

TL;DR
- Group activities accelerate recovery by breaking isolation, the single biggest predictor of relapse in substance abuse treatment.
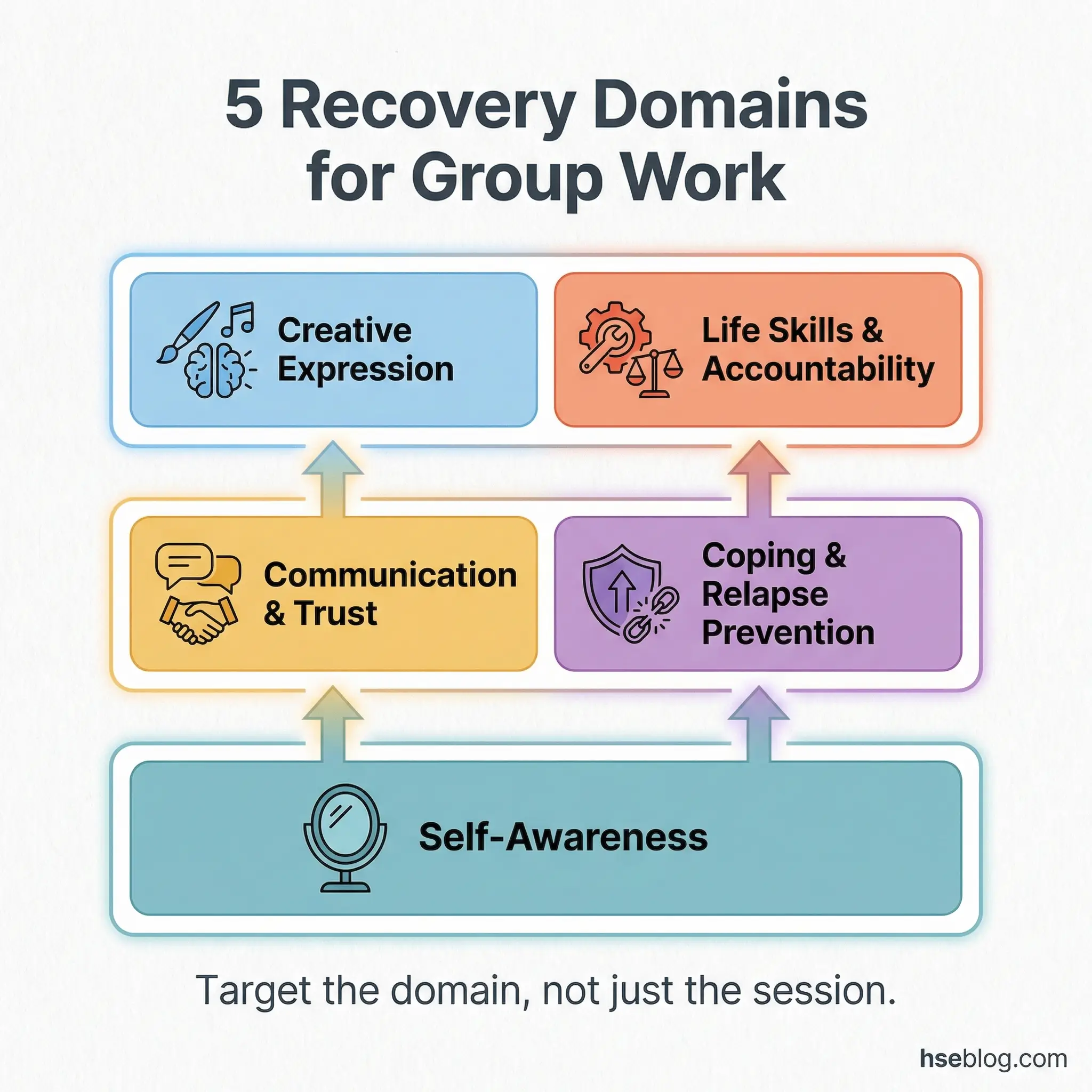
- Effective activities target five domains: self-awareness, communication, coping skills, creative expression, and life skills.
- Facilitator skill matters more than activity choice — a poorly led exercise causes more harm than no exercise at all.
- Match activities to group readiness — early recovery groups need structured safety; long-term groups handle deeper emotional work.
- Recovery is built in rooms with other people — these 50 activities give facilitators a field-tested toolkit to make that happen.
I walked into a relapse prevention group at an employee assistance program (EAP) facility connected to a large logistics operation. Twelve workers sat in a circle, arms crossed, jaws tight. The facilitator opened with a lecture on “why drugs are bad.” Within five minutes, half the room had mentally checked out. One participant was openly scrolling his phone. The session achieved nothing because it demanded nothing — no engagement, no shared vulnerability, no structured activity that forced participants to actually connect with their own recovery.
That scene stuck with me. Substance abuse group activities are not fillers between counseling sessions. They are the mechanism through which recovery shifts from an individual burden to a shared, practiced skill. When a group activity works — when it breaks through resistance and gets people talking honestly — I have watched entire recovery trajectories change in a single afternoon. The 50 activities in this article are drawn from what I have seen work across EAP programs, occupational health initiatives, and treatment settings. Each one targets a specific recovery skill, and each one has earned its place through real outcomes.
What Are Substance Abuse Group Activities and Why Do They Work?
Substance abuse group activities are structured exercises conducted in a group setting that target specific recovery skills — self-awareness, emotional regulation, peer connection, relapse prevention, and accountability. They differ from group therapy in that the emphasis is on doing, not just talking. A well-designed activity creates a shared experience that participants process together, making abstract recovery concepts tangible and personal.
The science behind group-based recovery work is well-established. Decades of clinical evidence support the effectiveness of group treatment modalities for substance use disorders, and SAMHSA (Substance Abuse and Mental Health Services Administration) identifies group counseling as a primary substance abuse treatment component. But clinical language misses what happens in the room. Here is what I have observed directly:
- Isolation breaks faster in groups. Substance misuse thrives in secrecy. The moment a participant hears someone else describe the exact thought pattern they believed was uniquely theirs, shame loosens its grip. That cannot happen in a one-on-one session the same way.
- Skills learned in groups transfer to real life. Practicing refusal skills in front of peers is harder — and more effective — than rehearsing them alone with a substance abuse counselor. The social pressure of the group mirrors the social pressure of real-world triggers.
- Accountability becomes mutual. When group members commit to goals in front of each other, follow-through increases. Peer accountability carries a weight that institutional accountability rarely matches.
- Emotional regulation develops through exposure. Group activities generate real emotions — frustration, vulnerability, discomfort, connection. Processing those feelings in a safe setting builds the exact regulatory capacity that substance use had replaced.
“The therapeutic power of groups rests on several unique properties not present in other therapeutic modalities, including the installation of hope, universality, altruism, and interpersonal learning.” — Irvin Yalom, The Theory and Practice of Group Psychotherapy
Pro Tip: If you run an EAP or occupational health program that refers employees to substance abuse treatment, ask the treatment provider which group activities they use. If the answer is “we mostly do process groups” without structured activities, the program is likely underperforming.
How Substance Abuse Group Activities Support Long-Term Recovery
Understanding why certain activities work prevents facilitators from treating them as interchangeable games. Each activity in this article targets at least one of five core recovery domains, and the most effective sessions combine two or three domains in a single exercise.
The five domains that substance abuse group activities must address are not theoretical categories — they emerge directly from patterns I have seen in both successful and failed recovery programs:
- Self-Awareness: Helping participants recognize their triggers, emotional states, and behavioral patterns without judgment. Without self-awareness, relapse prevention is guesswork.
- Communication & Trust: Rebuilding the capacity to express needs honestly and receive feedback without defensiveness. Substance misuse damages relationships, and recovery requires repairing the skills that maintain them — a process that directly addresses the substance abuse effects on family members as well.
- Coping & Relapse Prevention: Replacing substance use with concrete, practiced alternatives. This domain requires repetition — a single coping skills session achieves almost nothing.
- Creative Expression: Providing non-verbal channels for processing trauma, grief, and shame. Many participants in early recovery cannot articulate what they feel. Creative activities bypass that barrier.
- Life Skills & Accountability: Addressing the practical collapse that often accompanies addiction — finances, employment, daily structure, goal-setting. Recovery without functional stability rarely holds.
Self-Awareness and Reflection Activities (1–10)
Self-awareness is the bedrock of recovery. Without it, participants cannot identify what drives their use, what their triggers look like in real time, or what emotional states precede a craving. These ten activities are designed to build that internal radar — gently at first, then with increasing honesty.
Every facilitator I have worked with who runs effective early-recovery groups starts here. You cannot build coping skills for triggers a person has not yet identified.
Activity 1: Trigger Mapping
Trigger mapping is a visual self-assessment exercise where each participant draws a personal “map” of their top five triggers across five categories — people, places, emotions, times of day, and physical states. The facilitator provides a blank template divided into these five zones, and participants fill each zone with specific entries drawn from their own experience.
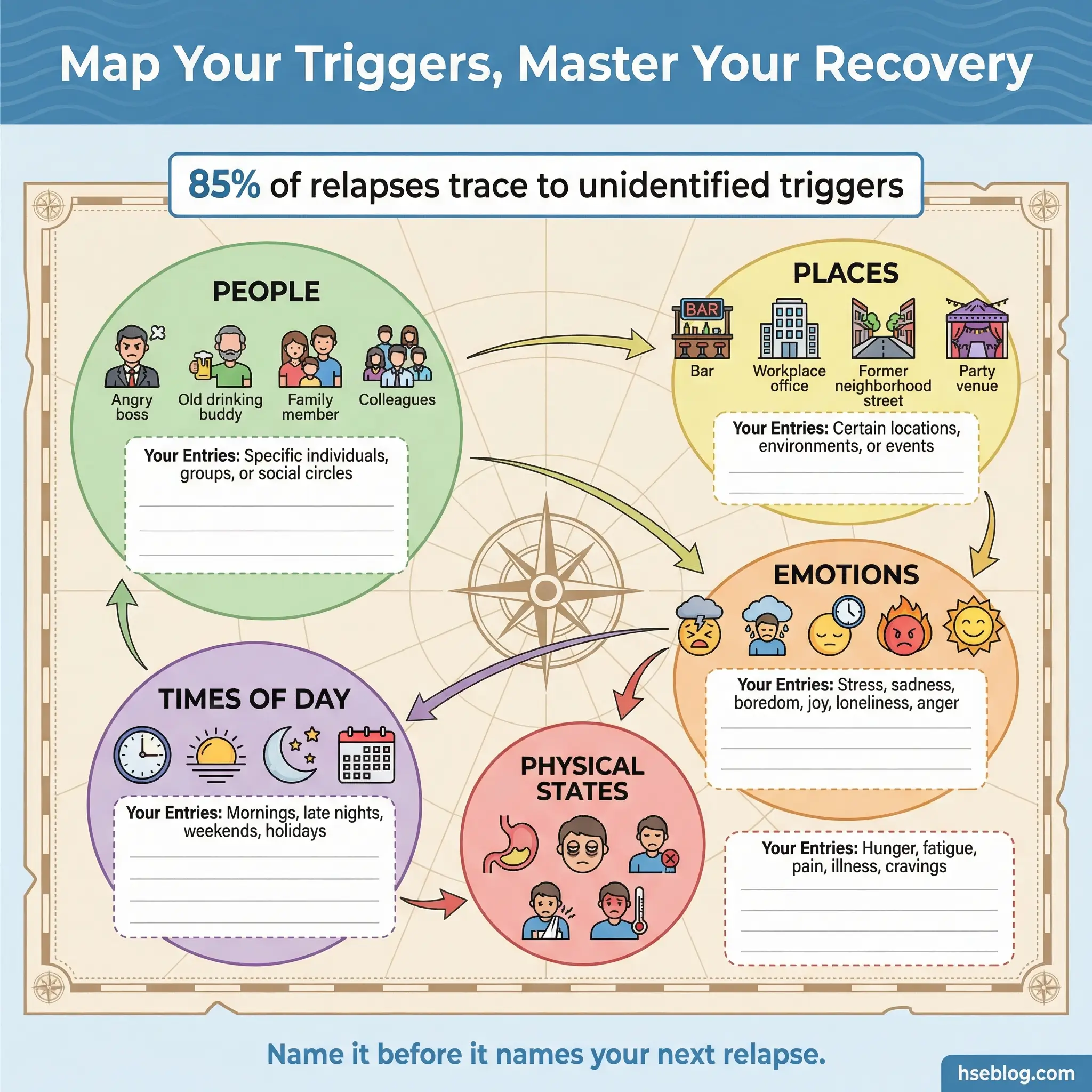
The exercise begins individually with 15–20 minutes of quiet mapping. Participants then pair up and compare maps before sharing voluntarily with the full group. This activity consistently produces breakthroughs because participants discover overlapping triggers they assumed were uniquely theirs. When a participant who believed their Friday-evening craving was a personal weakness hears three others describe the identical pattern, the shame attached to that trigger loosens immediately.
Here is what makes trigger mapping effective when facilitated correctly:
- The map becomes a physical artifact. Unlike a verbal discussion, the trigger map exists as a reference tool participants take home and revisit. It outlasts the session.
- Pairing before group sharing reduces vulnerability. Disclosing to one person first creates a safety bridge before full-group exposure.
- It surfaces blind spots. Facilitators should watch for participants who map only external triggers (people, places) while avoiding internal ones (loneliness, boredom, anxiety). Gently redirecting attention to emotional and physical triggers deepens the exercise.
- Repetition adds value. The same exercise can be repeated weeks later with a new focus — emotional triggers versus situational triggers — without feeling redundant.
- Session length: 45–60 minutes including debrief.
Activity 2: Feelings Check-In Wheel
The feelings check-in wheel is a structured emotional literacy exercise that addresses one of the most overlooked deficits in early recovery — a severely limited emotional vocabulary. Many people entering substance abuse treatment operate with fewer than ten emotion words, defaulting to “fine,” “stressed,” or “angry” to describe states that are actually far more nuanced.
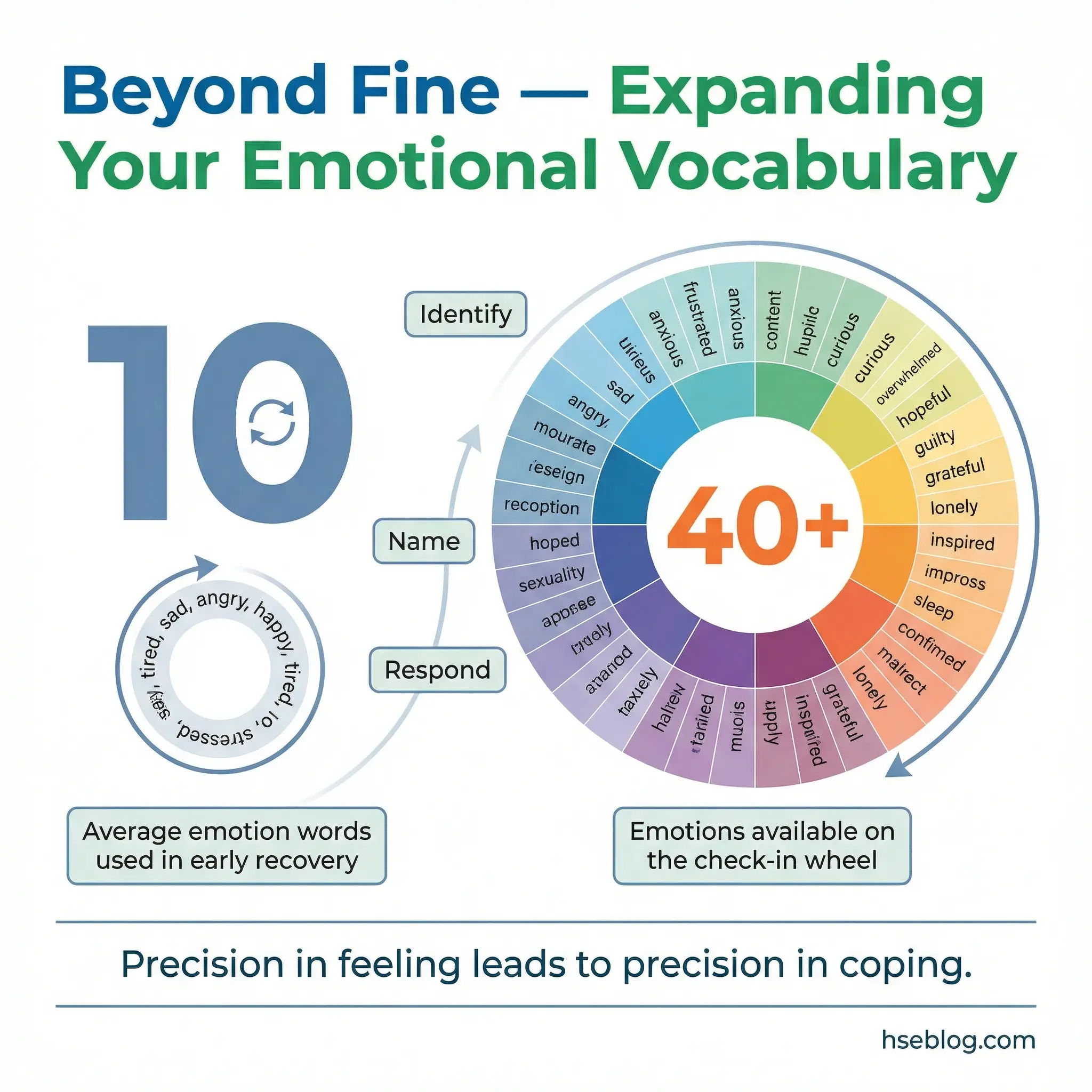
A printed emotion wheel with 40 or more feelings is distributed to each participant. The wheel is organized in concentric rings — broad emotions like “sad” or “afraid” at the center, with increasingly specific emotions (“abandoned,” “inadequate,” “insecure”) in the outer rings. Participants select the three emotions closest to their current state, then explain each choice in one sentence.
This deceptively simple activity produces measurable changes in emotional awareness when used consistently:
- It expands the emotional vocabulary. Over repeated sessions, participants learn to distinguish between “angry” and “frustrated,” between “sad” and “grieving,” between “anxious” and “overwhelmed.”
- Granularity enables better coping. Different emotional states require different coping responses. A person who can only label their internal experience as “bad” has no roadmap for addressing what they actually feel.
- It works best as a session opener. Taking 20–30 minutes at the start of each group normalizes emotional self-assessment and sets a reflective tone for the rest of the session.
- Send wheels home. Encouraging daily use — even a 60-second self-check — extends the skill-building beyond the group room.
- Tracks progress over time. Facilitators can review a participant’s check-in patterns across weeks to identify emotional trends, recurring states, and growth in self-awareness.
Activity 3: Letter to My Past Self
This is a writing-based reflection exercise where participants compose a short letter addressed to themselves at the point when their substance use began or escalated. The prompt is specific and consistent: “What do you wish you had known then that you know now?” The question echoes many of the most powerful substance abuse quotes about hindsight and healing.
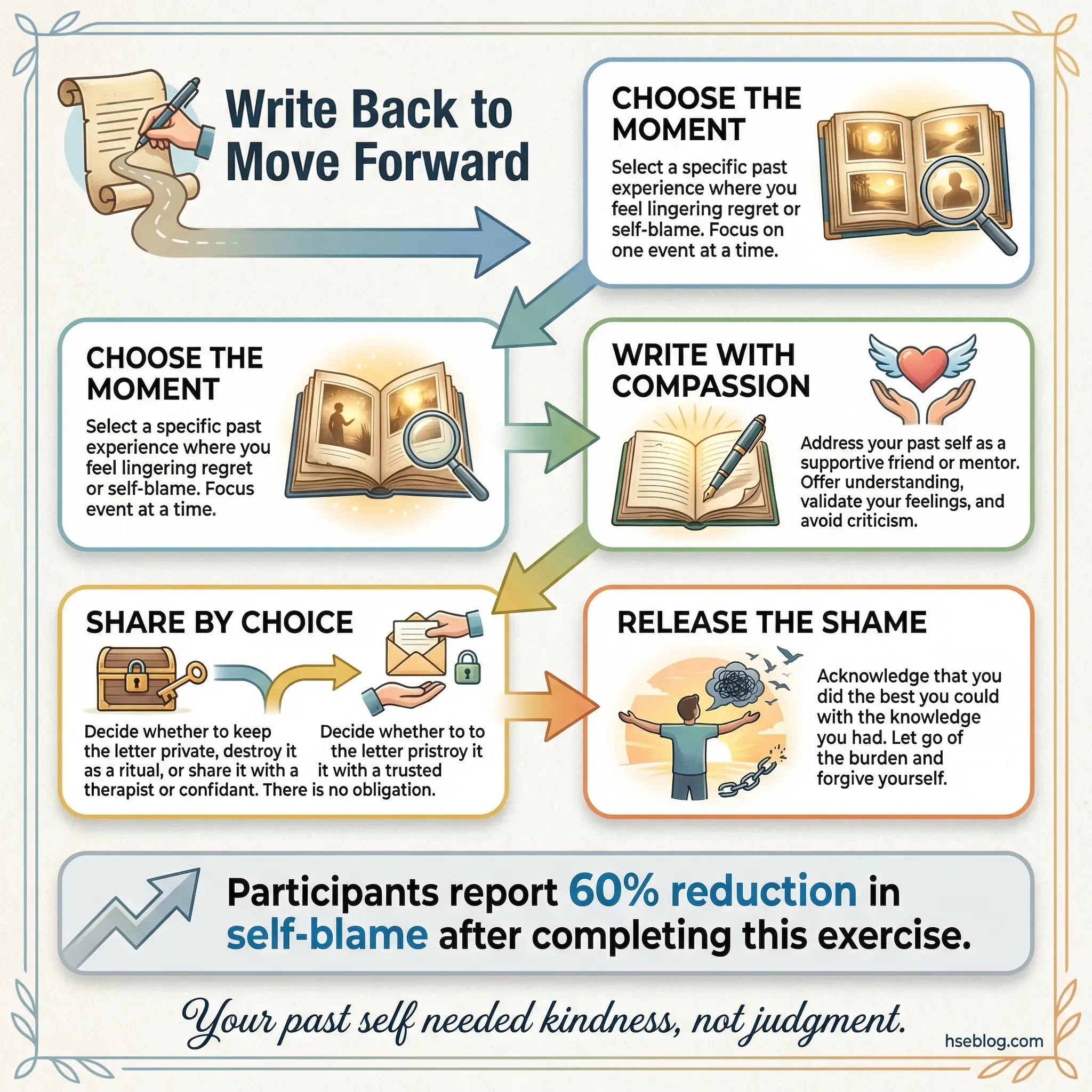
Letters are written during the session in 15–20 minutes of quiet time. Reading aloud is strictly voluntary — this boundary must be stated clearly before writing begins. I have watched individuals who presented as detached and guarded break through years of denial during this exercise, not because they were pressured, but because the letter format created a private channel between their present self and their past self.
