

TL;DR
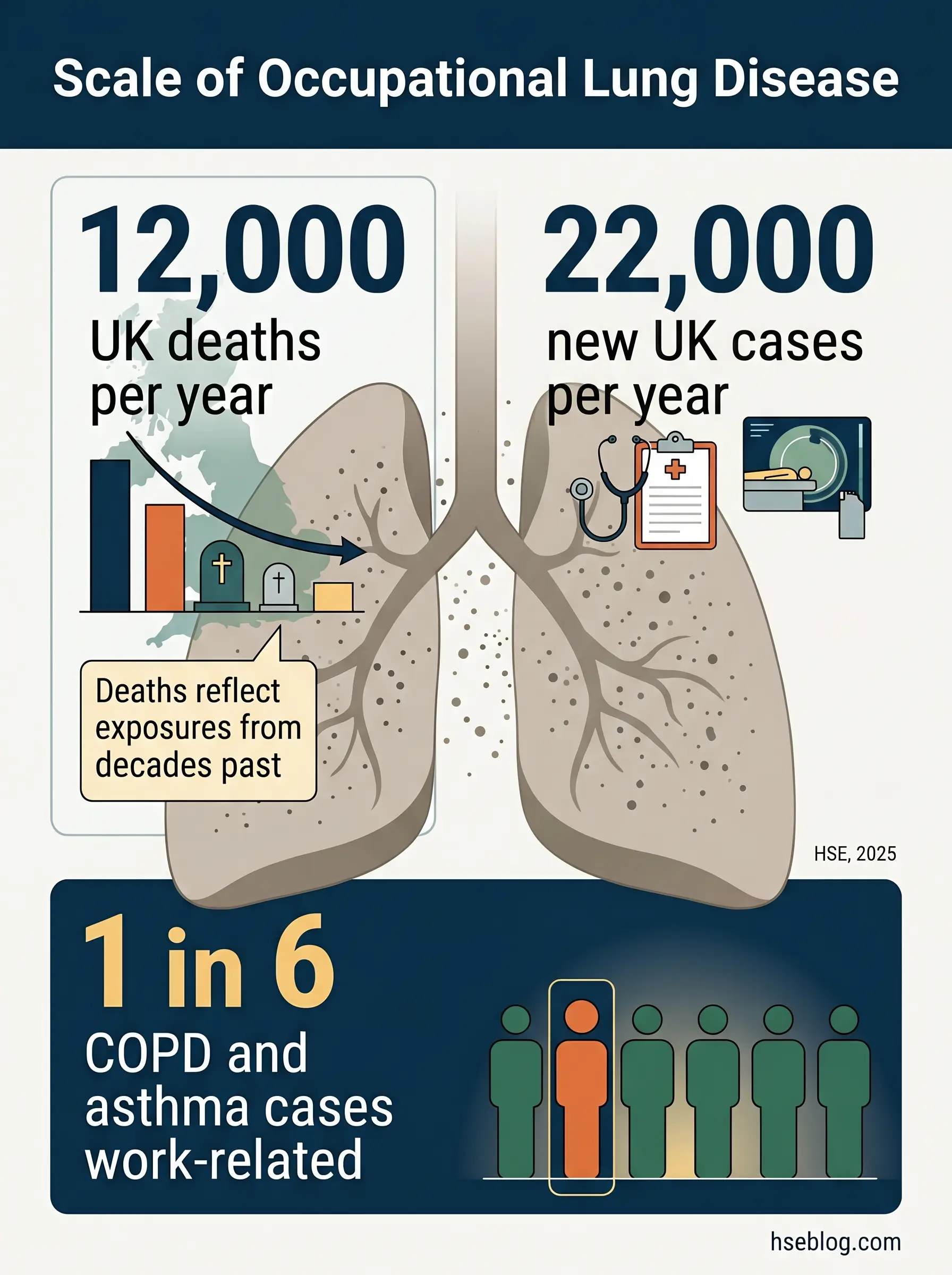
- ~12,000 deaths per year in Great Britain from past occupational lung exposures — mostly COPD, lung cancer, and mesothelioma (HSE, 2025).
- 22,000 new UK cases per year of breathing or lung problems caused or made worse by work (HSE, 2025).
- OSHA PEL for respirable crystalline silica: 50 µg/m³ as an 8-hour TWA; action level 25 µg/m³ (29 CFR 1910.1053).
- One in six global COPD and asthma cases is work-related — and most are never coded as occupational (PMC, 2025).
Occupational lung disease is a group of lung conditions caused or made worse by inhaling substances at work — dusts, fumes, gases, vapours, or biological agents. The main types include silicosis, asbestosis and mesothelioma, coal workers’ pneumoconiosis, occupational asthma, hypersensitivity pneumonitis, and work-related COPD, many of them preventable with proper controls.
About 12,000 people die each year in Great Britain from lung diseases linked to work they stopped doing decades ago (HSE, 2025). Another 22,000 develop new work-related breathing problems every year (HSE, 2025). In California alone, 219 workers cutting engineered-stone countertops had been diagnosed with silicosis by November 2024, including at least 14 deaths and 26 lung transplantations (California Department of Public Health via Annals ATS, 2024). These are not historical numbers. They reflect controls that either never existed or quietly failed.
