

TL;DR
- Early symptoms are the intervention window — tingling, morning stiffness, and post-shift aching are not “normal.” They signal the point where controls are cheapest and most effective.
- Physical and psychosocial risks interact — high workload pressure, low job control, and insufficient recovery time amplify biomechanical loading. Treating them as separate checklists underperforms.
- Engineering controls outperform training — adjustable workstations, mechanical aids, and tool redesign remove the exposure. Training alone cannot fix a workstation that forces 200 overhead reaches per shift.
- Assessment must capture the real task — evaluate what workers actually do, not what the SOP says. Floor-level lifts, improvised workarounds, and combination exposures are where injuries originate.
- Every major jurisdiction requires MSD risk management — through specific regulations or general duty provisions. “No ergonomics standard” does not mean “no legal obligation.”
Musculoskeletal disorders (MSDs) are injuries and conditions affecting muscles, tendons, nerves, joints, and spinal discs, caused or aggravated by work activities. They develop when physical risk factors — forceful exertions, repetitive motions, awkward postures, vibration, and static positions — combine with psychosocial stressors such as high workload and low job control, particularly when recovery time is insufficient.
Half a million workers in Great Britain alone were suffering from a work-related musculoskeletal disorder in 2024/25, costing 7.1 million working days (HSE, 2025). Across the Atlantic, US private industry recorded 937,620 MSD cases involving days away, restricted work, or job transfer in the 2023–2024 reporting period (Bureau of Labor Statistics / National Safety Council, 2026). These are not fringe statistics — musculoskeletal disorders are the single largest category of occupational ill health in virtually every industrialized economy, and they have been for decades.
What makes MSDs particularly stubborn is the gap between understanding and action. The risk factors are well established. The assessment tools are validated. The engineering solutions exist. Yet most organizations still default to stretching programs and manual handling training as their primary response — interventions that operate at the bottom of the control hierarchy while the biomechanical exposure remains unchanged. This article breaks down the causes of musculoskeletal disorders in the workplace, examines why physical and psychosocial risk factors must be treated as a connected system, walks through the hierarchy of controls with the specificity that generic guidance lacks, and maps the regulatory landscape across the US, UK, EU, and ISO frameworks so practitioners can build programs that are both effective and compliant.
What Are Musculoskeletal Disorders (MSDs)?
Musculoskeletal disorders encompass injuries and conditions affecting the body’s movement system — muscles, tendons, nerves, ligaments, joints, cartilage, blood vessels, and spinal discs. In occupational health, the term covers a spectrum from acute traumatic injuries (a torn rotator cuff from a single heavy lift) to gradual-onset conditions that develop over weeks, months, or years of cumulative loading.
Regulatory bodies differ on where they draw the boundary. NIOSH and EU-OSHA include both acute trauma and cumulative disorders under the MSD umbrella. Many national OHS agencies restrict the definition to gradual-onset conditions — the cumulative trauma disorders, repetitive strain injuries, and overuse syndromes that result from sustained exposure rather than a single event. Regardless of definitional scope, “MSD” has become the internationally preferred umbrella term, replacing older labels like repetitive strain injury (RSI) and cumulative trauma disorder (CTD).
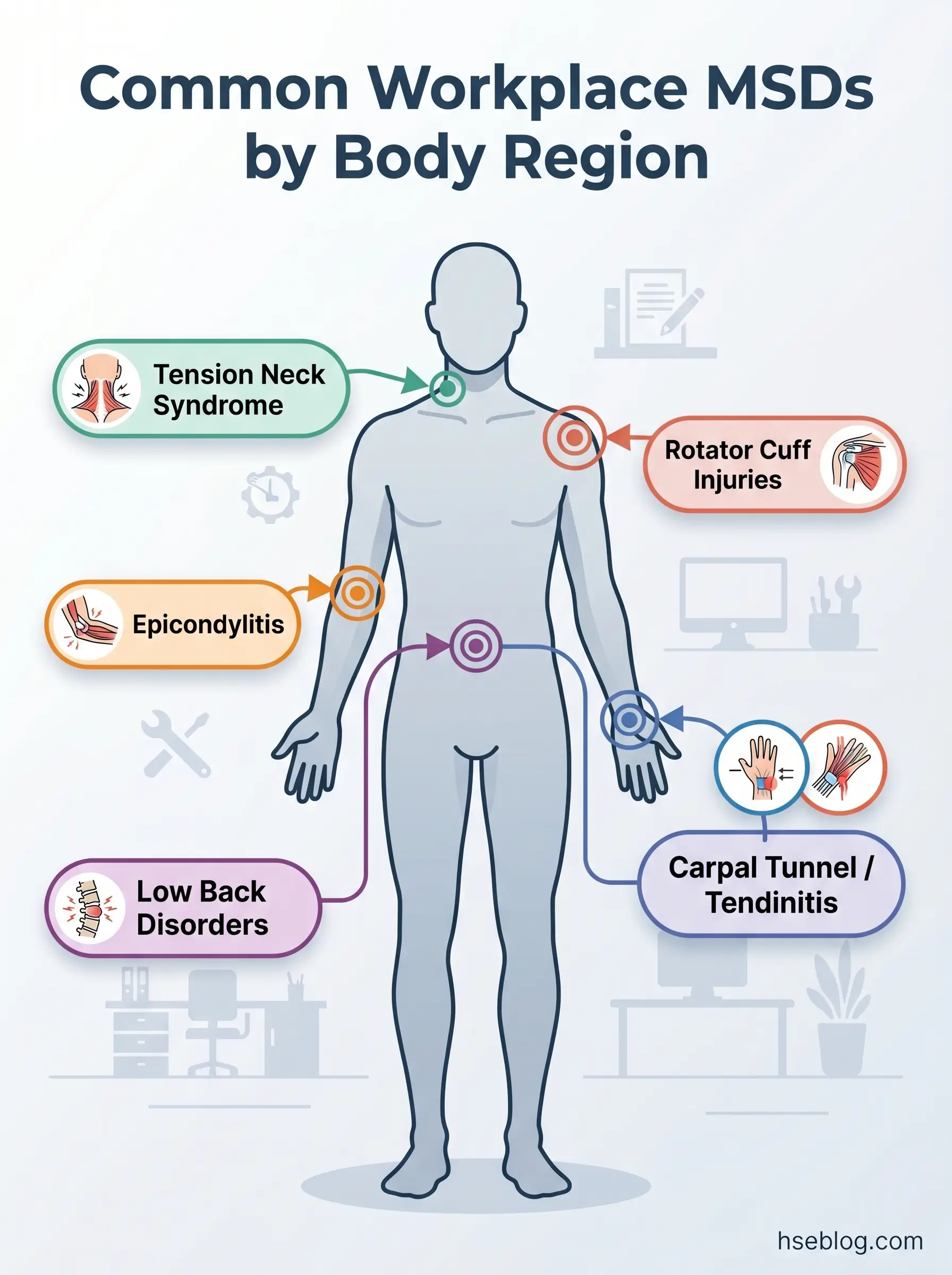
The common workplace MSDs that practitioners encounter most frequently include:
- Carpal tunnel syndrome — compression of the median nerve at the wrist, associated with repetitive hand/wrist movements, forceful gripping, and vibration exposure