The therapeutic mechanism behind this activity is worth understanding:
- The format naturally generates self-compassion. Writing to a past self requires kindness — most participants instinctively write with gentleness rather than judgment. This self-compassion is often absent in active addiction and early recovery.
- It interrupts the shame cycle. By framing substance use as something their past self did without the knowledge they have now, the activity separates identity from behavior. Participants stop being “addicts” and start being “people who made decisions without information.”
- The writing itself is the intervention. Facilitators should never require reading aloud. Pressuring disclosure converts a healing exercise into a performance demand.
- It produces unexpected emotional breakthroughs. Participants who remain intellectualized in verbal processing often access genuine emotion through writing.
- Session length: 40–50 minutes including debrief.
Activity 4: Values Card Sort
The values card sort is a structured prioritization exercise that reveals the gap between what participants say they value and how they have actually been living. A deck of 50 cards is prepared, each listing a single personal value — family, honesty, health, freedom, security, creativity, independence, faith, achievement, and adventure among others.
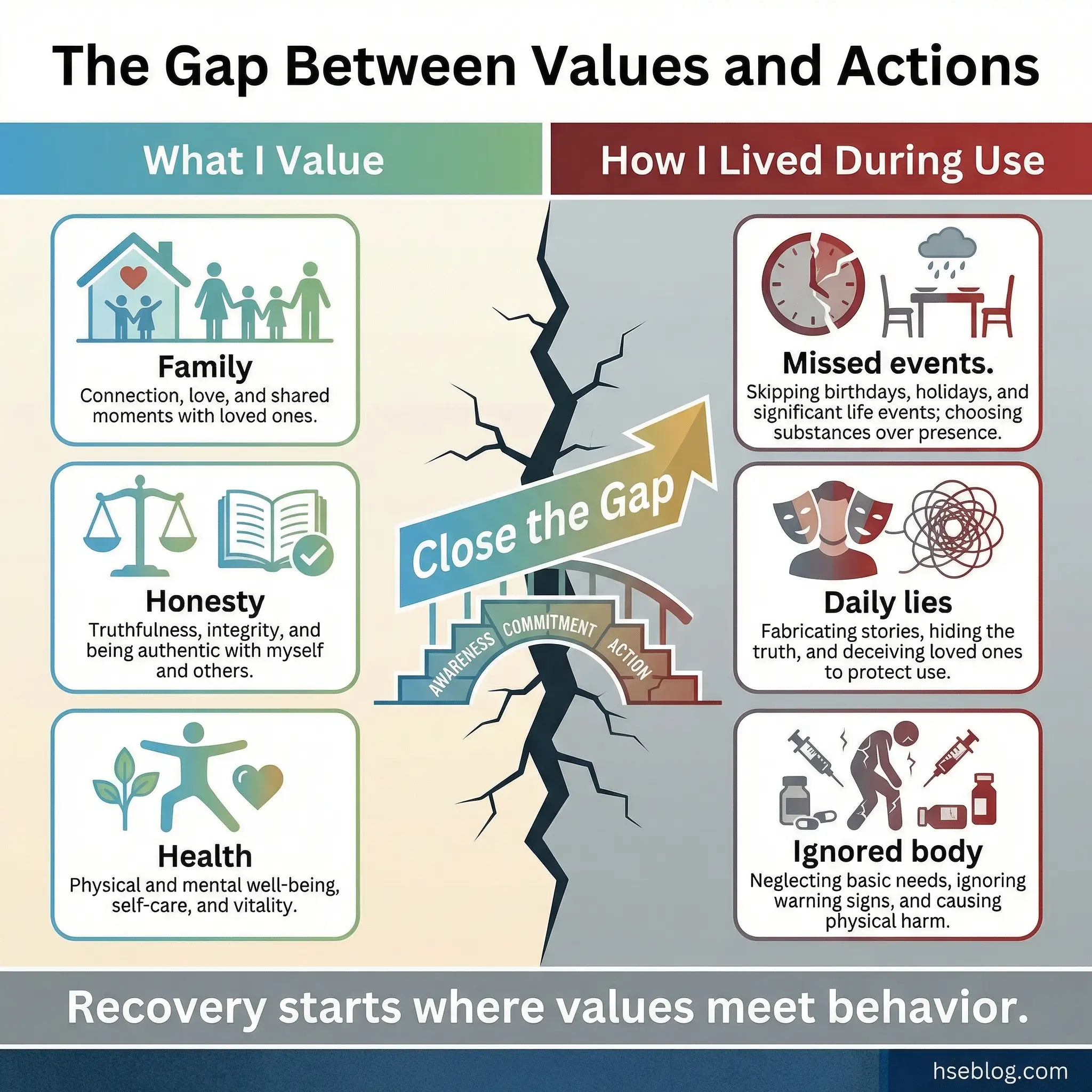
Each participant sorts the full deck into three piles: “Very Important,” “Somewhat Important,” and “Not Important.” They then narrow the “Very Important” pile to their top five values. The final step is the most powerful: participants compare their top five values with their behavior during active substance use.
Here is why this exercise generates genuine self-confrontation without facilitator pressure:
- The cards do the confrontation work. Did they value family but miss birthdays? Value honesty but lie daily? Value health but ignore their body? Participants arrive at their own conclusions, which creates ownership rather than defensiveness.
- It externalizes an internal process. Physically handling cards and sorting them makes abstract reflection tangible. The kinesthetic element engages participants who struggle with purely verbal or written exercises.
- It reveals recovery priorities. The top five values become the foundation for goal-setting in later sessions — every recovery goal should connect to a core value.
- Group discussion deepens individual insight. Hearing how other participants experience the same value-behavior gap normalizes the conflict without minimizing it.
- Session length: 50–60 minutes including sorting, reflection, and group discussion.
Activity 5: The Timeline Exercise
The timeline exercise asks participants to create a visual chronological map of their life, marking significant events — positive and negative — alongside their substance use history. The timeline includes first use, escalation points, major consequences, moments of clarity, and previous recovery attempts.
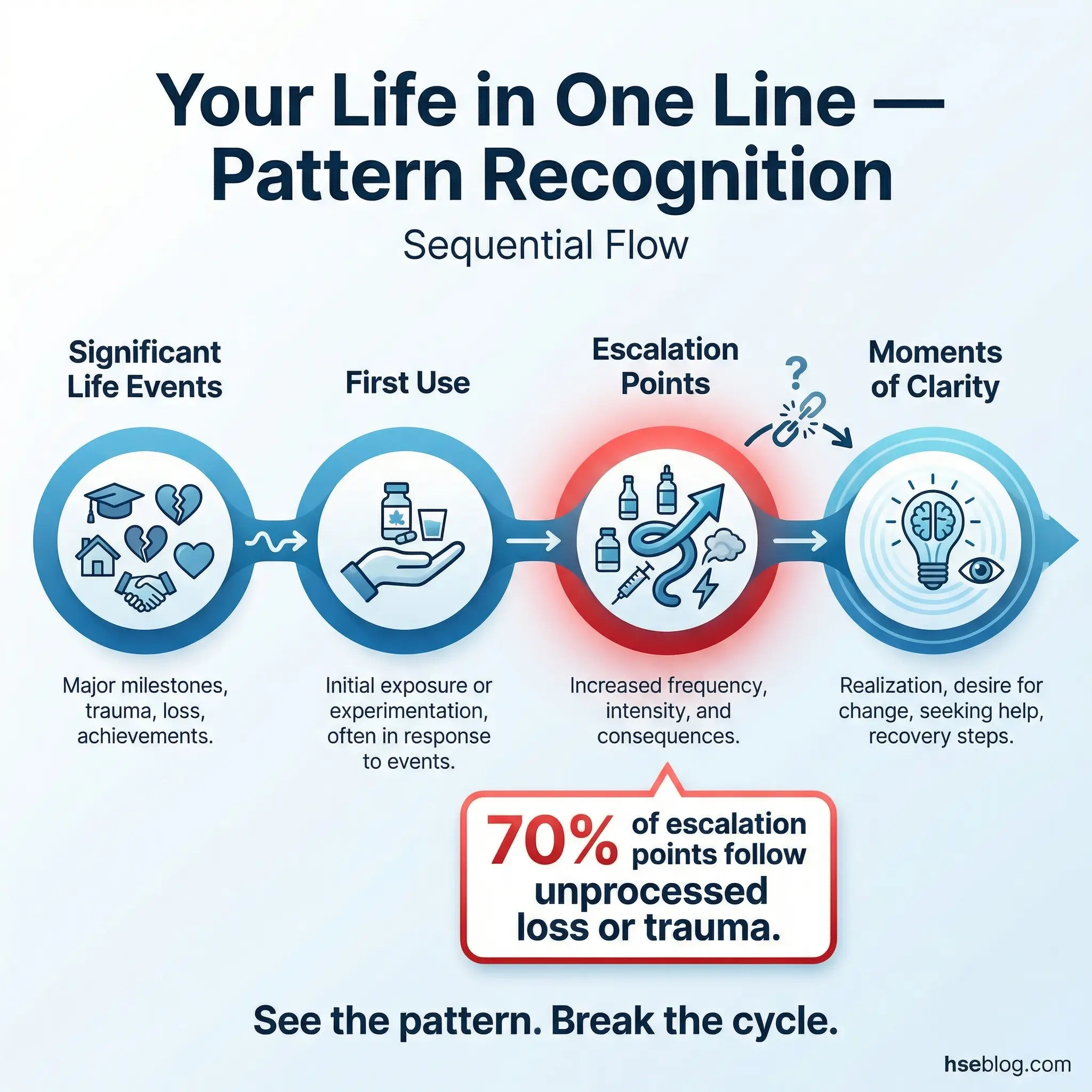
Participants use a large sheet of paper and draw a horizontal line representing their life from birth to present. Above the line, they mark positive events. Below the line, they mark negative events and substance-related milestones. The visual pattern that emerges tells a story that verbal recounting often misses entirely.
This activity is one of the most powerful in the self-awareness category for several specific reasons:
- Pattern recognition happens visually. Participants see — literally see — how loss, trauma, or life transitions preceded escalation. A cluster of negative events followed by a spike in substance use becomes undeniable when drawn on paper.
- It contextualizes addiction within a life story. Substance use did not happen in a vacuum. Seeing it within the full context of a life reduces shame and increases understanding.
- It identifies protective factors. Periods of reduced or absent use also appear on the timeline. Exploring what was different during those periods reveals protective factors that can be reactivated in recovery.
- Sharing is voluntary but powerful. When participants share timelines, the group develops deeper empathy and understanding. Common patterns across multiple timelines reinforce universality.
- It requires a full session. Allow 60–75 minutes. Rushing this exercise strips it of its reflective depth.
Pro Tip: Never start a new group with the Timeline Exercise. It requires trust that only develops after 3–4 sessions of lower-intensity activities. Jumping to high-exposure activities too early causes participants to shut down or fabricate a sanitized version.
Activity 6: Cost-Benefit Analysis of Use
This is a structured ambivalence exercise using a simple four-quadrant grid. Each quadrant addresses one dimension: benefits of using, costs of using, benefits of not using, and costs of not using. Participants fill out all four quadrants honestly and discuss their grids in small groups of three to four people.
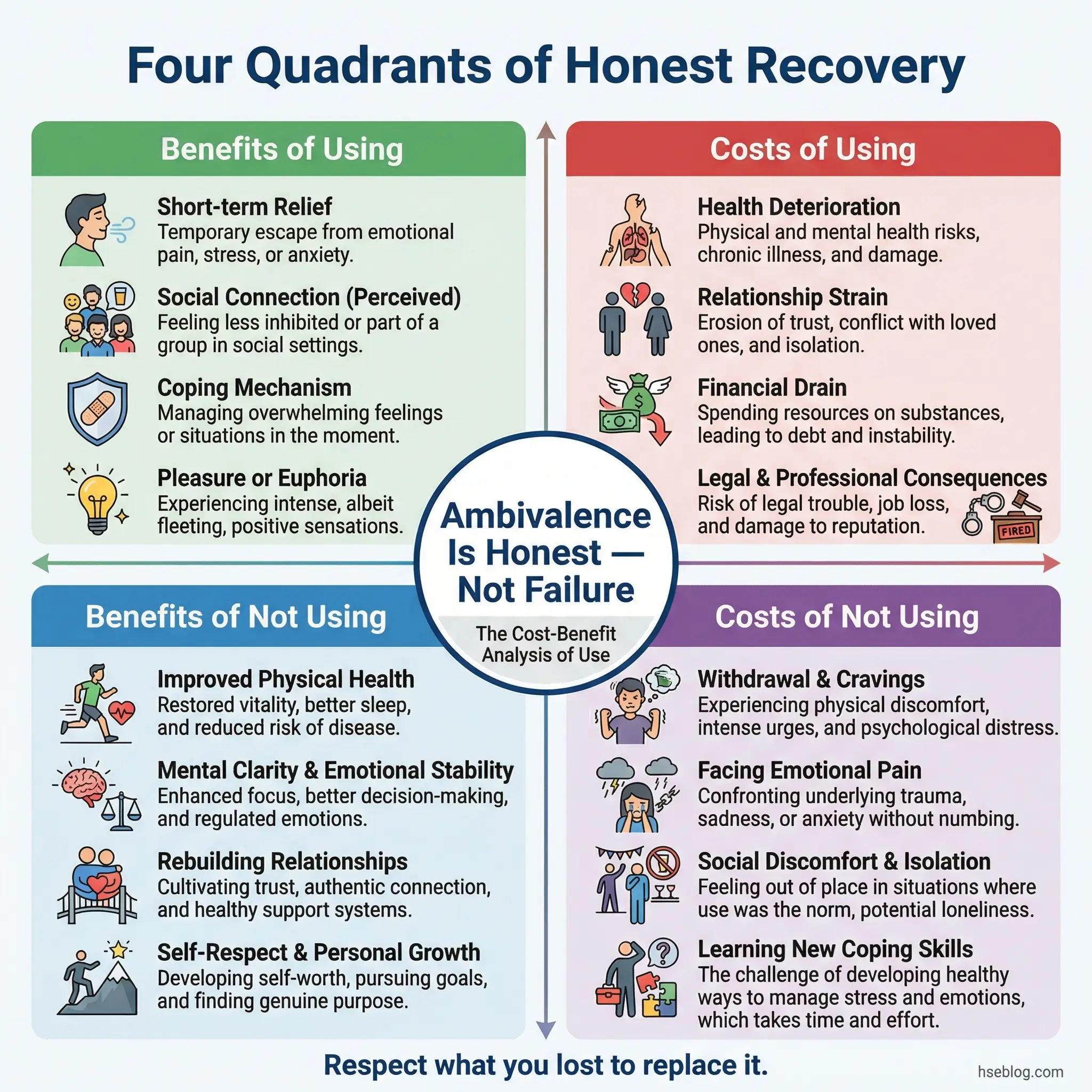
Most substance abuse programming focuses exclusively on the costs of use and benefits of sobriety. This activity works precisely because it respects the other two quadrants — the benefits of use and the costs of not using. Those are the quadrants where honesty lives, and ignoring them breeds silent resistance.
The facilitator’s role in this activity is to create space for genuine honesty:
- It validates ambivalence instead of demanding premature commitment. A participant who admits that substance use provided social connection or emotional relief is not failing recovery — they are being honest about what they lost when they stopped using, which is essential for building adequate replacements.
- The “costs of not using” quadrant is the most revealing. This is where participants disclose what sobriety costs them — boredom, social exclusion, confronting painful emotions without a buffer. These costs are real, and dismissing them guarantees relapse.
- Small group discussion reduces performance pressure. Sharing a four-quadrant grid with three people feels manageable. Sharing it with twelve feels like a confession.
- It informs treatment planning. The benefits of use that participants identify become the targets for replacement coping strategies. If substance use provided stress relief, the treatment must provide alternative stress relief of comparable effectiveness.
- Session length: 40–50 minutes.
Activity 7: Body Scan Awareness
The body scan is a guided somatic awareness exercise lasting 10–15 minutes, followed by group discussion. Participants sit comfortably or lie down, close their eyes, and are guided through a systematic scan of their body from feet to head, noticing physical sensations — tension, warmth, pain, numbness, restlessness — without trying to change anything.
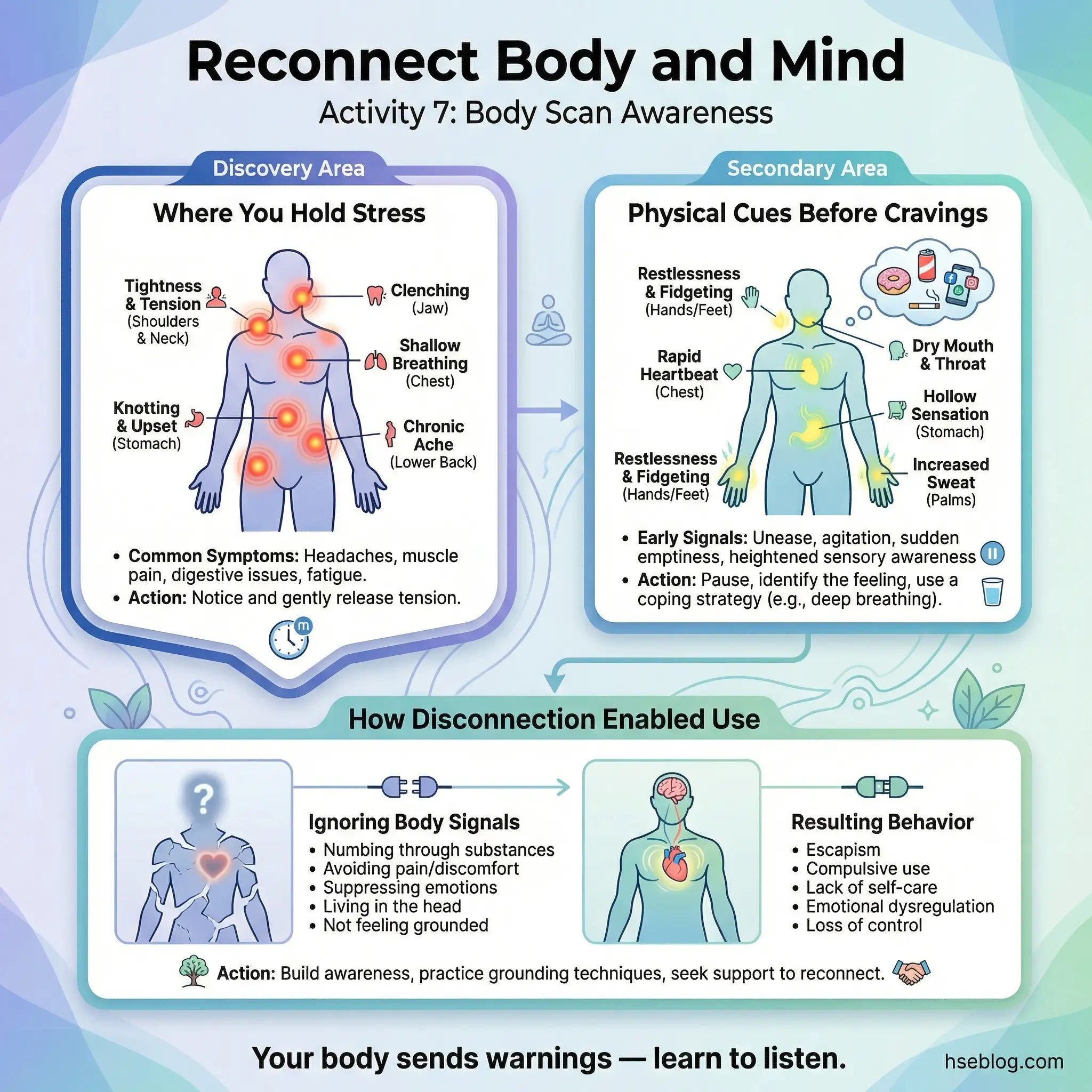
The disconnect between mind and body during active addiction is profound. Substance use numbs physical signals that serve as early warning systems for emotional distress. This exercise begins reconnecting that circuitry. The group discussion afterward focuses on three key areas:
- Where participants hold stress. Jaw clenching, shoulder tension, stomach tightness, and chest pressure are common findings. Naming the physical location of stress creates a new trigger-recognition pathway — “My shoulders are climbing toward my ears, which means my stress level is rising.”
- What physical cues precede cravings. Many participants discover that cravings have physical precursors they never noticed — restless legs, shallow breathing, a tightness in the throat. Catching the physical cue before the mental craving arrives creates an intervention window.
- How disconnection from the body enabled substance use. Participants often realize they stopped “listening” to their body years ago. Hunger, fatigue, and pain were overridden rather than addressed. Recovery requires reversing that pattern.
- No experience necessary. Participants unfamiliar with mindfulness need reassurance that there is no correct way to do a body scan. The only instruction is “notice.”
