

A fitter on the 2,000-bed warehouse I support slipped on a damp loading bay ramp at 04:40 during the overnight replenishment shift. Left wrist fracture, confirmed at A&E by 07:15. By the time the duty manager handed me the incident log at shift changeover, he’d already emailed HR about “updating the accident book.” What he hadn’t done was notify HSE — because he genuinely didn’t know a wrist fracture crossed the Regulation 4 threshold. He assumed only amputations and fatalities triggered a RIDDOR report. That single gap — one supervisor, one misclassified injury — is the exact pattern that produces most under-reporting across UK workplaces. The rules aren’t complicated. They’re just poorly taught.
RIDDOR reportable injuries are among the most misread parts of UK safety law. The Health and Safety Executive recorded 59,219 non-fatal employee injuries reported under RIDDOR in 2024/25 — the second-lowest number on record — while roughly 680,000 workers self-reported a non-fatal workplace injury over the same period. That gap isn’t workers exaggerating. It’s employers and site teams misclassifying what “reportable” actually means. This article gives you a field-tested framework to classify any injury in under a minute, walks through every specified injury with worked examples, and resolves the edge cases that most guides sidestep.
What Is a RIDDOR Reportable Injury?
A RIDDOR reportable injury is an injury that an employer, self-employed person, or person in control of premises has a legal duty to report to HSE under the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013. The duty sits primarily in Regulations 4, 5, and 6 — which govern injuries to workers, injuries to non-workers, and work-related deaths, respectively.
The term “reportable” carries a specific legal weight. It means the responsible person must notify HSE through the F2508 reporting route, not simply log the incident internally. Three points frame the entire regulatory scope:
- Reportable injuries sit inside RIDDOR’s wider remit, which also covers occupational diseases, dangerous occurrences, and gas incidents — each with its own triggers. This article focuses on injuries.
- Reporting and recording are different duties. Every accident goes in the accident book. Only a subset of those accidents becomes a RIDDOR report.
- The responsibility to report never falls on the injured person. It belongs to the dutyholder, regardless of where fault sits.
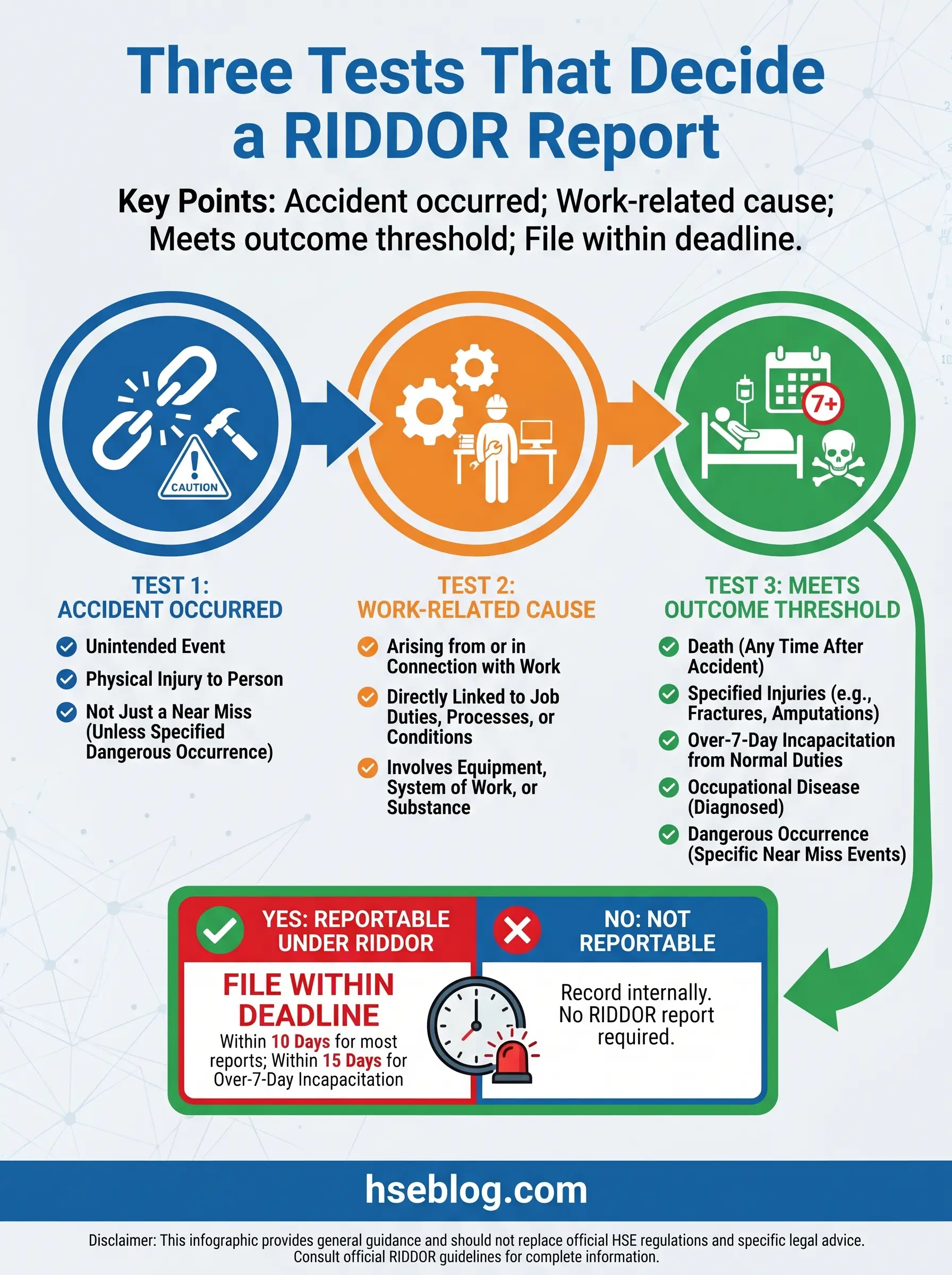
The 3-Test Framework: Is This Injury Reportable?
Every RIDDOR decision collapses into three questions, asked in sequence. If any one fails, the injury is not RIDDOR reportable — though accident book recording still applies. This framework is what I hand to site managers during their first RIDDOR briefing, and it holds up across every sector I’ve worked in.
