TL;DR
- Assess psychosocial risks first — use validated tools like the HSE Management Standards framework to identify your organization’s specific stressors before writing a single policy clause.
- Build multi-stakeholder ownership — a policy drafted by HR alone and launched by email rarely survives its first quarter; secure named senior leadership sponsorship and consult employees, managers, and occupational health professionals.
- Cover prevention and support equally — most failed policies treat an Employee Assistance Program as the entire strategy while ignoring workload design, management practices, and job control.
- Label every legal obligation by jurisdiction — ADA reasonable accommodations (US), Management Standards risk assessment (UK), and Framework Directive 89/391/EEC (EU) impose different obligations; organizations operating across borders should align with ISO 45003:2021 as the baseline.
- Set a review cycle from day one — a policy without monitoring metrics and a minimum annual review date becomes a static document, not an operational commitment.
A workplace mental health policy is a formal document that sets out how an organization prevents psychosocial harm, supports employees experiencing mental health challenges, and integrates psychological health into its occupational health and safety management system. It should cover scope, psychosocial risk assessment, preventive measures, support resources, reasonable accommodations, confidentiality protections, return-to-work protocols, anti-stigma commitments, assigned responsibilities, and a defined review cycle.
What Is a Workplace Mental Health Policy and Why Does It Matter?
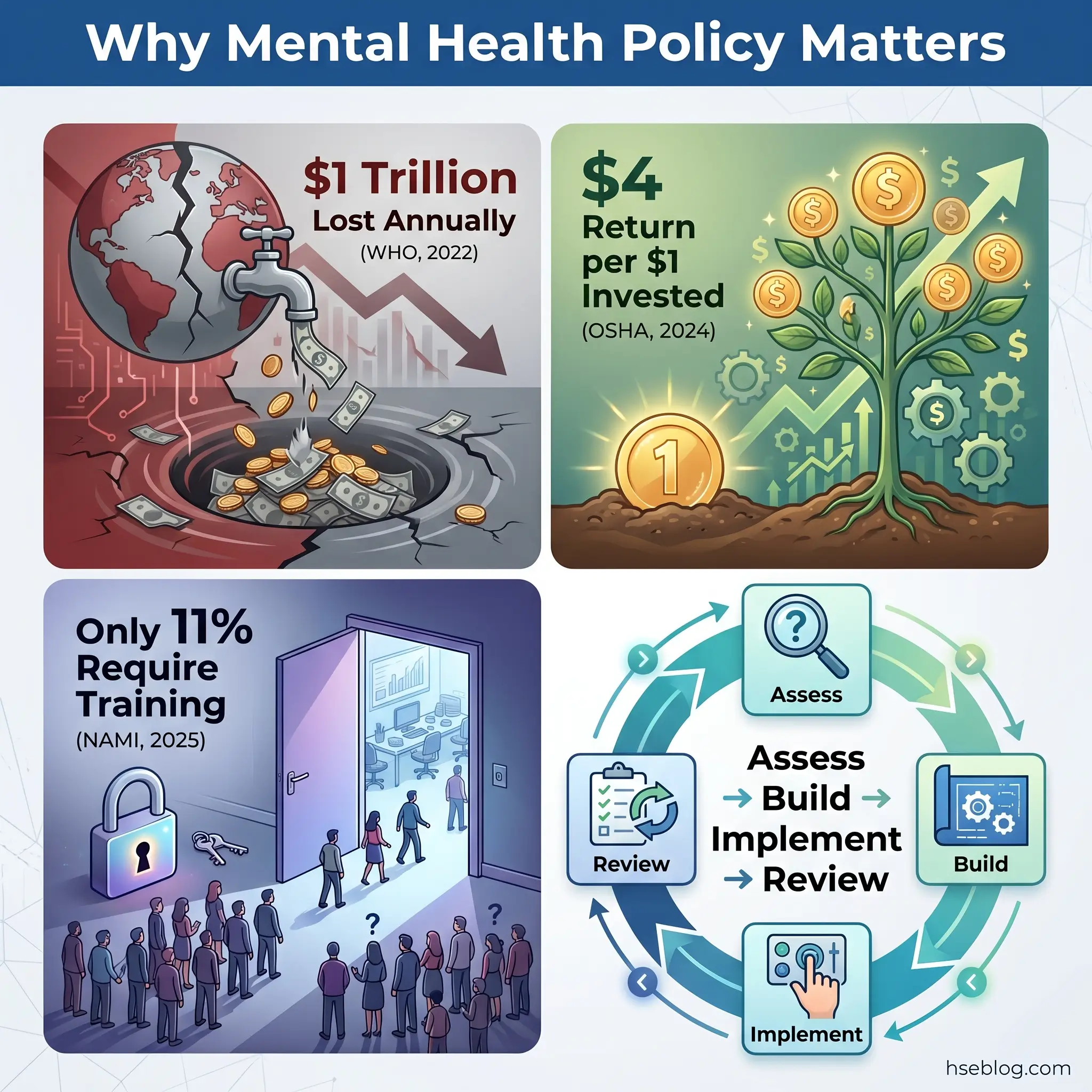
Poor mental health costs UK employers approximately £51 billion per year through combined presenteeism, absenteeism, and staff turnover (Deloitte, 2024). Globally, the World Health Organization estimates that 12 billion working days are lost annually to depression and anxiety alone, costing approximately $1 trillion in lost productivity (WHO, 2022). These are not abstract projections — they represent a quantifiable organizational failure that a well-built mental health policy is specifically designed to address.