Occupational lung disease sits at the long-latency end of workplace harm, which is exactly why it is under-recognised and under-prevented. A decision taken today — to substitute a solvent, tighten extraction on a grinder, put a written silica control plan in place — will not show its value for fifteen or twenty years, by which time the worker may have retired, moved on, and been coded as having “idiopathic” disease. This article walks through the main types of occupational lung disease, the exposure categories that cause each one, and the prevention framework a competent HSE function builds around them — with the specific OSHA, MSHA, COSHH, and ILO anchors that employers in different jurisdictions are actually bound by.
What Is Occupational Lung Disease?
Occupational lung disease is not a single condition but a family of lung disorders triggered or worsened by inhaled substances encountered through work. The distinction between disease caused by work — a new silicosis or a new sensitiser-induced asthma — and disease made worse by work, such as pre-existing asthma flared by cleaning chemicals, matters both clinically and for compensation. Most occupational lung diseases also share an awkward feature: long latency. A worker diagnosed today with mesothelioma was most likely exposed in the 1970s or 1980s.
The scale is larger than most employers realise. HSE estimates roughly 12,000 deaths per year in Great Britain from past occupational lung exposures, with COPD accounting for 35%, non-asbestos lung cancer 22–23%, asbestos-related lung cancer 20%, and mesothelioma 20% of the total (HSE, 2025). A 2025 narrative review in a Royal College of Physicians journal put the global burden at around one in six COPD and asthma cases being work-related (PMC, 2025). These figures understate reality because the diagnostic pathway is stacked against attribution.
Reviewing investigation reports and case series, the consistent gap is the unasked occupational history. Primary care and emergency presentations rarely capture it, and by the time a pulmonologist sees the patient, the workplace — the thing that could still be fixed for other workers — has already dropped out of the story.
The Main Types of Occupational Lung Disease
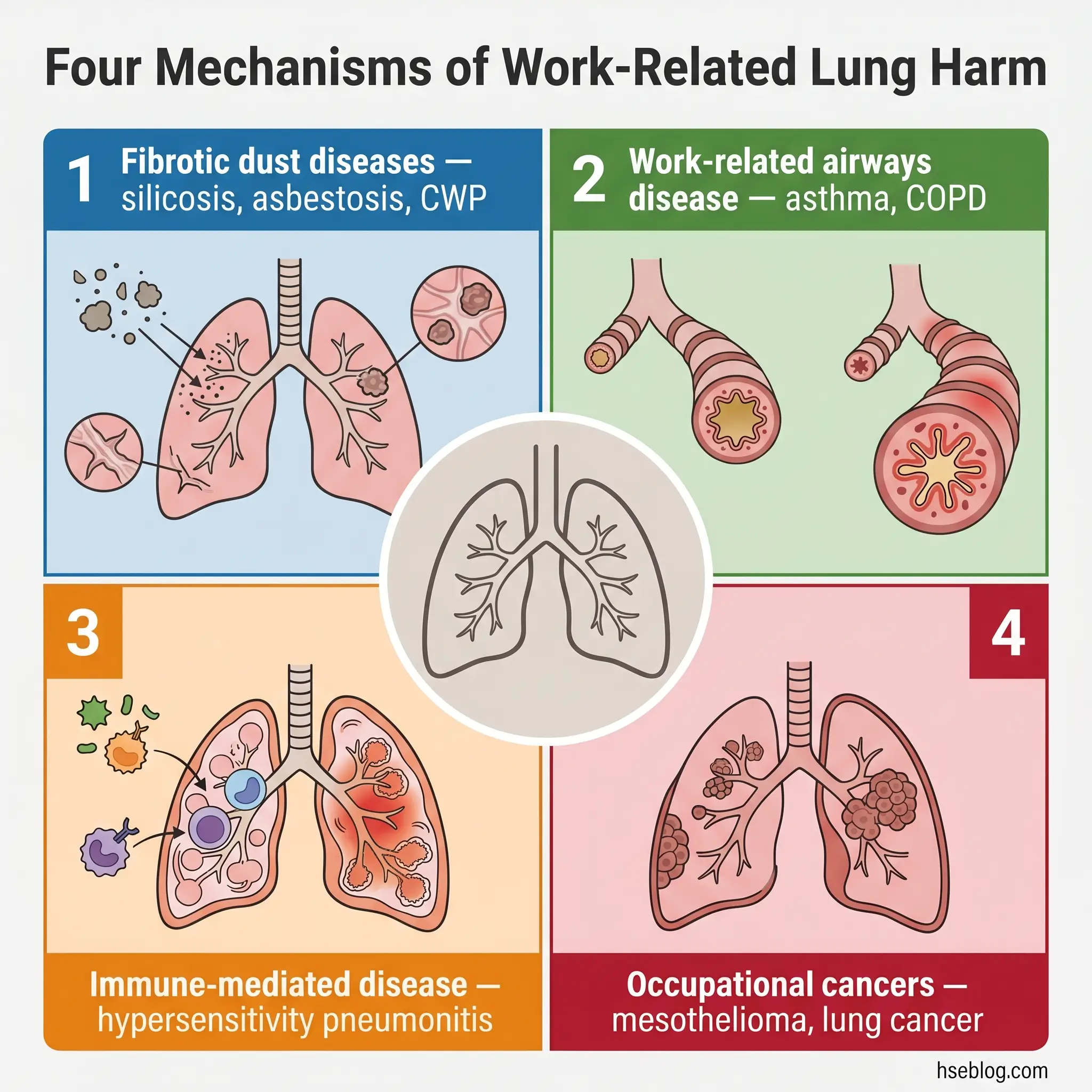
Seven named diseases dominate the clinical picture, but they cluster into four mechanism-based categories that are easier to hold in the head than a flat list: fibrotic dust diseases (the pneumoconioses), work-related airways disease (asthma and COPD), immune-mediated disease (hypersensitivity pneumonitis), and occupational cancers. The table below summarises the principal conditions before each is discussed in detail.