Test 1 — Was the Injury Caused by an “Accident”?
HSE defines an accident as a separate, identifiable, unintended external event causing physical injury. That phrasing matters. A warehouse operative who develops back pain after six months of repetitive pallet lifting has suffered a gradual injury with no identifiable event — outside the RIDDOR accident definition. A warehouse operative whose back gives way while catching a falling load has experienced a separate, identifiable event. The first is not a RIDDOR accident. The second is.
Acts of non-consensual physical violence against a person at work count as accidents. Heart attacks, strokes, and other naturally occurring medical events at work are not accidents unless an external work event caused them — a collapse from heat stress inside a confined space is accident-caused; a cardiac event while sitting at a desk is not.
Test 2 — Was the Accident Work-Related?
Work-related means “arising out of or in connection with work.” Being on work premises isn’t enough by itself. The injury must have a causal link to the work activity, the equipment used, or the way work is organised. I’ve seen supermarket clients over-report customer trips in the car park — assuming the premises connection is sufficient. It isn’t. A shopper who slips on their own dropped drink has no work-related nexus. A shopper who slips on a wet patch left by a staff member mopping without a sign does.
Test 3 — Does the Injury Meet a Reportable Threshold?
Even a work-related accident doesn’t trigger a report unless the outcome crosses one of four thresholds: a death, a specified injury under Regulation 4, over-7-day incapacitation, or a non-worker taken directly to hospital for treatment. The rest of this article breaks each threshold down in detail.
Work-Related Fatalities: When Deaths Must Be Reported
Regulation 6 requires the death of any person — worker or non-worker — to be reported if it arises from a work-related accident. The requirement extends beyond the day of the accident: if a worker dies within one year of a work-related injury, and that injury caused the death, a report is required even where an earlier RIDDOR report covered the original incident.
Great Britain recorded 124 worker fatalities in 2024/25, with construction accounting for 35, agriculture, forestry and fishing 23, and transportation and storage 15. Falls from height remained the leading cause. Those numbers reflect only what’s reported. The categories feeding them — falls, struck-by, trapped-by collapse — describe roughly 60% of fatal injuries and are the threshold cases where reporting duties most commonly activate.