A workplace mental health policy is distinct from a wellness program or an Employee Assistance Program. It is a formal, documented commitment that defines how an organization will:
- Prevent psychosocial harm through systemic controls — workload management, job design, management practices
- Support employees already experiencing mental health conditions — through accommodations, confidential referrals, and return-to-work procedures
- Integrate psychological health into its broader health and safety management system, not treat it as a standalone HR initiative
The legal imperative is equally concrete. In virtually every major jurisdiction, an existing duty of care already encompasses psychological health — even where no standalone mental health regulation exists. Employers who wait for a specific mental health statute before acting are already behind their legal obligations.
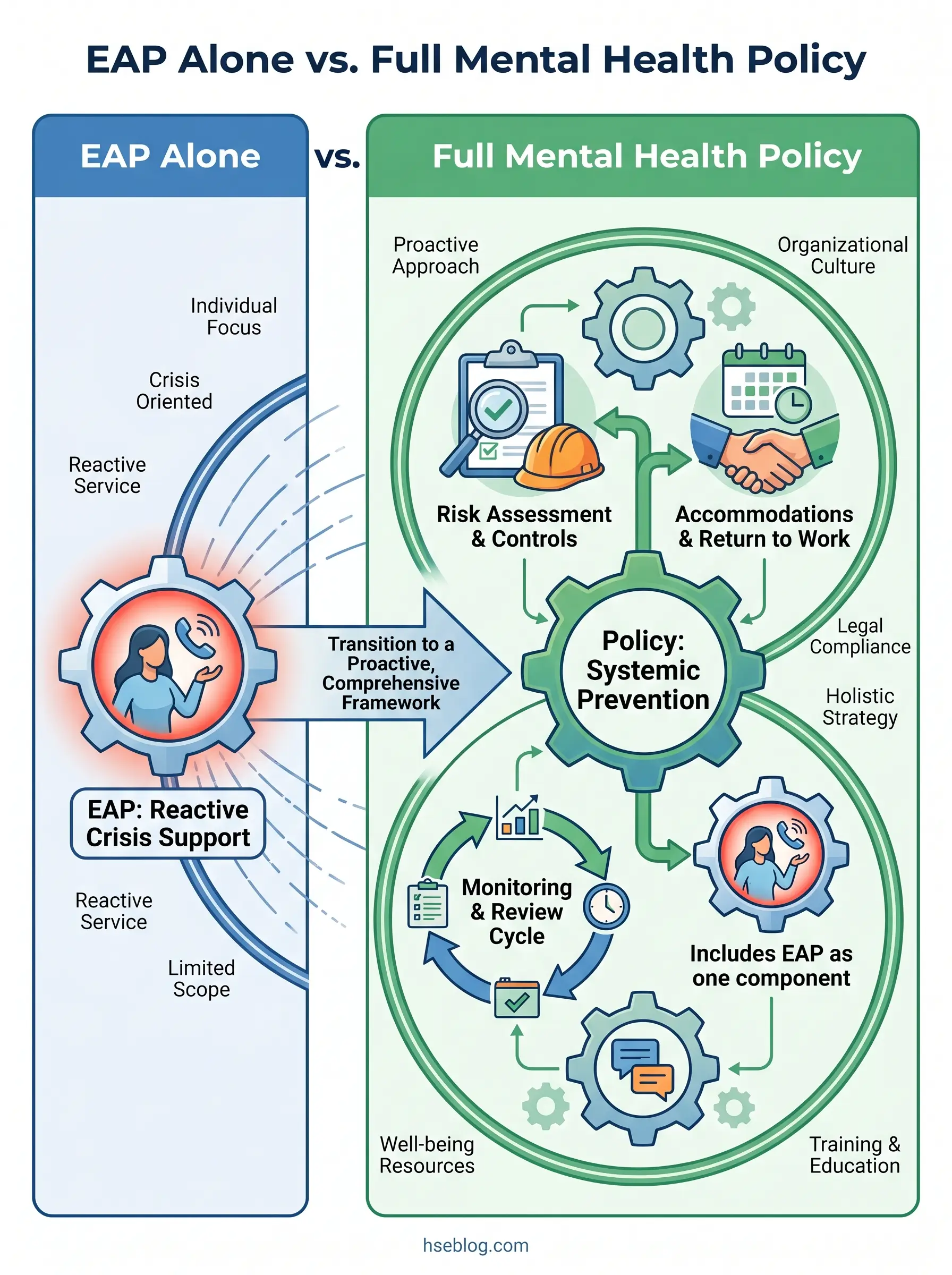
A pattern I consistently observe across organizations is the confusion between having an EAP and having a mental health policy. An EAP is a reactive resource — it helps individuals who have already reached a point of distress. A policy is a proactive framework that addresses the organizational conditions creating that distress in the first place. Treating the EAP as the entire mental health strategy is the single most common failure mode, and it leaves the preventive and systemic dimensions completely unaddressed.