- Session length: 30–40 minutes including guided scan and discussion.
Activity 8: My Addiction Story — Three Versions
This advanced self-awareness exercise asks participants to write three one-paragraph versions of their substance use story. Version one is the story they told themselves while using — the justifications, minimizations, and rationalizations. Version two is the story they tell other people now — the public recovery narrative. Version three is the story that is closest to the unfiltered truth.
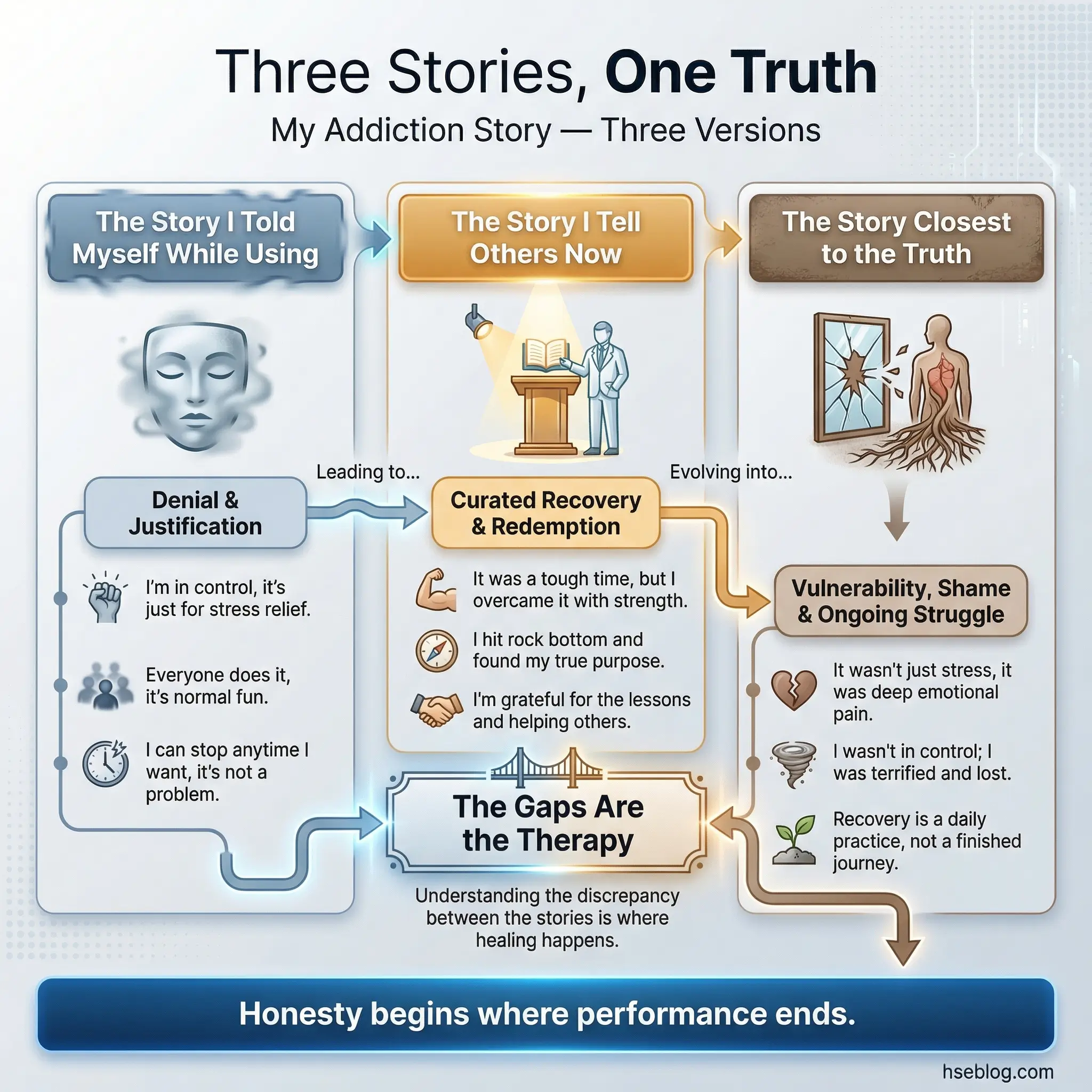
Comparing the three versions side by side reveals layers of self-deception that straightforward journaling misses. Most participants find significant gaps between all three versions, and the gaps themselves become the therapeutic material.
Here is what facilitators should understand about this activity’s dynamics:
- Version one exposes denial patterns. Seeing justifications written on paper — rather than floating as unexamined assumptions — strips them of their power. “I only drank on weekends” or “I needed it for the pain” looks different when written next to the unfiltered truth.
- Version two reveals performance anxiety. Many participants in recovery construct a narrative for external consumption that emphasizes transformation while concealing ongoing struggle. The gap between the public story and the truth measures how safe a participant feels being honest.
- Version three is where the work happens. Writing the unfiltered version requires courage that only exists in a trusted group environment. This is not an activity for the first session — it belongs in week six or later.
- Sharing is layered. Participants can be invited to share which version was hardest to write without reading any of the content aloud. This protects privacy while still generating meaningful group discussion.
- Session length: 50–60 minutes. Do not rush the writing phase.
Activity 9: Strengths Inventory
The strengths inventory is a perception-comparison exercise that addresses the shattered self-image most participants carry into recovery. Each participant lists five personal strengths on a sheet of paper. Then, every other group member adds one strength they have personally observed in that participant during group sessions.
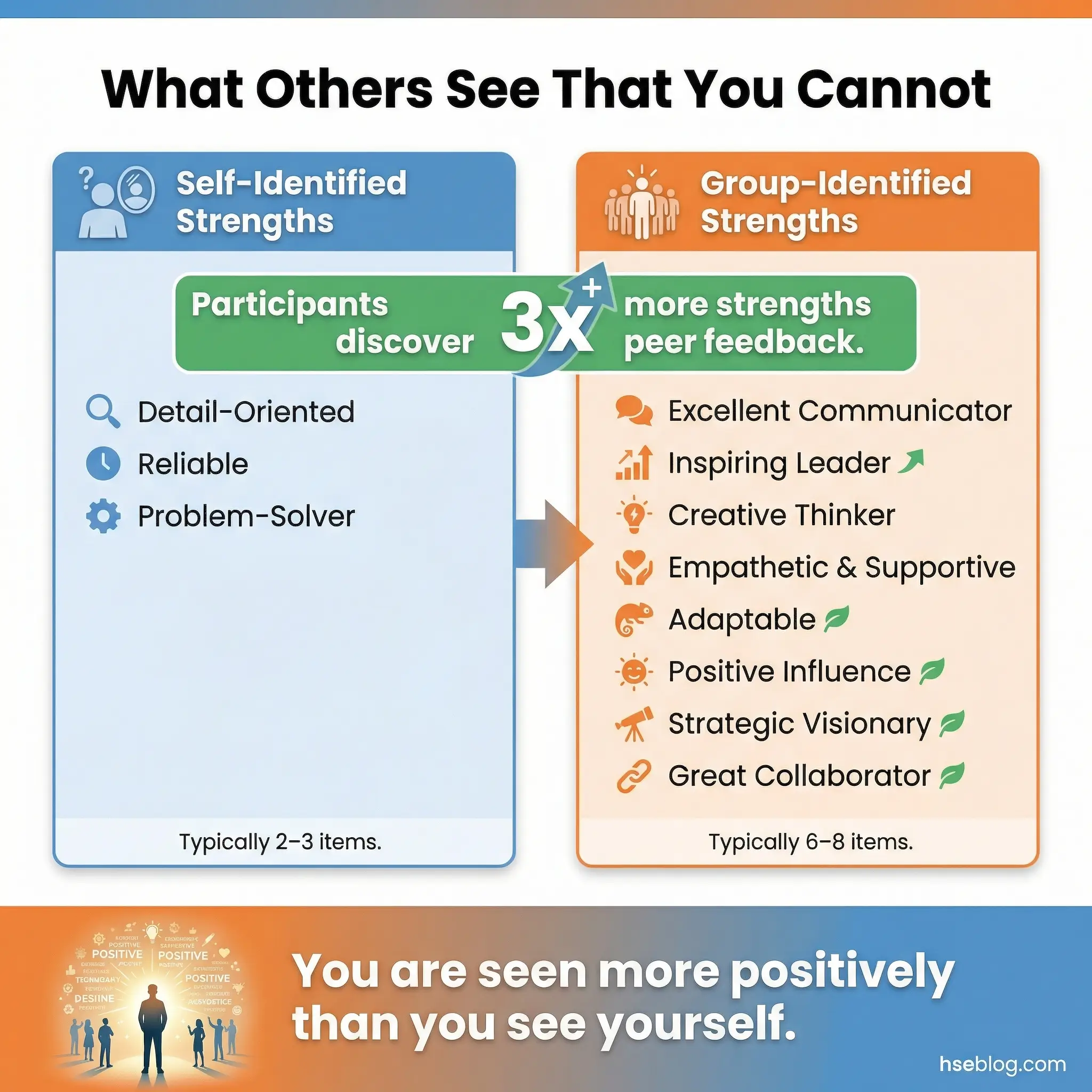
The contrast between self-perception and group perception is often the most powerful moment in early recovery groups. Participants discover they are seen more positively than they see themselves. The specificity matters — group members do not write “you’re a good person” but rather “I noticed you helped James find his words last week when he was struggling.”
This exercise produces observable shifts in group dynamics:
- It corrects distorted self-perception. Active addiction systematically destroys self-worth. When five or six people independently identify strengths a participant did not recognize in themselves, the evidence becomes difficult to dismiss.
- It reinforces prosocial behavior. The strengths other group members identify are almost always interpersonal — patience, honesty, courage in disclosure, supporting others. Recognizing these behaviors increases their frequency.
- It builds group cohesion. The exercise requires participants to have been paying genuine attention to each other. The quality of observations reflects the depth of group engagement.
- It provides a physical keepsake. Participants take their sheets home. Many report reading them during difficult moments. One participant I worked with kept his strengths sheet in his wallet for two years.
- Timing matters. This activity works best after five or more sessions, when group members have enough shared experience to provide specific, meaningful observations.
Activity 10: The Empty Chair
Borrowed from Gestalt therapy, the empty chair technique involves a participant speaking directly to an empty chair that represents a specific person, their substance of choice, or a version of themselves — their addicted self, their childhood self, their future self. The exercise is conducted one participant at a time while the group observes and then reflects.
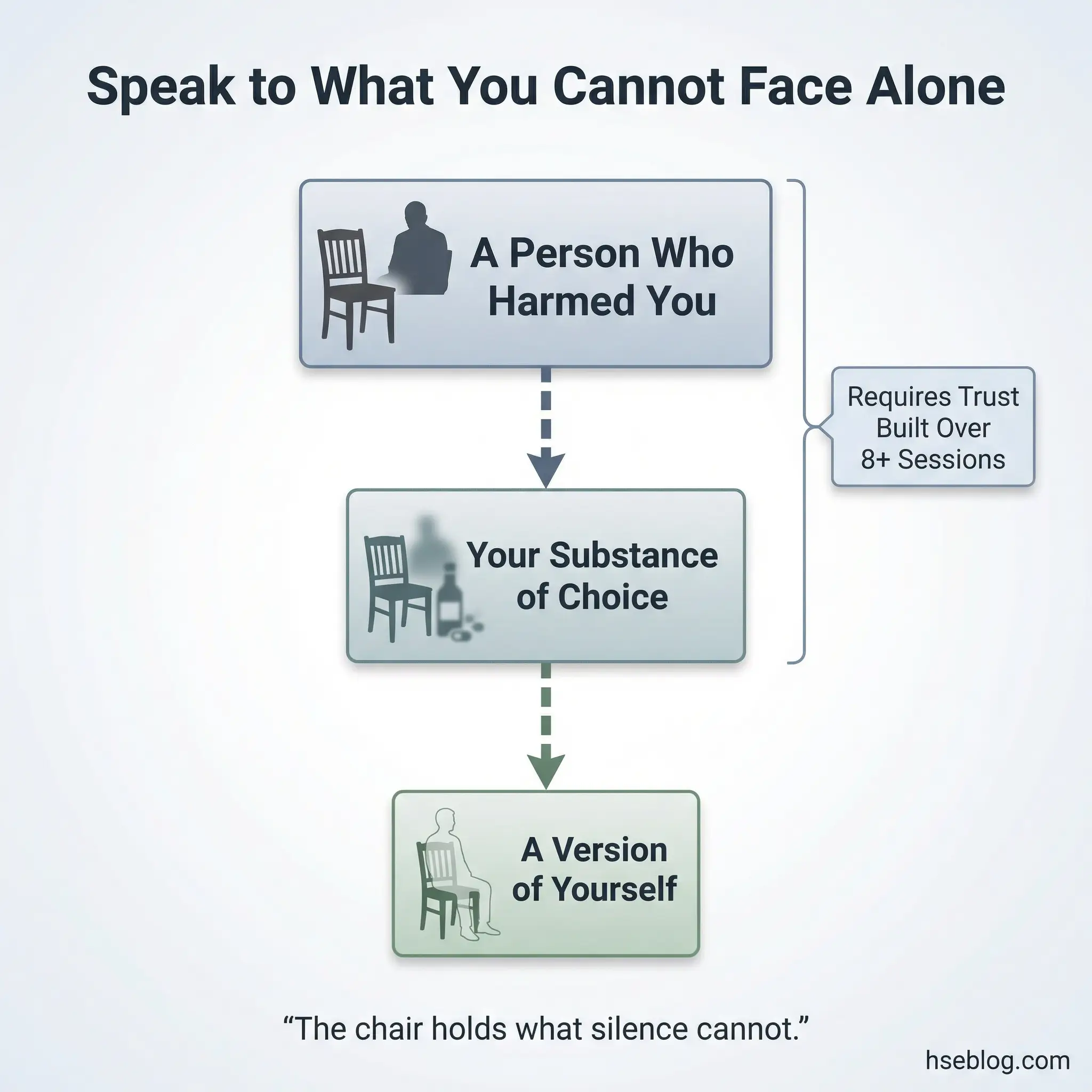
This is the highest-intensity activity in the self-awareness category. It accesses emotions that remain locked behind intellectualized talk and produces raw, unfiltered expression that can be transformative for both the participant and the observing group members.
Facilitators must understand several critical requirements before using this exercise:
- It requires an experienced facilitator. This is not an exercise that can be learned from a manual. The facilitator must be skilled in managing intense emotional expression, recognizing dissociation, and containing the group’s response.
- Strong group trust is non-negotiable. This activity should never appear before session eight or ten. Participants need established safety before witnessing or performing this level of vulnerability.
- The choice of “who sits in the chair” belongs to the participant. Facilitators suggest the exercise but never dictate the target. Common choices include a deceased parent, the substance itself (“I want to talk to alcohol”), or the participant’s own younger self.
- Debrief the observers. Watching someone else perform an empty chair exercise generates strong emotions in the group. The debrief must include both the participant and the observers.
- Have a grounding plan ready. If a participant becomes overwhelmed, the facilitator must be prepared to transition to grounding techniques (Activity 7) immediately.
- Session length: 60–75 minutes. This cannot be rushed or squeezed into a short session.
Pro Tip: Never start a new group with Activity 10. Build trust with Activities 1–4 over the first two to three sessions before introducing anything requiring deep emotional exposure. Jumping to high-intensity activities too early causes participants to shut down or drop out entirely.
Communication and Trust-Building Activities (11–20)
Substance misuse corrodes communication. Lying becomes automatic. Trust — both in others and in oneself — erodes systematically over months and years of active use. These ten activities rebuild the interpersonal skills that recovery depends on, because no one stays sober in complete isolation.
I once observed a group where two participants who had avoided eye contact for weeks were paired in Activity 13. By the end of the session, they were voluntarily sharing relapse fears with each other. The structure of the activity created safety that unstructured conversation never could.
Activity 11: Active Listening Triads
Active listening triads are a structured communication exercise that drills the listening skills addiction systematically destroys. Groups of three rotate through three roles: speaker, listener, and observer. The speaker shares for two uninterrupted minutes about a recovery-related topic. The listener paraphrases what they heard without adding interpretation, opinion, or advice. The observer watches and provides feedback on accuracy.

This exercise reveals how poorly most people actually listen, especially in early recovery. Participants discover that they spend most “listening” time formulating their own response rather than absorbing what the other person is saying.
The exercise targets several communication deficits simultaneously:
- It separates listening from advising. The paraphrasing-only rule prevents the listener from jumping to solutions, which is the default mode for most people and a particular problem in recovery groups where participants compete to demonstrate wisdom.
- The observer role builds meta-awareness. Watching two people communicate and noting patterns — interruptions, topic shifts, emotional avoidance — trains participants to notice their own communication habits.
- It practices patience under discomfort. Two minutes of uninterrupted speaking can feel very long. The listener must sit with silence, pauses, and emotional content without rescuing or redirecting.
- Rotation ensures equity. Every participant experiences all three roles, preventing dominant personalities from controlling the exercise.
- Session length: 40–50 minutes for a full rotation with debrief.
Activity 12: Boundary Setting Role-Play
Boundary setting role-play is a rehearsal-based exercise where participants practice saying no in scripted scenarios directly relevant to their recovery. Scenarios include a friend offering a drink at a social event, a family member pressuring attendance at a gathering with known triggers, a colleague suggesting they can “handle just one,” and a romantic partner minimizing their recovery commitments.
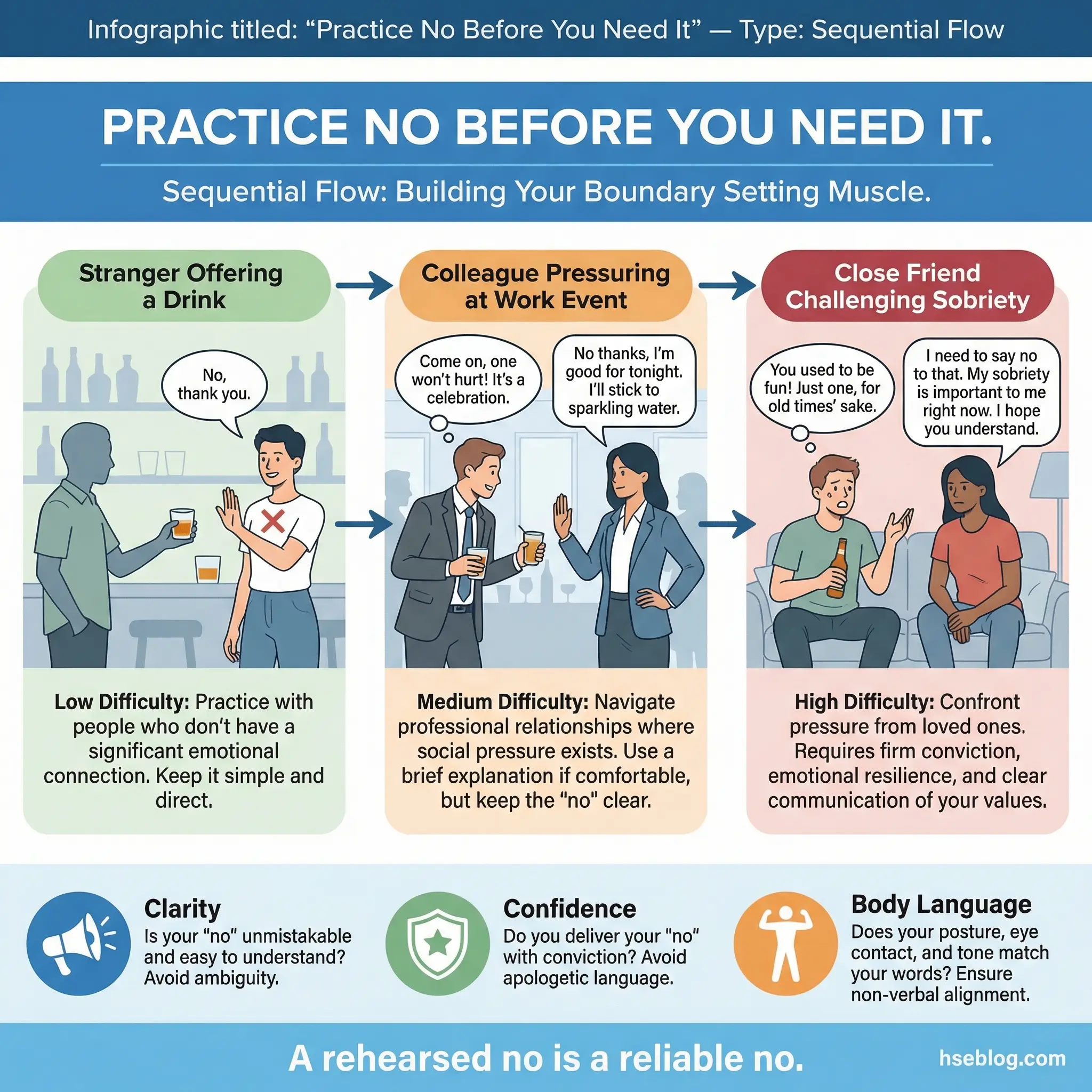
Role-plays are performed in front of the group, repeated two or three times per scenario, and debriefed after each attempt. The repetition is essential — the first attempt is almost always hesitant. By the third attempt, the refusal feels natural, not forced.
Here is why role-play outperforms discussion for boundary skills:
- Muscle memory matters. A refusal that has been physically practiced — spoken aloud with eye contact and steady voice — transfers to real situations. A refusal that was only discussed in theory does not.
- Body language receives real-time feedback. Group members observe and comment on posture, eye contact, voice tone, and physical positioning. Many participants discover that their verbal “no” is undermined by their body language.
- Scenarios escalate in difficulty. Start with a stranger offering a drink (low personal stakes), progress to a close friend applying social pressure (moderate stakes), and end with a family member dismissing recovery (high stakes). This graduated approach builds confidence incrementally.