A handful of exclusions apply:
- Suicides are currently excluded from the reportable scope, though this sits under active policy debate as HSE and stakeholders reconsider whether work-linked suicides should be captured.
- Natural-cause deaths unconnected to a work accident — a cardiac arrest unrelated to any external event — are outside Regulation 6.
- Self-employed persons dying on premises they solely own or occupy are excluded.
- Armed forces personnel killed on duty fall outside RIDDOR and are reported under military arrangements.
Specified Injuries Under Regulation 4
The specified injury list is where reporting most often goes wrong. Supervisors remember the category exists but misjudge the boundaries. A finger fracture is excluded; a wrist fracture is reportable. A burn to 5% of the body is excluded; a burn damaging the eye is reportable whatever the area. The table below sets out all eight specified injuries exactly as Regulation 4 and HSE’s specified-injuries guidance define them.

| Specified Injury | What’s Included | What’s Excluded | Quick Example |
|---|---|---|---|
| Fractures (other than fingers, thumbs, toes) | Any bone fracture diagnosed or confirmed by a doctor | Suspected or self-diagnosed fractures; finger, thumb, and toe fractures | Warehouse operative fractures wrist falling from mezzanine step |
| Amputations | Loss of arm, hand, finger, thumb, leg, foot, or toe — traumatic or surgical after the injury | Partial loss of soft tissue without bone separation | Machine operator loses index finger in an unguarded nip point |
| Permanent sight loss or reduction | Loss or reduction of vision in one or both eyes where effects are likely permanent | Temporary blurred vision; irritation that resolves | Welder suffers permanent corneal damage from arc flash without a shield |
| Crush injury to head or torso | Crushing causing damage to the brain or internal organs | Crush injuries to limbs without organ involvement | Operative trapped between a reversing forklift and racking, liver damage confirmed |
| Serious burns | Burns covering more than 10% of body surface OR damaging eyes, respiratory system, or vital organs | Smoke inhalation alone; minor scalds | Chemical splash burns the face and 15% of the torso |
| Loss of consciousness | Caused by head injury or asphyxia | Fainting from feeling unwell, low blood sugar, or heat without asphyxia | Operative knocked unconscious by a falling tool; asphyxiated in a poorly ventilated tank |
| Scalping requiring hospital treatment | Separation of the skin from the head | Superficial head lacerations | Long hair caught in a rotating shaft, partial scalping |
| Enclosed-space injury | Working in an enclosed space causing hypothermia, heat-induced illness, resuscitation, or admission to hospital for more than 24 hours | Minor discomfort from confined work | Fitter develops hypothermia repairing a refrigerated cold store |
Audit Point: An HSE inspector reviewing your RIDDOR log against your accident book will look first for wrist, ankle, and lower-leg fractures that were recorded but never reported. That’s the most common classification error on site.
Over-7-Day Injuries: The Most Commonly Missed Report
Over-7-day incapacitation is the single most under-reported category I encounter during compliance reviews. It fails not through negligence but through counting errors. A worker injured on Monday, off full duties from Tuesday, back on light duties the following Wednesday morning, has been incapacitated for seven full days — and crosses the threshold on the eighth.
The counting rules are precise:
- The day of the accident is excluded from the seven-day count.
- Weekends, rest days, and non-working days are included, regardless of whether the worker was scheduled to work.
- Incapacitation covers any inability to perform normal duties — not just full absence. If the worker is on modified or light duties because they can’t do their usual job, they are incapacitated for RIDDOR purposes.
The reporting deadline is 15 days from the date of the accident — not 15 days from when the seven-day point was crossed. Where the extent of the injury only becomes apparent later, the duty to report activates as soon as the seven-day threshold is passed.
This is where RIDDOR diverges sharply from the accident book. An over-3-day incapacitation must be recorded but does not need reporting. An over-7-day incapacitation must be both recorded and reported.
Injuries to Non-Workers
Regulation 5 covers members of the public, visitors, students, pupils, and volunteers. A non-worker injury is reportable when the person is taken directly from the scene of the accident to hospital for treatment of an injury arising from that accident. Two boundaries catch people out.
First, treatment means treatment. A precautionary visit, a diagnostic X-ray, or an examination that concludes “no injury present” does not trigger a report. The person must be receiving active treatment for an injury caused by the accident.