Who Is Responsible for a Workplace Mental Health Policy?
The single biggest predictor of whether a mental health policy becomes operational or decorative is whether a named senior leader — not the HR department generically — champions its rollout and reviews its outcomes. Policies launched by memo rarely survive their first quarter.
Many organizations default to treating mental health policy as purely an HR deliverable. In practice, it requires a stakeholder model with clearly assigned responsibilities:
- Senior leadership must visibly sponsor the policy and signal organizational commitment. Without executive-level ownership, the policy becomes a document filed in a shared drive rather than a culture driver.
- HR or people operations typically leads drafting, coordinates stakeholder input, and manages the consultation process — but cannot do this in isolation.
- Line managers are the implementation layer. They conduct day-to-day interactions, notice early signs of distress, and either enable or undermine the policy through their behavior.
- Employee representatives or unions provide frontline perspective on actual psychosocial stressors and, in unionized environments, may shape policy provisions through collective bargaining.
- Occupational health professionals advise on clinical aspects — referral pathways, fitness-for-work assessments, return-to-work protocols.
- Legal counsel reviews jurisdictional compliance, particularly around disability discrimination, confidentiality, and reasonable accommodation obligations.
ISO 45003:2021 explicitly requires worker participation and consultation in psychosocial risk management. This is not optional best practice — it is a structural requirement of the standard. Organizations that draft policy without employee input are building on assumptions about what matters rather than evidence of what employees actually experience.
What Should a Workplace Mental Health Policy Include?
A comprehensive employee mental health policy must cover both the prevention of psychosocial harm and the support of individuals already affected. The components below form the structural backbone — each one exists for a specific operational and legal reason, not as aspirational padding.
Scope, Purpose, and Commitment
The policy opens by defining who it covers and what it commits to. Scope should explicitly include all employees — remote, hybrid, part-time, and contractors where applicable. Remote and hybrid workers face distinct psychosocial risks including isolation, blurred work-life boundaries, and reduced manager visibility of distress, and the policy must address these directly.
A clear statement of organizational commitment to psychological health — signed by the most senior leader, not a department head — establishes accountability from the outset.
Psychosocial Hazard Identification and Risk Assessment
The policy must define the psychosocial hazards relevant to the organization and describe how they will be assessed. The HSE Management Standards for work-related stress provide a well-validated six-factor model covering demands, control, support, relationships, role, and change. ISO 45003 offers a broader categorization: aspects of work organization, social factors, work environment, equipment, and hazardous tasks.
This is where many policies fall short. They reference “psychosocial risks” in general terms but never specify a methodology or assign responsibility for conducting the assessment.
Preventive Measures and Controls
Prevention means addressing the organizational conditions that generate psychosocial harm — not just offering support after harm occurs. Effective provisions include:
- Workload management — defined expectations, realistic deadlines, monitoring of excessive hours
- Job control — employee input into how work is organized and sequenced
- Anti-bullying and harassment protections — with clear reporting pathways and enforcement
- Flexible working arrangements — where operationally feasible
- Communication practices — including right-to-disconnect provisions for remote workers
Support Resources
This section details the reactive supports available: EAP access, mental health days, counseling benefits, Mental Health First Aiders, and signposting to external services. The key practitioner insight here is that listing resources is insufficient — the policy must explain how employees access them and what confidentiality protections apply.
Reasonable Accommodations
Under US law (ADA, Title I), employers with 15 or more employees must provide reasonable accommodations for qualified employees with mental health conditions constituting disabilities. Under the UK Equality Act 2010, employers must make reasonable adjustments. The policy should establish the right to request accommodations and define the interactive process for determining them.
Examples include flexible scheduling, modified workload, quiet workspaces, time off for appointments, and phased return-to-work arrangements — but accommodations are determined individually, not listed exhaustively.
Confidentiality and Anti-Stigma Commitments
The policy must guarantee that disclosure of a mental health condition will not result in career penalty, disciplinary action, or unauthorized sharing of personal information. Anti-discrimination commitments should be explicit, not implied.
Return-to-Work Procedures
Structured return-to-work protocols following mental-health-related absence — including phased returns, adjusted duties, and ongoing support — reduce the risk of relapse and signal organizational commitment to recovery rather than punishment.
Monitoring, Review, and Accountability
Every provision needs a named owner or function and a review date. A policy that lists aspirations without assigning accountability for each is functionally inert.

How to Assess Psychosocial Risks Before Drafting the Policy
Before writing the policy, organizations must understand their specific psychosocial risk landscape. Skipping this step is the equivalent of writing a chemical safety policy without knowing which chemicals are on site.
The assessment process draws on multiple data sources:
- Anonymous employee surveys using validated instruments — the HSE Indicator Tool or the Copenhagen Psychosocial Questionnaire (COPSOQ) provide structured, comparable data.