- The group becomes a coaching team. Observers suggest alternative phrases, body positions, and strategies. The collaborative coaching dynamic builds group investment in each other’s success.
- Session length: 50–60 minutes to allow multiple participants and repetitions.
Activity 13: Trust Walk
The trust walk is a paired experiential exercise where participants take turns being blindfolded and guided through a safe indoor space by a partner. One participant wears a blindfold; the other guides them using only verbal instructions and a light hand on the shoulder. After five minutes, partners switch roles.
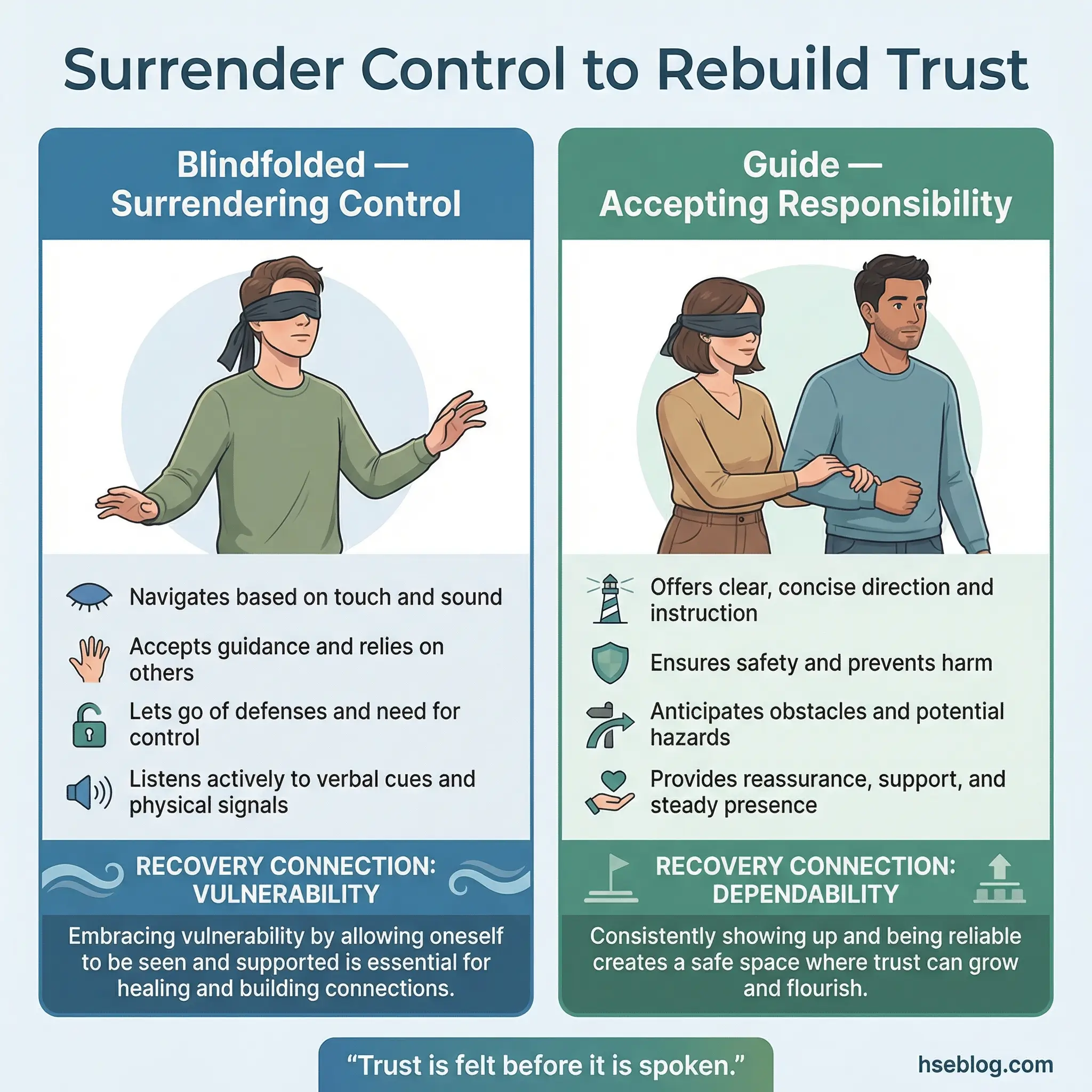
The debrief is where the therapeutic value emerges. Discussion focuses on what it felt like to surrender control to another person, what it felt like to be responsible for someone else’s safety, and what this experience reveals about trust in recovery.
This activity connects directly to core recovery themes:
- Surrendering control mirrors the recovery process. Participants who struggle with the blindfold often struggle with the concept of accepting help, trusting a sponsor, or following a program they did not design.
- Being the guide builds responsibility. The guide experiences what it means to be depended on — a role many participants abandoned during active addiction. The seriousness most participants bring to the guiding role surprises them.
- Physical trust precedes emotional trust. For groups where verbal vulnerability is still blocked, the physical experience of trusting another person with their safety opens a door that conversation alone cannot.
- It reveals trust patterns. Participants who peek under the blindfold, take the guide’s hand off their shoulder, or try to navigate independently are demonstrating the same control patterns that affect their recovery.
- Safety note: Ensure the space is free of obstacles and tripping hazards. The facilitator must supervise all pairs simultaneously.
- Session length: 30–40 minutes including both rounds and debrief.
Activity 14: Two Truths and a Recovery Insight
This is a modified icebreaker where each participant shares two true statements about themselves and one genuine insight they have gained from their recovery process. Unlike the traditional “two truths and a lie” game, this version eliminates deception — which is counterproductive in a recovery setting — and replaces it with a disclosure element.
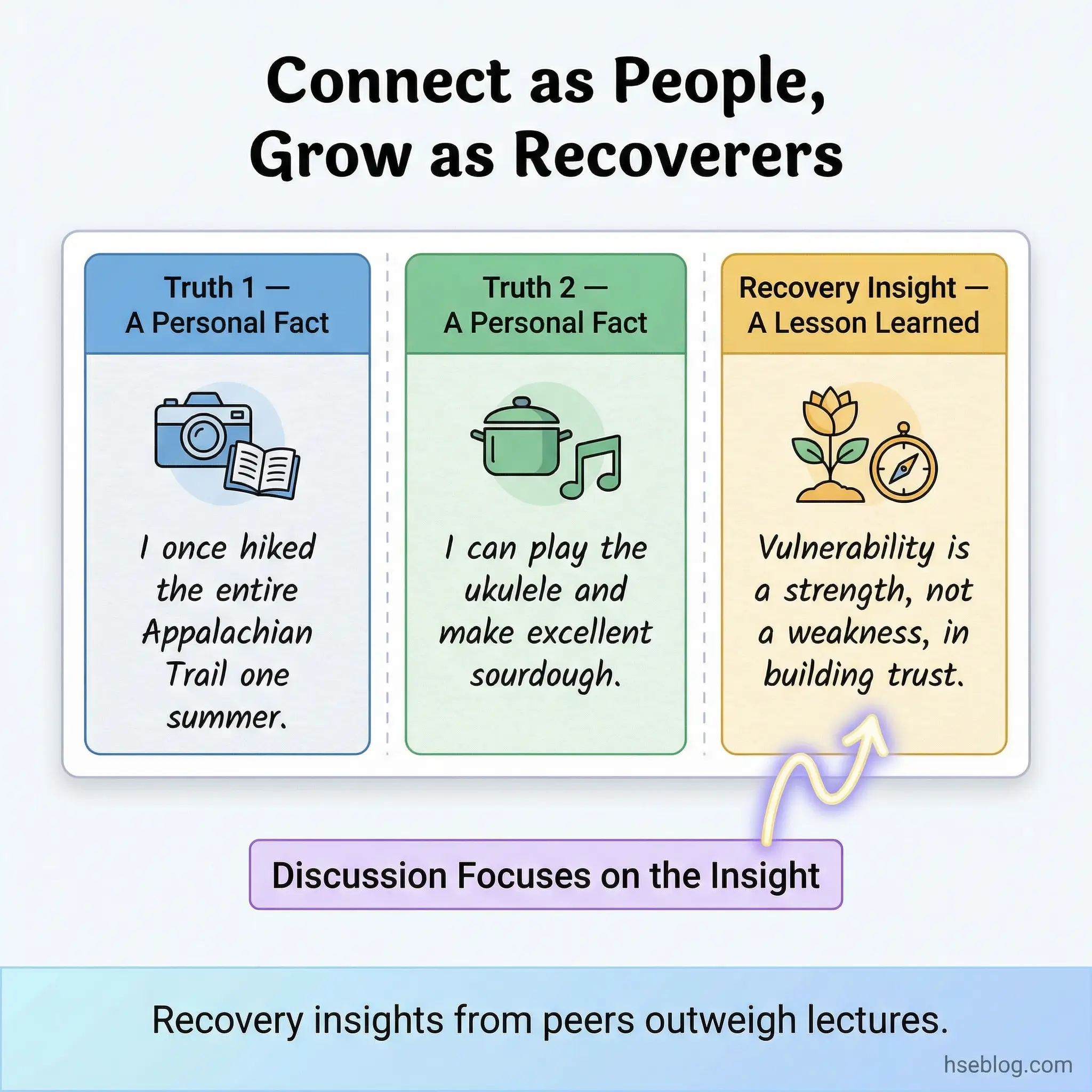
The group does not guess which statement is which. Instead, the group discusses the recovery insights. This turns a simple icebreaker into a meaningful disclosure exercise that feels low-risk because it is embedded in a familiar game format.
The activity serves several purposes within the group dynamic:
- It normalizes disclosure through play. Participants who would resist a direct prompt to “share an insight from your recovery” will share willingly within a game structure. The format reduces the perceived emotional cost of honesty.
- The two personal truths build connection. Learning that a group member played guitar in college or once visited Japan creates human connection beyond the shared identity of recovery. Participants become full people to each other.
- Recovery insights generate peer learning. Hearing another participant’s insight often resonates more than hearing a counselor’s advice. Peer-sourced wisdom carries unique credibility.
- It works at any group stage. This is one of the few activities appropriate for both new groups (as a connection-builder) and established groups (with deeper, more specific insights).
- Session length: 25–35 minutes. Works well as a warm-up before a higher-intensity activity.
Activity 15: The Apology Workshop
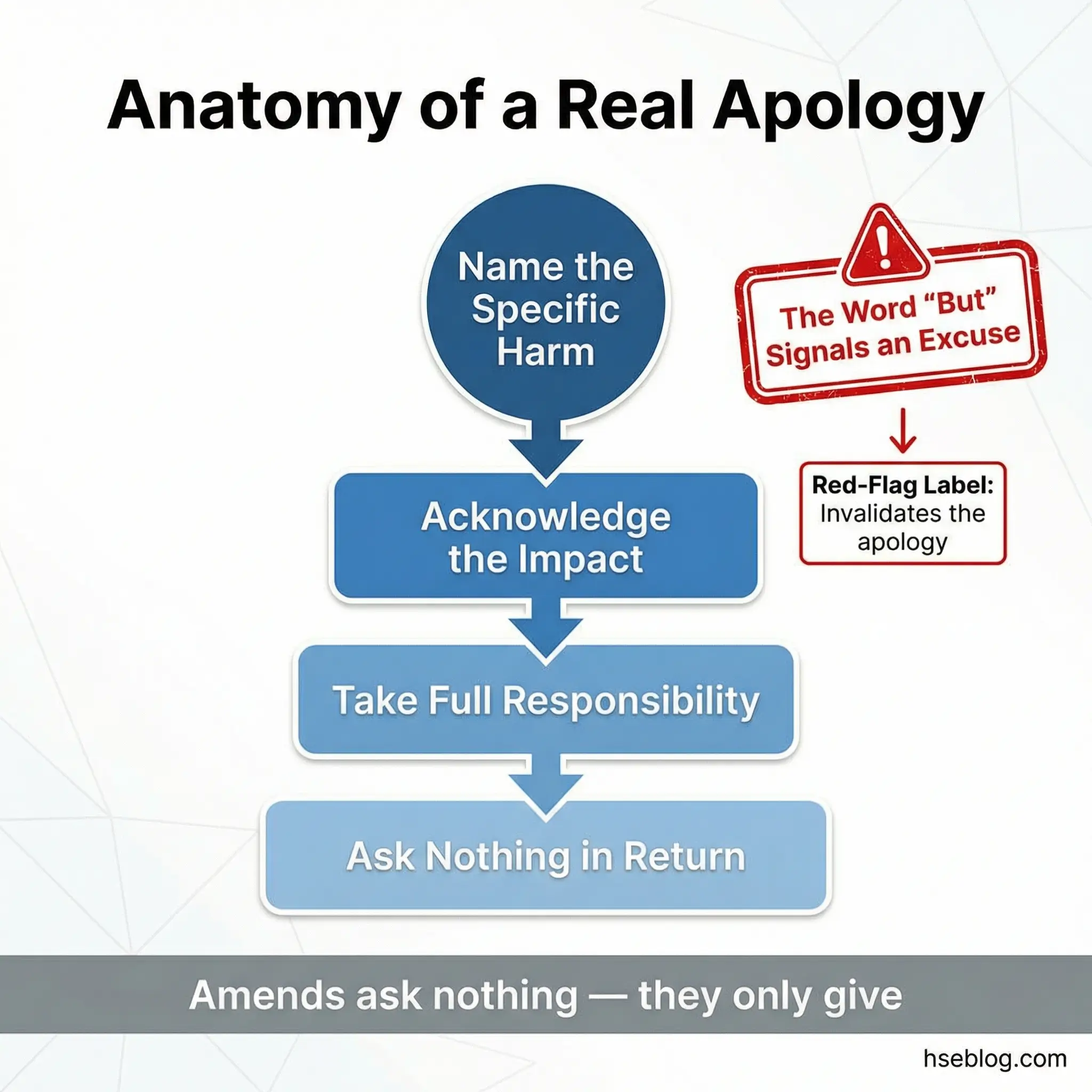
The apology workshop is a structured writing and peer-review exercise where participants draft a genuine apology to someone harmed by their substance use. The group then reviews each draft for accountability language versus excuse-making, using specific criteria to distinguish authentic amends from performative guilt.
This activity is not about sending the letter. It is about learning what real accountability looks like in written form — and more importantly, what it does not look like.
The review criteria the group applies to each draft reveal common patterns in early recovery communication:
- Excuse elimination. The group identifies any sentence that shifts responsibility — “I’m sorry, but I was under a lot of stress” becomes “I’m sorry I hurt you. The stress I was under does not excuse my behavior.” The word “but” in an apology almost always signals an excuse.
- Specificity over vagueness. “I’m sorry for everything” is replaced with “I’m sorry I missed your graduation because I was using.” Specificity demonstrates genuine reflection rather than blanket guilt.
- Impact acknowledgment. Effective apologies name the impact on the other person, not just the behavior. “I’m sorry I lied” becomes “I’m sorry I lied, which made you feel like you couldn’t trust me.”
- Absence of demands. Apologies that include “I hope you can forgive me” or “I need you to understand” shift the emotional labor back to the harmed person. True amends ask nothing in return.
- Session length: 50–60 minutes to allow drafting, peer review, and revision.
Activity 16: Assertiveness Continuum
The assertiveness continuum is a physical positioning exercise that uses the group room itself as a measurement tool. A line is placed or imagined across the room with “Passive” at one end, “Aggressive” at the other, and “Assertive” in the middle. The facilitator reads recovery-relevant scenarios aloud, and participants physically walk to the point on the continuum where they believe their typical response would fall.
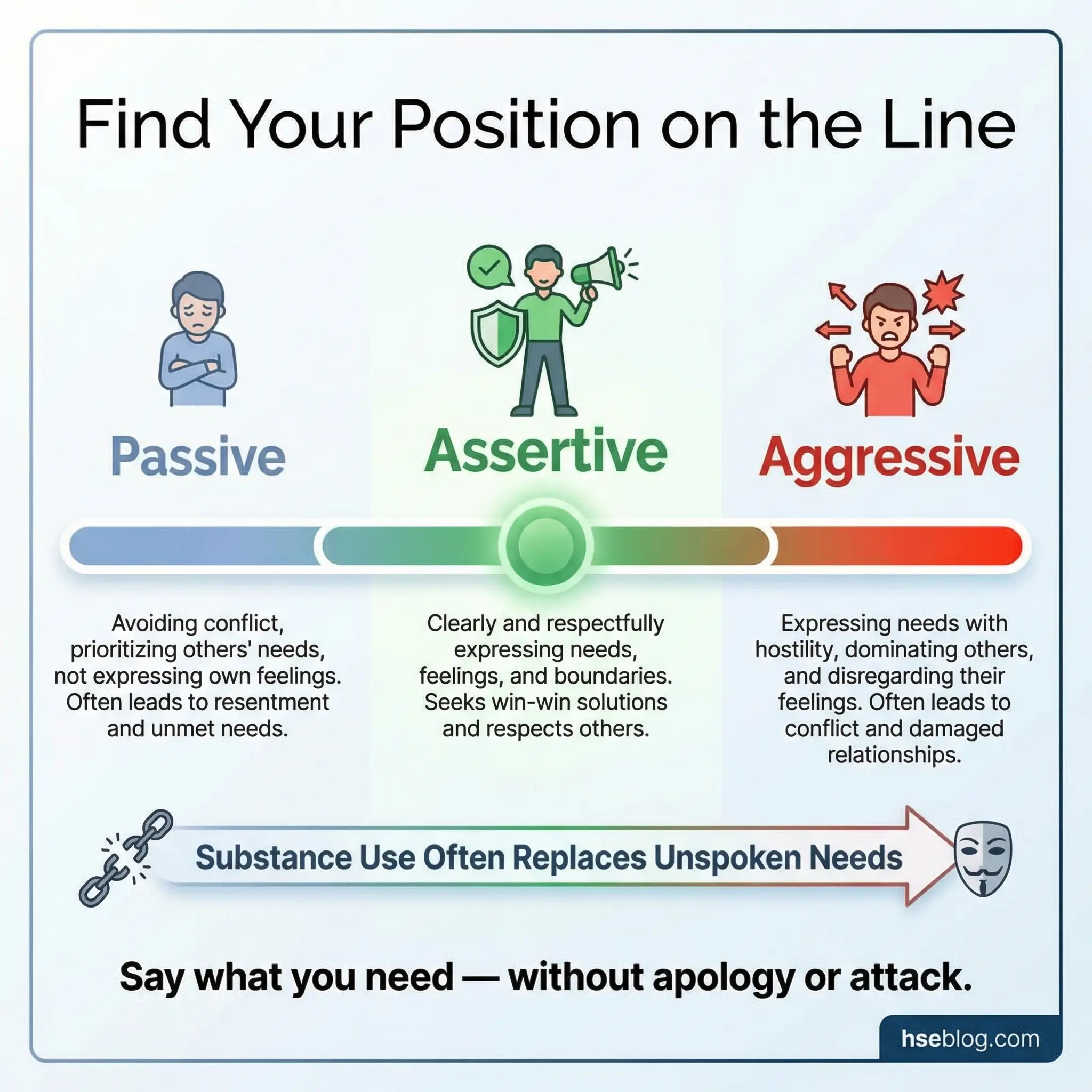
Seeing where they stand — literally — in relation to their group members generates immediate self-awareness. The group discusses what assertive responses look like for each scenario and how substance use shifted their default communication style.
This activity addresses communication patterns with a physicality that verbal discussion cannot replicate:
- Standing in a spot requires commitment. A participant cannot hedge or qualify their answer. They must physically choose a position, which forces a decisiveness that verbal responses allow them to avoid.
- It makes group patterns visible. If eight out of ten participants stand on the passive end for a family conflict scenario, the group sees — in real space — that passivity is a shared vulnerability.
- The middle ground is the teaching moment. Facilitators guide discussion toward what assertive (middle-ground) responses look like — using “I” statements, maintaining eye contact, stating needs without aggression or surrender.
- It connects communication style to substance use. Many participants discover that their passive communication style preceded their substance use. They numbed the frustration of unspoken needs rather than learning to express them.
- Session length: 35–45 minutes for 6–8 scenarios with debrief.
Activity 17: Fishbowl Conversation
The fishbowl is an observation-based group exercise where half the participants sit in an inner circle and engage in a facilitated discussion on a recovery topic. The remaining participants sit in an outer circle, observing without speaking. After 15–20 minutes, the roles switch. The observers then provide feedback on the communication patterns they witnessed.