Second, hospital premises operate under a special rule. If the accident occurs on hospital premises — a visitor trips in an A&E corridor, for example — only specified injuries to non-workers are reportable, not all hospital-treatment cases. Without that carve-out, hospitals would be reporting every inpatient fall.
Students and volunteers are classified as non-workers unless they are on a formal training scheme or work experience placement, in which case they’re treated as workers. And the work-related test still applies — the injury must arise out of or in connection with work. A child falling during normal PE play is not reportable; a child injured because a school’s climbing frame collapses from poor maintenance is.
Watch For: Receptionists and security staff often send non-worker casualties to hospital in a taxi “as a precaution.” Unless the hospital actually treats an injury, this doesn’t meet the Regulation 5 trigger — but it’s frequently over-reported.
What Is NOT a RIDDOR Reportable Injury
Under-served in most guides, this category matters because misclassification runs both ways. Every hour spent on a non-reportable entry is an hour taken from the genuine reports. The following injuries and scenarios fall outside RIDDOR’s scope:
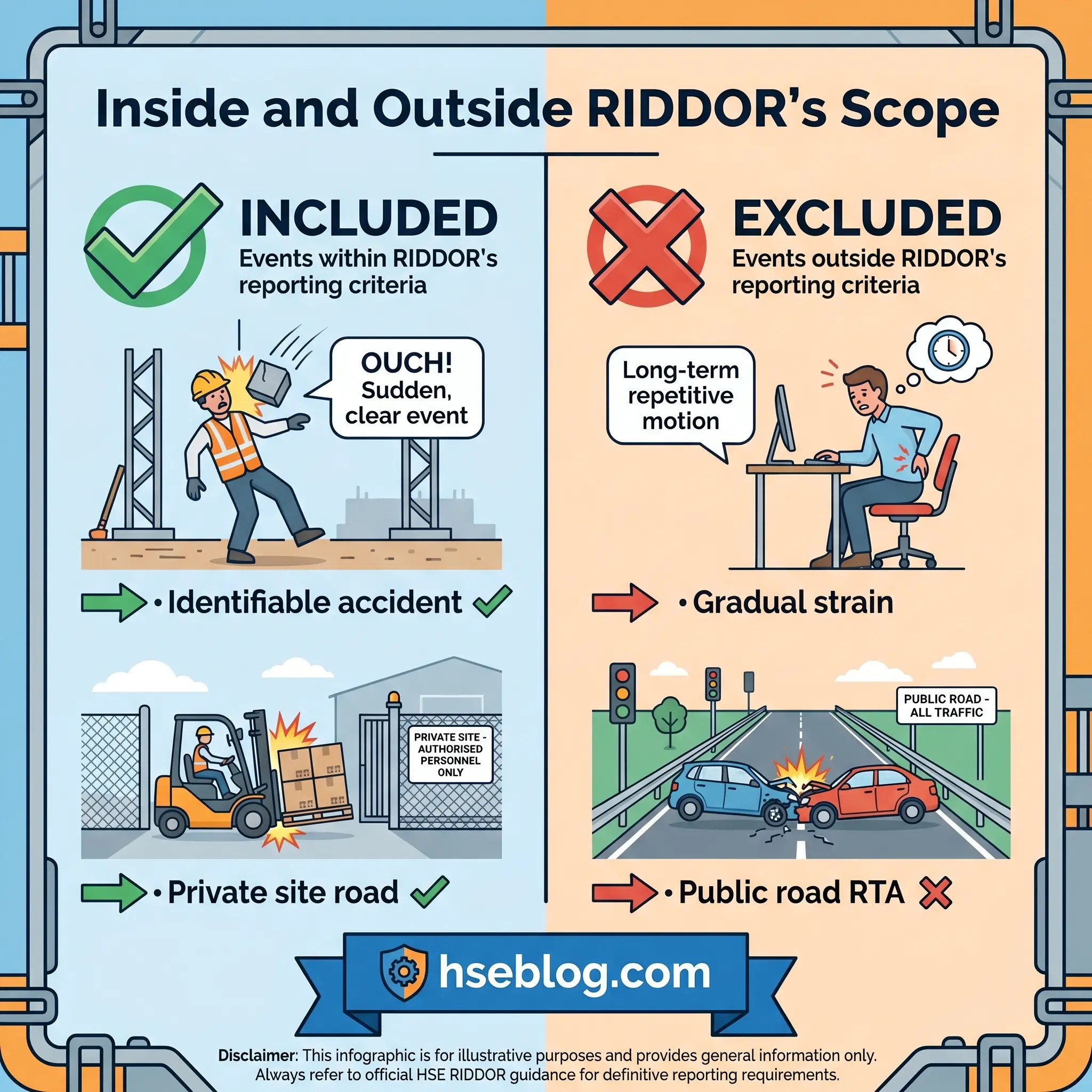
- Cumulative or gradual injuries without an identifiable triggering event — repetitive strain from routine work over months is outside the RIDDOR accident definition.