- Tendinitis and tenosynovitis — inflammation of tendons or their sheaths, driven by repetitive motion and sustained force in the hands, wrists, elbows, or shoulders
- Rotator cuff injuries — damage to the shoulder’s stabilizing muscles and tendons, often from repeated overhead work or forceful arm movements
- Epicondylitis (tennis/golfer’s elbow) — overuse of forearm muscles causing pain at the elbow, common in assembly, construction, and tool-intensive work
- Low back disorders — disc degeneration, herniation, and chronic pain from manual lifting, whole-body vibration, prolonged sitting, or awkward trunk postures
- Tension neck syndrome — chronic neck and upper shoulder pain from sustained static postures, particularly in display screen equipment (DSE) work
These conditions range from temporary discomfort resolved by workstation adjustment to chronic disability requiring career change. The critical point that gets lost in clinical classification: early-stage symptoms — tingling fingers, morning stiffness, mild aching that clears on rest days — are not “normal wear and tear.” They are the biological warning system signaling that tissue loading has exceeded recovery capacity. That early stage is where intervention is cheapest, least disruptive, and most effective. By the time a worker presents with established carpal tunnel or a herniated disc, the cost of intervention has multiplied and the prognosis has worsened.
How Significant Are MSDs in the Workplace?
The scale of the MSD burden is difficult to overstate — and consistently underestimated by organizations that rely on workers’ compensation data alone.
In the United States, the BLS and National Safety Council reported 937,620 MSD cases involving days away from work, restricted duty, or job transfer (DART cases) in US private industry across the 2023–2024 reporting period, including 484,620 cases involving days away from work (National Safety Council / BLS, 2026). In Great Britain, an estimated 511,000 workers were suffering from a work-related MSD in 2024/25, with a prevalence rate of 1,470 per 100,000 workers (HSE, 2025). Those conditions consumed 7.1 million working days — averaging 14 days lost per affected worker (HSE, 2025). Notably, 173,000 of those were new cases, an increase from 168,000 the previous year, signaling that prevention progress has stalled at pre-pandemic levels despite decades of available guidance (HSE, 2025). Across the European Union, approximately three in five workers report MSD complaints (EU-OSHA / Eurofound, European Working Conditions Survey).
The financial dimension compounds the human one. US employers pay an estimated $15–20 billion annually in direct workers’ compensation costs for MSDs, with total costs including indirect expenses reaching an estimated $13–54 billion range (OSHA/NIOSH estimates, 1999–2023). These figures carry a data-vintage caveat — no single verified up-to-date figure exists from a Tier 1 source — but the order of magnitude is consistent: billions annually in a single jurisdiction.
The sectors that carry the heaviest MSD burden are healthcare and social assistance, transportation and warehousing, construction, manufacturing, and agriculture. But the risk is not confined to manual labor — office-based MSDs from prolonged static sitting and display screen work account for a substantial share of upper limb and neck conditions, and the shift to remote and hybrid working has created a new population of workers in uncontrolled home workstation environments.
Watch For: The numbers above capture reported cases. The pattern practitioners consistently observe is that MSD costs are systematically underestimated because most tracking misses presenteeism — workers who show up symptomatic but at reduced capacity — informal task-swapping between colleagues to avoid painful duties, and the recruitment and retraining costs when experienced workers leave roles they can no longer physically sustain. The visible injury data is the tip of the iceberg.
What Causes Musculoskeletal Disorders at Work?