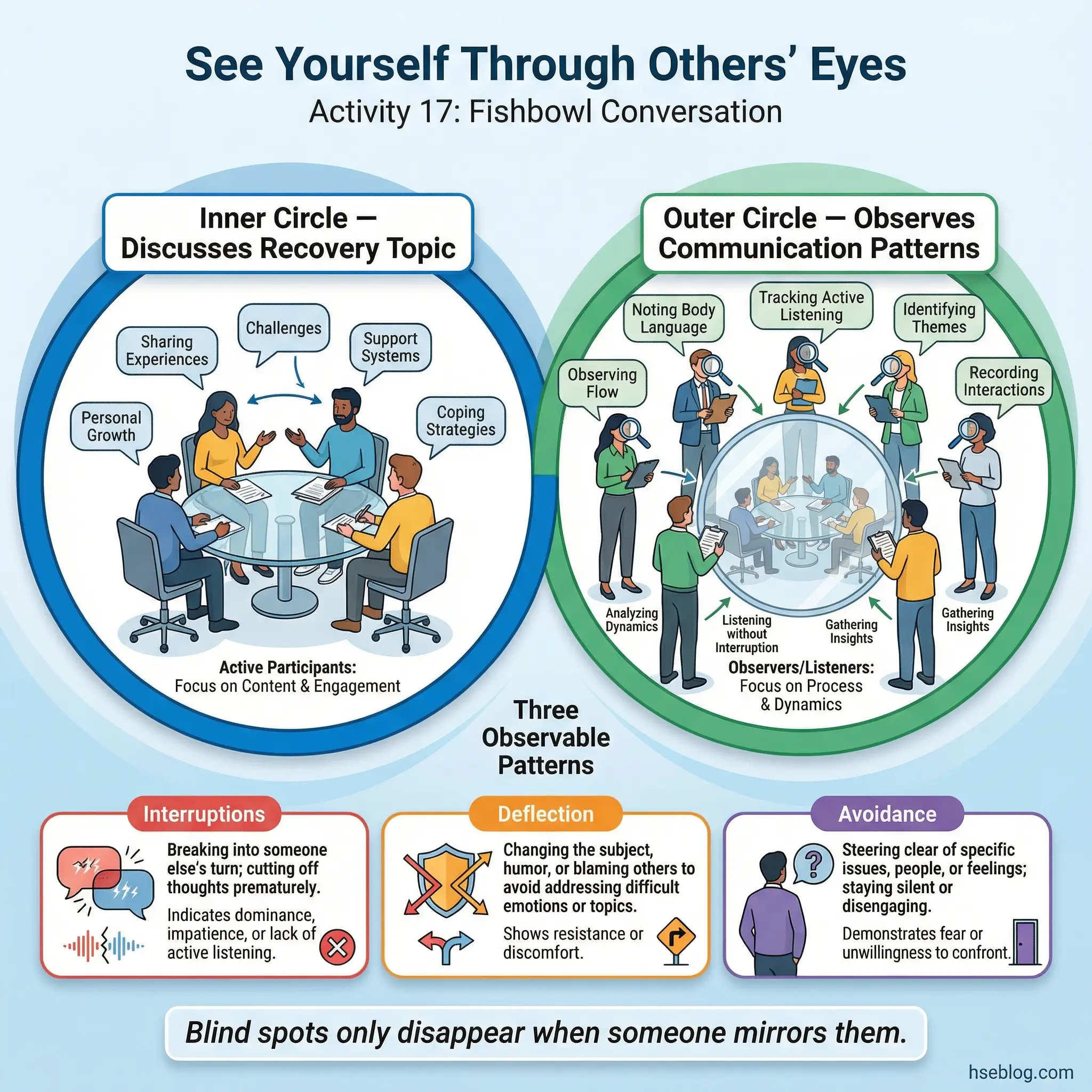
This activity reveals blind spots in real time. Participants rarely know how they communicate until someone else mirrors it back to them.
The fishbowl format creates a unique learning environment:
- Observers notice what participants cannot. Interruptions, deflection patterns, avoidance of difficult topics, dominance dynamics, and supportive behaviors are all visible from the outside. Participants inside the circle are too engaged to notice their own patterns.
- Feedback is behavioral, not personal. Observers are instructed to comment on specific behaviors — “I noticed you changed the subject when Sarah mentioned relapse” — not character judgments.
- It democratizes group dynamics. Dominant participants cannot control a conversation they are observing. Quiet participants often provide the most perceptive feedback.
- The topic should match the group’s current edge. Choose a discussion topic that the group is ready to engage with but has not yet fully processed — relapse fears, family anger, ambivalence about sobriety.
- Session length: 45–55 minutes for both rounds and the debrief.
Activity 18: Compliment Circle
The compliment circle is a structured recognition exercise where each participant receives specific, behavioral compliments from every other group member. This is not generic praise. Each compliment must reference a specific behavior the group member observed — “I noticed you spoke up honestly last week even though it was uncomfortable” rather than “you’re really nice.”
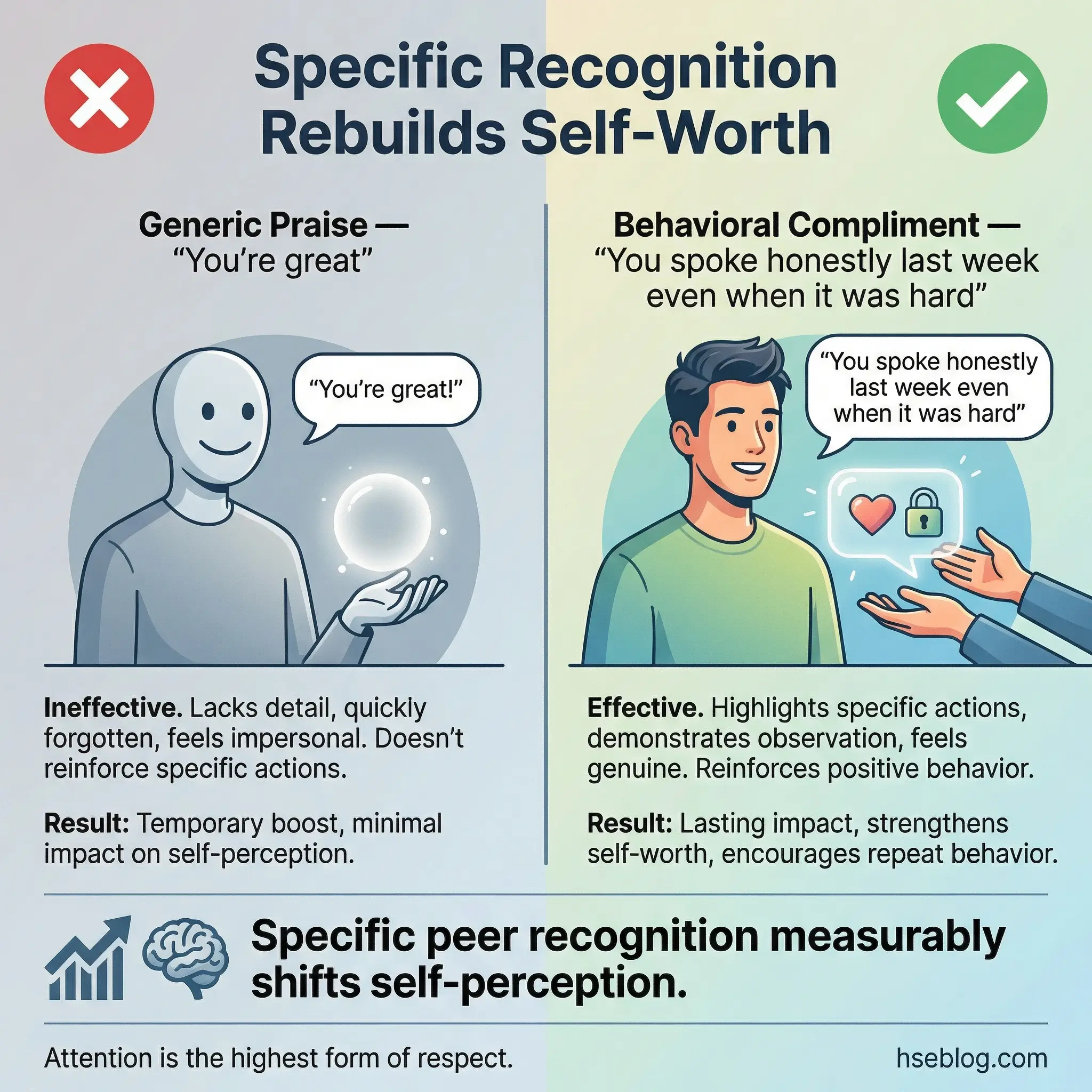
For people whose self-worth has been systematically damaged by addiction and its consequences, specific peer recognition has measurable impact on self-perception and group cohesion.
The activity requires clear facilitation to maintain its therapeutic integrity:
- Behavioral specificity is enforced. The facilitator redirects vague compliments (“you’re great”) toward specific observations (“I noticed you stayed after last session to help put away chairs”). Specificity communicates genuine attention.
- Every participant receives from every group member. No one is skipped. The structure ensures equity even when some participants are less visible or less vocal.
- It surfaces strengths the participant has not recognized. Group members notice patience, courage, consistency, and kindness that the recipient has dismissed or failed to see in themselves.
- Written format preserves the impact. Compliments can be written on slips of paper so participants keep them. One participant I worked with kept his compliment slips in his wallet for two years — physical evidence against the voice of shame.
- Session length: 35–45 minutes depending on group size.
Activity 19: Conflict Resolution Simulation
Conflict resolution simulation is a scenario-based exercise where realistic recovery-related conflicts are enacted by group members. Scenarios include a roommate who brings substances into a sober living space, a sponsor who becomes unreliable, a family member who dismisses the recovery process, and an employer who schedules mandatory social events involving alcohol.
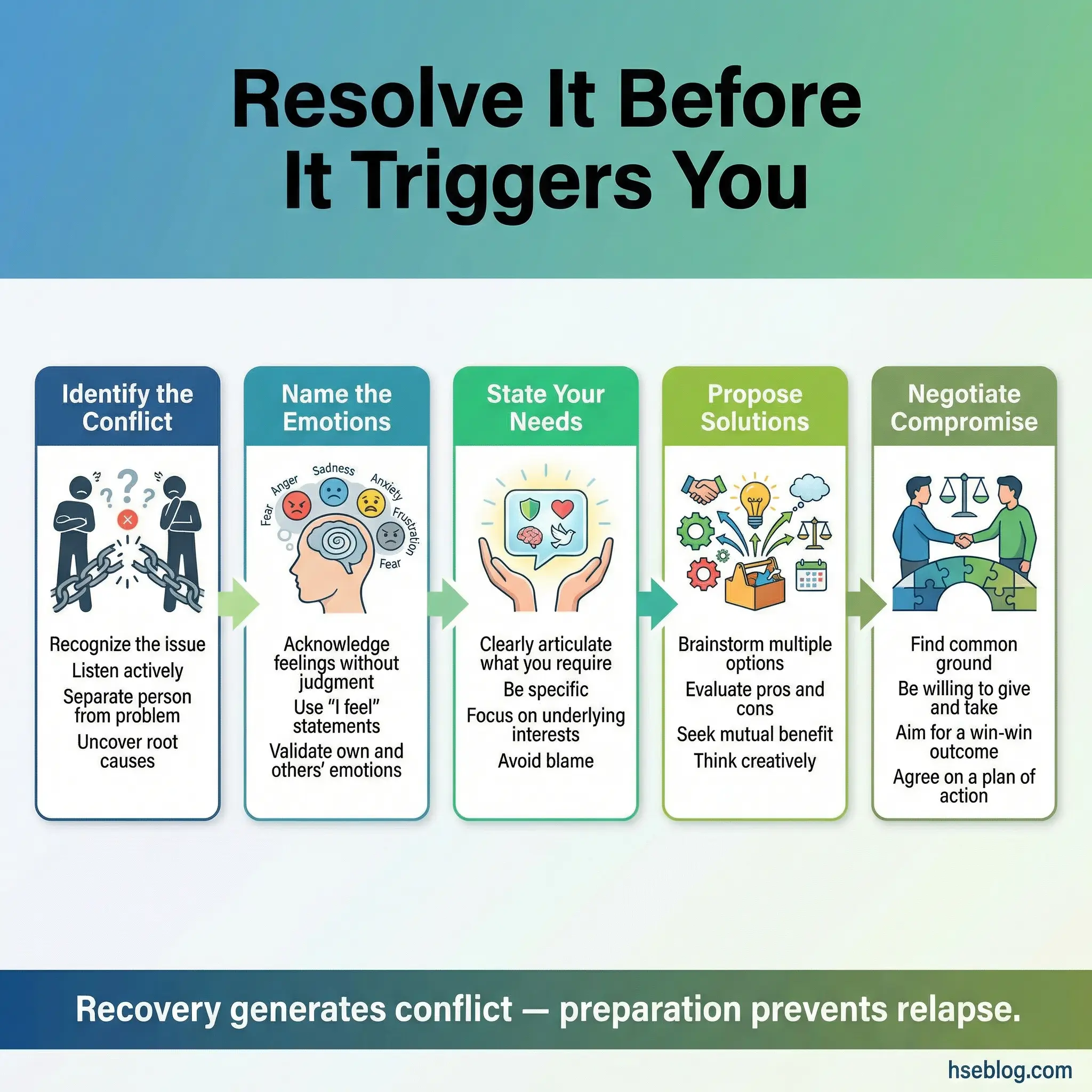
Groups work through resolution steps together — identifying the conflict, naming emotions, stating needs, proposing solutions, and negotiating compromise. The process is as important as the outcome.
This activity prepares participants for conflicts that will arise — not that might arise:
- Recovery generates conflict. Setting boundaries, changing social patterns, and communicating new needs inevitably creates friction with people who benefited from the participant’s old behavior. Practicing resolution in advance prevents reactive responses.
- It teaches “I” statements under pressure. Converting “You don’t respect my sobriety” into “I feel unsupported when substances are present in our shared space, and I need that to change” is a skill that requires practice, not just instruction.
- Multiple solutions are explored. The group brainstorms several possible responses to each scenario, discusses trade-offs, and identifies which approach best balances the participant’s recovery needs with relationship preservation.
- It normalizes imperfect resolution. Not every conflict ends in mutual satisfaction. Sometimes the assertive response costs a relationship. The group discusses this honestly.
- Session length: 50–60 minutes for 2–3 scenarios with discussion.
Activity 20: Shared Storytelling Chain
The shared storytelling chain is a collaborative narrative exercise where one participant begins a recovery-themed story with three sentences. Each subsequent participant adds three sentences, maintaining continuity with what came before. The story must maintain a coherent narrative arc as it passes through the entire group.
This activity builds collaborative thinking and reveals group dynamics in real time — who dominates the narrative, who withdraws, who introduces conflict, and who resolves it.
The exercise appears playful but contains significant therapeutic depth:
- It requires listening to build on. Each participant must understand what the previous person said before contributing. This demands the same active listening practiced in Activity 11 but in a creative context.
- The story reveals group themes. Without explicit instruction, the narrative almost always gravitates toward themes the group is collectively processing — loss, hope, fear of relapse, family conflict. The facilitator can debrief these themes after the story concludes.
- It balances control and surrender. Participants cannot control the story. Their contribution is shaped by what came before and will be shaped by what comes after. This mirrors the collaborative nature of recovery itself.
- Dominant and withdrawn patterns become visible. If one participant redirects the story dramatically while another adds only safe, inconsequential details, the facilitator has diagnostic information about group dynamics.
- Session length: 30–40 minutes including debrief.
Coping Skills and Relapse Prevention Activities (21–30)
Coping skills taught in a lecture are forgotten by lunchtime. Coping skills practiced in a group under simulated pressure become automatic responses. That distinction is the difference between a program that produces certificates and one that produces sustained recovery.
These activities are the operational core of any substance abuse group program. I have seen facilities spend weeks on self-awareness and trust-building, then rush through coping skills in a single session. That is a critical error. These activities require repetition, variation, and honest debriefing.
Activity 21: Craving Surfing Exercise
Craving surfing is a mindfulness-based experiential exercise where participants sit with a deliberately induced mild craving and practice “riding the wave” — observing the craving’s intensity rise, peak, and fall without acting on it. The facilitator guides the group through a visualization that introduces a trigger scenario, then coaches participants to observe their internal response with curiosity rather than resistance.
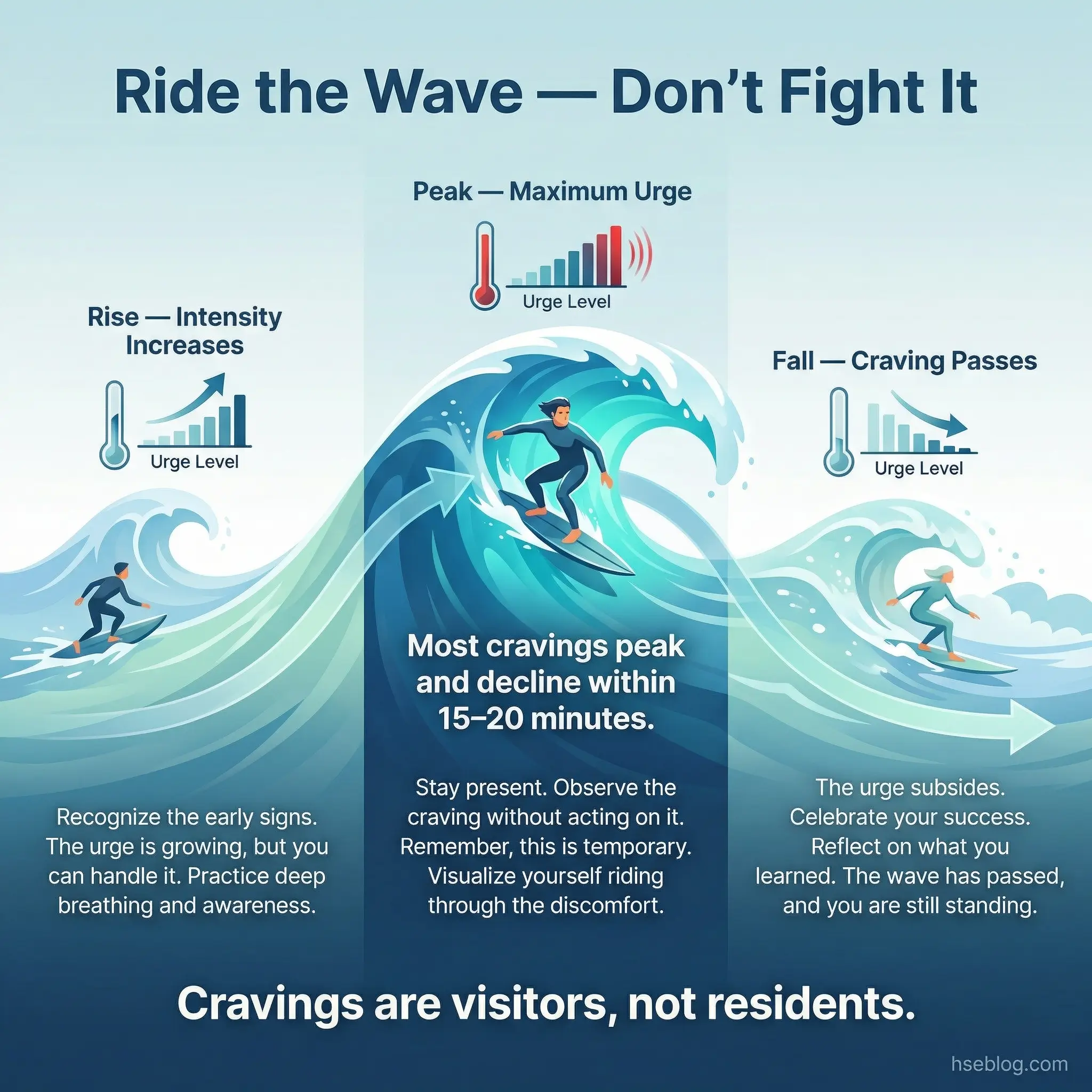
The core teaching is that cravings are time-limited events — not permanent states. Most cravings peak and begin declining within 15–20 minutes if they are observed rather than fed or fought.
This exercise teaches a skill that directly prevents relapse:
- Observation replaces reaction. Participants learn to say “I am experiencing a craving” rather than “I need to use.” This shift from identification with the craving to observation of the craving creates a critical decision-making space.
- It demonstrates impermanence. Experiencing a craving rise, peak, and fall within a safe environment provides evidence — felt, not just told — that cravings pass. This evidence is more powerful than any lecture.
- Silence is essential. Facilitators must resist the urge to fill uncomfortable quiet. A craving surfing session where the facilitator talks throughout teaches nothing about sitting with discomfort. Let the silence work.
- It pairs well with Activity 7 (Body Scan). Participants who have already practiced noticing physical sensations are better equipped to observe craving-related sensations without reacting.
- Session length: 30–40 minutes including guided exercise and discussion.
Activity 22: HALT Check-In
HALT stands for Hungry, Angry, Lonely, Tired — four physiological and emotional states that dramatically increase vulnerability to relapse. The HALT check-in teaches participants to assess which of these states they are experiencing before every group session, eventually building it into a daily self-monitoring habit.

The check-in takes only five minutes at the start of each session, but its cumulative impact over weeks is substantial. Participants begin catching high-risk states before they escalate into craving or relapse.
The power of HALT lies in its simplicity and repeatability:
- It converts vague vulnerability into specific, addressable states. “I feel terrible” becomes “I am hungry and tired, which means I need food and rest — not a substance.”
- Each HALT state has a concrete countermeasure. Hungry → eat. Angry → express or process. Lonely → connect. Tired → rest. The directness of the framework cuts through the complexity that paralyzes decision-making in early recovery.
- It becomes automatic with practice. After four to six weeks of HALT check-ins at the start of every session, participants begin using the framework outside the group — in their car, at their desk, before a social event.
- Facilitators should track patterns. If a participant is consistently “lonely” at every check-in, that becomes a treatment priority that might otherwise remain invisible.
- It prevents avoidable relapses. A significant percentage of relapse episodes trace back to unchecked HALT states — situations where the person was simply too hungry, too tired, or too isolated to resist a craving that adequate self-care would have neutralized.
