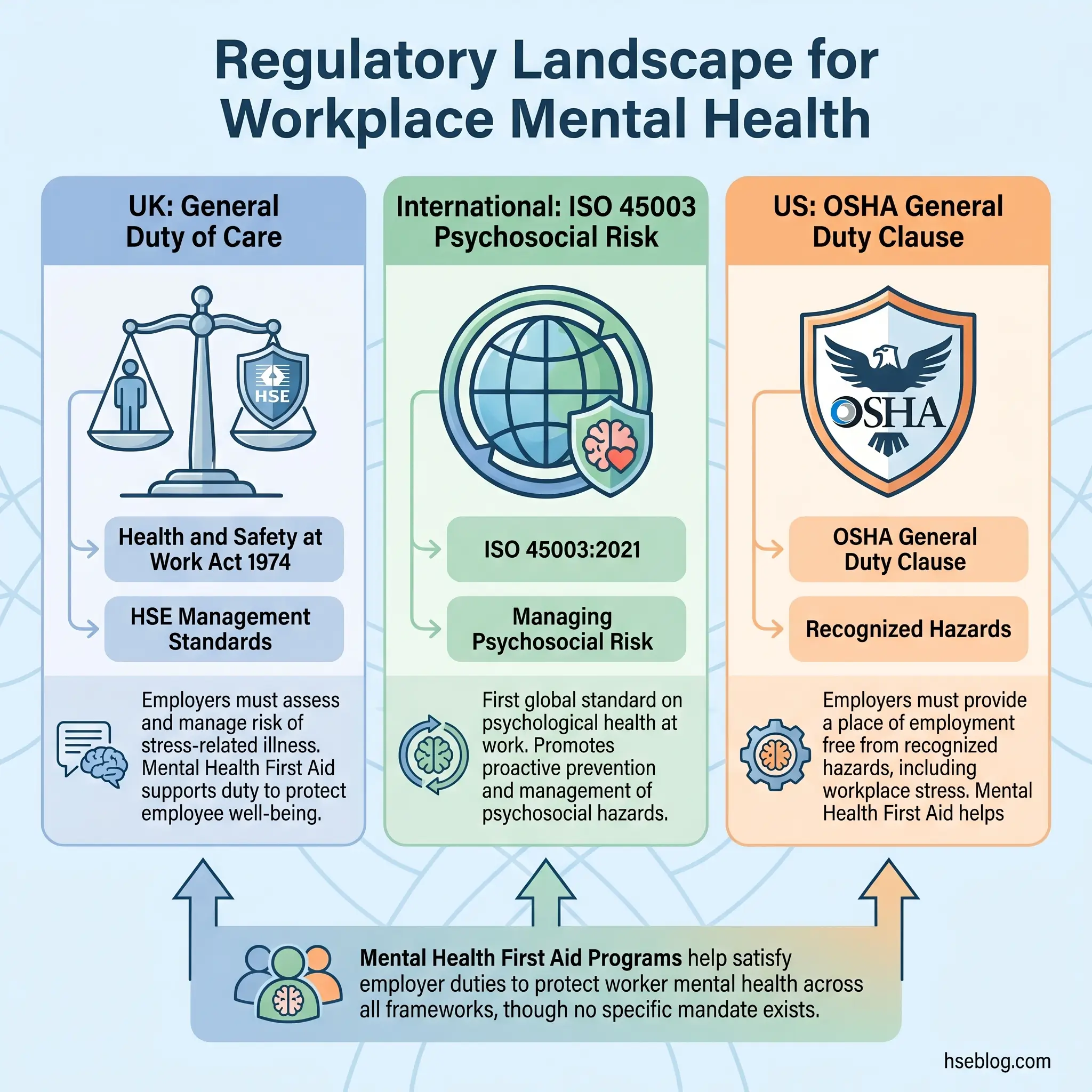
Under the Health and Safety at Work Act 1974 (UK), employers have a general duty to ensure, so far as is reasonably practicable, the health, safety, and welfare of employees at work. “Health” in this context is not limited to physical health.