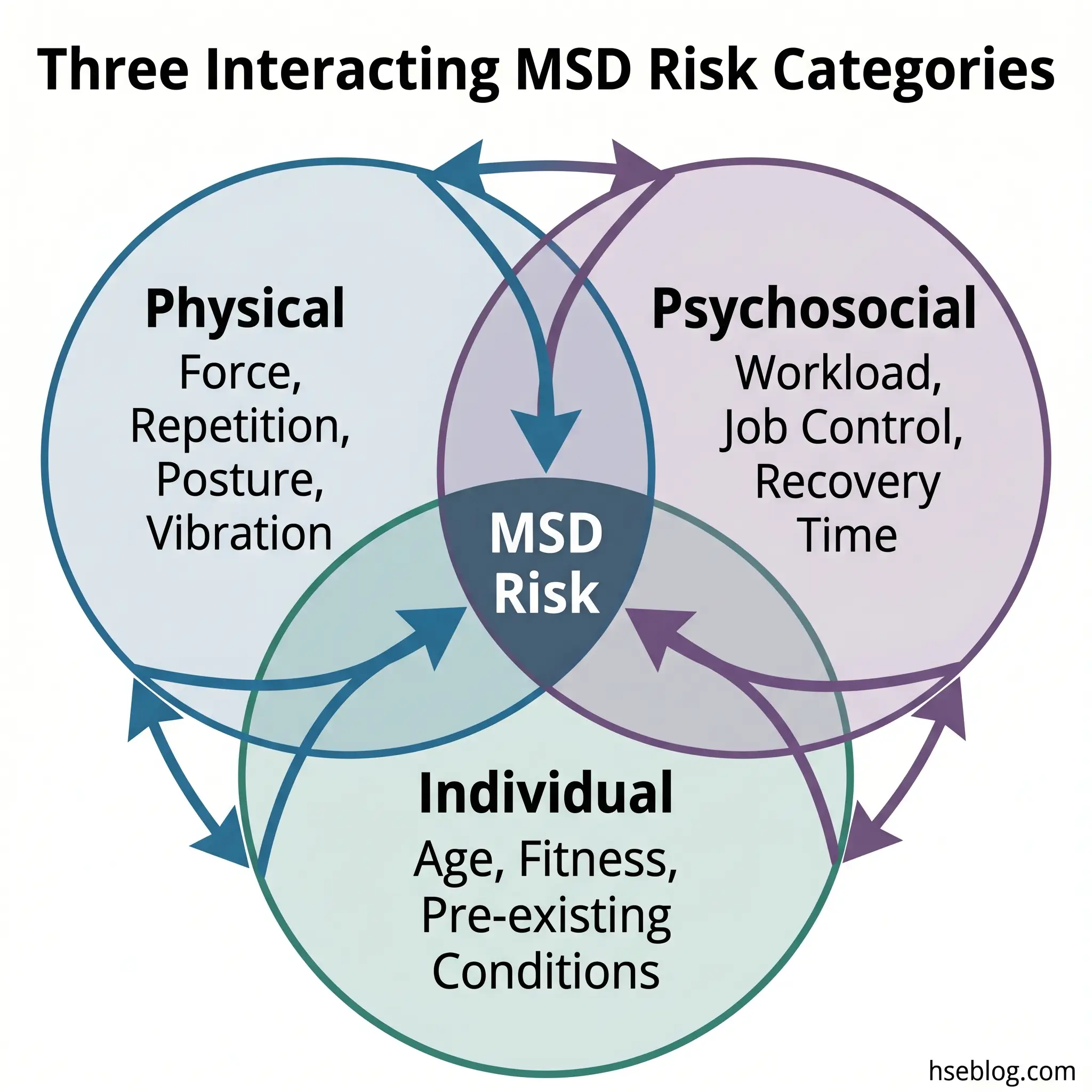
MSD causation is rarely a single-factor problem. The current evidence base, reflected in both EU-OSHA research programs and NIOSH guidance, identifies three interacting categories of risk factors: physical/biomechanical, psychosocial/organizational, and individual. What matters most is the interaction between these categories — a task that is biomechanically moderate can become high-risk when workers have no control over pacing, no ability to take micro-breaks, and high production pressure. That interaction effect is where most risk assessments fail.
The dose-response relationship governs all physical risk factors. Intensity, frequency, and duration of exposure, combined with insufficient recovery time, determine whether ordinary movement becomes pathological tissue loading. A single heavy lift rarely causes a chronic MSD. The same lift performed 80 times per shift, at floor level, with a twisted trunk, six days per week — that is the loading pattern that produces injury.
Physical and Biomechanical Risk Factors
Each physical risk factor operates through a specific mechanism of tissue damage.
- Forceful exertions — heavy lifting, pushing, pulling, gripping, and pinching generate mechanical stress that can exceed the tensile strength of muscles, tendons, and ligaments. When force demands exceed tissue capacity repeatedly, micro-tears accumulate faster than the body repairs them.
- Repetitive motions — high-frequency movements, particularly of the hands, wrists, and arms, impair tendon lubrication (the synovial fluid mechanism) and create friction-based inflammation. Assembly line work, keyboard use, and packaging tasks are classic exposures.
- Awkward postures — working with joints near their range-of-motion limits (overhead reaching, deep squatting, sustained wrist deviation) places disproportionate load on supporting structures. The further from neutral posture, the higher the biomechanical stress for any given force.
- Static postures — sustained positions without movement, including prolonged sitting, restrict blood flow and impair the clearance of metabolic waste products from muscle tissue. Paradoxically, not moving is as damaging as moving too much.
- Vibration — hand-arm vibration from power tools damages small blood vessels and nerves (vibration white finger, carpal tunnel). Whole-body vibration from vehicles and heavy equipment contributes to spinal disc degeneration.
