

TL;DR — Three Questions That Frame This Discipline
What is occupational hygiene? The science and practice of anticipating, recognizing, evaluating, controlling, and confirming workplace hazards that cause disease or impaired wellbeing — focused on the work environment, not the worker’s medical status.
Why does it matter? Work-related diseases kill approximately 1.9 million people globally each year (WHO/ILO, 2021) — far exceeding workplace injury fatalities. Most of these deaths are preventable through competent exposure assessment and control.
What’s the most dangerous misconception? That measuring below a legal exposure limit means workers are safe. Occupational exposure limits protect most workers, not all — and in many jurisdictions, the legal limits are decades out of date.
Occupational hygiene is the science and practice of anticipating, recognizing, evaluating, controlling, and confirming workplace hazards that can cause illness or impaired wellbeing. Also called industrial hygiene in the US, it focuses on preventing work-related disease — from chemical exposure to noise, ergonomic strain, and psychosocial stress — through measurement, control, and professional judgment.
What Is Occupational Hygiene? A Working Definition
Globally, approximately 1.9 million deaths each year are attributable to work-related factors (WHO/ILO Joint Estimates, 2021). The vast majority of those deaths come not from the incidents that make headlines — collapses, explosions, falls — but from disease. Cancers linked to chemical exposure. Cardiovascular disease driven by long working hours. Respiratory conditions from years of inhaling dust no one measured. Occupational hygiene exists because those deaths are preventable, and prevention starts with understanding what workers are actually exposed to.
The discipline carries different names depending on geography — “occupational hygiene” in the UK, EU, Australia, Canada, and most international contexts; “industrial hygiene” in the United States — but it is the same field. The International Occupational Hygiene Association (IOHA), the American Industrial Hygiene Association (AIHA), and the British Occupational Hygiene Society (BOHS) all define it as the science and art devoted to the anticipation, recognition, evaluation, control, and confirmation of workplace hazards capable of causing illness, impaired wellbeing, or significant discomfort. OSHA’s industrial hygiene training guide uses functionally identical language. The “science and art” phrasing matters: measurement gives the science, but professional judgment — deciding which exposures to prioritize, how to interpret variable data, which controls are reasonably practicable — is where the art operates.
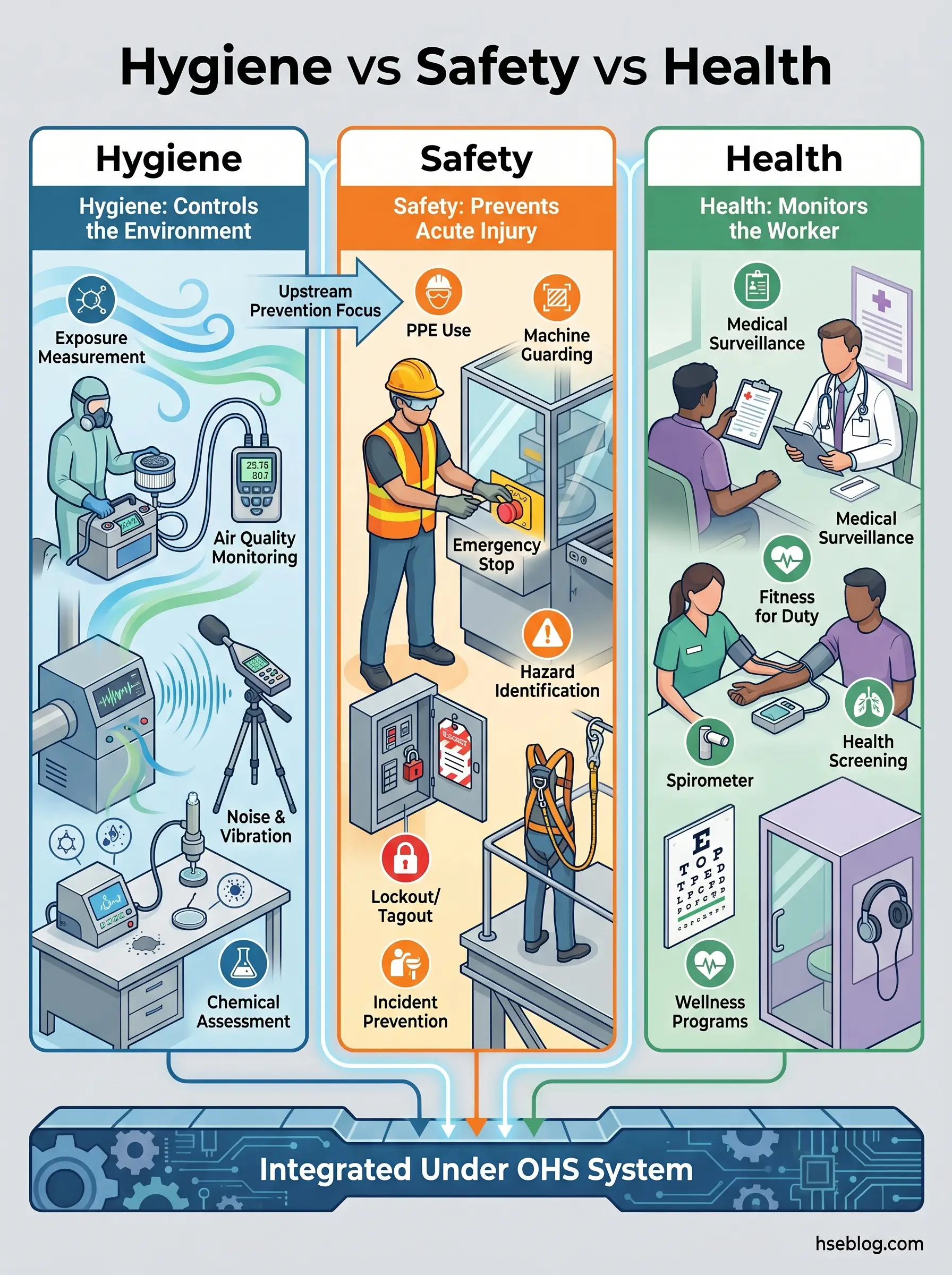
A critical distinction that organizations routinely miss: occupational hygiene is not occupational safety, and it is not occupational health. Safety addresses acute injury risk. Occupational health monitors workers for signs of harm through medical surveillance. Hygiene works upstream of both — measuring and controlling the environment before it damages the worker. Programs that treat these as interchangeable consistently develop blind spots. A safety-heavy program may have excellent incident rates while silica exposures go unmeasured for years. A health-surveillance program may detect early hearing loss without anyone investigating the noise source generating it.