- Heart attacks and strokes occurring at work where no external accident caused the event.
- Injuries arising from medical or dental treatment by a registered practitioner, including examinations.
- Road traffic accidents on public roads, which are reported to the police under Regulation 14, with exceptions for loading or unloading, roadside work (construction, maintenance, examination), escape of conveyed substances, and train-related incidents.
- Armed forces personnel injured on duty, reported under military arrangements.
- Sporting injuries from normal participation in a sport, unless caused by faulty equipment, poor organisation, or inadequate supervision.
- Precautionary hospital visits where no injury is diagnosed.
- Verbal abuse or psychological harm without an accompanying physical injury — though this remains a live policy debate, particularly around work-related suicide.
- Self-employed persons dying on premises they solely own or occupy.
RIDDOR Reporting Deadlines: How Fast Must You Report?
Three timeframes apply, matched to incident severity. The mistake I see most often is treating them all as 10 days — which delays serious reports and leads to avoidable compliance gaps.
| Incident Type | Notification Trigger | Deadline | Method |
|---|---|---|---|
| Fatality or specified injury | Without delay upon becoming aware | Written report within 10 days | Phone (0345 300 9923, office hours) or online F2508 |
| Over-7-day injury | When 7-day incapacitation is crossed | Within 15 days of the accident | Online F2508 |
| Non-worker taken to hospital | Without delay upon becoming aware | Within 10 days | Online F2508 |
| Death within 1 year of accident | Upon becoming aware of the death | Without delay | Online F2508 |
“Without delay” is interpreted in HSE enforcement guidance as “as soon as reasonably practicable.” In practical terms, this means the same day or the next working day for serious incidents. A responsible person who waits a week before notifying a fatality is not meeting the duty, even if the written report follows within 10 days.
Who Is the “Responsible Person” Required to Report?
The term “responsible person” in RIDDOR identifies who carries the reporting duty. It is never the injured worker or the member of the public. Where confusion arises — and it arises often — is in multi-employer sites, agency placements, and host-guest arrangements.
- Employers are responsible for reporting injuries to their own employees, wherever those injuries occur.
- Self-employed persons report their own injuries and the injuries of anyone else hurt on their premises.
- Persons in control of premises report non-worker injuries and, importantly, injuries to self-employed workers on their site.
- Host businesses carry the reporting duty for agency or contractor workers placed on their premises, even though those workers are formally employed elsewhere.
When an employer fails to report, an injured worker can contact HSE directly to raise the concern. The duty sits with the dutyholder, but the enforcement route for workers remains open.
Recording vs Reporting: The Accident Book Duty
A client once asked me why their accident book had 140 entries for the year when only 11 RIDDOR reports went to HSE. They thought they’d been under-reporting. In fact, they’d been doing it right. The accident book captures everything. RIDDOR captures the legally defined subset.
| Aspect | Accident Book (Recording) | RIDDOR (Reporting) |
|---|---|---|
| Scope | Every workplace accident | Only accidents meeting RIDDOR criteria |
| Over-3-day incapacitation | Recorded | Not reported |
| Over-7-day incapacitation | Recorded | Reported |
| Retention | 3 years minimum under Regulation 12 | 3 years minimum under Regulation 12 |
| Legal basis | Social security and HSE guidance | RIDDOR 2013 |
Records must include the date and time of the incident, details of the injured person, the circumstances, and the nature of the injury. Regulation 12 sets the three-year minimum retention period.
What to Do When the Extent of the Injury Is Unclear
HSE’s own guidance accepts that the severity of an injury isn’t always immediately knowable. A worker with a serious eye injury may not have a confirmed prognosis for weeks. An injured limb may be under medical review for possible amputation. The correct approach isn’t to file a precautionary report — it’s to wait for confirmation.