- Contact stress — localized pressure from tool edges, hard work surfaces, or equipment pressing against soft tissue can compress nerves and restrict blood flow.
Psychosocial and Organisational Risk Factors
A persistent misconception in MSD risk management treats psychosocial factors as secondary — background noise that might make workers complain more but doesn’t actually cause tissue damage. The evidence says otherwise. Research published in BMC Musculoskeletal Disorders (Macdonald, 2015) and multiple EU-OSHA research projects has established that psychosocial factors are independent risk factors for MSDs, not merely confounders or amplifiers.
The mechanisms are specific and measurable. Psychological stress increases baseline muscle tension — even without physical exertion, stressed workers show elevated electromyographic activity in the trapezius and forearm muscles. That elevated tension means every physical task starts from a higher loading baseline. High workload demand with low control reduces the micro-pauses that workers naturally take when self-paced — pauses that allow metabolic recovery in loaded tissues. Poor social support and job insecurity suppress early symptom reporting, pushing workers past the early-intervention window into established injury. Monotonous, externally paced work eliminates the task variation that distributes loading across different body regions.
The practical implication is direct: MSD prevention programs that focus exclusively on physical hazards while ignoring work organization, pace control, and psychosocial conditions will systematically underperform. The biomechanical intervention may be technically correct, but it cannot compensate for the loading amplification that psychosocial exposure creates.
Individual and Lifestyle Factors
Age, body mass index, physical fitness, pre-existing conditions, and non-work physical activities all modify how an individual responds to workplace exposures. An older worker with pre-existing disc degeneration will reach the injury threshold sooner under identical loading conditions than a younger worker without that history.
These factors are real and relevant to risk assessment — but they carry a critical legal and ethical boundary. Individual susceptibility does not reduce the employer’s duty to control workplace risk. Under the UK’s Manual Handling Operations Regulations 1992 and the EU Framework Directive 89/391/EEC, the obligation is to assess and reduce risk at source, accounting for the range of workers who will perform the task — including those who are older, smaller, less fit, or returning from injury. Using individual factors to argue that “the task is fine, the worker is the problem” is both legally indefensible and factually wrong.
How to Assess MSD Risk in the Workplace
Risk assessment for MSDs follows the same fundamental logic as any workplace risk assessment — identify the hazards, evaluate the risk, implement controls, and review. But the execution demands specific tools because MSD risk factors are continuous variables (force, frequency, duration, posture angle) rather than binary present/absent conditions.
The starting point is structured observation combined with worker consultation. Walk the task. Watch the actual work being performed, not the written procedure. Ask workers where they feel discomfort, which tasks they dread, and which workarounds they’ve invented. Incident data from OSHA 300 logs, first-aid records, and health surveillance results identify the tasks and departments that are already producing injuries — the reactive data that points to where proactive assessment is most urgent.
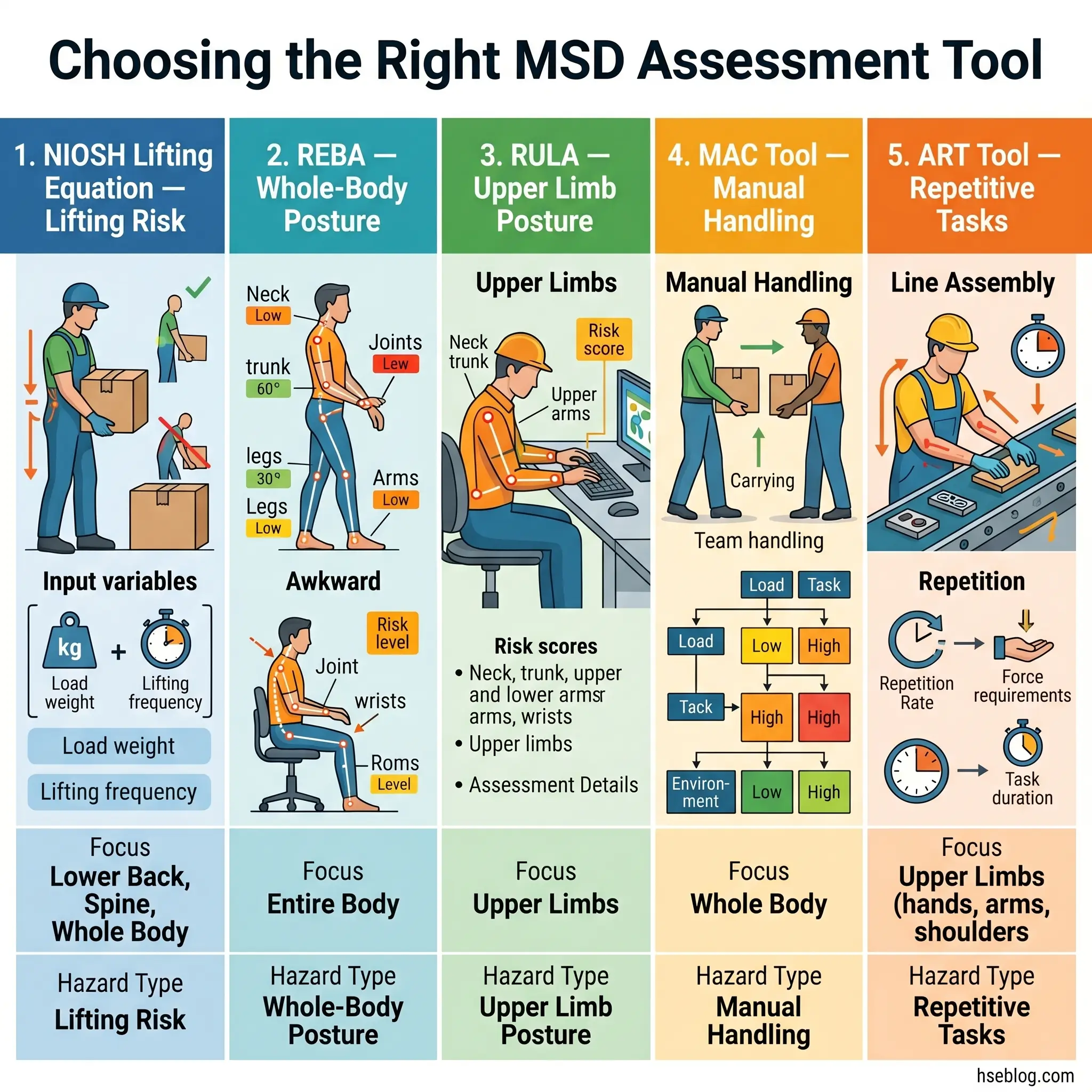
Several validated assessment tools exist, each designed for specific exposure types. The choice of tool should match the dominant risk factor in the task being assessed.