Watch For: Organizations that claim their “occupational hygiene program” consists entirely of annual noise surveys and a chemical inventory spreadsheet. If no one is conducting personal exposure assessments, interpreting data against occupational exposure limits, and verifying that controls actually reduce exposure — what’s operating is a filing system, not a hygiene program.
Why Occupational Hygiene Matters: The Global Burden of Work-Related Disease
The scale of work-related disease is difficult to grasp precisely because it operates on a delay. A worker exposed to respirable crystalline silica today may not develop silicosis for 10–20 years. An employee working 55+ hours per week may suffer a stroke a decade later. This latency decouples cause from consequence in a way that workplace injuries do not — and it systematically suppresses the urgency organizations feel about hygiene.
The numbers, when aggregated, are stark. The WHO/ILO Joint Estimates (2021) attributed approximately 1.9 million deaths globally to occupational factors in their 2016 reference-year analysis. Of these, long working hours alone accounted for an estimated 745,000 deaths from ischemic heart disease and stroke (WHO/ILO, 2021) — the single largest burden from any occupational risk factor studied. A more recent analysis by Takala et al. in the Scandinavian Journal of Work, Environment & Health (2024) estimated 2.9 million work-related deaths globally in 2019, of which 2.58 million were from work-related diseases and only 0.32 million from occupational injuries.
In Great Britain alone, the Health and Safety Executive estimates approximately 13,000 deaths each year linked to past occupational exposures to chemicals and dusts (HSE, annual statistics). These are not historical artifacts — they reflect exposures that occurred in workplaces operating under regulatory frameworks that were, at the time, considered adequate.
The pattern that practitioners observe across published burden-of-disease data is consistent: organizations measure current incident rates, see low numbers, and conclude their hygiene program is working. But the consequences of today’s exposures will not surface until the 2030s and 2040s. Current injury statistics tell you nothing about whether your current exposure controls are protecting workers from chronic disease.
The Core Principles of Occupational Hygiene: The ARECC Framework
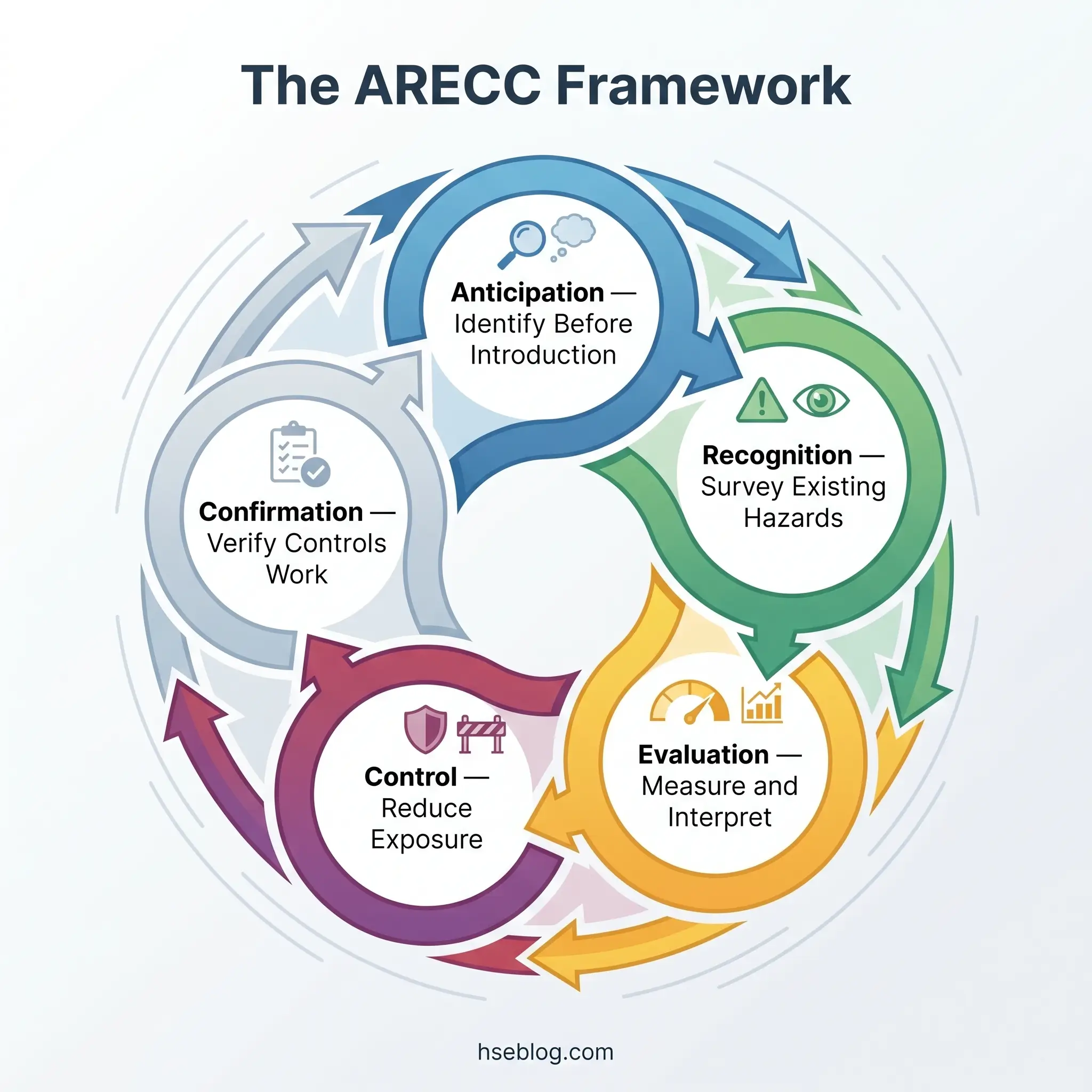
The foundational framework that structures occupational hygiene practice has evolved over decades. The original model — Recognition, Evaluation, Control (REC) — served as the discipline’s operational logic for most of the 20th century. In 1994, AIHA formally added Anticipation as the first stage, recognizing that the most effective point of intervention is before a hazard enters the workplace. More recently, AIHA added Confirmation as the fifth stage, creating the ARECC framework now referenced by AIHA, IOHA, and BOHS. Many textbooks and training providers still teach the four-principle version, which causes confusion when readers encounter five stages elsewhere — both are legitimate, but ARECC reflects current professional consensus.