The HSE UK Management Standards for Work-Related Stress identify six key areas of work design that, if not properly managed, are associated with poor health and wellbeing:
- Demands — workload, work patterns, and work environment
- Control — how much say a person has in the way they do their work
- Support — encouragement, sponsorship, and resources provided by the organization and colleagues
- Relationships — promoting positive working to avoid conflict and dealing with unacceptable behavior
- Role — whether people understand their role and whether the organization ensures they do not have conflicting roles
- Change — how organizational change is managed and communicated
Mental health first aiders fit within the “Support” pillar. While not explicitly mandated, their appointment demonstrates proactive management of psychosocial risk — a factor that becomes relevant in enforcement action and civil claims.
International — ISO 45003:2021
ISO 45003:2021, published as the first global standard providing guidance on managing psychosocial risk in the workplace, sits within the ISO 45001 occupational health and safety management system framework. It directs organizations to identify psychosocial hazards, assess the risks, and implement controls.
The standard does not prescribe mental health first aiders by name, but its requirements for worker support, early intervention, and return-to-work processes align directly with what trained first aiders provide.
US — OSHA General Duty Clause
Under OSHA’s General Duty Clause, Section 5(a)(1) of the OSH Act, employers must provide a workplace free from recognized hazards likely to cause death or serious physical harm. OSHA has increasingly acknowledged workplace psychosocial hazards, though enforcement remains less developed than in the UK or EU.
The practical reading of this for US-based operations: while there is no specific OSHA standard requiring mental health first aiders, organizations in industries with elevated psychosocial risk — emergency services, healthcare, high-stress manufacturing environments — demonstrate due diligence by implementing structured mental health support.
Workplace Benefits — What the Evidence Actually Shows
Published outcome studies on mental health first aid training report consistent patterns, though the evidence base has limitations worth acknowledging. The benefits are real, but they are conditional on organizational context.
For the Organization
Research published in peer-reviewed journals and organizational case studies consistently identifies several measurable outcomes:
- Reduced absenteeism related to mental health — the UK lost 17.1 million working days to work-related stress, depression, or anxiety in 2022/23 (HSE UK, 2023). Organizations with early intervention mechanisms report faster identification and support, reducing the duration of absence episodes.
- Improved return-to-work outcomes — employees who receive early, non-judgmental support are more likely to engage with professional treatment and return to productive work sooner.
- Positive return on investment — research by Deloitte found that for every £1 invested in mental health interventions in the workplace, employers received an average return of £5 (Deloitte, 2020). Mental health first aider programs represent one of the lower-cost intervention types within that landscape.
- Reduced presenteeism — workers present but functioning below capacity due to untreated mental health issues represent a larger productivity cost than absenteeism in most analyses.
For the Workforce
The benefits to individual employees operate through two mechanisms:
- Direct support — the person in distress receives timely, informed initial help rather than being ignored, misunderstood, or told to “toughen up.”
- Cultural signal — the visible presence of trained mental health first aiders communicates that the organization takes psychological wellbeing seriously, which reduces stigma and increases willingness to seek help across the entire workforce.
The Honest Limitation
A common misconception holds that appointing mental health first aiders solves an organization’s mental health problem. It does not.