| Disease | Primary Exposure | Highest-Risk Industries | Typical Latency |
|---|---|---|---|
| Silicosis | Respirable crystalline silica | Construction, mining, stone fabrication | 10+ yrs (chronic); months–years (accelerated/acute) |
| Asbestosis | Asbestos fibres | Demolition, shipbuilding, insulation, brake work | 10–20 years |
| Mesothelioma | Asbestos fibres | Same as asbestosis | 20–40 years |
| CWP / Black lung | Coal mine dust (with silica) | Underground and surface coal mining | 10+ years |
| Occupational asthma | Isocyanates, flour, latex, wood dust, cleaning chemicals | Spray painting, bakeries, healthcare, woodworking | Months to a few years |
| Hypersensitivity pneumonitis | Mould, bird proteins, metalworking fluid microbes | Farming, bird handling, metalworking, food processing | Hours (acute) to years (chronic) |
| Occupational COPD | Coal, silica, welding fume, grain dust | Mining, welding, agriculture, cleaning | 10+ years |
Silicosis
Silicosis is a fibrotic lung disease caused by inhaling respirable crystalline silica — the dust released whenever quartz-bearing stone, concrete, brick, or engineered countertop material is cut, drilled, ground, or blasted. It presents in three forms. Chronic silicosis follows decades of lower-level exposure and is the classic construction or foundry presentation. Accelerated silicosis develops in 5–10 years from heavier exposures. Acute silicosis — silicoproteinosis — can appear within months of extreme exposures, most notoriously in engineered-stone fabrication and uncontrolled sandblasting. Once fibrosis is established, it is irreversible.
Silicosis is also the defining modern occupational lung disease story. Engineered stone typically contains over 90% crystalline silica, compared with 10–45% in natural granite (NIOSH, 2026), and dry or semi-dry cutting of the material has produced a global outbreak. In California, 219 cases among countertop workers had been identified by November 2024, including at least 14 deaths and 26 lung transplantations (California Department of Public Health via Annals ATS, 2024). Silicosis also elevates the risk of tuberculosis, lung cancer, autoimmune disease, and chronic kidney disease — a point most patient-facing pages omit.
Under 29 CFR 1910.1053, the OSHA PEL is 50 µg/m³ as an 8-hour TWA, with an action level of 25 µg/m³. The construction standard 29 CFR 1926.1153 operates in parallel and offers Table 1 task-specific controls that let employers comply without individual exposure monitoring when they follow the specified control combination — typically on-tool water suppression or on-tool LEV with HEPA filtration. The practical reading of Table 1 is that it works when the control is maintained. The recurring pattern in silica enforcement is not absent equipment but equipment that has degraded: a torn shroud on a handheld grinder, a water feed switched off to stop slurry, a HEPA filter that has never been changed. Dust control has to live as a daily pre-use inspection item, not a commissioning document.
Jurisdiction Note: ACGIH’s TLV for respirable crystalline silica is 25 µg/m³, half the OSHA PEL. Engineered-stone silicosis has been reported in workers exposed at or near the OSHA limit, which is why industrial hygienists working on high-energy silica processes generally treat the ACGIH value as the design target for engineering controls.
Asbestosis and Asbestos-Related Diseases (Including Mesothelioma)
Three distinct conditions arise from asbestos exposure, and conflating them is one of the most common errors in non-specialist writing. Asbestosis is interstitial fibrosis of the lung parenchyma and generally requires heavy cumulative exposure with a 10–20 year latency. Asbestos-related lung cancer follows a similar latency and is dramatically amplified by smoking — the combined risk is multiplicative, not additive. Mesothelioma is a cancer of the pleural or peritoneal lining with a latency of 20–40 years, and can follow relatively low-dose exposures including take-home exposure of household members.
OSHA 29 CFR 1910.1001 sets the US asbestos PEL at 0.1 fibre/cc as an 8-hour TWA, with an excursion limit of 1.0 fibre/cc over any 30-minute period. The UK banned asbestos use in 1999, but under the Control of Asbestos Regulations 2012 the duty to manage asbestos in pre-2000 buildings remains active and enforced. The highest current exposures are not in new handling but in renovation, demolition, shipyard repair, and brake work — trades that routinely encounter legacy asbestos-containing materials.