Practitioners treat ARECC as a feedback loop, not a linear checklist. Confirmation data routinely triggers re-anticipation when it reveals that a controlled exposure has drifted upward or that a process change has introduced an unanticipated stressor.
Anticipation: Identifying Hazards Before They Enter the Workplace
Anticipation operates at the design, procurement, and change-management stage — before a new chemical, process, or piece of equipment is introduced. The practical activities include reviewing safety data sheets before a substance enters the site, assessing new processes during engineering design, and evaluating equipment before commissioning. This is where Prevention through Design (PtD), a NIOSH initiative, has its strongest application. The judgment call at this stage is whether the hazard can be eliminated or substituted before it ever reaches the workforce.
Recognition: Identifying Existing Hazards On-Site
Recognition involves systematic identification of hazards already present — through walkthrough surveys, chemical inventory reviews, process mapping, and structured worker interviews. A critical teaching point: a walkthrough by someone without hygiene training will miss the majority of chronic-exposure hazards. Visible dust clouds are obvious. Vapor exposures at concentrations well above the occupational exposure limit are often invisible and odorless. Recognition requires trained observation and knowledge of exposure routes — inhalation, dermal absorption, ingestion.
Evaluation: Measuring and Interpreting Exposures
Evaluation is the quantitative backbone. This is where the hygienist measures actual worker exposures — through personal air sampling, area monitoring, direct-reading instruments, noise dosimetry, or biological monitoring — and compares the results against occupational exposure limits. The methods section below expands on the specific techniques, but the key principle here is that evaluation produces data, and data must be interpreted statistically, not as isolated pass/fail readings.
Control: Reducing or Eliminating Exposure
Control decisions should flow from evaluation data, not from default PPE selection. The hierarchy of controls (discussed in its own section below) governs control selection: eliminate first, substitute second, engineer third, administer fourth, and reach for PPE only as the last line. A common failure mode across industry is skipping straight to respirators or hearing protection without documenting why higher-tier controls were not feasible.
Confirmation: Verifying Controls Actually Work
Confirmation closes the loop. Post-control air sampling, LEV verification testing, biological monitoring to confirm reduced uptake — these are the activities that distinguish a functioning hygiene program from a paper one. AIHA added this fifth step specifically because controls implemented without verification routinely fail silently. Ventilation systems degrade. Substituted chemicals introduce new exposure routes. Administrative controls depend on behavior that drifts. Without confirmation, the entire cycle operates on assumption.