| Assessment Tool | Target Hazard | Body Region | Complexity | Origin |
|---|---|---|---|---|
| NIOSH Revised Lifting Equation | Manual lifting / lowering | Low back | Moderate — requires measurement of task variables | US (NIOSH) |
| REBA (Rapid Entire Body Assessment) | Whole-body posture | Full body | Low-moderate — observational scoring | UK |
| RULA (Rapid Upper Limb Assessment) | Upper limb posture and force | Neck, trunk, upper limbs | Low-moderate — observational scoring | UK |
| Strain Index | Repetitive upper extremity tasks | Hand, wrist, forearm | Moderate — requires intensity and duration estimates | US |
| MAC Tool (Manual Handling Assessment Charts) | Manual handling (lift, carry, team handling) | Full body | Low — color-coded risk bands | UK (HSE) |
| ART Tool (Assessment of Repetitive Tasks) | Repetitive work | Upper limbs | Low-moderate — structured guide | UK (HSE) |
The NIOSH Revised Lifting Equation deserves particular mention. It calculates a recommended weight limit (RWL) for a manual lifting task based on six multipliers — horizontal distance, vertical position, asymmetry angle, lifting frequency, hand-coupling quality, and task duration. When the actual load exceeds the RWL, the Lifting Index (actual load ÷ RWL) quantifies how far the task deviates from acceptable risk. The method is referenced in ISO 11228-1:2021 and remains the most widely validated lifting risk assessment in occupational ergonomics.
Audit Point: MSD risk assessments commonly fail in two specific ways. First, they assess the designed task rather than the performed task — the SOP says lift from waist height, but the real pallet position forces lifting from floor level with a twisted trunk. Second, they assess individual risk factors in isolation rather than in combination, missing the multiplicative effect of force combined with awkward posture combined with high repetition happening simultaneously in the same task cycle. An assessment that scores force as “moderate” and posture as “moderate” separately may miss a combined exposure that is actually high-risk.
When assessment results identify high-risk tasks, or when the organization lacks in-house ergonomics expertise, involving a qualified ergonomist or occupational health professional is not optional — it is the point where competent-person requirements under the Management of Health and Safety at Work Regulations 1999 (UK) and equivalent frameworks become directly applicable.
Workplace Controls for Musculoskeletal Disorders
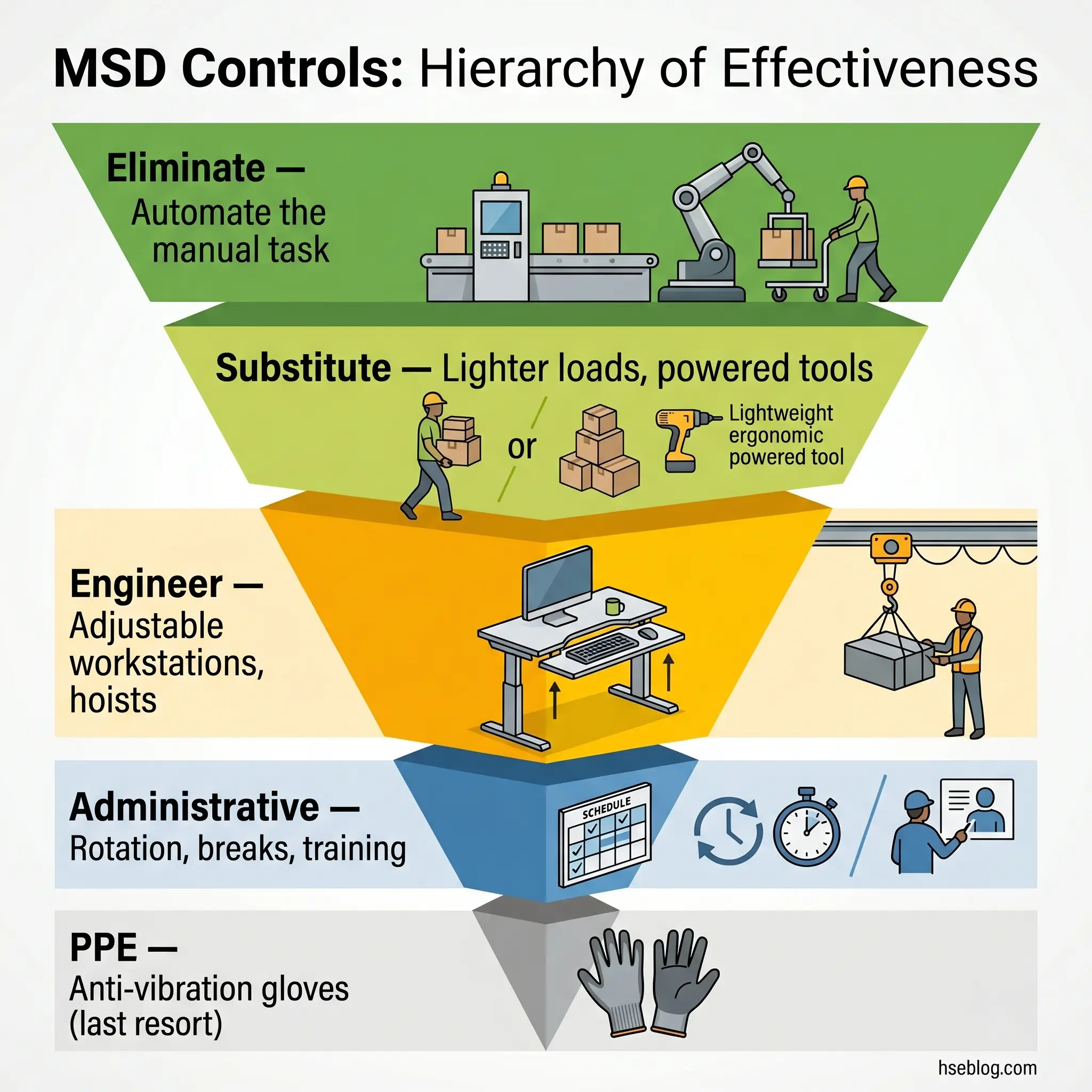
The hierarchy of controls applies to MSDs with the same logic it applies to any workplace hazard — but with a specific failure mode that practitioners need to recognize. The persistent pattern across industries is over-reliance on administrative controls (training, stretching programs, job rotation) while leaving the engineering problem unaddressed. Training a worker to “lift correctly” does not fix a workstation that forces reaching above shoulder height 200 times per shift. The hierarchy exists precisely because upstream controls remove the exposure, while downstream controls only manage the worker’s time within it.
Elimination sits at the top. Can the hazardous manual task be removed entirely? Automation of repetitive handling, gravity-fed delivery systems that eliminate manual lifting from receipt to workstation, and process redesign that removes the need for the task altogether. Elimination is underused because it requires capital investment and process re-engineering — but it is the only control level that reduces MSD risk to zero for that specific exposure.