Reviewing HSE prosecution notices and US contractor citations, the recurring failure mode is assumed-clean refurbishment. A pre-2000 building without an updated asbestos register is not an inspected building. Contractors rely on outdated surveys, disturb friable insulation behind ceiling tiles or in riser cupboards, and proceed without air monitoring because “the survey said it was fine.” High-risk materials include sprayed coatings, lagging, insulating board, and textured decorative coatings.
Coal Workers’ Pneumoconiosis (Black Lung)
Coal workers’ pneumoconiosis — CWP — is a fibrotic disease caused by respirable coal mine dust. Simple CWP produces small nodular opacities on imaging; its severe complication is progressive massive fibrosis (PMF), which continues advancing even after exposure stops. “Black lung” is a lay umbrella that in practice covers CWP, mixed-dust pneumoconiosis, silicosis in miners, and PMF.
CWP was nearly eliminated in US coal mining by the 1990s but has resurged in central Appalachia and elsewhere. The driver, documented by NIOSH, is silica exposure from cutting roof and floor rock in thinning coal seams — the respirable dust miners now inhale contains more quartz than the classic coal-dust exposures of earlier decades. MSHA’s 2024 final rule (30 CFR Parts 60, 70, 71, 72, 75, 90) lowered the respirable crystalline silica exposure limit for miners to 50 µg/m³ TWA and expanded medical surveillance to metal and non-metal miners, phasing in through 2025.
The recurring diagnostic misread is treating a younger miner’s shortness of breath as deconditioning. Published surveillance has documented PMF in miners under 40 with under 10 years of service; diffusion-capacity testing, not only chest radiography, is what identifies the subtle early decline that surveillance is meant to catch.
Occupational Asthma
Occupational asthma divides into three entities, and the distinction drives the intervention. Sensitiser-induced occupational asthma is new-onset disease from immunological sensitisation to a workplace agent — isocyanates in spray painting and polyurethane, flour in bakeries, latex in older healthcare settings, wood dust, and some cleaning chemicals. Irritant-induced asthma, or Reactive Airways Dysfunction Syndrome (RADS), follows a single high-dose irritant exposure — a chlorine release, an ammonia spill. Work-exacerbated asthma is pre-existing asthma worsened by workplace conditions.
Around 10–25% of adult-onset asthma is occupational in origin (American College of Allergy, Asthma, and Immunology, 2023), and OSHA lists more than 250 known causative substances. The diagnostic red flag the published literature emphasises most is symptoms that improve on weekends and holidays and return within the first day or two back at work. Serial peak expiratory flow monitoring and, where available, specific inhalation challenge are the confirmatory tools.
The most dangerous misconception — the one I see replayed in clinical summaries and workplace safety advice — is that a worker with suspected sensitiser asthma can be trialled on “better PPE” to see if symptoms resolve. Sensitisation does not reverse. Once established, even low-dose re-exposure can trigger severe attacks, and every additional exposure after sensitisation is cumulative damage. The only reliable intervention is removal from the agent.
Hypersensitivity Pneumonitis (Including Farmer’s Lung and Bird Fancier’s Lung)
Hypersensitivity pneumonitis (HP) is an immune-mediated alveolar inflammation triggered by inhaled organic antigens. Over 300 causative antigens have been described — bacterial (farmer’s lung, hot-tub lung), fungal (mushroom worker’s lung, cheese worker’s lung), animal protein (bird fancier’s lung), and chemical (metalworking-fluid HP, isocyanate HP). Acute HP produces flu-like symptoms within hours of exposure and is frequently missed at presentation. Chronic HP produces progressive interstitial fibrosis that can be indistinguishable from idiopathic pulmonary fibrosis if the exposure history is not taken.
A recurring pattern in published case series is the metalworking-fluid HP cluster. When two or more operators on the same line develop respiratory symptoms in the same season, the correct response is a sentinel-event investigation into fluid-reservoir microbial load — not a sequential workup of each affected worker in isolation. Respiratory protection alone is not reliably preventive once sensitisation has occurred; antigen elimination or substitution is.
Occupational COPD and Chronic Bronchitis
Occupational COPD is the most under-recognised category on this list. The published evidence places roughly one in six COPD cases globally as work-related (PMC, 2025), and HSE data attributes 35% of UK occupational lung disease deaths to COPD (HSE, 2025). Yet primary care rarely codes COPD as occupational because the exposure history is seldom collected.
The relevant exposures overlap with the pneumoconiosis story — coal, silica, welding fume — and extend into grain dust, textile dust, and cleaning-chemical vapours. Smoking and occupational exposure interact synergistically, not additively, which means a light smoker in a dusty trade carries more than the sum of the two individual risks. Prevention follows the same controls as for the pneumoconioses: source extraction, exposure monitoring, and surveillance.
The practical implication for employers is that pre-employment spirometry has no value unless it becomes a baseline against which the same worker’s future results are compared. Published normals are population averages; early decline shows up as a drop from the worker’s own baseline long before it breaches predicted values. Employers who skip baseline testing forfeit their own ability to catch early disease.