The Five Categories of Workplace Health Hazards
Occupational hygienists address five broad categories of workplace stressor. Each operates through different mechanisms, requires different measurement techniques, and demands different controls. The classification below follows the framing used by IOHA and is consistent with current BOHS and AIHA training curricula.
| Category | Examples | Primary Route / Mechanism | Typical Control Approach |
|---|---|---|---|
| Chemical | Dusts, fumes, vapors, gases, mists, solvents, acids | Inhalation, dermal absorption, ingestion | Substitution, LEV, enclosure, RPE |
| Physical | Noise, vibration, ionizing/non-ionizing radiation, thermal extremes, pressure | Energy transfer to tissues | Engineering isolation, shielding, exposure-time limits |
| Biological | Bacteria, viruses, fungi, parasites, bloodborne pathogens, bioaerosols | Inhalation, inoculation, ingestion, contact | Containment, ventilation, vaccination, hygiene protocols |
| Ergonomic | Awkward postures, repetitive motion, manual handling, workstation design | Cumulative musculoskeletal strain | Task redesign, mechanical aids, workstation adjustment |
| Psychosocial | Excessive workload, long working hours, harassment, shift-work disruption, low autonomy | Chronic stress response, cardiovascular and mental health effects | Organizational redesign, workload management, policy |
The inclusion of psychosocial hazards as a core category has gained significant traction. The fourth edition of Principles of Occupational Health and Hygiene (Reed, ed., Routledge, 2024) dedicates a full chapter to psychosocial hazards — a first for this foundational reference text. The WHO/ILO Joint Estimates data further reinforces this: long working hours were identified as the largest single occupational risk factor for mortality.
Audit Point: A common structural gap in organizational hygiene programs is treating ergonomic and psychosocial hazards as “HR issues” rather than hygiene concerns. ISO 45001 does not make this distinction — it requires hazard identification and risk assessment across all categories. Auditors assessing conformity with Clause 6.1.2 will look for evidence that the organization has identified psychosocial and ergonomic stressors, not only chemical and physical agents.
Methods Used in Occupational Hygiene Practice
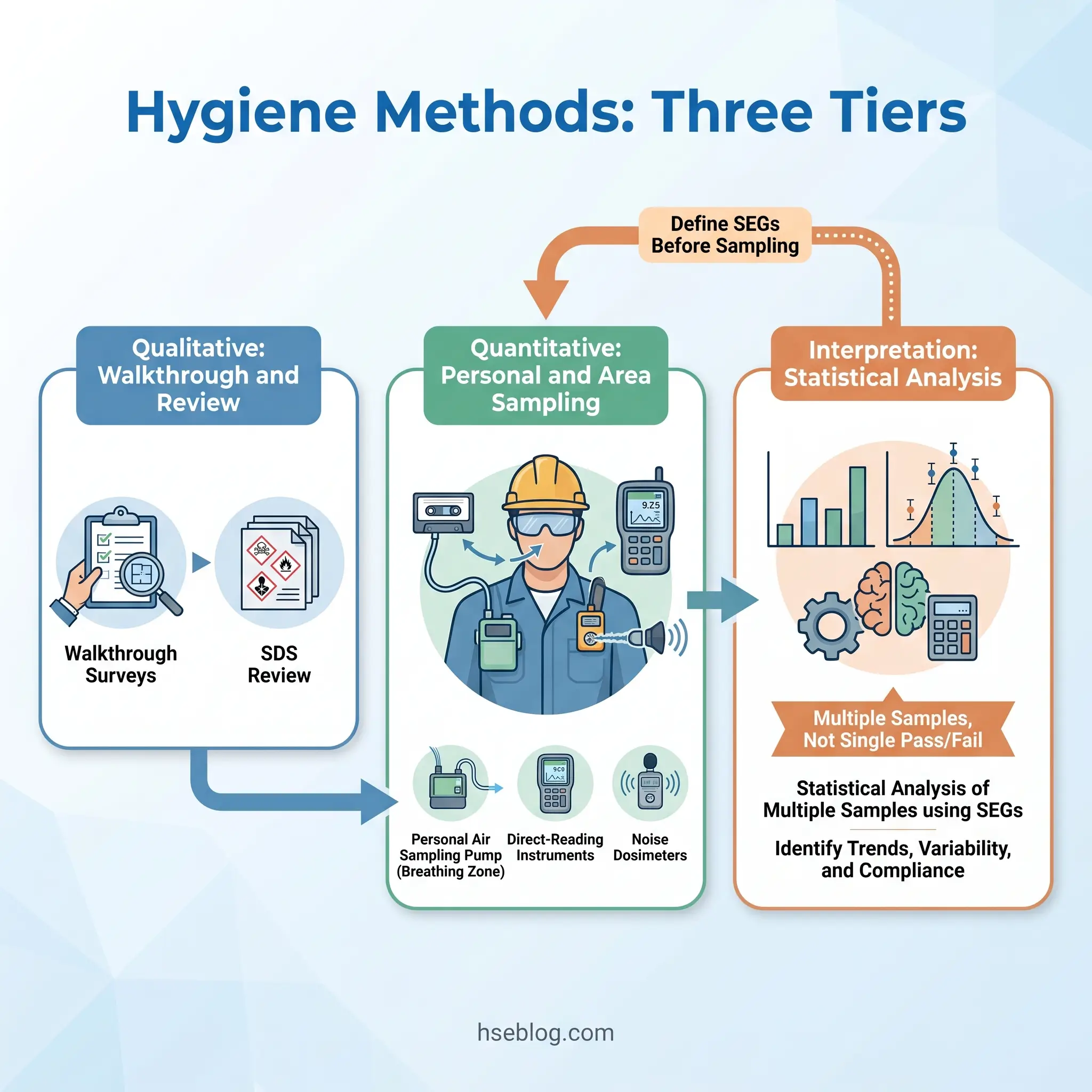
This section addresses the “methods” half of the article’s title — and it is where most competing reference material falls short. Hygiene methods organize into three tiers: qualitative assessment, quantitative sampling, and data interpretation.