Substitution replaces the hazardous element with something less harmful. Lighter packaging that reduces the per-unit load. Powered tools replacing manual ones, cutting the force demand. Smaller containers that bring weights within acceptable limits. Substitution rarely eliminates the risk entirely but can bring exposure below the injury threshold.
Engineering Controls for MSDs
This is where the most impactful interventions live — and where competitive guidance is thinnest. Engineering controls redesign the work environment, equipment, or tools to reduce biomechanical exposure at source.
Workstation design is the foundation. The governing principle is adjustability — the workstation adapts to the worker, not the reverse. Adjustable-height work surfaces that keep task height in the power zone (between knuckle and shoulder height). Tilting fixtures that bring the work piece to the optimal angle. Monitor arms and keyboard trays positioned to maintain neutral neck and wrist posture. Sit-stand options that alternate between positions throughout the shift.
Mechanical aids address the force dimension. Lift tables and scissor lifts that raise loads to working height. Vacuum lifters for sheet materials. Hoists and jib cranes for repetitive overhead transfers. Conveyor systems that eliminate manual carrying between workstations. The judgment call with mechanical aids is selecting equipment that workers will actually use — a hoist that takes 90 seconds to rig for a 5-second lift will be bypassed. Effective engineering controls must be faster or comparable in time to the manual method they replace.
Tool design matters at the hand-interface level. Grip diameter matched to hand anthropometry (too large or too small both increase grip force demand). Vibration-damped power tools that reduce hand-arm vibration exposure below the action values set by Directive 2002/44/EC (hand-arm: 2.5 m/s² daily exposure action value). Balanced tool suspension systems that eliminate the need to support tool weight.
Industrial exoskeletons represent an emerging engineering support — passive devices that offload shoulder or back muscles during overhead or lifting tasks. Current evidence shows modest reduction in muscle activation, but adoption barriers around worker acceptance, fit variability, and the risk that exoskeletons mask rather than eliminate the underlying hazard make them a supplementary measure, not a primary control.
Administrative Controls and Work Organization
Administrative controls reduce exposure duration and distribute loading — but they require careful design to deliver actual biomechanical benefit.
Job rotation is the most frequently cited administrative control for MSDs, and the most frequently implemented badly. Rotation only prevents MSDs if it moves workers between tasks that load different body regions through different movement patterns. Rotating between three tasks that all involve shoulder-height reaching provides no meaningful recovery for the shoulder complex — the worker simply performs the same biomechanical exposure at three different workstations. Effective rotation schemes must be designed from the risk assessment data, matching tasks by their loading profile, not by department convenience.
Work-rest scheduling provides the recovery periods that prevent cumulative damage from exceeding repair capacity. The evidence on break frequency versus duration consistently favors more frequent shorter breaks over fewer longer ones — five minutes every hour outperforms fifteen minutes every three hours for sustained repetitive or static work. Micro-breaks of 20–30 seconds between task cycles, where workers actively move through the opposite range of motion, are the most cost-effective administrative intervention available.