Activity 23: Relapse Prevention Planning Workshop
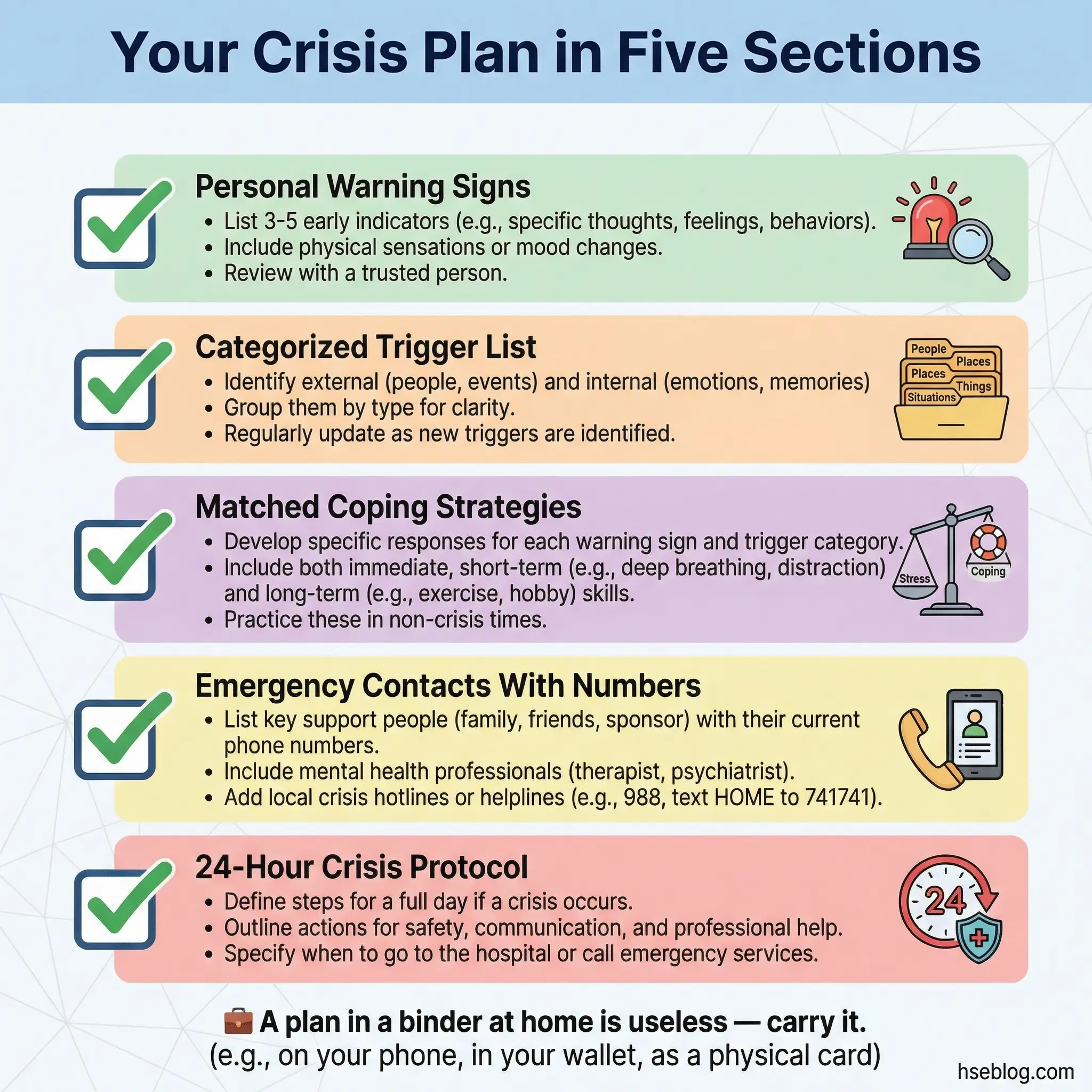
The relapse prevention planning workshop is a structured, full-session exercise where each participant builds a comprehensive written relapse prevention plan. The plan includes specific sections: personal warning signs, categorized trigger list, matched coping strategies for each trigger, emergency contacts with phone numbers, a detailed 24-hour crisis plan, and recovery maintenance activities.
This is not a fill-in-the-blank worksheet. The plan is drafted, reviewed by group members for blind spots, revised, and finalized into a document the participant keeps.
The group review process is where this activity becomes significantly more effective than individual planning:
- Group members spot blind spots. A participant might list “call my sponsor” as their only crisis strategy. Group members challenge: “What if your sponsor doesn’t answer at 2 AM?” The plan must have depth.
- Warning signs are validated. Group members who have observed the participant over multiple sessions can add warning signs the participant does not recognize — increased sarcasm, withdrawal from group discussion, skipping meals.
- The crisis plan must be time-specific. “Call someone” is not a plan. “At 0–15 minutes: call sponsor. If no answer, call secondary contact. At 15–30 minutes: go to the nearest meeting location (address included). At 30–60 minutes: go to the emergency room if suicidal ideation is present” — that is a plan.
- Plans are living documents. The facilitator should schedule a plan review session every four to six weeks, because triggers and circumstances change.
- Session length: 60–75 minutes. This requires a full session with no other activities.
Pro Tip: Activities 21 and 25 work best when facilitators allow silence. The urge to fill uncomfortable quiet undermines the exercise. A craving surfing session where the facilitator talks throughout teaches nothing about sitting with discomfort.
Activity 24: Refusal Skills Tournament
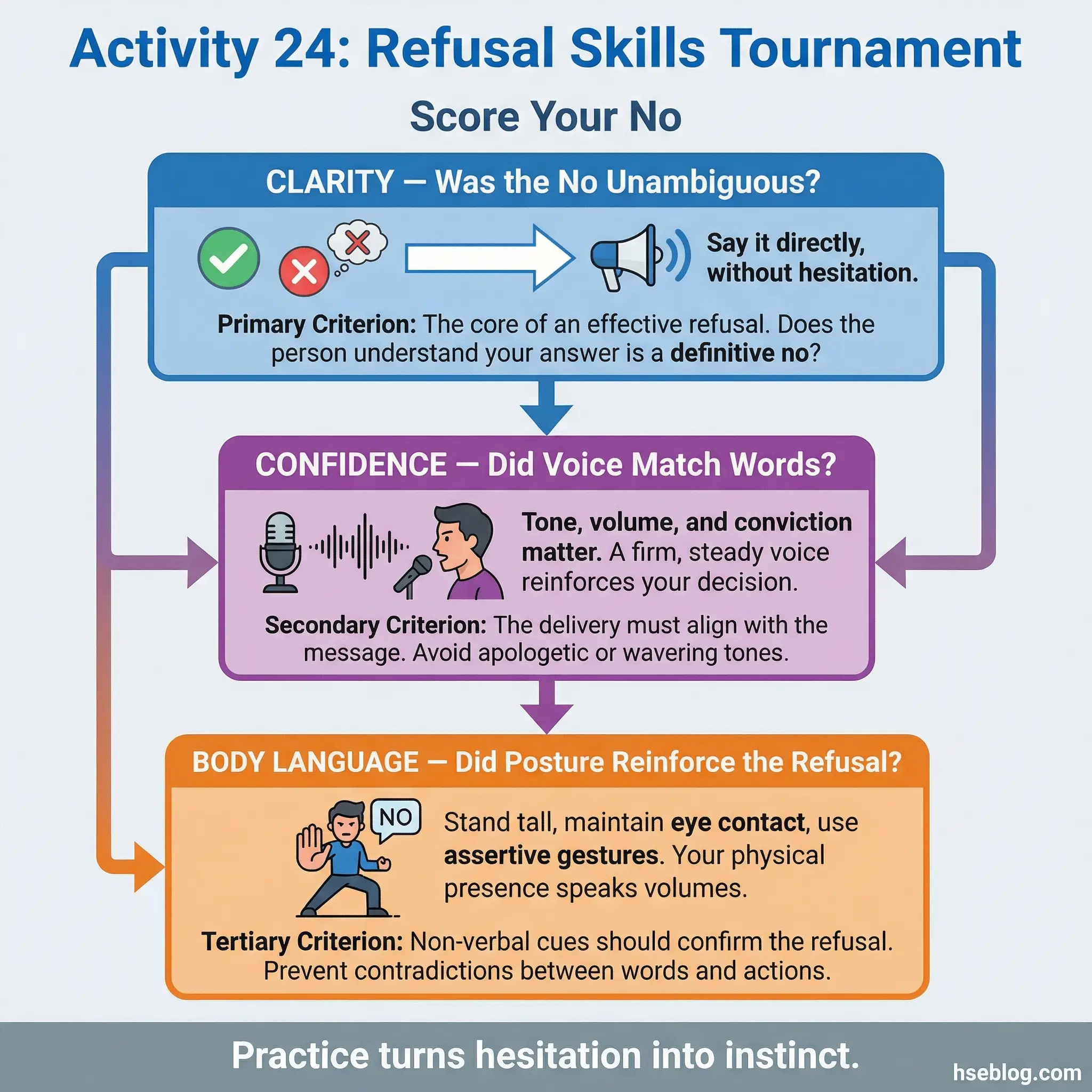
The refusal skills tournament is a structured, gamified exercise where participants practice refusing substances in increasingly difficult scenarios. The competitive element — participants are rated by the group on clarity, confidence, and body language — transforms a potentially awkward role-play into an engaging challenge.
Scenarios progress from low difficulty (a stranger offering a drink at a bar) through moderate difficulty (a colleague at a work event insisting they have “just one”) to high difficulty (a close friend at a private gathering expressing frustration with the participant’s sobriety).
The tournament format adds dimensions that standard role-play lacks:
- Competition increases effort. Participants try harder when performance is rated. The quality of refusal improves visibly across rounds.
- Group rating uses specific criteria. The group scores each refusal on three axes — clarity (was the “no” unambiguous?), confidence (did voice and posture match the words?), and body language (did eye contact, stance, and gestures reinforce the refusal?).
- Scenarios escalate social pressure. The progression from stranger to close friend mirrors real-world escalation. Participants who handle a stranger’s offer easily often stumble when the scenario involves someone they care about. That stumble is the learning moment.
- Winners share their techniques. The participants rated highest explain what they did and why. This peer coaching is often more practical than facilitator instruction.
- Repeated performance builds automaticity. By the third or fourth refusal, participants stop thinking about what to say and start saying it naturally. That automaticity is the goal.
- Session length: 45–55 minutes for 3–4 rounds with scoring and discussion.
Activity 25: Grounding Techniques Stations
Grounding techniques stations is a rotation-based experiential exercise where four stations are set up, each teaching a different grounding technique. Participants spend 8–10 minutes at each station, practice the technique with guidance, and then rotate. After completing all four stations, participants identify which technique worked best for their personal physiology.
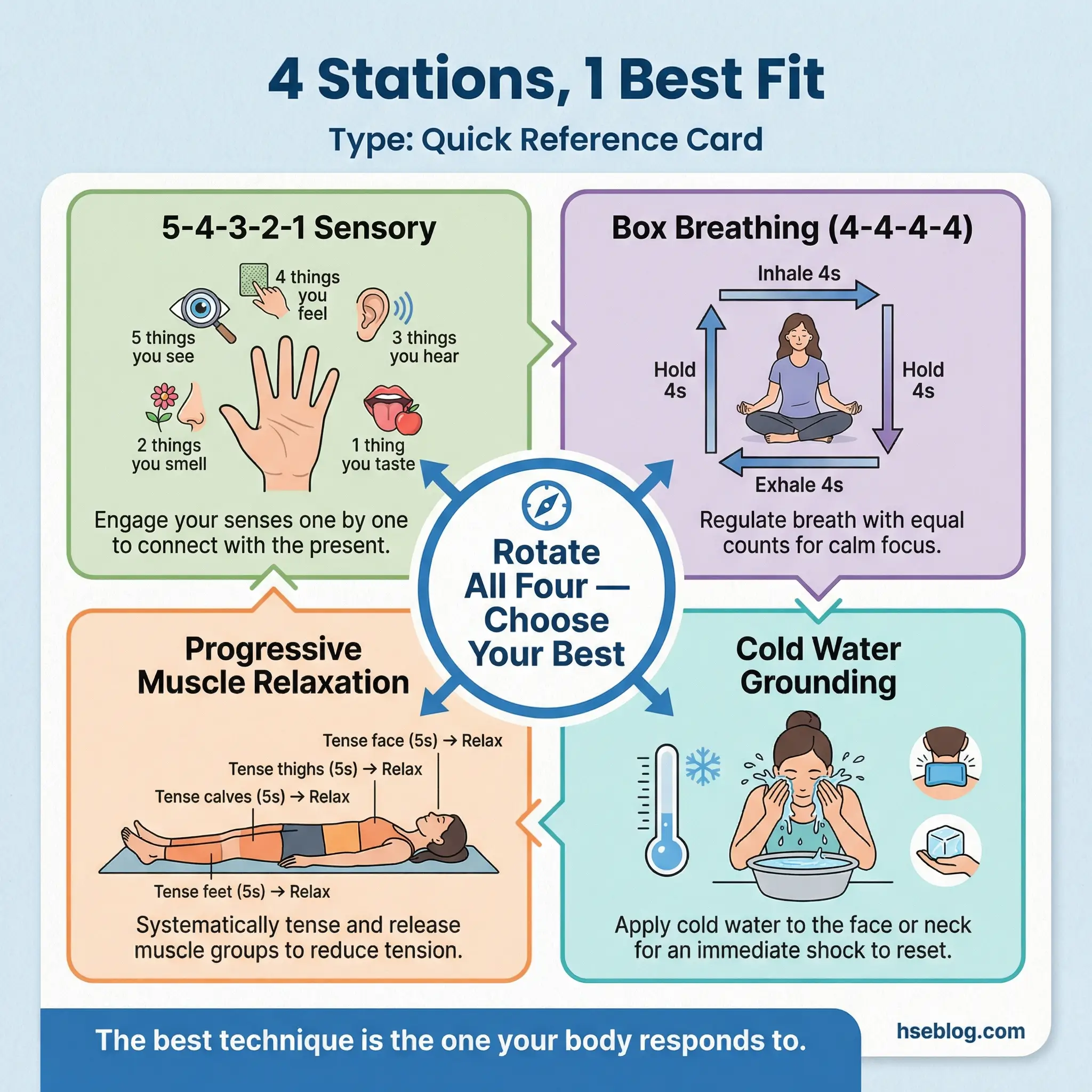
The four stations cover distinct grounding approaches to ensure every participant finds at least one technique that resonates:
- Station 1 — 5-4-3-2-1 Sensory Grounding: Participants name five things they can see, four they can hear, three they can touch, two they can smell, and one they can taste. This technique redirects attention from internal distress to external sensory reality.
- Station 2 — Box Breathing: Inhale for four counts, hold for four counts, exhale for four counts, hold for four counts. Repeat for five cycles. This technique directly activates the parasympathetic nervous system, reducing the physiological arousal that accompanies cravings and anxiety.
- Station 3 — Progressive Muscle Relaxation: Participants systematically tense and release each muscle group from feet to face, holding tension for five seconds and releasing for ten. This technique addresses the physical component of stress that many participants carry without awareness.
- Station 4 — Cold Water Grounding (hands only): Participants hold their hands in a bowl of cold water for 30 seconds while focusing on the sensation. The temperature shift interrupts rumination and craving loops by demanding sensory attention.
- The “best fit” identification is critical. Not every technique works for every person. The rotation format ensures participants discover their personal best-fit technique rather than being told to use one.
- Session length: 50–60 minutes for four rotations plus debrief and technique selection.
Activity 26: High-Risk Situation Mapping
High-risk situation mapping is a collaborative group exercise where participants collectively map an entire week in the life of a person in early recovery, identifying every high-risk moment — Friday evenings, payday, family gatherings, boredom on weekends, work stress peaks, doctor appointments where medication access occurs, grocery store alcohol aisles, and social media triggers.
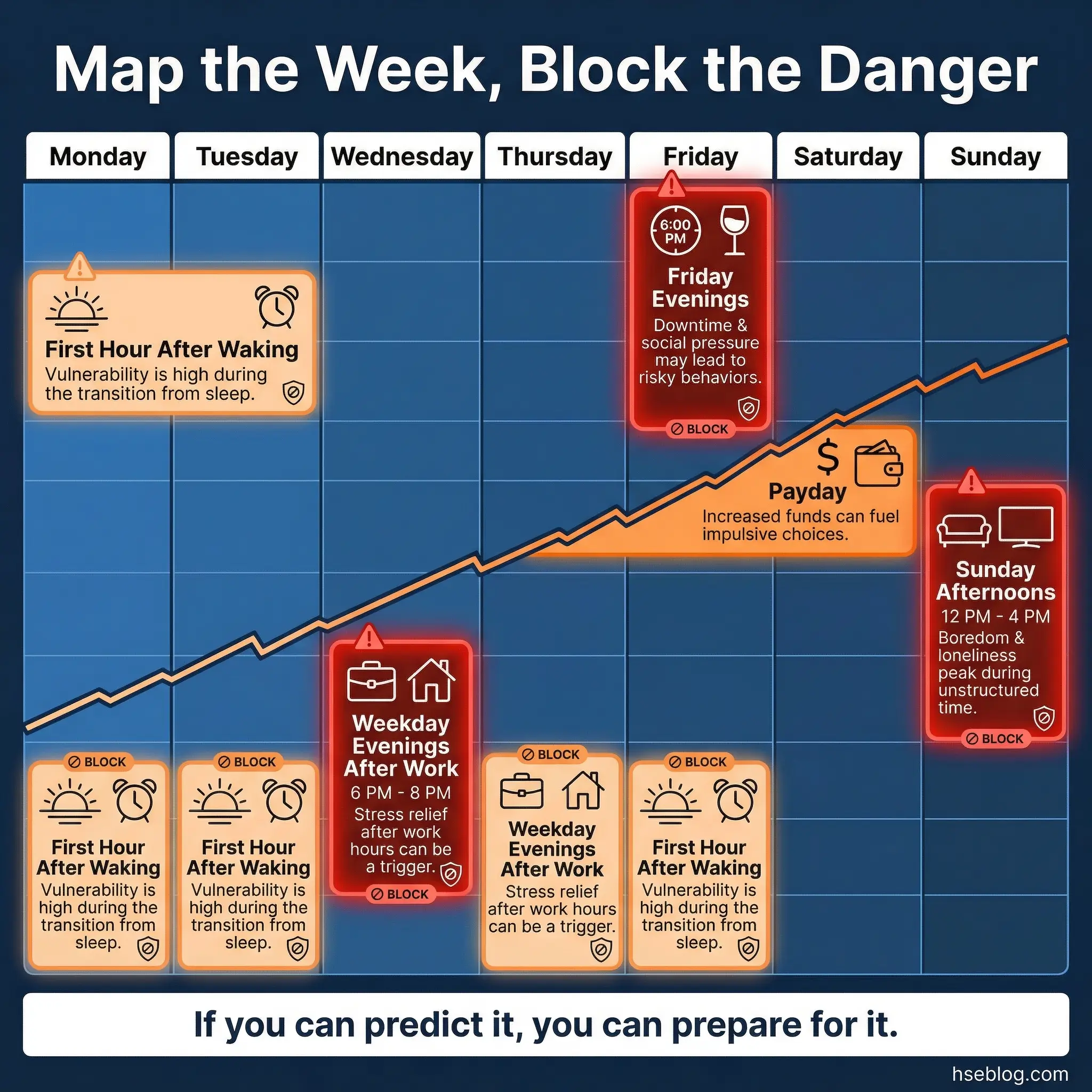
A large sheet of paper is laid out with seven columns representing each day of the week. The group collectively identifies high-risk moments for each day and time period, then brainstorms specific control strategies for each mapped moment.
This collective approach produces a more comprehensive risk map than any individual could create alone:
- Participants trigger each other’s awareness. One participant mentions payday as a risk. Another immediately adds “the ATM near the liquor store.” A third adds “driving home alone after work on Fridays.” The chain reaction of recognition fills gaps that individual reflection misses.
- Control strategies are group-sourced. For each high-risk moment, the group generates multiple options — not just one. Friday evenings might get: attend a meeting, call a recovery partner, go to a gym, cook a meal with a sober friend, schedule a therapy session.
- It makes the invisible visible. Many high-risk moments operate below conscious awareness. A participant who relapses “suddenly” often missed a predictable high-risk window that this map would have identified.
- It produces a take-home tool. The completed map — or a photographed copy — functions as a weekly navigation guide during early recovery.
- Session length: 50–60 minutes.
Activity 27: The Thought Record
The thought record is a cognitive-behavioral exercise where participants learn to identify and restructure the automatic thoughts that drive substance use. The format is structured into columns: activating event, automatic thought, emotion (with intensity rated 0–10), evidence supporting the thought, evidence against the thought, and rational alternative thought.
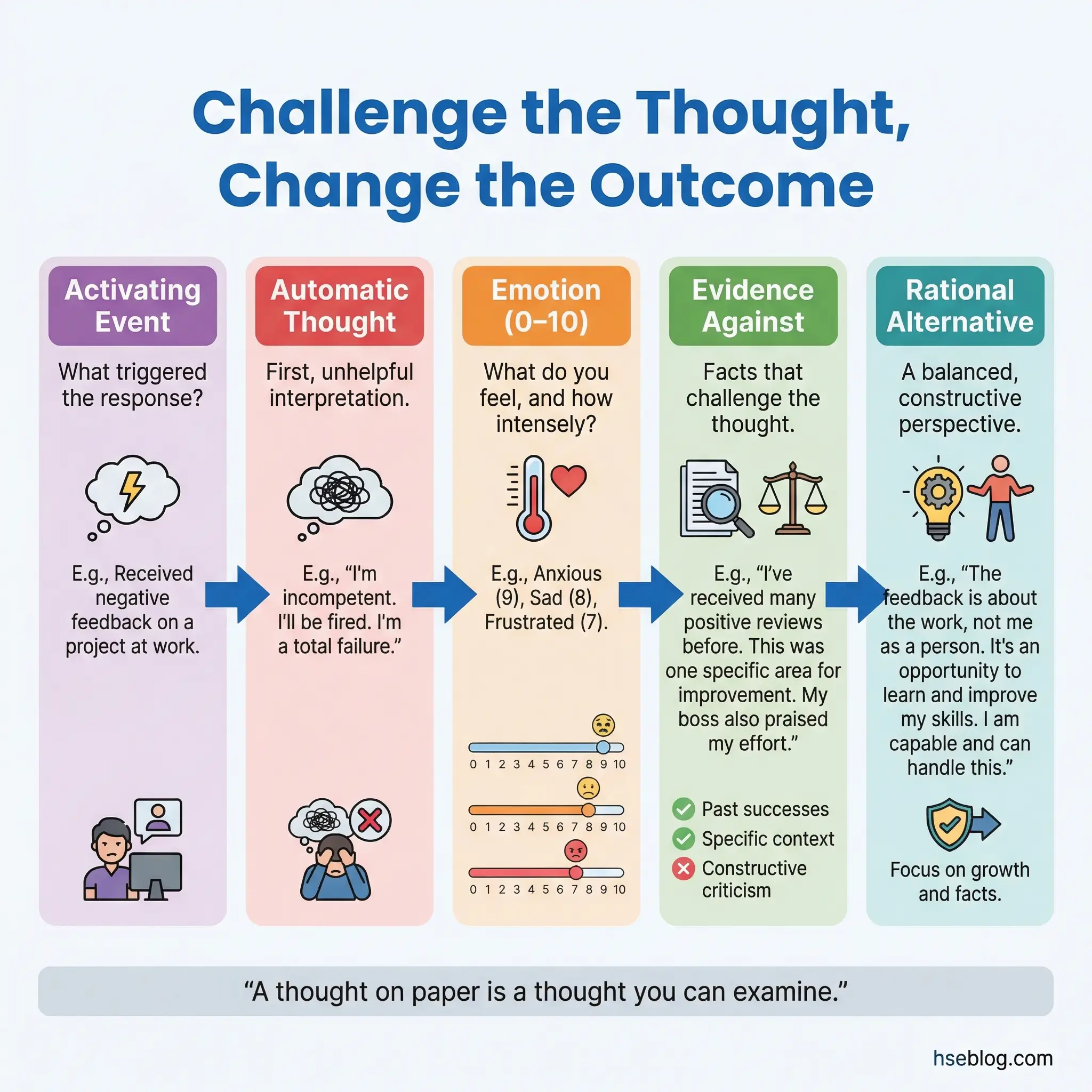
Three real examples from the past week are processed in group. This is one of the few activities that consistently changes thinking patterns when repeated over multiple sessions.