Qualitative methods form the foundation. The walkthrough survey — a structured observation of the workplace by a trained hygienist — identifies potential exposure sources, affected workers, exposure routes, and control status. Basic characterization also involves reviewing chemical inventories, safety data sheets, process descriptions, and maintenance records. These steps feed the anticipation and recognition stages of the ARECC framework and determine the sampling strategy that follows.
Quantitative sampling methods produce the exposure data that drives evaluation and control decisions. The principal techniques include:
- Personal air sampling — a calibrated pump draws air through a collection medium (filter, sorbent tube, impinger) positioned in the worker’s breathing zone for a defined period, typically a full-shift 8-hour TWA. This is the gold standard for characterizing individual exposure.
- Area sampling — static samplers placed at fixed locations characterize the general environment but do not represent worker exposure directly.
- Direct-reading instruments — photoionization detectors (PIDs), electrochemical sensors, and real-time aerosol monitors provide immediate concentration data, valuable for identifying exposure peaks and source characterization.
- Surface and dermal sampling — wipe sampling and tape-lift methods assess contamination on surfaces and skin, critical for substances with significant dermal absorption routes.
- Biological monitoring — measurement of a substance or its metabolite in blood or urine, confirming actual worker uptake rather than environmental concentration.
- Noise dosimetry — personal noise dosimeters record time-weighted noise exposure over a shift; integrating sound-level meters measure area noise.
- Heat stress monitoring — wet bulb globe temperature (WBGT) measurement characterizes the thermal environment for heat-stress assessment.
The NIOSH Manual of Analytical Methods (NMAM), 5th edition is the primary published reference for validated sampling and analytical procedures. It is continuously updated — the most recent chapter guidance on surface sampling and dermal exposure assessment was released in August 2022. The OSHA Technical Manual Section II serves as a parallel reference for OSHA compliance officers and practitioners.
Data interpretation is where competence separates functional hygiene from checkbox compliance. Occupational exposures are lognormally distributed and highly variable from shift to shift, task to task, and worker to worker. A single sample result below the occupational exposure limit tells the hygienist almost nothing about whether the exposure group is actually protected over time. AIHA’s exposure-assessment strategy uses the concept of Similar Exposure Groups (SEGs) — groups of workers with comparable exposure profiles — and applies statistical analysis (geometric mean, geometric standard deviation, 95th percentile, exceedance fraction) to determine whether the group’s exposure is acceptably controlled. Properly conducted hygiene evaluation uses multiple samples and statistical interpretation, not single-sample pass/fail judgments.
The Fix That Works: When building a sampling strategy, define your SEGs first — by task, location, material, and duration — before selecting instruments or analytical methods. A beautifully executed sample from the wrong group answers the wrong question.
The Hierarchy of Controls: How Hygienists Reduce Exposure
The NIOSH Hierarchy of Controls ranks control measures from most to least effective. The principle is straightforward: controls that remove the hazard entirely work without relying on worker behavior, while controls at the bottom of the hierarchy depend entirely on it.
The five levels, in descending order of effectiveness:
- Elimination — physically remove the hazard from the workplace. A process that no longer uses a carcinogenic solvent eliminates the exposure entirely.
- Substitution — replace a more hazardous substance or process with a less hazardous one. Replace solvent-based degreasing with aqueous cleaning where technically feasible.
- Engineering controls — isolate workers from the hazard through physical means. Local exhaust ventilation (LEV), enclosure, automated handling, and wet suppression are common engineering approaches.
- Administrative controls — change how work is organized. Job rotation to reduce individual exposure duration, scheduling high-exposure tasks when fewer workers are present, training, and standard operating procedures.
- PPE (Personal Protective Equipment) — the last line, not the first. Respirators, hearing protection, chemical-resistant gloves. Effectiveness depends on correct selection, proper fit, consistent use, and maintenance — all of which introduce failure points.