- Review of existing organizational data — absence records coded for stress, anxiety, or depression; staff turnover patterns; grievance and complaint trends; exit interview themes.
- Focus groups or structured conversations across different teams and levels — these surface qualitative insights that surveys miss.
- Identification of sector-specific hazards — shift work, lone working, client-facing aggression, high-consequence decision-making, or organizational change all carry distinct psychosocial risk profiles.
The judgment call here is between survey-heavy and conversation-heavy approaches. A 30-question survey distributed to 5,000 employees generates data that frequently sits unanalyzed. Three well-facilitated focus groups across different teams often surface more actionable insights. Match the consultation method to the organization’s size and culture — there is no universal correct approach.
The WHO guidelines on mental health at work, published in 2022, provide evidence-based recommendations for organizational interventions, manager training, and individual support that can inform the assessment framework.
How to Handle Confidentiality and Disclosure
Employees must never be required to disclose a mental health diagnosis to their line manager as a condition of accessing support. The policy should clarify the limited circumstances where health information may be shared — on a need-to-know basis, with consent, or through formal occupational health referral processes.
Under US law, the ADA restricts employer medical inquiries to specific circumstances, and HIPAA protections apply to health information. Under UK law, the Equality Act 2010 prohibits employers from asking about health conditions before a job offer except in narrow, defined situations. The EEOC guidance on mental health conditions and ADA rights provides authoritative reference on the US framework.
A common misconception is that encouraging openness about mental health means expecting disclosure. Psychological safety means employees feel safe to disclose if they choose to — not that they are expected or pressured to share diagnoses. The policy must protect both the right to disclose and the right not to.
How to Write and Draft the Policy Step by Step
The procedural core of creating a workplace mental health policy follows a defined sequence. Each step builds on the previous one — skipping steps is where most drafting processes fail.
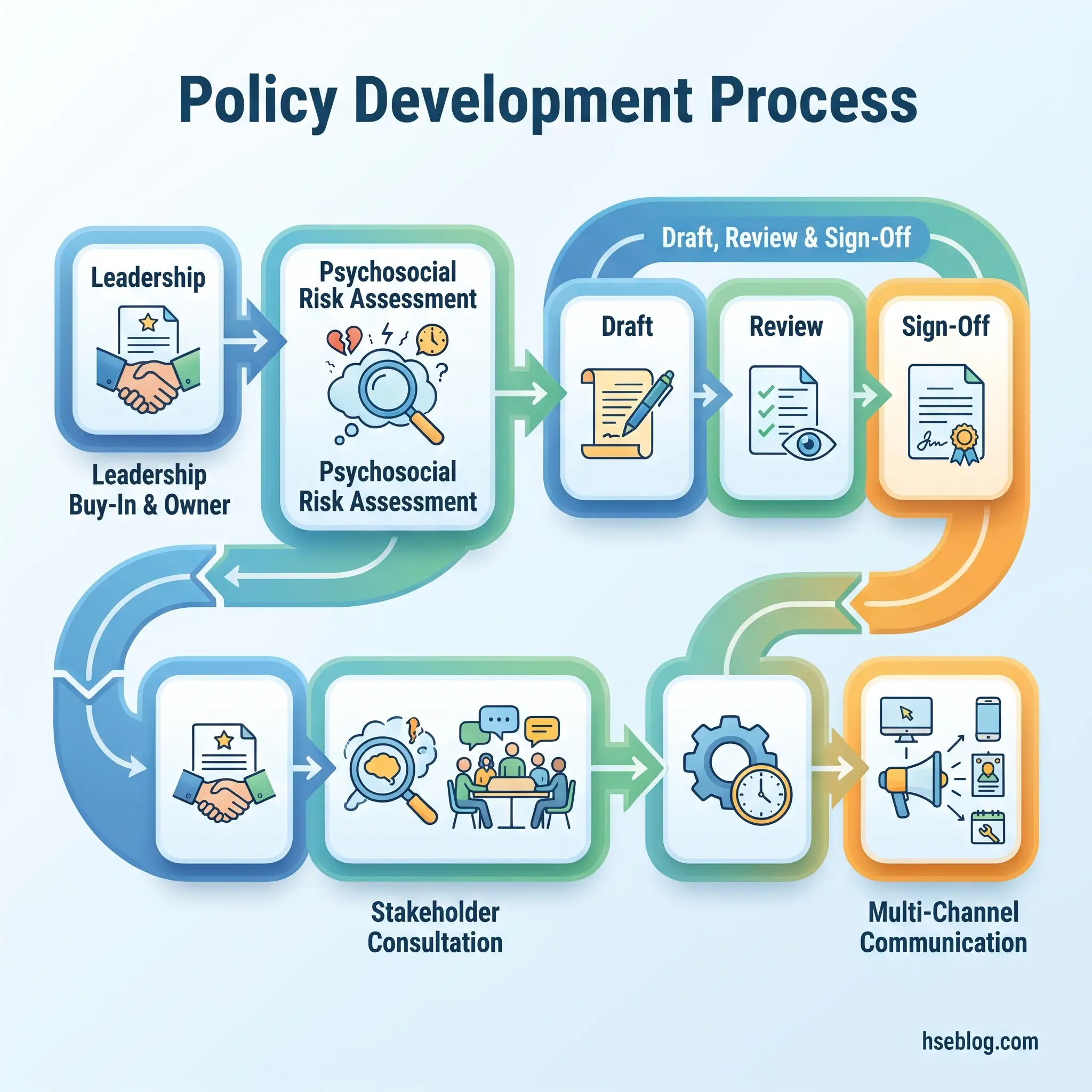
- Secure leadership buy-in and appoint a policy owner. Identify a named senior leader who will sponsor the policy publicly. Appoint an operational owner — typically in HR or OHS — responsible for managing the development process.