Pace-of-work control directly addresses one of the strongest psychosocial-physical interaction mechanisms. When workers control their own speed, they naturally insert the micro-pauses that prevent continuous loading. When pace is externally determined — conveyor speed, machine cycle, call queue — those natural recovery periods disappear.
Early symptom reporting programs require two conditions to function: workers must know what to report (specific symptoms, not just “injury”), and reporting must be genuinely non-punitive. Any system that results in disciplinary action, loss of bonus, or social pressure against reporting will suppress exactly the early-stage data that makes proactive intervention possible.
Ergonomics training occupies the bottom of the administrative tier, and its limitations should be honestly stated. Training can improve awareness of risk factors and correct specific technique errors. It cannot compensate for hazardous workstation design, excessive production targets, or inadequate equipment. Organizations that invest heavily in training while deferring engineering controls are, in operational terms, asking workers to protect themselves from hazards the employer should have eliminated.
The Fix That Works: Match the control to the risk factor. If the assessment identifies excessive force, the answer is mechanical assistance or load reduction — not a training video on lifting technique. If the assessment identifies repetitive motion, the answer is task redesign or automation — not a stretching poster. If the assessment identifies static posture, the answer is workstation adjustability and break scheduling — not a reminder to sit up straight. The hierarchy of controls is a diagnostic tool, not a menu to pick from based on budget.
Building an Effective Workplace Ergonomics Program
Individual controls address individual tasks. A program addresses the system that produces MSD risk across the organization. The elements that OSHA, HSE UK, and ISO guidance converge on are not accidental — they reflect decades of evidence about what distinguishes organizations that reduce MSD incidence from those that don’t.
Management leadership and resource commitment is the precondition, not a platitude. An ergonomics program without budget authority to modify workstations, purchase equipment, or adjust staffing levels is a documentation exercise. Leadership commitment manifests in approved capital for engineering controls, in production targets that account for rest breaks, and in supervisors who are evaluated on ergonomic compliance rather than output alone.
Worker participation is not optional consultation — it is the primary source of information about actual task demands. Workers know which workarounds they’ve invented, which tools they’ve modified, which tasks they rotate away from, and which symptoms they’re managing silently. Formal mechanisms — ergonomics committees, discomfort surveys, hazard-reporting channels — create structured pathways for this knowledge to reach decision-makers.
Systematic job hazard analysis and MSD risk assessment using the validated tools described above, applied to tasks as performed rather than tasks as designed. Priority should follow injury data, discomfort survey results, and sector-specific risk profiles.
Health surveillance and early reporting mechanisms capture the leading indicators. Discomfort surveys administered quarterly can detect rising symptom trends in a work group months before the first lost-time injury. Occupational health referral pathways give symptomatic workers access to assessment before conditions become chronic. These systems require occupational health professional oversight — they are not DIY projects.
Training — for workers, supervisors, and managers — tailored to role. Workers need symptom recognition and reporting procedures. Supervisors need the ability to identify task-level risk factors and escalate. Managers need to understand the business case and the regulatory duty.
Program evaluation and continuous improvement closes the loop. Track both lagging indicators (MSD incidence, severity, workers’ compensation costs) and leading indicators (discomfort survey trends, hazard report volumes, assessment completion rates, control implementation timelines). Programs that measure only lagging indicators are permanently reactive. The leading indicators — rising discomfort scores, increased use of pain medication within a work group, informal task-swapping, or growing overtime in physically demanding roles — predict future MSD problems before they become injury statistics.
Regulatory Framework for MSD Prevention
The regulatory landscape for MSDs differs in structure across jurisdictions but converges on a single obligation: employers must assess and control MSD risk, using a hierarchy that prefers eliminating the hazard over managing the worker.
In the United States, there is no standalone OSHA ergonomics standard. The Ergonomics Program Standard finalized in 2000 was repealed under the Congressional Review Act in 2001 — one of the only workplace safety rules ever nullified through that mechanism. Enforcement relies on the General Duty Clause, Section 5(a)(1) of the OSH Act, which requires employers to provide employment free from recognized hazards likely to cause death or serious physical harm. OSHA has successfully cited employers for ergonomic hazards causing MSDs under this provision, though the burden of proof is higher than under a specific standard. OSHA also publishes industry-specific ergonomics guidelines (healthcare, grocery, meatpacking) and requires MSD case recording on OSHA 300 logs under the recordkeeping standard. The 2023 revision of the BLS Occupational Injury and Illness Classification System (OIICS) has changed how MSD events are categorized starting with the 2023 data year, creating a data-series break that will affect trend comparisons going forward (BLS, 2026).
In the United Kingdom, the regulatory framework is more prescriptive. The Manual Handling Operations Regulations 1992 (amended 2002) require employers to avoid hazardous manual handling so far as is reasonably practicable, and where avoidance is not possible, to assess the risk and reduce it to the lowest level reasonably practicable. The Health and Safety (Display Screen Equipment) Regulations 1992 cover workstation ergonomics for DSE users. The Control of Vibration at Work Regulations 2005 implement the EU Vibration Directive, setting exposure action values and limit values for hand-arm and whole-body vibration and requiring health surveillance for exposed workers. The Management of Health and Safety at Work Regulations 1999 underpin all of these with the general duty to conduct suitable and sufficient risk assessment. HSE’s MSD guidance pages provide assessment tools (MAC, ART, RAPP) and practical interpretation.