The thought record attacks the cognitive distortions that sustain addiction:
- It externalizes thinking. Writing a thought on paper separates the thinker from the thought. “I’ll always be an addict” becomes a sentence to examine rather than a truth to accept.
- The evidence columns force objectivity. A participant writes “Nobody supports my recovery.” The evidence-against column reveals: sponsor called twice, group members showed up, sister texted encouragement. The catastrophic thought cannot survive contact with specific evidence.
- Repetition is mandatory. A single thought record session teaches the format. Four to six sessions build the habit. Eight to ten sessions produce automatic cognitive restructuring — the participant begins catching and challenging distorted thoughts without the written exercise.
- Group processing adds perspectives. When a participant shares their thought record, other group members often provide evidence against the distorted thought that the participant could not see themselves.
- Session length: 45–55 minutes for processing three examples with group discussion.
Activity 28: Sober Fun Brainstorm
The sober fun brainstorm is a structured ideation exercise where the group collectively lists 50 activities they can do for enjoyment without substances. The list is then stress-tested against practical constraints — anything requiring significant money is flagged, anything requiring other people is marked as dependent, anything available at 2 AM (a common high-risk window) is highlighted.

The result is a practical, realistic recreation toolkit that addresses the boredom and anhedonia that plague early recovery.
This exercise sounds simple but addresses a critical gap in most treatment programs:
- Anhedonia is real and underaddressed. Early recovery suppresses the brain’s ability to experience pleasure from normal activities. A brainstormed list of 50 options increases the odds of finding something that produces even mild enjoyment during this difficult period.
- The stress test is the real exercise. An activity list that only works when the participant has money, company, and daytime availability is useless during the highest-risk moments — alone, broke, at 2 AM on a Tuesday. The constraint filter ensures practical applicability.
- Group brainstorming beats individual brainstorming. Participants learn about activities they never considered. Rock climbing, community theater, cooking classes, volunteer work at animal shelters, amateur radio, urban hiking — the diversity of group input expands individual horizons.
- The list becomes a crisis tool. During a craving, decision-making capacity collapses. Having a pre-made list of specific activities eliminates the need to generate options under duress.
- Session length: 35–45 minutes including brainstorming, stress-testing, and discussion.
Activity 29: Stress Inoculation Role-Play
Stress inoculation role-play is the most intensive coping exercise in this category. High-stress recovery scenarios are enacted with escalating intensity. A facilitator or experienced group member plays the role of a pressure source — offering substances, minimizing recovery, applying emotional manipulation — while the target participant practices real-time coping responses. The remaining group members observe and coach.
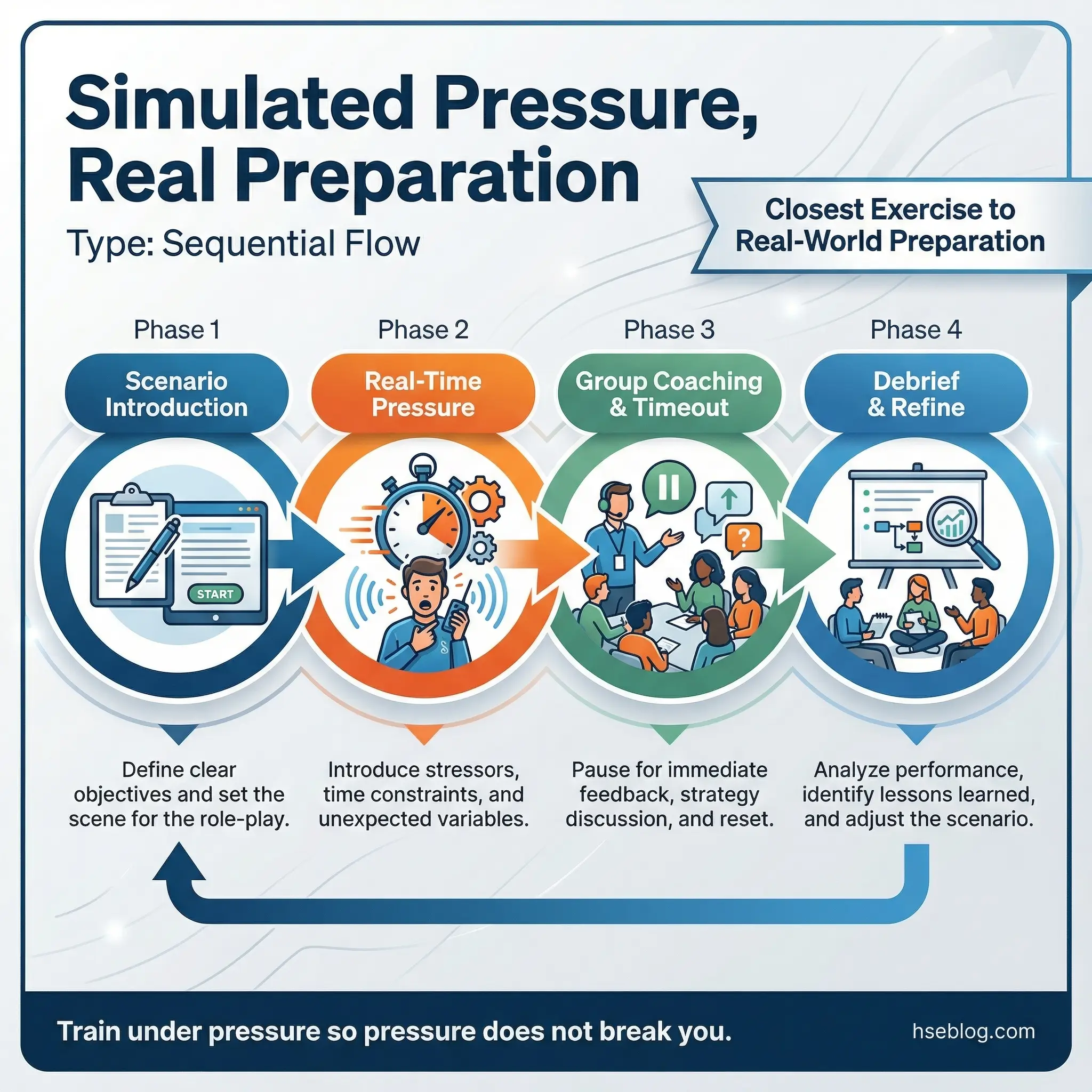
This is the closest a group activity gets to real-world preparation. The stress is simulated, but the physiological and emotional responses are real.
The exercise requires careful facilitation to be effective and safe:
- Scenarios must be realistic but controlled. The pressure should feel genuine — not theatrical. Effective facilitators draw from common real-world situations: a former using friend showing up unexpectedly, a family celebration where alcohol is central, a work failure that triggers the “I deserve a drink” thought pattern.
- Coaching happens in real time. Group members can call “time out” to offer suggestions. The participant can restart the scenario using a new approach. This iterative process builds resilience through repetition.
- Debriefing explores what worked and what did not. After each scenario, the group discusses which coping responses were effective, which felt forced, and what needs more practice.
- Emotional reactions are expected and processed. Some participants become genuinely upset during intense scenarios. The facilitator must be prepared to shift from exercise mode to support mode immediately.
- This activity belongs late in the program cycle. Participants need established coping skills (from Activities 21–28) before facing simulated high-pressure scenarios.
- Session length: 55–65 minutes for 2–3 scenarios with coaching and debrief.
Activity 30: Accountability Partner Contract
The accountability partner contract is a formalization exercise where pairs of group members draft a written agreement specifying what they will hold each other accountable for during the coming week. Contracts include specific commitments — check-in calls at designated times, meeting attendance targets, behavioral goals like daily exercise or meal preparation, and consequences for unmet commitments.
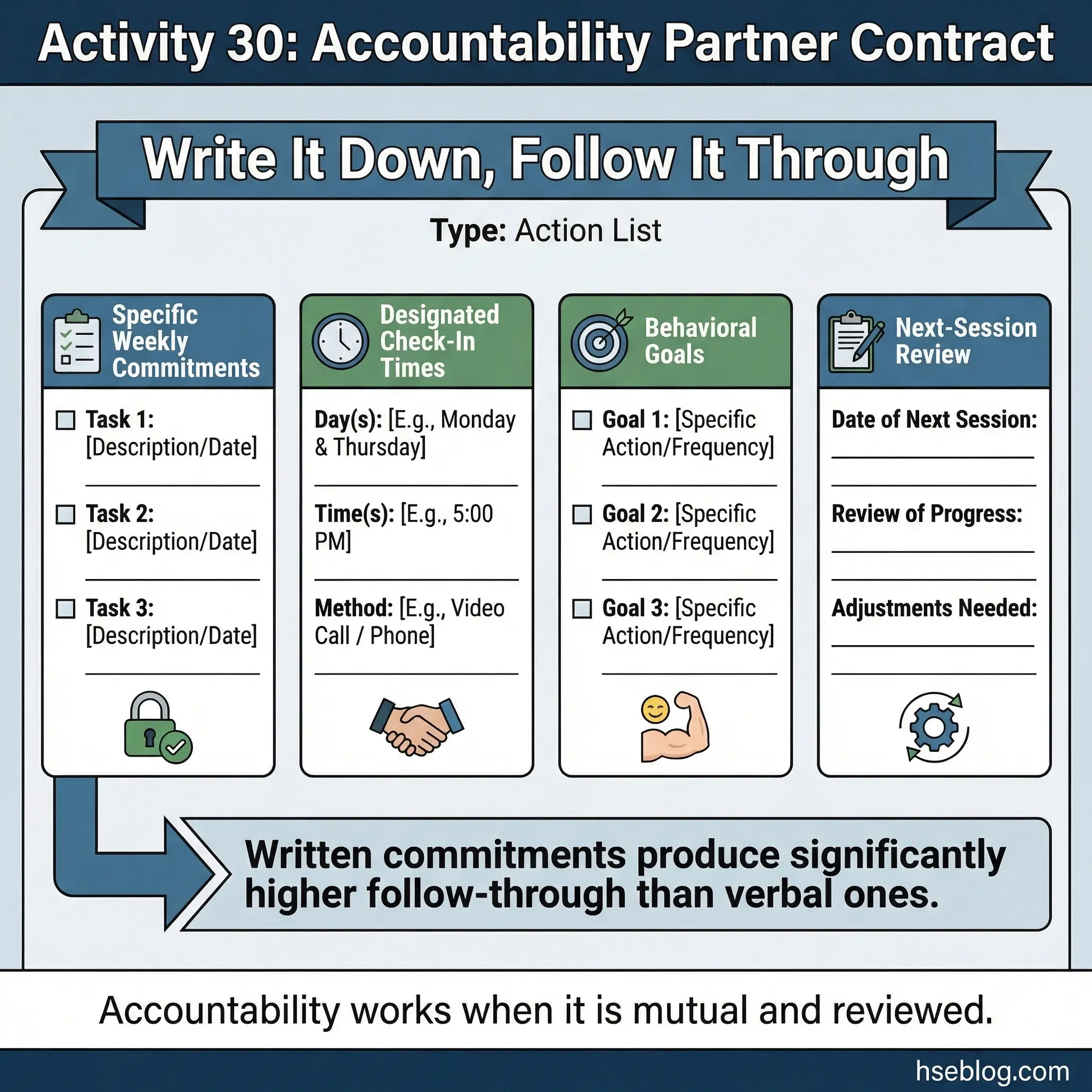
Contracts are reviewed at the next session. The formality of a written agreement increases follow-through measurably compared to verbal commitments.
This activity bridges group sessions and real life in a way few other activities achieve:
- Written commitments carry more weight. Research on commitment psychology consistently shows that written, public commitments produce higher follow-through than verbal or private ones. The contract format leverages this effect.
- Mutual accountability prevents hierarchy. Both partners commit to goals and both are reviewed. This is not a sponsor-sponsee relationship — it is a peer contract, which reduces power dynamics and increases honesty.
- The review session is essential. If contracts are written but never reviewed, participants learn that commitments in this group do not matter. Weekly review sessions must be non-negotiable.
- Contracts evolve over time. Early contracts focus on basic recovery maintenance — attend three meetings, call sponsor daily. Later contracts address deeper goals — have a difficult conversation with a family member, apply for a job, confront a trigger situation.
- Pairing should be intentional. The facilitator pairs participants based on compatibility and complementary needs, not random assignment.
- Session length: 35–45 minutes for drafting, review, and pairing.
Creative Expression and Healing Activities (31–40)
Trauma, shame, and grief sit underneath most substance use disorders. Talk-based therapy reaches them eventually. But for many participants — especially those with limited emotional vocabulary or histories of intellectualizing their pain — creative expression accesses what words cannot.
I have facilitated groups where a participant who had said nothing meaningful in four sessions of talk-based work produced a collage that told their entire story in twenty minutes. The group responded to the collage with a depth of empathy that no verbal exchange had generated. Creative activities earn their place because they bypass the defenses that addiction builds.
Activity 31: Recovery Collage
The recovery collage is a visual storytelling exercise where participants cut images and words from magazines to create a representation of their recovery journey — where they have been, where they are, and where they want to go. The three-phase structure (past, present, future) gives the collage a narrative arc that random clipping does not.
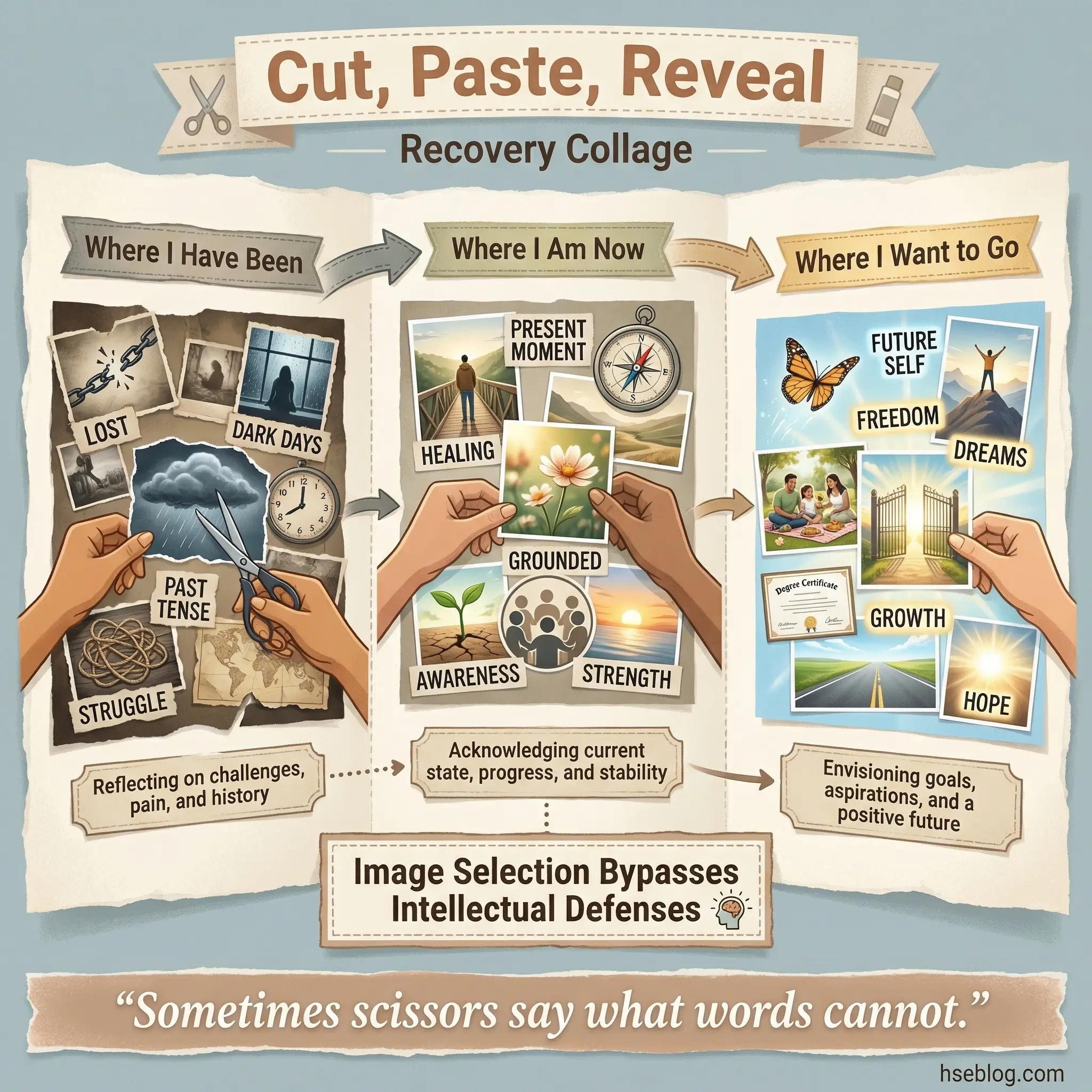
Each participant receives a stack of magazines, scissors, glue, and a large sheet of poster paper. The creation phase runs 25–30 minutes, followed by voluntary presentations where participants walk the group through their collage.
The visual medium unlocks expression that verbal participants often cannot access:
- Image selection bypasses intellectual defenses. A participant might struggle to say “I feel trapped” but will instinctively select an image of a cage or a closed door. The unconscious communication through image choice is often more honest than deliberate verbal disclosure.
- The future section is particularly powerful. Participants in early recovery rarely project forward. Being asked to find images representing their desired future forces engagement with hope — a capacity that active addiction suppresses.
- Collages become group artifacts. Displayed on the group room wall, collages create a visible record of the group’s collective recovery. New members see the collages of those who came before them, which instills hope.
- No artistic skill is required. The exercise uses magazine clippings, not original art. This eliminates the “I can’t draw” barrier that blocks many participants from creative activities.
- Session length: 55–65 minutes including creation, presentation, and debrief.
Activity 32: Music and Memory Mapping
Music and memory mapping is an emotionally evocative exercise where each participant selects two songs — one connected to their substance use and one connected to their recovery or their vision of recovery. Songs are played for the group (30–60 second clips), and participants briefly explain the connection.
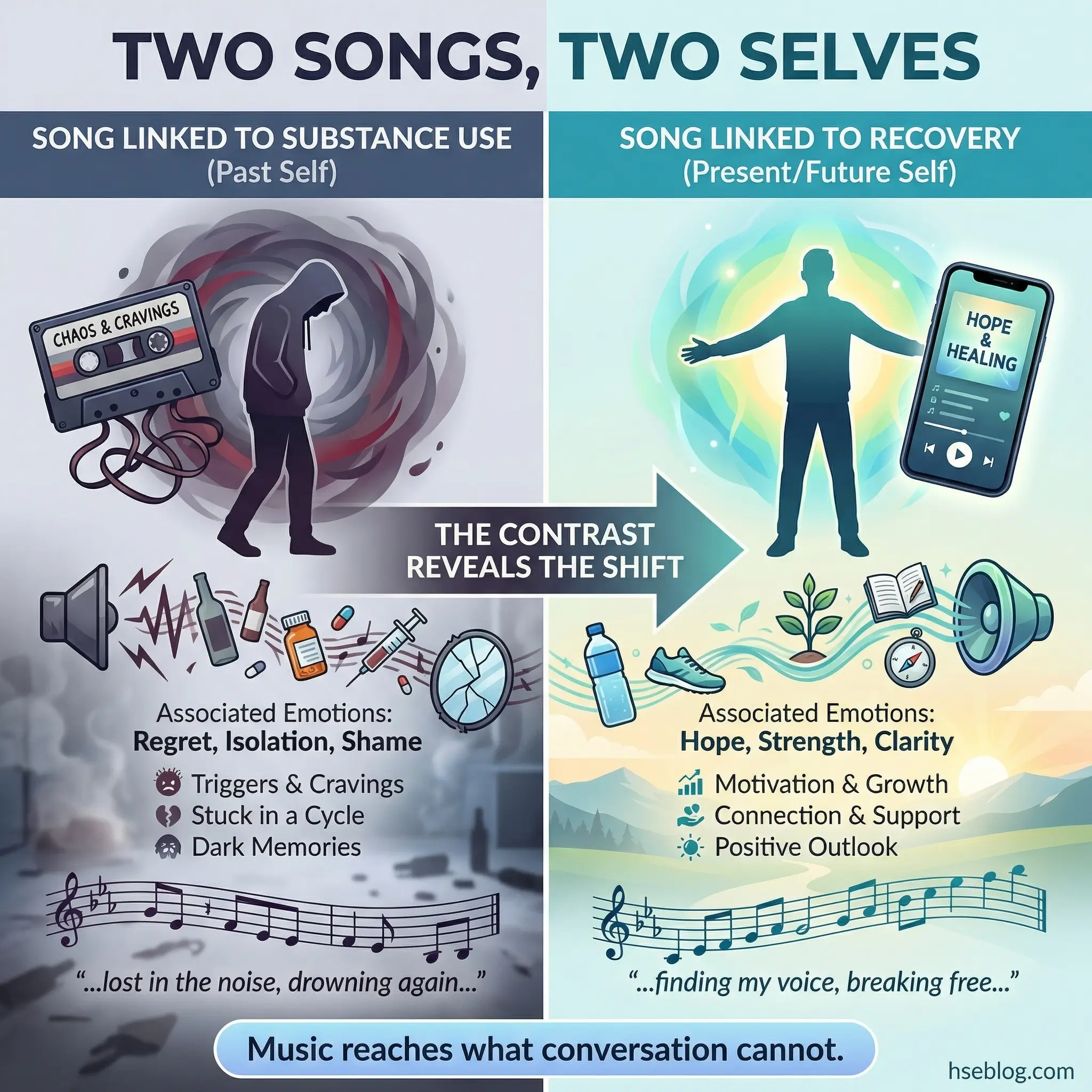
Music accesses emotional memory faster than any verbal prompt. This activity is particularly effective when a group feels emotionally stuck or intellectualized.