- Conduct a baseline psychosocial risk assessment. Use the methods described above to establish the organization’s specific risk profile before drafting begins.
- Consult stakeholders. Engage employees, line managers, union representatives, occupational health professionals, and legal counsel. ISO 45003:2021 requires worker participation — this is not a courtesy step.
- Research jurisdictional legal obligations. Identify which frameworks apply based on where the organization operates. Multi-jurisdiction employers must map obligations across all relevant territories.
- Draft the policy using the components framework. Build each section around the structure outlined in the previous section — scope, risk assessment, preventive controls, support resources, accommodations, confidentiality, return-to-work, and review.
- Circulate the draft for feedback. Include frontline managers and employee representatives, not just senior leadership. The people who will implement the policy daily must find it workable.
- Finalize and obtain sign-off. Set an effective date and a first review date. Senior leadership sign-off signals organizational commitment.
- Communicate through multiple channels. A single email announcement is insufficient. Use team briefings, induction programs, intranet placement, and visible leadership endorsement.
The consultation step deserves particular attention. It is where organizations most frequently either cut corners or over-engineer. The goal is actionable insight into the organization’s actual psychosocial conditions — not a data-collection exercise that generates reports nobody reads.
Legal Requirements Employers Must Understand
The regulatory content below reflects general HSE professional understanding of each jurisdiction’s requirements as of 2025. It is not legal advice. Specific compliance questions or enforcement situations should be directed to qualified legal counsel in the applicable jurisdiction.
The most common compliance error is assuming that the absence of a standalone mental health regulation means there is no legal obligation. In every major jurisdiction covered here, existing duty-of-care legislation already encompasses psychological health.
The following table summarizes how employer obligations differ across key jurisdictions:
| Jurisdiction | Primary Legal Basis | Core Employer Obligation | Enforcement | Standalone Psychosocial Regulation? |
|---|---|---|---|---|
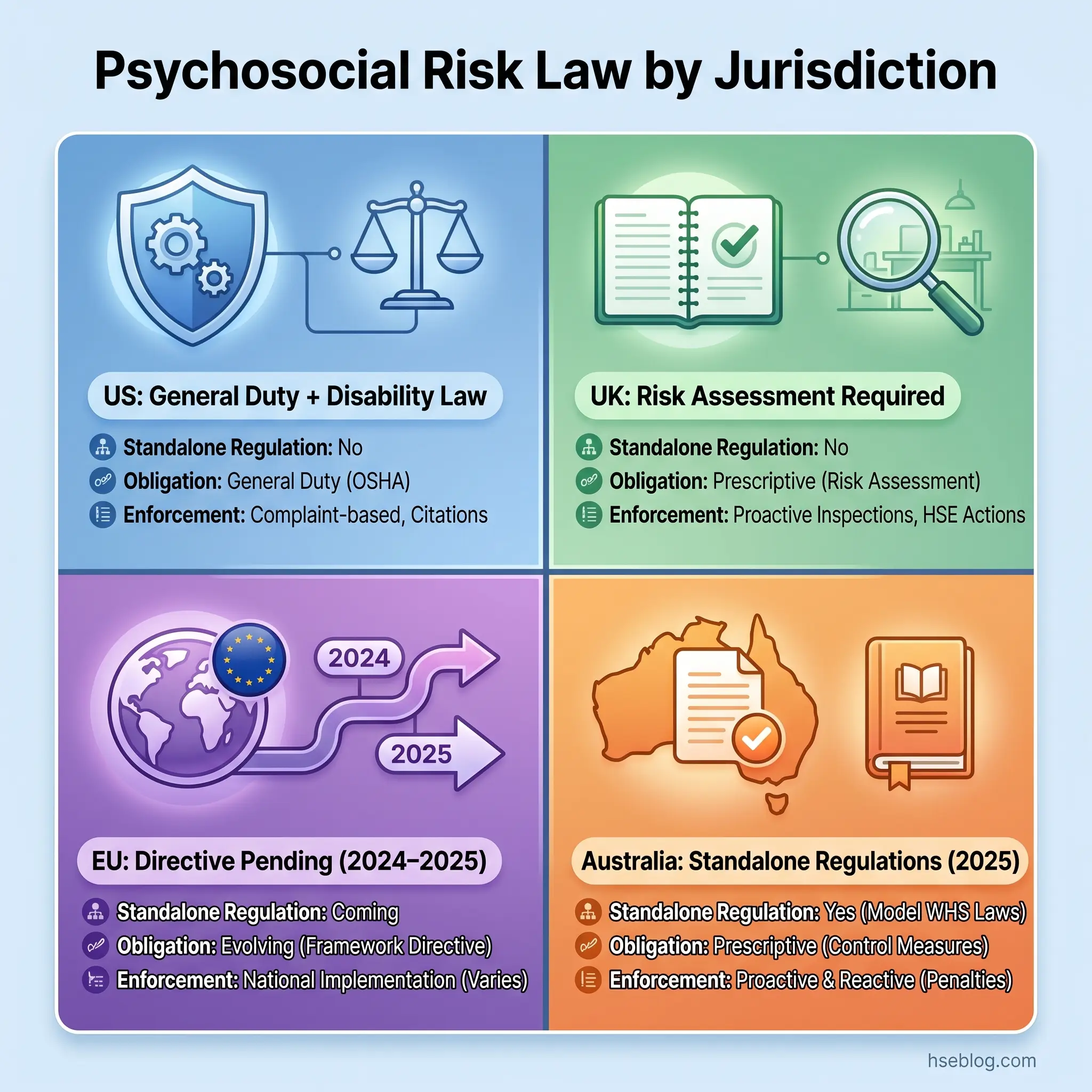
| US | ADA Title I; OSHA General Duty Clause §5(a)(1); FMLA; MHPAEA | Reasonable accommodations for mental health disabilities; workplace free from recognized hazards; job-protected leave; benefit parity | EEOC (discrimination); OSHA (hazards); DOL (FMLA) | No — relies on general duty and disability law |
| UK | HSWA 1974 §2; Management of H&S at Work Regs 1999; Equality Act 2010 | Ensure health, safety, and welfare including psychological health; assess all risks including psychosocial; reasonable adjustments for disabilities | HSE (safety); Employment Tribunal (discrimination) | No standalone statute, but HSE Management Standards provide a detailed framework |
| EU | Framework Directive 89/391/EEC | Assess and manage all workplace risks including psychosocial; general duty to ensure safety and health in every work-related aspect | Member state enforcement bodies | Not yet — ETUC adopted a resolution in October 2024 calling for a binding EU Directive on psychosocial risk prevention |