Occupational Lung Cancer and Other Specific Diseases
Occupational lung cancers include asbestos-related lung cancer, silica-related lung cancer, and — as of IARC’s 2017 reclassification — welding-fume lung cancer, now Group 1. Diesel engine exhaust is also Group 1. Beyond the cancers, two specific diseases deserve mention because they fall outside the classical pneumoconiosis pattern. Bronchiolitis obliterans — “popcorn lung” — caused by diacetyl and related flavouring chemicals, has emerged most recently in coffee-roasting and e-cigarette manufacturing settings, not only in the original microwave-popcorn exposures. Beryllium disease, covered under 29 CFR 1910.1024 (PEL 0.2 µg/m³), can follow very low-level sensitisation in beryllium machining and alloy work.
What Causes Occupational Lung Disease? Exposure Categories
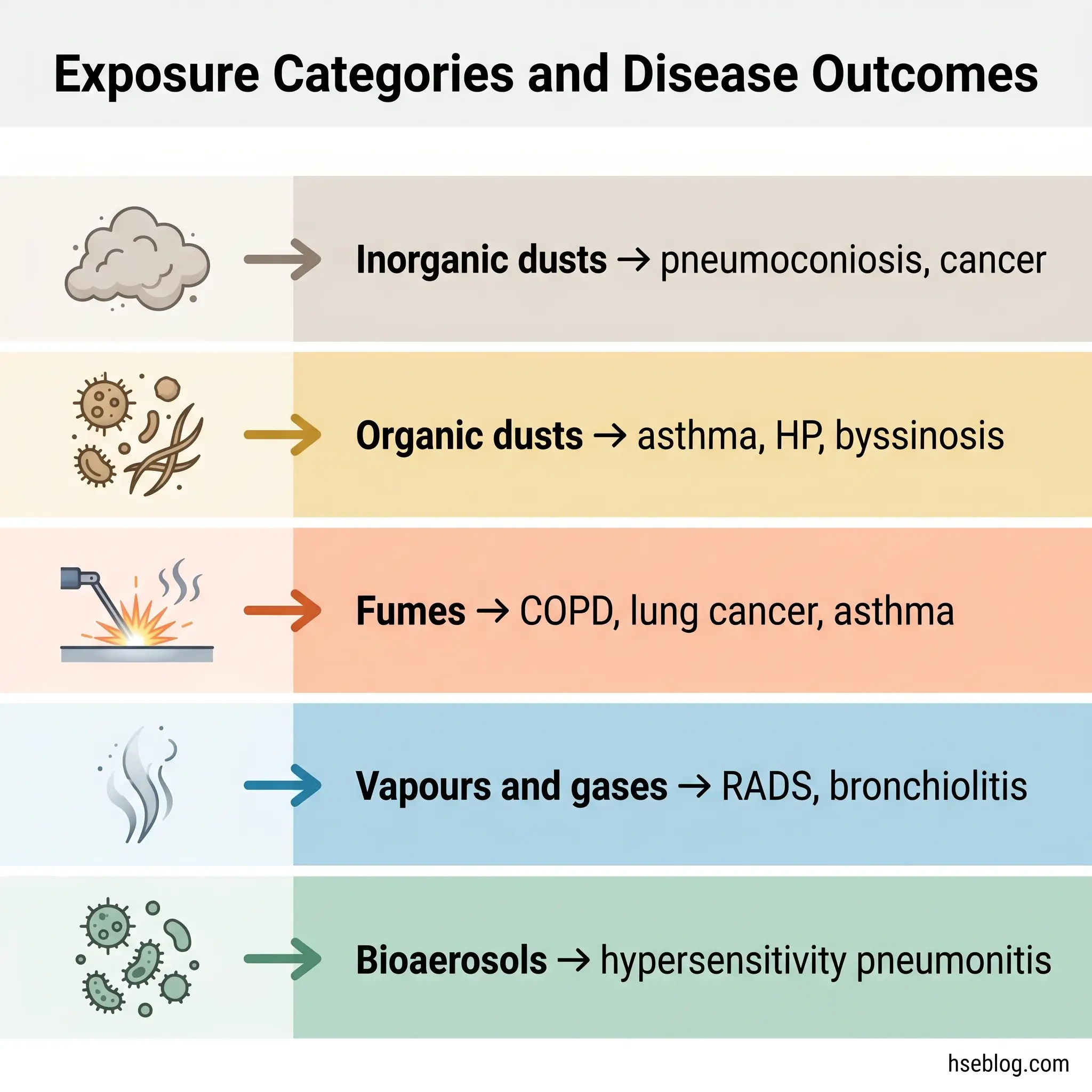
Causation in occupational lung disease maps onto six hygiene categories a working risk assessment can test against. Inorganic dusts — silica, coal, asbestos — produce the pneumoconioses, lung cancer, and mesothelioma. Organic dusts — grain, flour, cotton, wood — produce asthma, HP, and byssinosis. Fumes, which are condensation aerosols from hot processes, include welding fume (now an IARC Group 1 carcinogen, linked to COPD and lung cancer), isocyanate fume from polyurethane processing (asthma), and thermal-decomposition products from coatings.