The European Union framework operates through Directives transposed into member-state law. The Framework Directive 89/391/EEC establishes the general obligation to assess and control workplace risks. Three sector-specific Directives target MSD risk directly: the Manual Handling Directive 90/269/EEC requires employers to use organizational measures or mechanical equipment to avoid hazardous manual handling; the Display Screen Equipment Directive 90/270/EEC requires workstation assessment, minimum ergonomic standards, and breaks or activity changes for DSE work; and the Physical Agents (Vibration) Directive 2002/44/EC sets daily exposure action values (hand-arm: 2.5 m/s², whole-body: 0.5 m/s²) and exposure limit values (hand-arm: 5 m/s², whole-body: 1.15 m/s²).
At the international level, the ISO 11228 series provides global benchmark guidance. Part 1 (revised 2021) covers lifting, lowering, and carrying, proposing reference values of 25 kg for men and 15 kg for women under ideal conditions and referencing the NIOSH Revised Lifting Equation methodology. Part 2 addresses pushing and pulling. Part 3 covers low-load high-frequency handling. ISO 6385 establishes ergonomic principles in the design of work systems.
Jurisdiction Note: For manual lifting limits, different standards cite different reference values. NIOSH recommends 23 kg under ideal conditions. ISO 11228-1 specifies 25 kg for men and 15 kg for women. HSE UK guidance tables provide zone-based values varying by lift height and reach distance. These reflect different assessment methodologies and population assumptions, not contradictory science. The practitioner’s decision should apply the most conservative limit applicable to their specific worker population and task conditions.
A common compliance trap is treating regulatory minimums as the performance target. The Manual Handling Regulations require risk assessment and reduction “so far as is reasonably practicable” — practitioners who stop at a basic assessment checklist often miss the combination-effect risks that the regulations implicitly require them to address. Compliance and effectiveness are not interchangeable.
Emerging Trends in MSD Prevention
Several developments are reshaping how organizations identify and control MSD risk, though each comes with limitations that practitioners should evaluate critically.
Wearable sensor technology and AI-powered biomechanical analysis are moving MSD risk assessment from periodic observational snapshots to continuous exposure monitoring. Inertial measurement units worn on the trunk, arms, or wrists capture real-time posture data, force estimates, and repetition counts across entire shifts. Machine learning algorithms flag high-risk movement patterns and generate exposure profiles that would take an ergonomist weeks to compile manually. The value is clear — capturing the variability and cumulative loading that observational tools miss. The limitation is equally clear: sensor data still requires competent interpretation, and the technology captures biomechanical exposure without addressing the psychosocial and organizational factors that amplify it.
Industrial exoskeletons — both passive spring-loaded devices and powered assist systems — have moved from laboratory prototypes to pilot deployments in automotive manufacturing, logistics, and construction. Current evidence shows measurable reductions in muscle activation for specific tasks, particularly overhead work and static forward-bending. But adoption barriers are real: fit variability across body types, worker acceptance and comfort over full shifts, maintenance requirements, and the risk that exoskeletons reduce perceived effort without actually eliminating the hazardous loading pattern. The practitioner’s role is to evaluate whether a specific device genuinely reduces exposure for a specific task and worker population — not to adopt the technology as a generic solution.
Integration of psychosocial hazard management into MSD programs reflects the growing evidence base that physical-only approaches systematically underperform. The systems approach advocated by current EU-OSHA research treats work organization, pace control, recovery scheduling, and psychosocial climate as integral components of MSD prevention — not separate wellbeing initiatives. Organizations that have adopted this integrated model report better outcomes than those running parallel physical-ergonomics and mental-health programs with no connection between them.
Remote and hybrid work has created a new MSD risk population. Workers who previously used employer-provided, ergonomically assessed workstations now spend significant hours at kitchen tables, couches, and improvised desk setups with no adjustment, no external monitor, and no structured break patterns. Display Screen Equipment regulations (UK, EU) technically apply to home workstations used regularly, but enforcement and assessment present practical challenges that most organizations have not resolved.

Frequently Asked Questions
Conclusion
The single highest-impact shift most organizations can make in MSD prevention is moving investment from the bottom of the hierarchy of controls to the top. The evidence base is unambiguous: engineering controls that redesign workstations, introduce mechanical aids, and eliminate hazardous loading patterns produce sustained reductions in MSD incidence. Administrative controls — training, rotation, stretching programs — have a role, but only as supplements to engineering solutions that address the exposure at source. When training becomes the primary control, the organization is asking workers to manage a hazard the employer should have engineered out.
The second shift, less visible but equally consequential, is integrating psychosocial risk management into the MSD prevention framework. Physical risk factors and psychosocial stressors do not operate in parallel — they interact. High production pressure compresses recovery time. Low job control eliminates the micro-pauses that prevent cumulative loading. Poor reporting culture pushes workers past the early-intervention window where outcomes are best. Organizations that run separate ergonomics and wellbeing programs with no connection between them are managing half the problem.
The data tells a consistent story across jurisdictions: 511,000 affected workers in Great Britain (HSE, 2025), 937,620 DART cases in US private industry (BLS/NSC, 2026), three in five European workers reporting MSD complaints (EU-OSHA/Eurofound). These numbers have not improved in proportion to the knowledge available. The assessment tools are validated, the engineering solutions exist, the regulatory duties are clear. What remains is the organizational decision to act on all of it — upstream, integrated, and sustained.