| Australia | Model WHS Regulations; Victoria OHS (Psychological Health) Regulations 2025 | Identify psychosocial hazards; eliminate or reduce risks so far as reasonably practicable | State regulators (e.g., WorkSafe Victoria) | Yes — Victoria’s 2025 Regulations are the first standalone psychosocial hazard regulations in Australia |
| Global | ISO 45003:2021 | Guidelines for managing psychosocial risk within an OHS management system | Voluntary (not certifiable) — but demonstrates best practice | Guidelines standard, not regulatory |
US Framework
Under the Americans with Disabilities Act (Title I), employers with 15 or more employees must provide reasonable accommodations for qualified employees whose mental health conditions constitute disabilities. The ADA Amendments Act of 2008 broadened the definition of disability substantially.
The OSHA General Duty Clause — Section 5(a)(1) of the OSH Act — requires employers to maintain a workplace free from recognized hazards likely to cause death or serious physical harm. OSHA has applied this to psychosocial risks including workplace violence and severe harassment, and its 2024 guidance explicitly references workplace stress.
The Mental Health Parity and Addiction Equity Act (MHPAEA) requires that mental health benefits in employer-sponsored health plans are no more restrictive than medical and surgical benefits. FMLA provides up to 12 weeks of job-protected leave for serious health conditions, including mental health conditions.
UK Framework
Section 2 of the Health and Safety at Work etc. Act 1974 requires employers to ensure, so far as reasonably practicable, the health, safety, and welfare of all employees — “health” explicitly includes psychological health. The Management of Health and Safety at Work Regulations 1999 require employers to assess all workplace risks, including psychosocial risks.
In 2024/25, 964,000 workers in Great Britain were suffering from work-related stress, depression, or anxiety — approximately 2,770 per 100,000 workers, more than double the rate when annual records began in 2001/02 (UK HSE, 2025). The HSE Management Standards provide the operational framework for assessing and managing the six key stressor areas.
EU Framework
Framework Directive 89/391/EEC imposes a general duty on employers across EU member states to assess and manage all workplace risks, including psychosocial risks. The practical gap is enforcement consistency — EU-OSHA’s ESENER 2024 survey found that only 39% of EU workplaces have an action plan to prevent work-related stress.
The European Trade Union Confederation adopted a resolution in October 2024 calling for a binding EU Directive on psychosocial risk prevention. While no directive has been adopted as of this writing, organizations operating in the EU should anticipate tightening regulatory requirements in this area.
Australia
Victoria’s Occupational Health and Safety (Psychological Health) Regulations 2025, which came into force on December 1, 2025, represent the most prescriptive psychosocial hazard regulations in any jurisdiction covered here. Employers must identify psychosocial hazards, eliminate associated risks or reduce them so far as reasonably practicable through a defined hierarchy of controls, and review controls regularly.