Vapours and gases — chlorine, ammonia, nitrogen oxides, ozone — drive acute and irritant-induced airways disease including RADS and bronchiolitis obliterans. Bioaerosols — mould spores, bacterial endotoxins, animal allergens — drive HP and occupational infections. Fibres, notably asbestos and some engineered nanomaterials, produce fibrosis and cancer through dimensional mechanisms rather than chemical ones.
The single most useful framing when reading a workplace is that most people are exposed to more than one agent at once. A welder grinding on a painted steel surface is simultaneously taking in metal fume, silica from the abrasive, and organic decomposition products from the coating. A single-agent risk assessment that checks only “welding fume” will understate the actual exposure picture.
How to Prevent Occupational Lung Disease
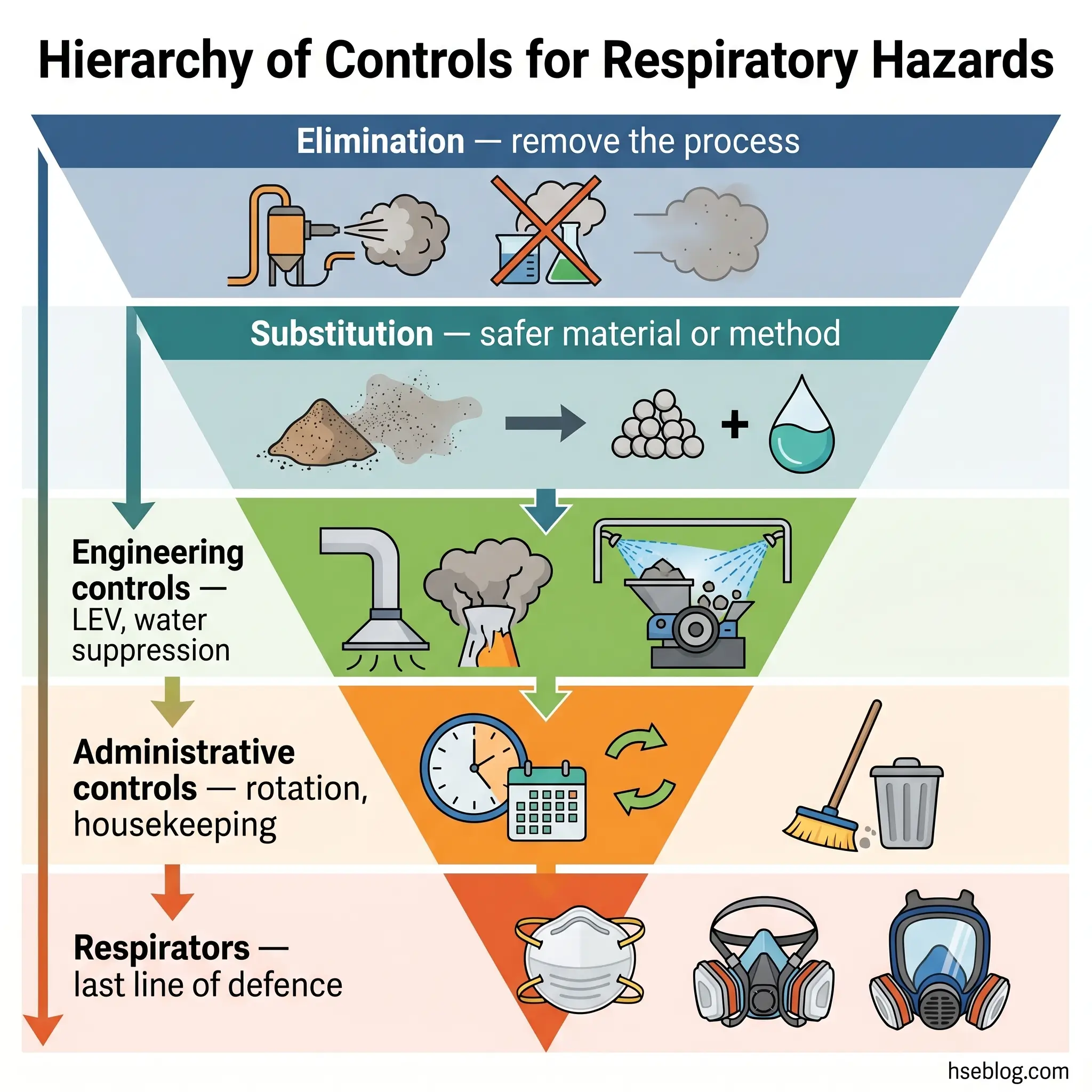
Prevention is a hierarchy, not a menu. NIOSH’s Hierarchy of Controls orders interventions by effectiveness: elimination first, then substitution, then engineering controls, then administrative controls, then respiratory protection as the backstop. The respiratory-hazard reading of that hierarchy is specific and worth walking through, because the pattern that produces most cases is a programme that inverts it — leaning on respirators while engineering controls go un-maintained.
This article provides general HSE knowledge. Life-critical respiratory exposure assessment, control selection, and respirator-programme management must be led by a competent person — typically an industrial hygienist and an occupational physician — with jurisdiction-specific authorisation and site-specific data. The information here does not replace that. Formal training pathways include NEBOSH, IOSH, OSHA Outreach and OSHA 10/30-hour courses, and equivalent national occupational hygiene certifications.