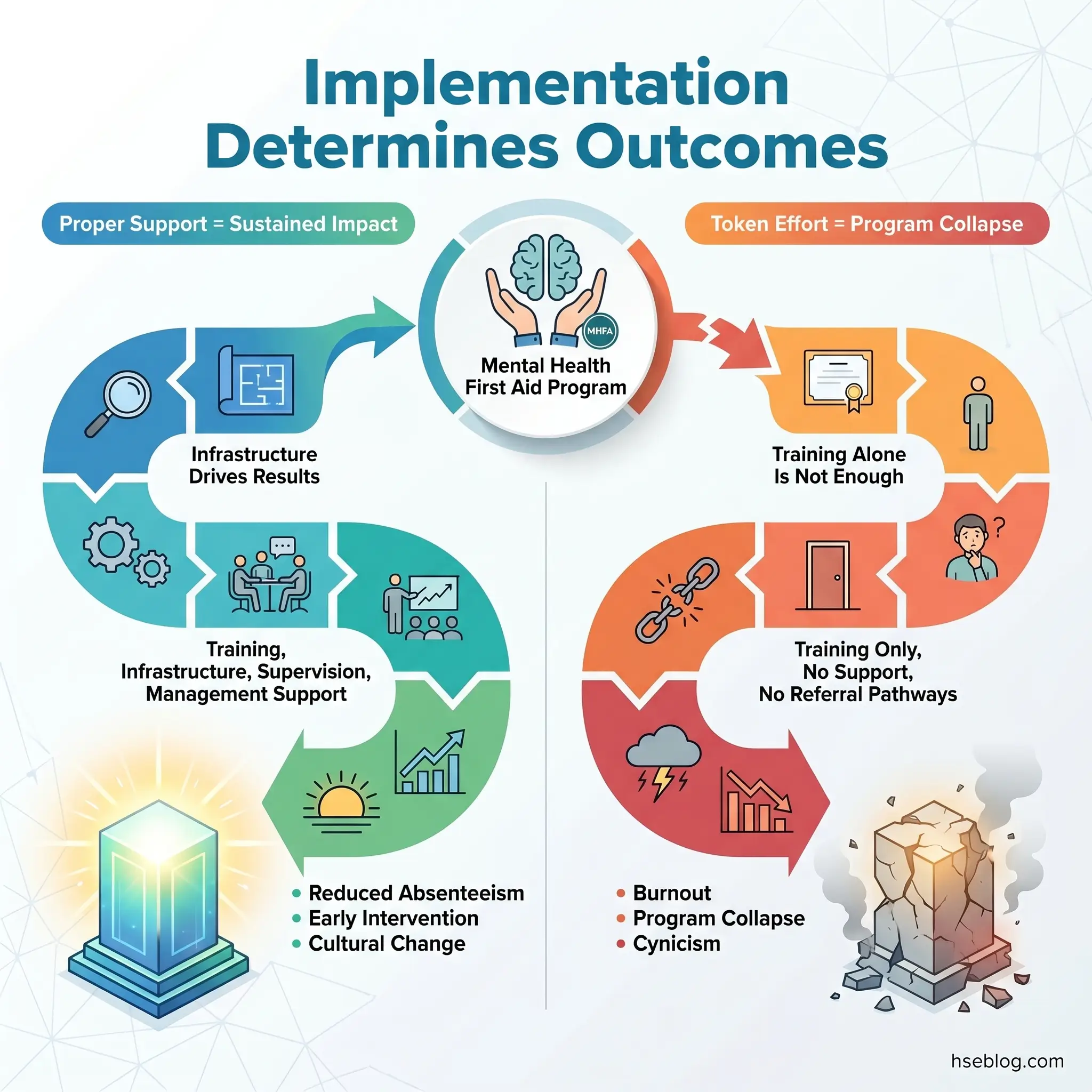
Mental health first aiders are a point-of-contact intervention. They cannot fix toxic management, excessive workload, bullying cultures, or systemic organizational dysfunction. If the psychosocial hazards remain uncontrolled, first aiders become overwhelmed, burn out, and the program collapses — often leaving the organization convinced that “mental health initiatives don’t work.”
The published record on failed programs consistently shows the same pattern: training was delivered, certificates were issued, but no supporting infrastructure followed. No protected time for the role, no supervision, no clear referral pathways, and no management commitment to addressing the root causes first aiders were reporting.
Common Misconceptions About Mental Health First Aiders
Several persistent misunderstandings undermine both the credibility and the effectiveness of mental health first aid in the workplace. Each deserves direct correction.