The Multi-Jurisdiction Approach
Organizations operating across jurisdictions face a practical choice: maintain separate policies for each territory or align with the most comprehensive framework and layer jurisdictional requirements on top. ISO 45003:2021 provides the most coherent global baseline for psychosocial risk management within an OHS management system. It is not certifiable independently but guides policy development, risk assessment, and continual improvement in a way that satisfies or exceeds most jurisdictional requirements.
How to Implement and Communicate the Policy Effectively
A policy exists on paper; implementation exists in behavior. The gap between the two is where most workplace mental health strategies fail — and the failure almost always occurs at the line-manager layer.
Organizations invest in policy text and EAP contracts but skip the training that would equip managers to have a supportive conversation when someone discloses distress. The result is managers who know the policy exists but default to awkward avoidance, premature referral to HR, or — worst case — treating the disclosure as a performance problem.
The data reinforces this gap. Only 11% of workplaces require mental health training, though more than half of those who receive it report increased comfort in discussing mental health (NAMI, 2025). Separately, 15% of working-age adults are estimated to have a mental disorder at any point in time (WHO, 2022). The workforce reality and the organizational preparedness are misaligned.
Effective implementation requires action across several dimensions:
- Manager training — equip line managers with specific skills: recognizing signs of distress, initiating supportive conversations, understanding referral pathways, and knowing the limits of their role (they are not counselors).
- Multi-channel communication — team briefings, induction programs, intranet, posters in break areas, leadership talks. A single email announcement reaches compliance; it does not build awareness.
- Integration into existing processes — embed mental health provisions into onboarding, performance reviews, risk assessments, and incident reporting. The policy should not sit as a standalone document disconnected from operational systems.
- Leadership modeling — senior leaders who speak about psychological safety, who take mental health days visibly, and who ask about wellbeing in operational reviews send a more powerful signal than any policy document.
- Anti-stigma action — Mental Health First Aid training, awareness campaigns, and — critically — consistent enforcement when discrimination or stigma occurs.
The return on investment for getting this right is well-documented. For every $1 spent on ordinary mental health concerns, employers see a $4 return in productivity gains (OSHA, 2024). The investment case is not theoretical — it is grounded in reduced absenteeism, lower presenteeism, and improved retention.
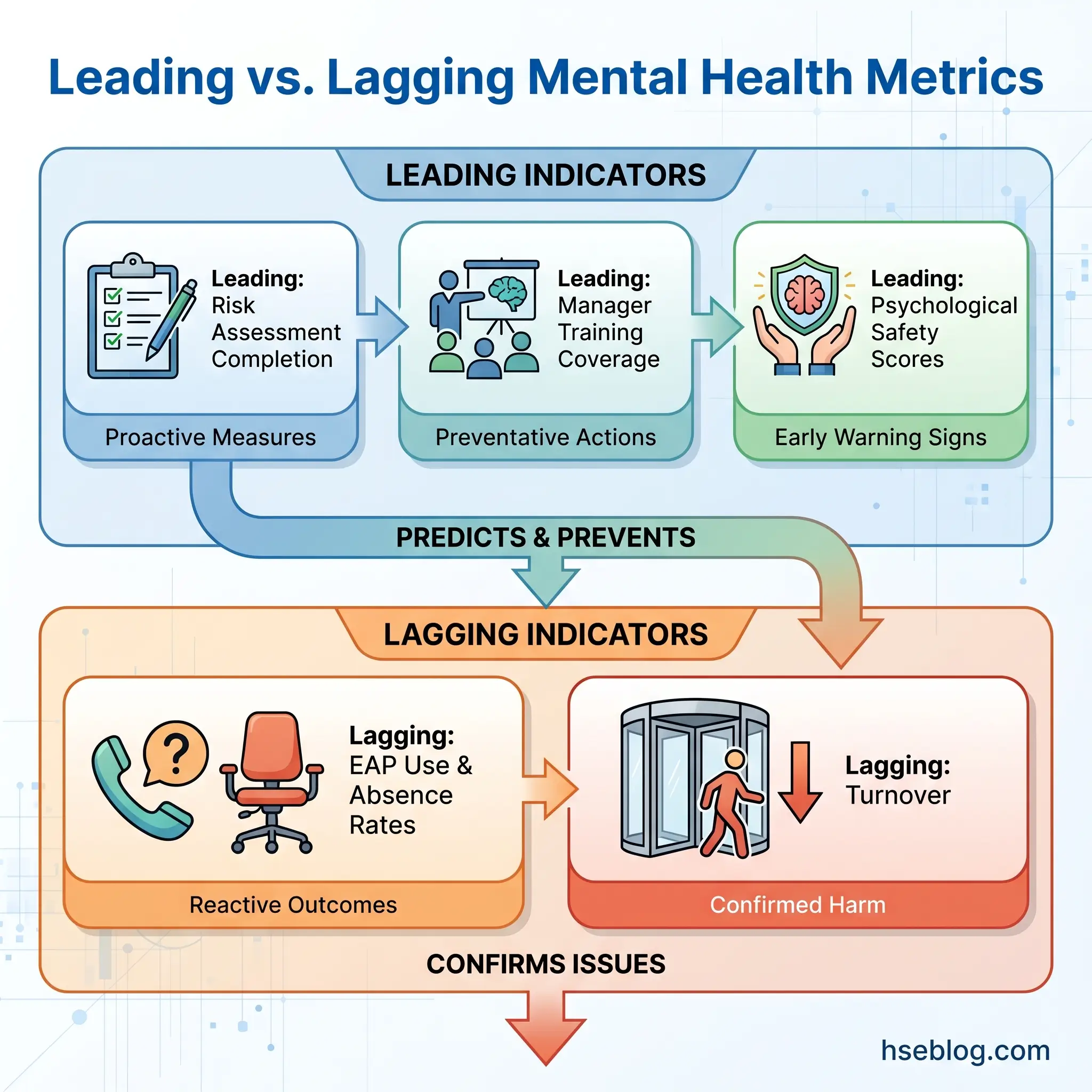
How to Monitor, Measure, and Review the Policy
The metric organizations most commonly track — EAP utilization — is actually a lagging indicator. It tells you how many people reached crisis point, not whether the policy is preventing harm. Leading indicators provide more actionable intelligence.