Elimination and Substitution
Elimination removes the hazard; substitution replaces it with something less harmful. Concrete options include water-based coatings in place of solvent-based, low-silica or silica-free abrasives in place of silica sand for blasting, and captive-spray or dip-coating in place of open spraying. Some exposures cannot be eliminated — demolition of legacy asbestos, mining of quartz-bearing rock — but even there the question worth asking is whether a specific sub-task can be substituted, not the whole operation.
Engineering Controls
Engineering controls do the heavy lifting in every mature respiratory programme. The main options are local exhaust ventilation (LEV) with HEPA filtration, on-tool extraction for handheld cutting and grinding, water suppression on silica-generating tasks, enclosure and isolation of high-exposure processes, and general dilution ventilation as a secondary measure. HSE’s HSG258 (3rd edition, 2017) is the authoritative UK design reference and mandates 14-monthly thorough examination and testing of LEV — a duty many sites note on paper and miss in practice.
Administrative Controls
Work rotation, exposure-time limiting, regulated-area demarcation, clean-change procedures, and housekeeping practices sit at this level. Housekeeping is the most frequently neglected: dry sweeping and compressed-air blow-down of silica or asbestos dust actively re-suspend the hazard into the breathing zone and are prohibited under both OSHA and COSHH control principles. HEPA vacuuming and wet methods are the only acceptable approaches.
Respiratory Protective Equipment
Respirators are selected by assigned protection factor against the measured or estimated exposure, require medical clearance and annual fit testing under 29 CFR 1910.134, and function only inside a written respiratory protection programme. IDLH atmospheres require air-supplied respirators, not filtering facepieces. Surgical masks are not respirators and do not protect against respirable dusts — worth stating explicitly because this misconception recurs widely.
Medical and Health Surveillance
Baseline and periodic spirometry, chest imaging where mandated by the substance-specific standard (silica, coal, asbestos, beryllium), symptom questionnaires, and occupational physician review make up the surveillance layer. The pattern in OSHA and HSE enforcement data is that PPE-first programmes — where respirators substitute for missing engineering controls — produce the highest silicosis case rates. Dust control at the source plus surveillance outperforms respirators-everywhere every time.
Regulatory Framework: What Employers Must Do
Regulatory content here reflects general HSE professional understanding of US, UK, and international requirements as of 2026. It is not legal advice. Specific compliance, enforcement, or prosecution questions should be directed to qualified legal counsel in the applicable jurisdiction.
In the US, substance-specific OSHA standards set the duty structure for the major respiratory hazards: 29 CFR 1910.1053 and 1926.1153 for respirable crystalline silica, 1910.1001 and 1926.1101 for asbestos, 1910.1024 for beryllium, 1910.1025 for lead, 1910.1027 for cadmium, and 1910.1048 for formaldehyde. Each imposes exposure assessment, engineering and work-practice controls, respiratory protection, medical surveillance, hazard communication, training, and recordkeeping. The umbrella Respiratory Protection Standard at 29 CFR 1910.134 governs respirator programmes across all of these. MSHA’s 2024 silica rule brings miners into broadly parallel territory, with implementation milestones running through 2025.
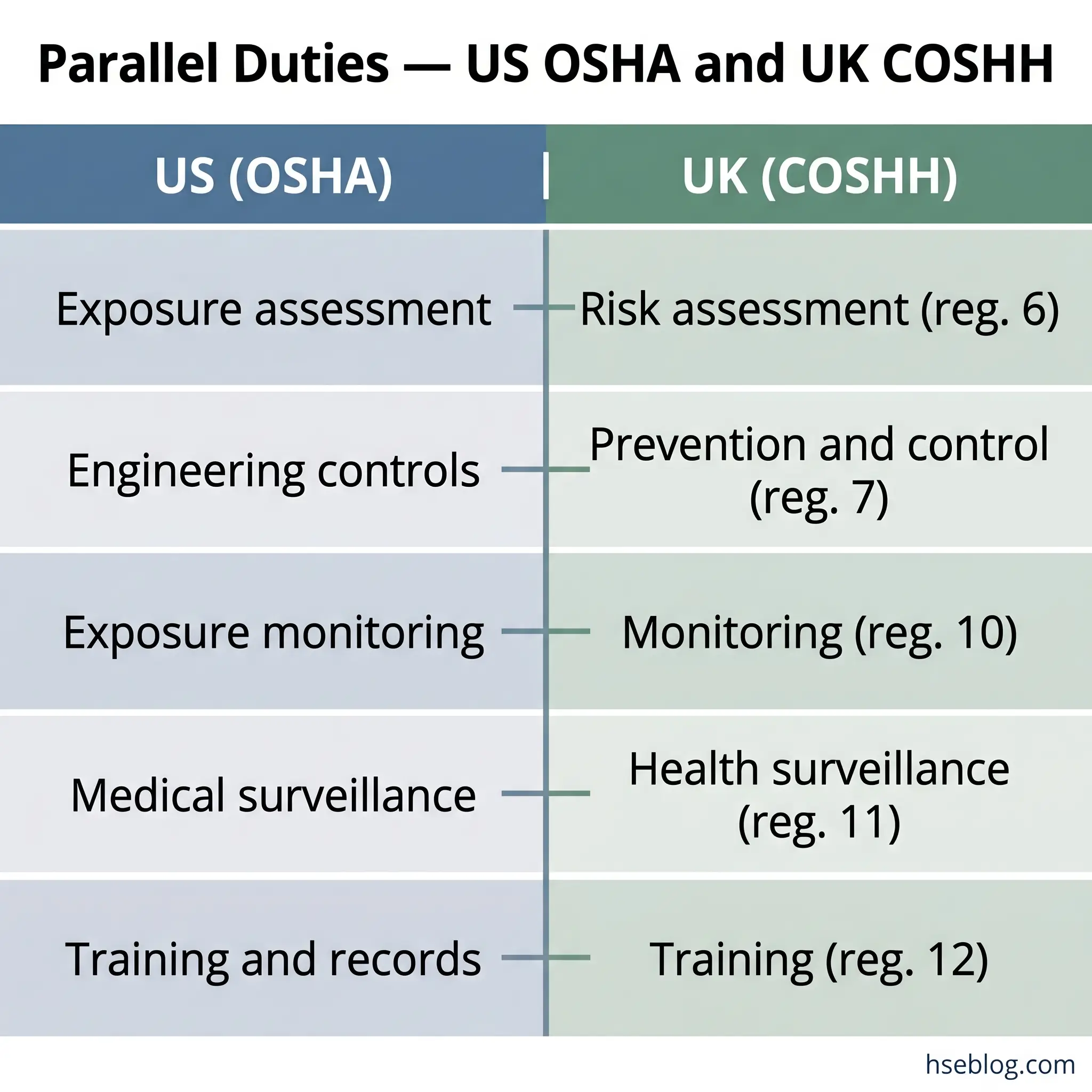