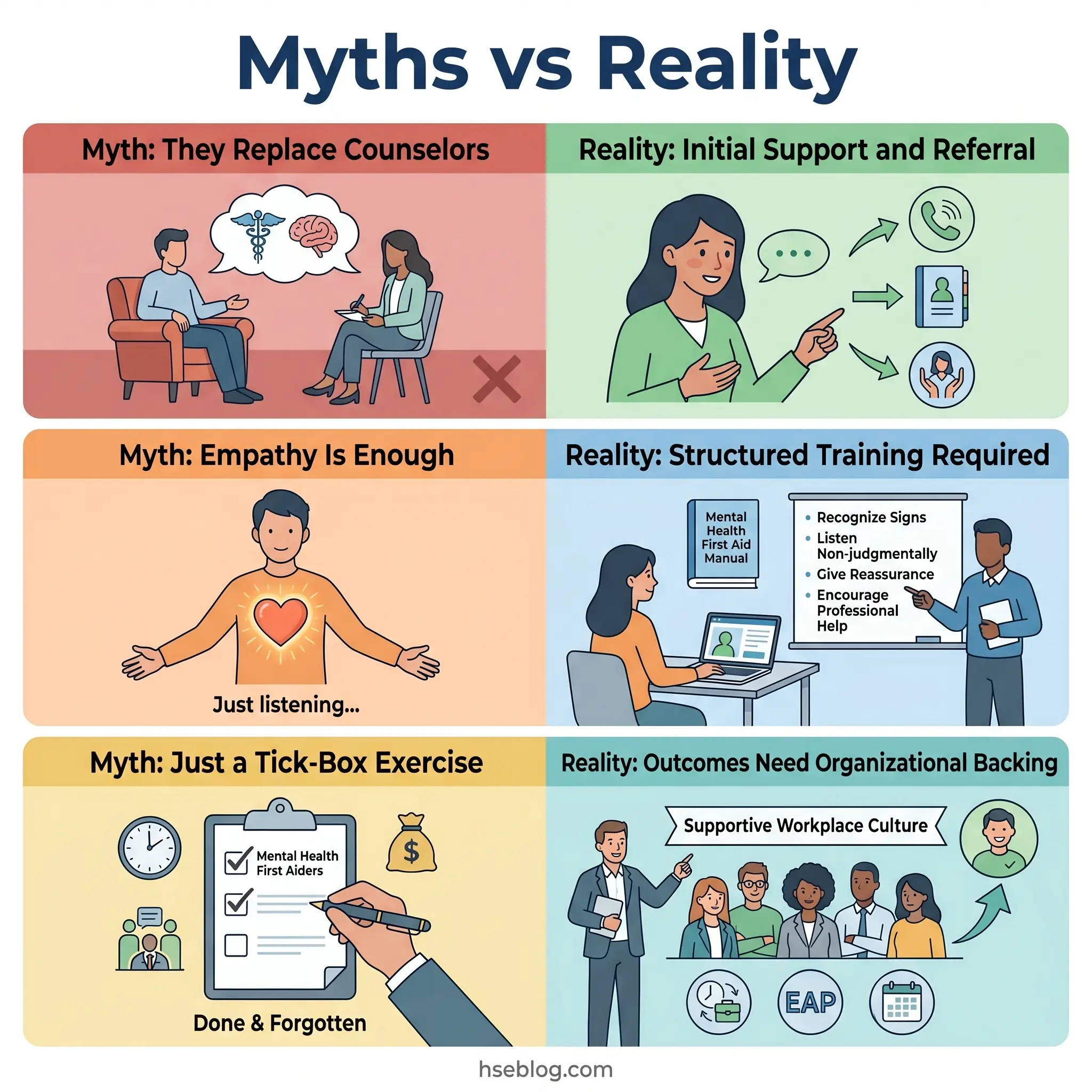
“They’re Basically In-House Counselors”
This is the most damaging misconception because it sets up the first aider for failure and the distressed worker for inadequate care. A mental health first aider has 12–16 hours of training. A qualified counselor has years of supervised clinical practice.