Two scenarios come up regularly:
A crush injury to the hand where surgeons are deciding whether to amputate the middle finger. The worker is clearly incapacitated, so the over-7-day trigger will almost certainly apply regardless, and that report can be made on schedule. If amputation is later confirmed, update HSE with the specified injury detail.
An eye injury where the ophthalmologist won’t confirm permanence for six weeks. Wait for confirmation. If permanence is confirmed, report as a specified injury at that point. If vision recovers, no specified injury report is required — though the over-7-day rule may still have applied.
Worked Examples: Reportable or Not?
Every scenario in the table below maps onto the 3-test framework. Read each one, decide for yourself, then check the reasoning.
| Scenario | Reportable? | Reason |
|---|---|---|
| Warehouse worker fractures arm falling from a ladder | Yes | Specified injury (fracture other than finger/thumb/toe) |
| Office worker sprains ankle, off normal duties for 10 days | Yes | Over-7-day incapacitation |
| Employee has a heart attack at work, unrelated to any accident | No | No accident; fails Test 1 |
| Shopper collides with another car in supermarket car park during a personal visit | No | Not work-related; fails Test 2 |
| Delivery driver struck by moving vehicle on a private site road | Yes | Private road exempt from the RTA exclusion |
| Catering worker trapped in a cold store, develops hypothermia | Yes | Specified injury — enclosed-space harm |
| Pupil injured in a PE lesson through normal sporting contact | No | Sporting injury during normal participation |
| Pupil injured at school due to faulty climbing-frame equipment | Yes | Equipment failure brings it into work-related scope |
| Staff member verbally abused, takes 2 weeks off with stress | No | No physical injury from an accident |
| Worker killed by a delivery van in a car park while leaving work | Yes | Van engaged in work activity; Regulation 6 applies |
Consequences of Failing to Report
RIDDOR is a criminal reporting duty. Non-reporting isn’t an administrative oversight — it’s a breach of statutory duty under the Health and Safety at Work etc. Act 1974, Section 33. HSE has the power to prosecute, and the courts can impose unlimited fines in serious cases and, rarely, imprisonment where individual directors are charged.
Enforcement context matters. Approximately 9% of RIDDOR-reported non-fatal injuries are investigated by HSE, and prosecution conviction rates sit around 94% where charges are brought. The commercial and reputational fallout runs deeper than the fine: insurance renewal questions, contract pre-qualification failures, and public tender exclusions all flow from a history of reporting failures.