ISO 45001:2018 Clause 8.1.2 requires organizations to apply this hierarchy when planning actions to address OH&S risks. The UK COSHH Regulations impose a parallel duty: employers must prevent exposure where reasonably practicable, and where prevention is not reasonably practicable, must adequately control it — working through the hierarchy, not jumping to the bottom.
PPE-first thinking remains the most prevalent hygiene failure mode across industry. Organizations default to respirators and hearing protection because they are faster to procure than engineering solutions and do not require process change. A well-run hygiene program documents why each higher-tier control was considered — and why it was or was not selected — before arriving at PPE. This documented rationale is precisely the evidence a regulator or auditor will request.
Occupational Exposure Limits: How Hygienists Know When Exposure Is Too High
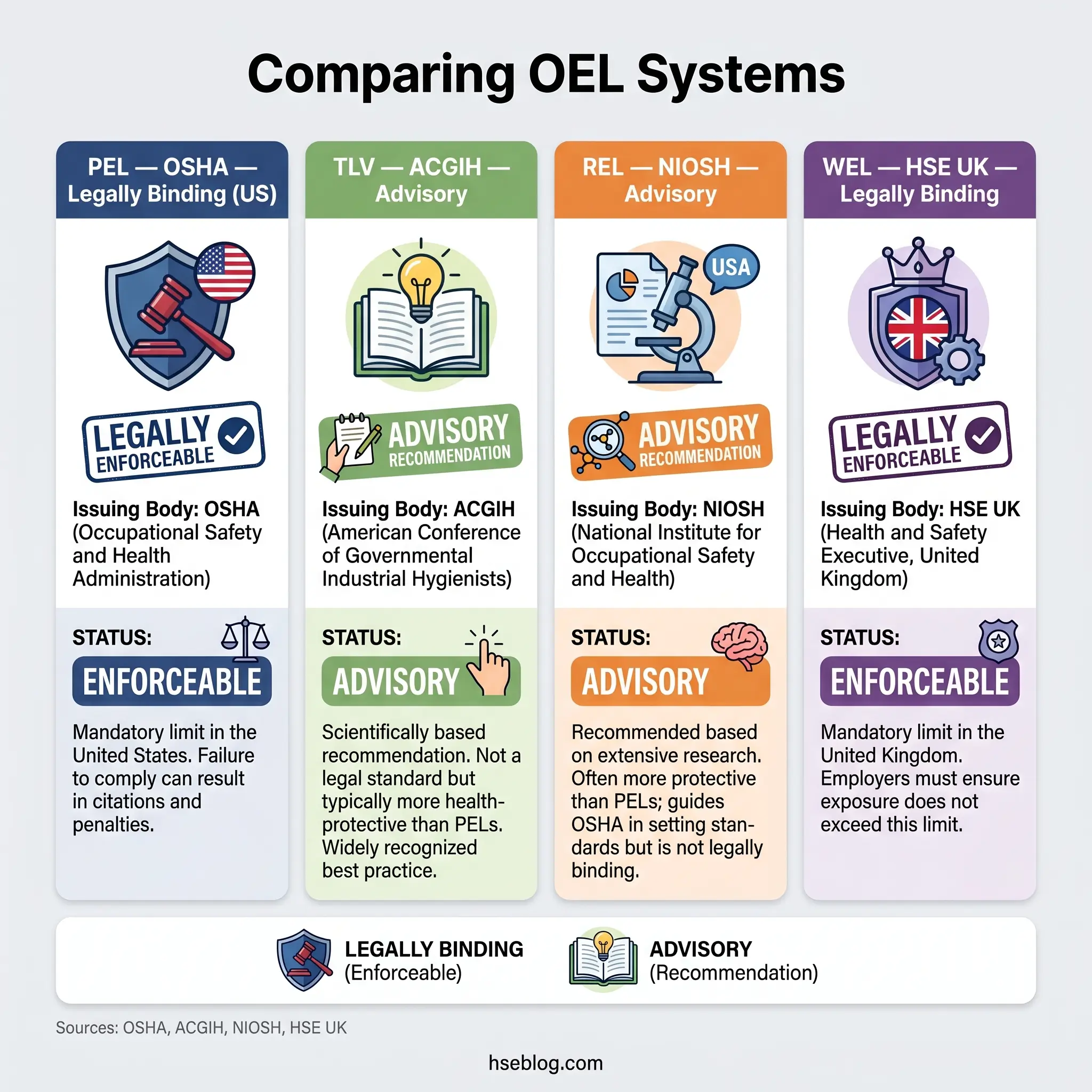
Four OEL systems dominate global practice, and the differences between them are a persistent source of practitioner confusion. Clarity on what each is, who issues it, and whether it carries legal force is fundamental to competent hygiene work.
| OEL System | Issuing Body | Jurisdiction | Legal Status | Update Cadence |
|---|---|---|---|---|
| PEL (Permissible Exposure Limit) | OSHA | US | Legally enforceable (29 CFR 1910.1000 Z-tables) | Most unchanged since 1971 |
| TLV® (Threshold Limit Value) | ACGIH | US-based, internationally referenced | Advisory (not legally binding) | Reviewed annually |
| REL (Recommended Exposure Limit) | NIOSH | US | Advisory (not legally binding) | Updated periodically |
| WEL (Workplace Exposure Limit) | HSE | UK (Great Britain) | Legally enforceable under COSHH (EH40/2005) | Revised periodically; 4th edition 2020 |
EU member states additionally implement Binding Occupational Exposure Limit Values (BOELVs) set under the Chemical Agents Directive and the Carcinogens and Mutagens Directive (2017/2398/EU), transposed into national law.