The analogy holds precisely: a physical first aider applies a bandage and calls the paramedic. They do not perform surgery. A mental health first aider listens, supports, and guides toward professional help. They do not provide ongoing therapy.
“Anyone With Empathy Can Do It”
Empathy is necessary but insufficient. Without structured training, well-meaning colleagues commonly make three errors:
- Giving advice instead of listening — “Have you tried exercise?” / “You should talk to your manager.”
- Minimizing — “Everyone feels stressed sometimes.”
- Over-involving themselves — taking on emotional burden they are not equipped to process, leading to secondary trauma.
Training provides the framework that channels empathy into effective, boundaried support.
“It’s Just a Tick-Box Exercise”
This becomes true only when organizations treat it as one. Where mental health first aiders are properly supported — given protected time, access to supervision, clear referral pathways, and genuine management backing — the programs produce measurable outcomes. The tick-box criticism describes implementation failure, not a flaw in the concept.
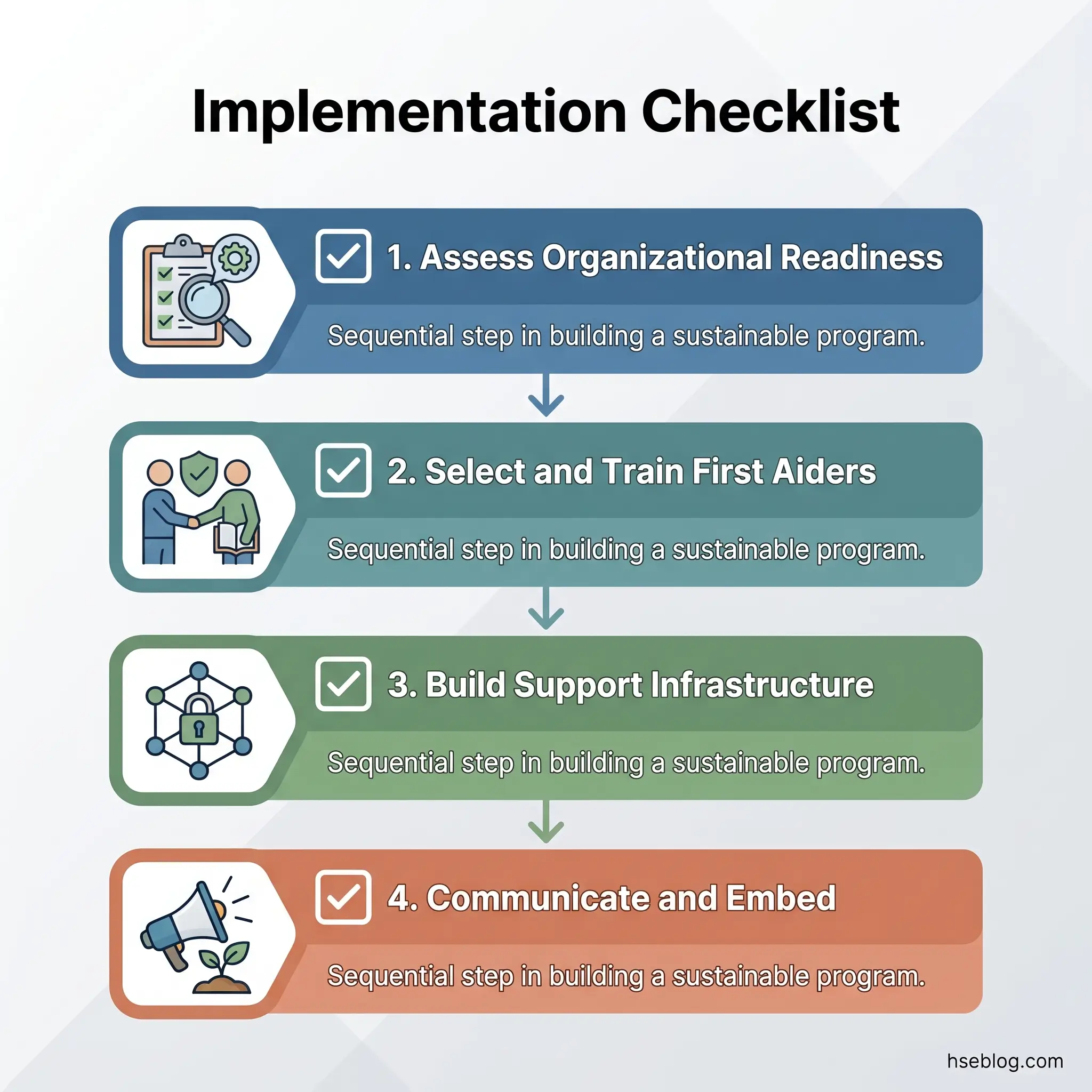
How to Implement a Mental Health First Aid Program
Implementation determines whether a mental health first aid program delivers value or becomes another expired certificate in a training file. The difference lies in treating mental health first aid as a system, not an event.