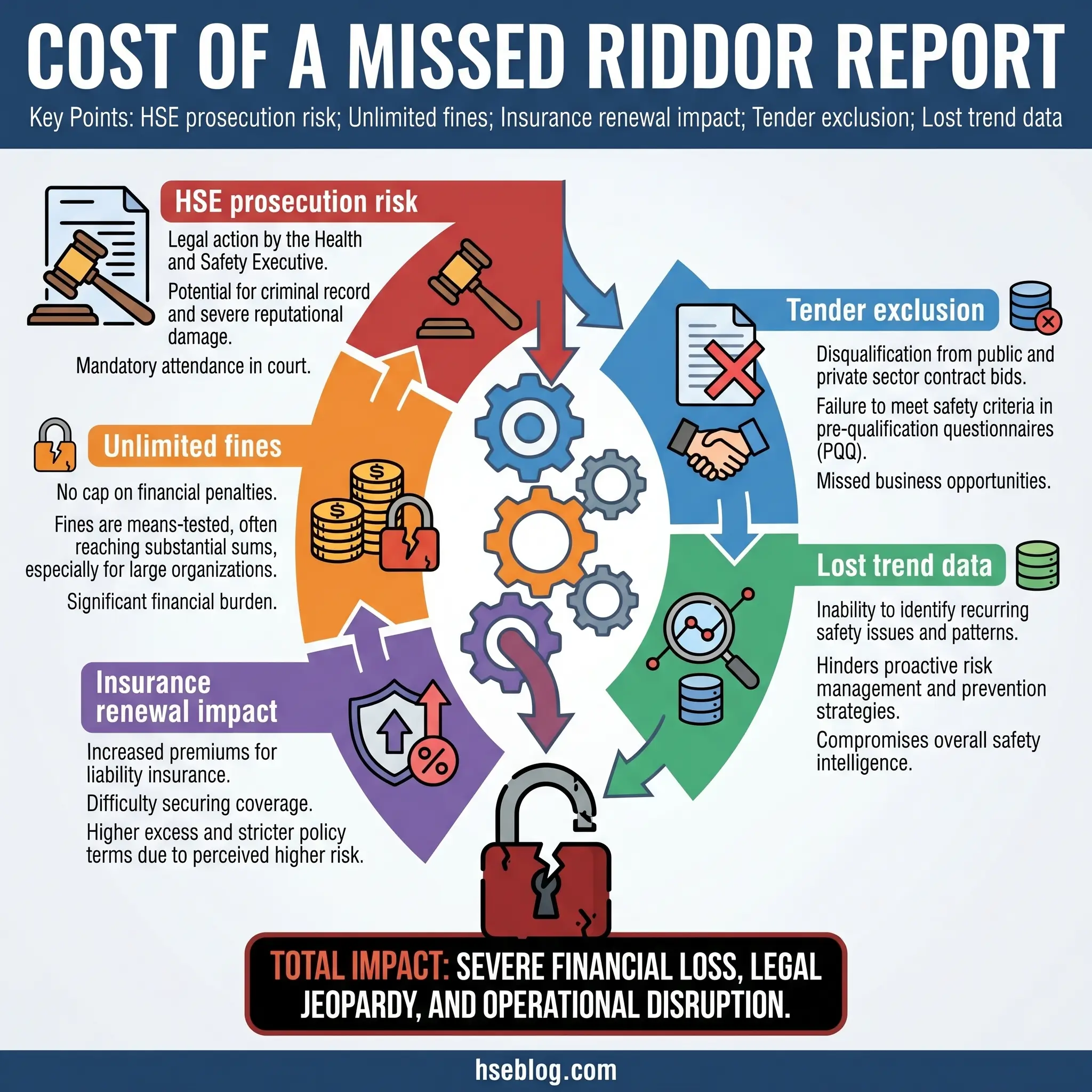
Beyond the legal risk, missed reports distort the national picture. HSE uses aggregated RIDDOR data to set inspection priorities, drive campaigns, and target enforcement. Every missed report is a missing data point that could have informed a safer workplace somewhere else.
How to Report a RIDDOR Injury (Brief Overview)
Once you’ve classified an injury as reportable, the mechanics are straightforward. Use this sequence:
- Gather the core information: dutyholder details, injured person details, date, time, and location of the accident, the nature of the injury, and a description of the cause.
- Choose the right form from the F2508 series on the HSE online reporting portal — there are separate forms for injuries, dangerous occurrences, and diseases.
- For fatalities and specified injuries during office hours, call HSE on 0345 300 9923 as the fastest notification route, then follow up with the written report within 10 days.
- For railway incidents, report to the Office of Rail and Road (ORR) instead of HSE.
- Retain a copy of the submission alongside your accident book entry for at least 3 years under Regulation 12.
Frequently Asked Questions
What Good RIDDOR Compliance Actually Looks Like
Walk any site in the UK and the difference between employers who get RIDDOR right and those who don’t isn’t the paperwork. It’s the classification culture. The ones who report well have trained their supervisors to run the 3-test framework in their heads before writing the first line of an accident book entry. They understand that a wrist fracture crosses a threshold and a finger fracture doesn’t — and they know why. They distinguish between accident book recording, which catches everything, and RIDDOR reporting, which catches a defined subset.
The highest-impact change any employer can make isn’t a new form or a new system. It’s a half-day of supervisor training on the specified injury list and the over-7-day counting rules. Those two topics, understood properly at the supervisory level, close the majority of the gap between the 680,000 self-reported workplace injuries and the 59,219 that reach HSE through formal reports. The regulations aren’t the obstacle. The translation of those regulations into supervisory decision-making is.
Compliance with RIDDOR reportable injuries rules is ultimately about honesty with the data. Every missed report narrows the national picture of how and where UK workers are getting hurt. Every over-report wastes dutyholder time on noise. Getting it right sits in the middle — and the 3-test framework is the cleanest path to that middle ground.