The values for the same substance frequently diverge across these systems. Carbon monoxide, for example: OSHA PEL is 50 ppm TWA; ACGIH TLV is 25 ppm TWA; NIOSH REL is 35 ppm TWA with a 200 ppm ceiling. Where values diverge, the stricter limit is the more health-protective reference. Compliance with the legally binding limit for the applicable jurisdiction is the minimum — not the ceiling — of protective action.
Three exposure-duration concepts apply across all OEL systems: the 8-hour time-weighted average (TWA), the short-term exposure limit (STEL, typically 15 minutes), and the ceiling limit (never to be exceeded at any time). HSE guidance on Workplace Exposure Limits explains the UK’s application of these concepts under COSHH.
The single most consequential misunderstanding in applied hygiene is equating “below the PEL” with “safe.” OELs are designed to protect most workers over a working lifetime — they do not protect every worker, they do not account for combined exposures from multiple substances, and for carcinogens, asthmagens, and mutagens, many authoritative bodies hold that no truly safe threshold exists. The UK COSHH framework addresses this through the “ALARP” duty (as low as is reasonably practicable) for carcinogens and asthmagens, which applies on top of the WEL — meaning that even when the WEL is met, further exposure reduction is required if reasonably practicable.
Responsible hygienists working in jurisdictions with outdated statutory limits — and most OSHA PELs are widely acknowledged as outdated — use the stricter of the available reference values (often the ACGIH TLV or NIOSH REL), document the rationale, and design control strategies that aim well below the legal minimum.
Jurisdiction Note: When working across borders or with multinational operations, always identify which OEL system applies legally and which additional reference values are appropriate as health-based targets. A single “exposure limits” column on a risk assessment that does not specify source and jurisdiction is a compliance liability.
Who Practices Occupational Hygiene? Roles, Qualifications, and When to Engage One
An occupational hygienist measures workplace exposures, interprets the data, advises on controls, designs monitoring programs, and conducts health risk assessments. The role requires a foundation in science or engineering combined with specific hygiene training and, for full professional standing, credentialing through a recognized body.
The principal credentialing pathways reflect regional structures. In the US, the Certified Industrial Hygienist (CIH) designation — awarded by the Board for Global EHS Credentialing (BGC, formerly ABIH) — requires a STEM degree, a minimum of 48 months of professional hygiene experience, adherence to a code of ethics, and successful completion of a comprehensive examination. In the UK, BOHS awards the Certificate of Operational Competence in Occupational Hygiene (CertOH) and the Chartered Occupational Hygienist status through its Faculty of Occupational Hygiene. Australia’s AIOH offers the Certified Occupational Hygienist (COH) designation. IOHA provides an international recognition framework linking these national bodies. The Occupational Hygiene Training Association (OHTA) modules offer a recognized foundation-level pathway used internationally.
The practical question most readers of this article are asking is when their organization needs a hygienist. The trigger events are identifiable: introduction of new hazardous processes or chemicals, regulatory enforcement action or inspection findings, worker health complaints suggesting uncontrolled exposure, unknown exposure baselines in established operations, complex mixed-exposure environments, or — ideally — at the design stage of a new facility.
Small and mid-sized organizations routinely delay engaging a certified hygienist until after an enforcement notice or a confirmed case of occupational disease. The cost differential between a planned baseline assessment and a post-incident investigation is typically an order of magnitude — and the latter brings regulatory and reputational consequences the former avoids entirely.
Occupational Hygiene in the Wider HSE System
The clearest framing: occupational hygiene works from the environment inward, measuring and controlling workplace stressors. Occupational health works from the worker outward, conducting surveillance, medical assessment, and fitness-for-work evaluation. Occupational safety addresses acute injury risk. Environmental management addresses off-site emissions and ecological impact.