Step 1: Assess Organizational Readiness
Before selecting candidates for training, answer three questions:
- Do referral pathways exist? If there is no EAP, no occupational health service, and no relationship with external mental health providers, training first aiders creates a dead end. They will identify need but have nowhere to direct it.
- Will management support the role? This means protected time, not just permission. A first aider who is pulled away from their primary duties to support a colleague needs their workload adjusted, not a sympathetic nod followed by the expectation to catch up.
- Is there a psychosocial risk assessment in place? ISO 45003:2021 and the HSE UK Management Standards both require organizations to assess and manage psychosocial risks. First aiders operating without this context are treating symptoms of hazards nobody is controlling.
Step 2: Select and Train the Right People
Selection criteria matter more than many organizations recognize.
- Voluntary participation — coerced first aiders are ineffective first aiders. The role requires genuine willingness.
- Diverse representation — first aiders should reflect the workforce in terms of role level, department, shift pattern, age, and background. A program staffed entirely by HR managers will not reach the shop floor.
- Emotional resilience and boundaries — candidates with their own unresolved mental health difficulties may be retraumatized by the role. This requires sensitive screening, not exclusion, but honest conversation.
Choose an accredited training provider. The certification should be nationally recognized, include crisis skills, and specify a refresher period.
Step 3: Build the Support Infrastructure
This is where most programs fail.
- Supervision — regular check-ins with a qualified mental health professional who can debrief complex cases and monitor the first aider’s own wellbeing.
- Clear escalation protocols — written procedures for when and how to escalate to occupational health, HR, or emergency services.
- Confidentiality framework — what is recorded, where, who has access, and under what circumstances confidentiality is overridden (imminent risk of harm).
- Refresher training — skills degrade. Most accredited programs recommend refresher training every two to three years.
Step 4: Communicate and Embed
- Make first aiders visible — names, photos, contact methods displayed in common areas and on the intranet.
- Brief all managers on the first aider’s role and its limits.
- Integrate mental health first aid into induction programs for new staff.
- Report on program activity (anonymized) to senior leadership quarterly.
Frequently Asked Questions
Conclusion
The pattern across organizations that fail at workplace mental health support is remarkably consistent: they invest in training, appoint first aiders, and then leave those individuals to operate without referral pathways, supervision, or management commitment to addressing the psychosocial hazards creating the demand. The training certificate becomes a substitute for systemic change, and when the program inevitably underperforms, the concept is blamed rather than the implementation.
What the evidence and regulatory trajectory make clear — from the HSE UK Management Standards through ISO 45003:2021 — is that mental health first aiders function as one component of a psychosocial risk management system, not as the system itself. Their value is genuine and measurable when they operate within a structure that supports them: clear role boundaries, accessible professional referral pathways, regular supervision, and an organizational culture that treats mental health with the same seriousness it applies to physical hazards.
The single highest-impact change most organizations can make is to stop treating mental health first aider training as the end point and start treating it as the beginning of a support infrastructure. Train the right people, build the system around them, manage the hazards they report, and protect the first aiders from the compassion fatigue that will otherwise drive them out of the role within a year.