In the UK, the Control of Substances Hazardous to Health Regulations 2002 (COSHH) set the equivalent duties. Regulation 6 requires a suitable and sufficient risk assessment, regulation 7 mandates prevention or adequate control using the hierarchy, regulation 10 requires exposure monitoring where needed to demonstrate adequate control, regulation 11 requires health surveillance for listed processes, and regulation 12 covers information, instruction, and training. Workplace Exposure Limits live in HSE’s EH40 publication and are revised periodically. The Control of Asbestos Regulations 2012 sits alongside COSHH for that substance. Internationally, ILO Convention C155 (1981) frames the general employer duty to prevent injury to health arising out of work, and WHO guidance supports member states in occupational health programme design.
The single most-missed COSHH duty, looking across published HSE enforcement notices, is regulation 10 — exposure monitoring. Many employers write a risk assessment, buy PPE, and never sample. Without measurement, there is no evidence that controls work, and the first confirmed exposure figure is often the one that accompanies a diagnosed case.
Both OSHA and COSHH require long record retention — 30 years for medical and exposure records under OSHA 29 CFR 1910.1020 — precisely because of disease latency. Records destroyed too early are records that cannot support a legitimate compensation claim two decades later.
Recognising Early Signs: When Work Could Be Causing Lung Disease
Pattern recognition is what catches occupational lung disease early enough to change outcomes. Symptoms that improve on weekends or during holidays, symptom onset a few hours after the shift starts, seasonal clustering tied to a specific process, a new material or solvent preceding symptom onset, and a cluster of cases within the same work area are the signals worth investigating. Persistent cough or breathlessness in a worker from a dusty trade is not “just getting older.”
The single most productive question a clinician can add to any respiratory history is whether symptoms change with days away from work. It is also the question most often omitted, which means workers themselves should volunteer it unprompted. Where suspicion exists, the referral pathway runs from occupational physician to respiratory specialist, and in complex cases to a specialist occupational lung disease centre.
Content covering symptoms, diagnosis, and surveillance of occupational lung disease is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms or exposure concerns should consult an occupational physician or qualified medical professional.
Frequently Asked Questions
Conclusion
The industry’s recurring error is not the absence of controls — it is the absence of the link between the workplace of 2026 and the lung-disease statistics of 2046. Silica dust extracted today prevents a silicosis diagnosis two decades from now, in a worker who will probably not remember which site installed the on-tool LEV that quietly saved his lungs. Because the benefit lands out of sight, the investment keeps getting deferred. That is the single highest-impact change for any HSE function dealing with occupational lung disease: treat engineering controls and surveillance as the return on a long-dated instrument, not as optional overhead.
The second lesson sits on the clinical side. Most occupational lung disease is missed at diagnosis because no one asks the work history. A clinician who adds the weekend-pattern question and the dusty-trade question to the standard respiratory workup identifies attributable cases that would otherwise be coded as idiopathic, opens the compensation route for the worker, and — the part that matters most to an HSE function — creates the sentinel signal that tells a workplace its controls are failing. Occupational lung disease is a preventable epidemic that is currently prevented one site at a time, by the people who take exposure measurement seriously before anyone gets ill.