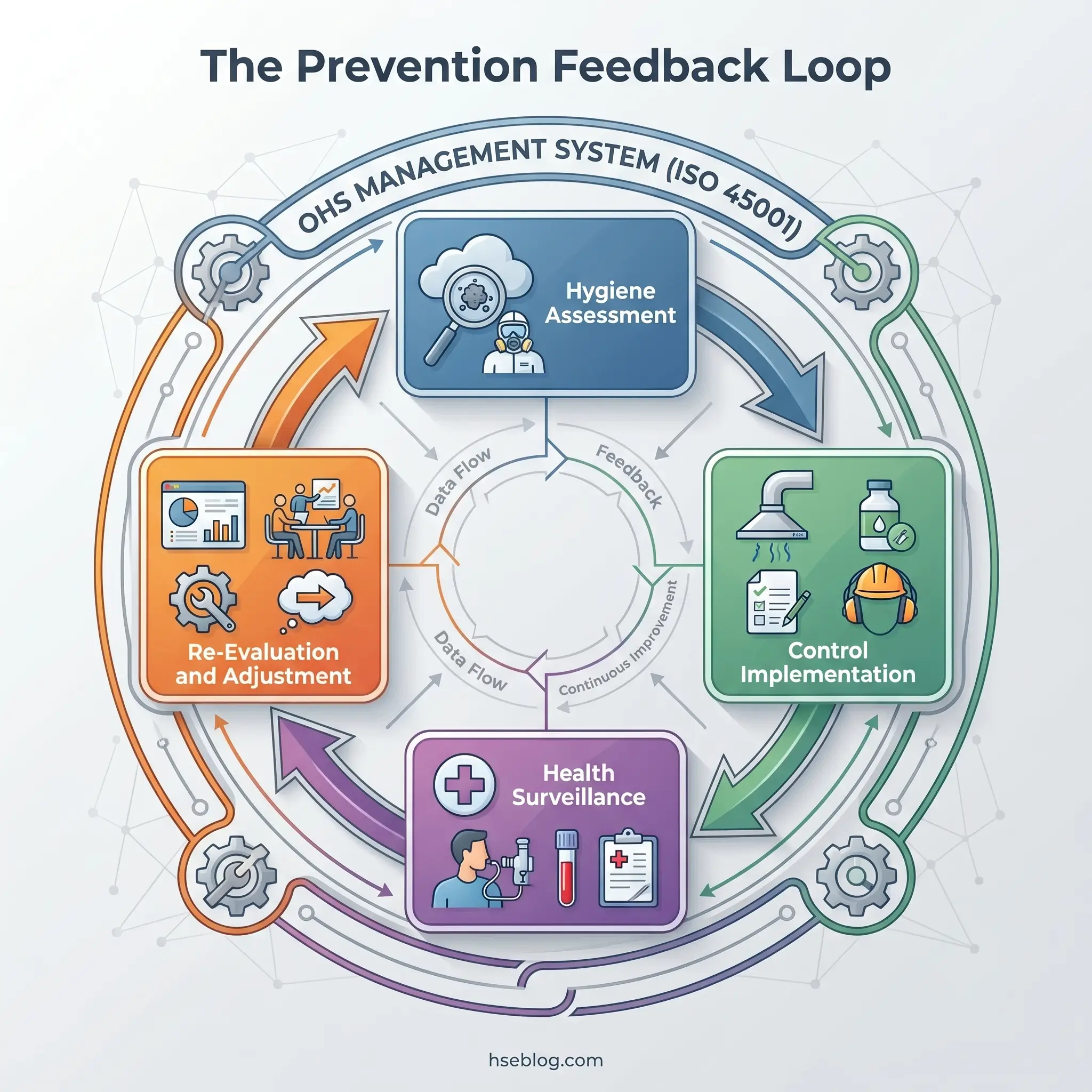
All four sit inside an OH&S management system. ISO 45001:2018 integrates them by requiring hazard identification across all categories, application of the hierarchy of controls (Clause 8.1.2), worker consultation, and continual improvement through a Plan-Do-Check-Act cycle.
The productive feedback loop runs: hygiene assessment → control implementation → health surveillance → hygiene re-evaluation. When organizations run these functions as silos, biological monitoring results fail to inform air-sampling strategy, and elevated health-surveillance findings do not trigger re-evaluation of engineering controls. Integration across these disciplines is not an abstract management-system aspiration — it is what ISO 45001 operationally requires, and it is where the prevention of work-related disease actually happens.
AI-enabled wearable sensors and real-time exposure monitoring are now moving from pilot to operational deployment for heat stress, ergonomic risk, and airborne contaminants. AIHA, the British Safety Council, and NIOSH have all published guidance on the ethical and technical deployment of these technologies (British Safety Council, 2025). These tools do not replace the trained hygienist — they generate data that still requires professional interpretation, SEG design, and control decision-making — but they are expanding the volume and immediacy of exposure data available.
Frequently Asked Questions
Conclusion
The discipline of occupational hygiene exists to solve a specific problem: work-related disease kills millions of people, and most of those deaths are preventable through competent exposure assessment and control. What the industry most consistently gets wrong is treating hygiene as a subset of safety, staffing it with generalists, and measuring success by the absence of current symptoms rather than the quality of current exposure controls.
The single highest-impact change an organization can make is shifting from single-sample compliance checking against outdated exposure limits to a statistically grounded, SEG-based exposure assessment strategy — interpreted by a qualified hygienist and verified through confirmation monitoring. This is not an academic refinement. It is the difference between a program that detects and controls unacceptable exposures and one that repeatedly measures the wrong workers, in the wrong locations, against the wrong benchmarks, and calls the result “compliant.”
Occupational hygiene, practiced well, is a discipline of precision, judgment, and accountability. The framework is clear — anticipate, recognize, evaluate, control, confirm. The methods are validated. The exposure limits, imperfect as they are, provide actionable reference points. What remains is the organizational decision to fund, staff, and empower the function — and to hold it to the standard the discipline demands.