Quantitative Metrics
- Absence rates coded for stress, anxiety, or depression
- EAP utilization rates (lagging, but still necessary to track)
- Staff turnover — particularly in teams or departments with known psychosocial risk factors
- Grievance and complaint trends
- Presenteeism indicators — where measurable
Qualitative Metrics
- Employee survey data on perceived psychological safety
- Focus group feedback on policy awareness and accessibility
- Manager confidence assessments — do managers feel equipped to handle mental health conversations?
- Return-to-work experience feedback from employees who have used the policy’s provisions
Review Cycle
ISO 45003 requires continual improvement through monitoring and review. The policy itself should specify a minimum annual review, with triggered reviews following:
- Significant regulatory changes (such as the adoption of new psychosocial hazard regulations)
- Organizational restructuring, mergers, or major operational changes
- Critical incidents — including workplace suicides, clusters of mental-health-related absence, or formal complaints
- Monitoring data indicating the policy is not achieving its stated objectives
Benchmarking against external frameworks — the Thriving at Work standards in the UK or the WHO workplace mental health framework globally — provides additional structure for evaluating policy maturity.
Common Mistakes When Creating a Workplace Mental Health Policy
Every well-intentioned policy can fail in execution. The failure patterns below appear consistently across organizations of different sizes, sectors, and jurisdictions — and recognizing them early is more valuable than any template.
Treating the policy as an HR document rather than an organizational commitment. When the policy is “owned” by HR and invisible to senior leadership, it carries no operational weight. Managers treat it as optional guidance. Employees learn that it exists but has no teeth.
Copying a generic template without tailoring. A template designed for a US office-based employer does not address the psychosocial risks of a UK shift-work operation, a remote-first technology company, or a healthcare organization where staff face vicarious trauma. The risk assessment must precede the drafting, not the other way around.
Focusing exclusively on reactive support. EAP access, counseling benefits, and mental health days are necessary — but they address consequences, not causes. If the policy ignores workload design, management practices, and job control, it is treating symptoms while the organizational conditions that generate harm remain untouched.
Failing to consult employees. A policy developed entirely by HR and legal counsel addresses what management thinks matters. Employee consultation — required by ISO 45003 — surfaces the actual psychosocial stressors people experience daily.
Leaving confidentiality unclear. If employees are uncertain whether disclosing a mental health condition is safe — whether it will affect their career, be shared without consent, or appear in performance records — they will not use the policy’s provisions regardless of how comprehensive they are.
Writing the policy and never revisiting it. A policy without a review cycle, monitoring metrics, or accountability for outcomes becomes a static artifact. The organization changes; the policy does not.
The most insidious failure mode is what might be called the “performative policy” — a well-written document that satisfies every checklist but exists in an organizational culture where managers still penalize vulnerability, workloads remain unsustainable, and employees learn that the policy describes an aspiration rather than a reality. The policy must be accompanied by cultural and systemic change, or it risks becoming an exercise in institutional contradiction.
Frequently Asked Questions
Conclusion
The gap between having a mental health policy and having one that changes anything is almost entirely a question of organizational honesty. A policy built on genuine psychosocial risk assessment, clear stakeholder ownership, jurisdictional compliance, and measurable review commitments functions as an operational tool. A policy copied from a template, launched by email, and never revisited functions as a liability — it creates an expectation the organization has no mechanism to meet.
Every framework covered here — ISO 45003, the HSE Management Standards, the ADA, Victoria’s 2025 Regulations — converges on the same principle: psychological health is not separate from occupational health and safety. It belongs inside the management system, not beside it.
The question worth asking is direct. If an employee in your organization experienced a mental health crisis tomorrow, would the policy you have — or the one you are about to write — tell every person involved exactly what to do, who is responsible, and what protections apply? If the answer is uncertain, the work is not finished.