The exercise works through the neurological power of music-emotion associations:
- Music bypasses cognitive defenses. A song linked to a specific period of active use can trigger emotional recall more rapidly and completely than a verbal prompt asking “tell us about that time.” The facilitator must be prepared for strong emotional responses.
- The contrast between songs is the insight. The difference between the substance-linked song and the recovery-linked song often reveals a shift in values, emotional capacity, or self-perception that the participant has not consciously recognized.
- Group bonding intensifies. Sharing personal music creates intimacy and vulnerability. Participants often discover shared musical connections that strengthen peer relationships.
- Facilitator readiness is critical. If a participant becomes overwhelmed by the emotions a song triggers, the facilitator must be prepared to shift into grounding (Activity 7) or support mode.
- Song selection is homework. Assign the selection as homework before the session. In-session selection takes too long and reduces the reflective quality of the choices.
- Session length: 45–55 minutes for a group of 8–10 participants.
Activity 33: Mask Making
Mask making is a dual-surface art exercise that explores the gap between public presentation and internal reality. Using blank plastic or paper masks and art supplies (paint, markers, fabric, collage materials), participants decorate the outside of the mask to represent what they show the world and the inside to represent what they actually feel.
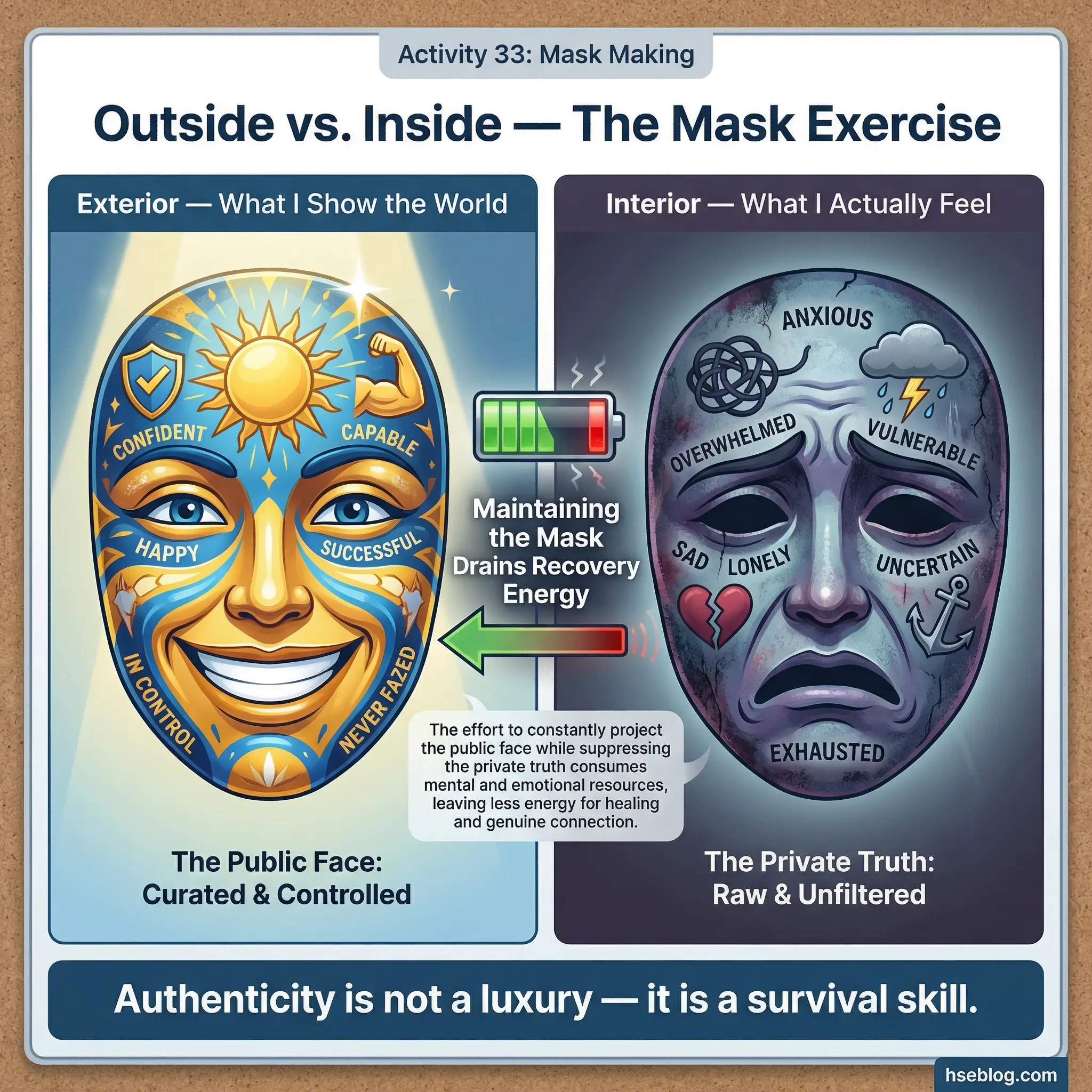
The contrast between exterior and interior drives discussion about authenticity, hiding, and the exhaustion of maintaining a false self during active addiction and into recovery.
This activity reaches therapeutic depth that few other exercises achieve:
- The physical metaphor is immediately understood. Every participant grasps the concept of wearing a mask without explanation. The universality of the metaphor eliminates the need for facilitator framing and lets participants engage directly.
- The interior surface accesses hidden content. What participants paint on the inside — fear, shame, loneliness, rage, hope — is often content they have not disclosed verbally. The artistic medium provides a safer channel for expressing what words make too real or too permanent.
- Sharing the interior is voluntary but powerful. Participants who choose to turn their mask around and show the group what they painted inside are performing an act of vulnerability that strengthens both individual courage and group trust.
- It connects to relapse risk. The energy required to maintain a public mask (pretending everything is fine, performing wellness) depletes the resources needed for genuine recovery. Recognizing this dynamic motivates authenticity.
- Session length: 60–70 minutes. Do not compress this activity — the art takes time, and rushing it undermines the reflective quality.
Activity 34: Group Mural
The group mural is a collaborative art exercise where a large sheet of paper (ideally 4–6 feet wide) is divided into sections — one for each participant. Each person contributes to a collective mural on a single theme: “What Recovery Looks Like.” The collaborative nature of the exercise mirrors the collaborative nature of recovery itself.
No artistic instruction is given beyond the theme. Participants choose their own medium — paint, markers, collage, writing — and their own interpretation. The absence of rules creates space for genuine creative expression.
The mural functions on both individual and group levels:
- Individual sections reveal personal recovery visions. Some participants draw nature scenes. Others write words. Some create abstract representations of emotion. The diversity itself becomes a discussion point — recovery looks different for everyone.
- The collective product is greater than its parts. When individual sections are viewed as a whole, unexpected visual conversations emerge — one participant’s image of a mountain connects to another’s image of climbing. These accidental connections mirror how group recovery creates meaning no individual could produce alone.
- It creates a tangible group legacy. The completed mural stays on the group room wall, serving as a visual anchor for future sessions and a record of what this particular group built together.
- It accommodates all comfort levels. Participants who are intimidated by individual creative exercises often feel safer contributing to a group project where their section is one of many.
- Session length: 45–55 minutes including creation and group reflection.
Activity 35: Poetry Slam (Recovery Edition)
The recovery poetry slam is a spoken-word exercise where participants write and perform short pieces — two to five minutes each — about their recovery experience. No literary skill is required. Raw honesty is the only criterion. For groups with performance anxiety, pieces can be read by the facilitator anonymously, sometimes incorporating substance abuse slogans as creative starting points.
Performance-based activities generate a unique quality of vulnerability and connection:
- Writing forces distillation. Converting a complex recovery experience into a short spoken-word piece requires identifying what matters most. The editing process itself is therapeutic — participants must decide what to keep and what to cut.
- Performance creates courage. Standing in front of a group and speaking personal truth — even badly, even nervously — is an act of bravery that transfers to other recovery situations requiring courage.
- The audience experiences resonance. Listeners often feel seen by another person’s words. The shared recognition — “that’s exactly how I feel” — is one of the most powerful mechanisms in group recovery work.
- Anonymous reading removes barriers. Facilitators who read pieces anonymously enable participation from individuals who would never perform. The writing is still therapeutic; the performance is a bonus.
- Session length: 50–60 minutes for a group of 8–10 participants.
Activity 36: Gratitude Jar
The gratitude jar is a cumulative, multi-session exercise. At the end of every group session, each participant writes one specific thing they are grateful for on a slip of paper and adds it to a shared glass jar. Monthly, the jar is opened and all entries are read aloud.
The accumulation over time creates a tangible, physical record of recovery’s positive trajectory. What begins as a sparse collection of small gratitudes becomes, over months, a full jar of evidence that life in recovery contains genuinely good moments.
The power of this activity lies in its simplicity and consistency:
- Specificity is enforced. “I’m grateful for my health” is rejected. “I’m grateful that I woke up without a hangover for the 30th day in a row” is accepted. Specificity connects gratitude to concrete experience rather than abstract sentiment.
- Monthly readings reveal growth. Early entries tend to be basic — “I showed up today.” Later entries reflect deepening recovery — “I had a difficult conversation with my brother and stayed calm.” The progression is visible to the entire group.
- It counteracts negativity bias. Addiction trains the brain to focus on what is missing, what hurts, and what is wrong. Regular gratitude practice rewires attention toward what is present, what heals, and what is right.
- The jar itself becomes a symbol. A full jar sitting in the group room communicates that this group has accumulated months of good moments. For a new participant, that visual evidence of collective progress is quietly powerful.
- Session length: 5 minutes per session, plus 20–30 minutes for monthly reading.
Activity 37: Clay Sculpting — Before and After
The clay sculpting exercise uses modeling clay as a medium for externalizing internal states. Each participant sculpts two objects: one representing how addiction made them feel and one representing how recovery feels. No artistic skill is needed — abstract shapes, rough forms, and symbolic objects all work.
The physical act of shaping something tangible from an internal state is grounding and often deeply emotional. The before-and-after contrast creates a visual narrative of transformation that verbal description struggles to match.
This activity accesses therapeutic territory through the body, not just the mind:
- Working with hands engages different processing. The kinesthetic act of molding clay activates neural pathways that verbal and visual exercises do not. Participants who are “talked out” often find new emotional access through tactile engagement.
- Abstract forms reveal honest emotion. A participant who sculpts a tight, hard ball to represent addiction is communicating constriction and rigidity without needing to find words for it. The group can respond to the object directly — “That looks really tense” — opening discussion.
- The before-and-after contrast motivates continued recovery. Holding the two sculptures side by side — one tense, the other open — provides physical evidence of change. Participants sometimes keep the “recovery” sculpture as a tactile reminder.
- It normalizes imperfection. Clay is forgiving. It can be reshaped, which mirrors recovery itself — a process of constant reshaping, not a single perfect outcome.
- Session length: 45–55 minutes including sculpting, presentation, and discussion.
Activity 38: Photo Voice Project
The photo voice project extends recovery reflection beyond the group room and into daily life. Over the course of a week, participants photograph five things in their daily environment that represent five assigned themes: hope, challenge, strength, loss, and change. At the next session, participants present their five photos to the group with brief explanations of each choice.
This activity transforms daily life into a recovery practice. Participants begin seeing their environment through the lens of recovery themes, which strengthens the integration of recovery identity into everyday awareness.
The exercise produces insights that in-session activities alone cannot generate:
- It captures real-world context. Photos taken in participants’ actual environments — their kitchen, their bus stop, their workplace — ground recovery in the reality they navigate daily, not in the artificial safety of the group room.
- The assignment changes how participants see. Actively looking for “hope” in one’s daily environment is itself a therapeutic intervention. Participants report noticing positive elements they had previously overlooked.
- Photos create discussion starting points. A photograph communicates instantly what verbal description might take five minutes to establish. The visual anchor allows the group to engage with the participant’s environment directly.
- It reveals environmental risk factors. Photos representing “challenge” often depict triggers the participant encounters routinely — a bar on their walking route, an empty room, a clock showing a high-risk time. These become actionable targets for environmental modification.
- Session length: 45–55 minutes for presentation and discussion.
Activity 39: Guided Visualization and Drawing
Guided visualization and drawing combines a facilitator-led 10-minute visualization of the participant’s life one year into sustained recovery with an immediate drawing exercise to capture what they saw. The facilitator guides participants through specific domains — morning routine, work or purpose, relationships, physical health, emotional state, and daily habits — one year into the future.
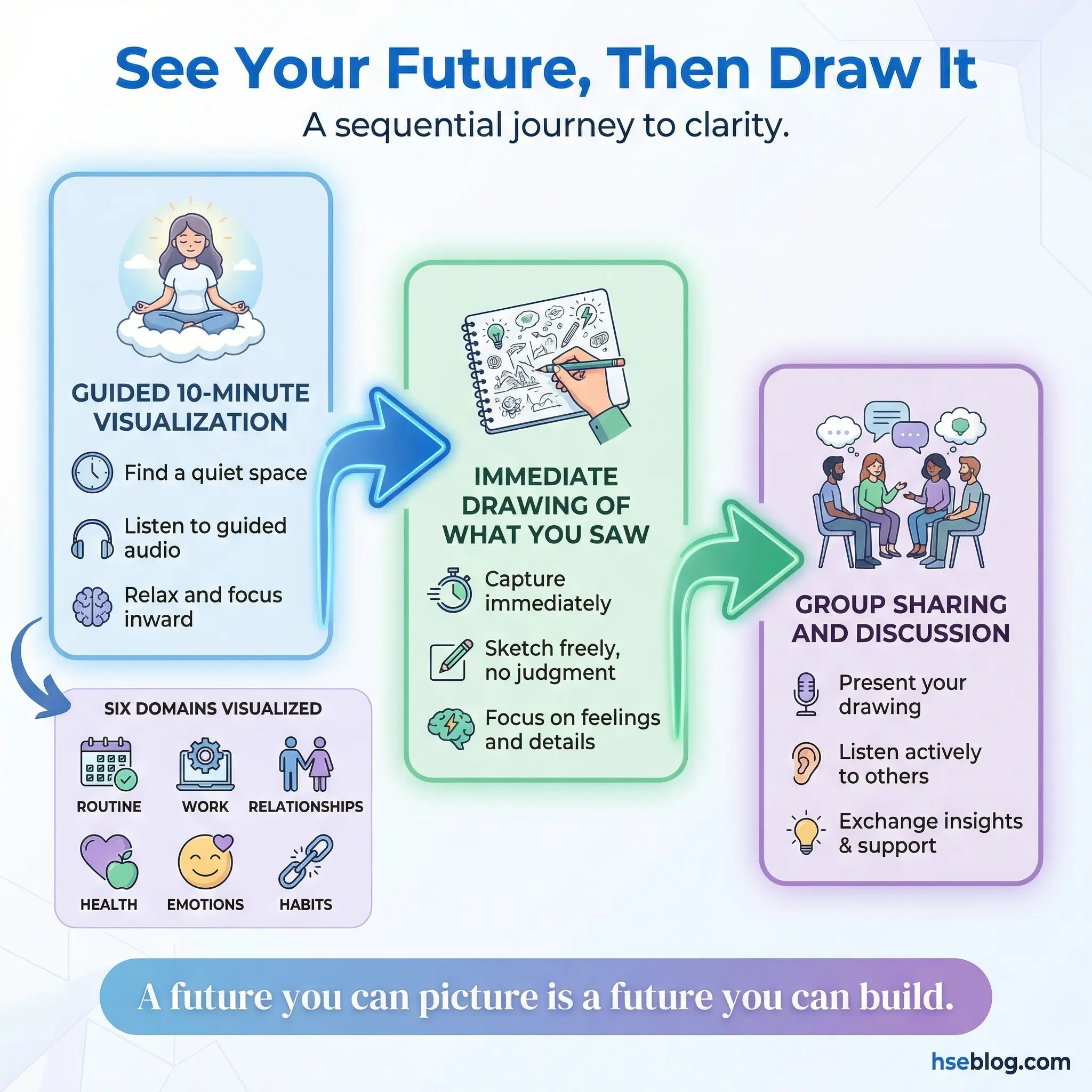
Immediately after the visualization ends, participants draw what they saw. Drawings are shared with the group. This activity strengthens future-oriented thinking, which is often severely underdeveloped in early recovery.
The combination of visualization and drawing produces a more durable impact than either exercise alone:
- Visualization creates emotional experience. Participants do not just think about their future — they feel it. The guided format activates emotional and sensory processing that pure imagination often fails to engage.
- Drawing captures the vision before it fades. The immediate shift from visualization to drawing prevents the rational mind from editing or dismissing what was imagined. The drawing preserves the raw vision.
- Future orientation motivates present action. Participants who can see a concrete future worth having are more motivated to do the difficult work required to get there. Vague hopes do not motivate. Specific, emotionally felt visions do.
- Shared drawings build collective hope. Seeing ten different drawings of ten different recovery futures communicates that recovery is not a single narrow path but a landscape of possibilities.
- Session length: 40–50 minutes including visualization, drawing, and sharing.
Activity 40: Movement and Rhythm Circle
The movement and rhythm circle is a non-verbal, body-based group exercise using simple percussion instruments (drums, shakers, tambourines) or body percussion (clapping, stomping, snapping). The group creates a shared rhythm together. Participants take turns leading tempo changes, volume shifts, and rhythmic variations while the rest of the group follows.

This activity builds group cohesion faster than most verbal exercises because it creates a shared physical experience that requires cooperation, listening, and mutual attunement without a single word being spoken.
The therapeutic properties of rhythm-based group work are distinct from verbal and visual modalities:
- Non-verbal participation eliminates language barriers. Participants who are withdrawn, inarticulate, or resistant to verbal exercises can participate fully. The activity demands presence, not disclosure.
- Leading and following alternate. Each participant experiences both roles — leading the group’s rhythm and following someone else’s lead. This mirrors the recovery dynamic of sometimes guiding and sometimes being guided.
- Synchrony creates belonging. Neuroscience research on group rhythmic activity shows that synchronized movement and sound production increase feelings of social bonding and group identity. Participants feel connected after the exercise without being able to articulate why.
- It regulates the nervous system. Rhythmic activity has a direct calming effect on the autonomic nervous system. Groups that begin sessions agitated or disconnected often settle visibly after a rhythm circle.
- Session length: 20–30 minutes. Works well as a session opener or a reset after an emotionally intense exercise.
Life Skills and Accountability Activities (41–50)
Recovery that addresses only the emotional and psychological dimensions of addiction while ignoring the practical wreckage is incomplete. Financial chaos, unemployment, damaged daily routines, and absent goal-setting capacity all fuel relapse. These final ten activities target the functional life skills that sustained recovery requires.
I have seen individuals complete excellent treatment programs — strong emotional insight, solid coping skills, genuine peer connections — and relapse within weeks because they returned to a life with no structure, no financial plan, and no daily routine. These activities close that gap, addressing the long-term effects of substance abuse on daily functioning.
Activity 41: Weekly Schedule Building
Weekly schedule building is a practical planning exercise where each participant creates a detailed weekly schedule accounting for every waking hour — including recovery meetings, work, exercise, meals, sleep, social connection, recreation, and critically, unstructured time.

The activity’s real value lies not in filling hours but in identifying and filling “danger hours” — the empty time blocks where boredom, isolation, or routine triggers could lead to use.
Effective scheduling in recovery requires specific attention to patterns most participants miss:
- Danger hours must be explicitly identified. Friday evenings, Sunday afternoons, weekday evenings after work, and the first hour after waking are common high-risk windows. These must be scheduled with specific activities, not left blank.
- Recovery activities are scheduled as non-negotiable. Meetings, therapy appointments, and sponsor calls go on the schedule first — before work commitments, social events, or errands. This communicates their priority.
- Rest is scheduled, not residual. Sleep hygiene — consistent bedtime, screen-free wind-down, seven to eight hours — is built into the schedule as a structured commitment. Fatigue is a HALT state that drives relapse.
- The group reviews each schedule. Group members who know each other’s triggers can identify gaps — “You left Saturday morning empty, and you told us weekends are your hardest time.”
- Schedules are updated weekly. A single schedule built once becomes obsolete. Weekly revision during the accountability portion of group sessions keeps the tool current.
- Session length: 40–50 minutes including drafting, peer review, and revision.
Activity 42: Financial Recovery Workshop
The financial recovery workshop addresses the economic devastation that addiction leaves behind. Participants assess the total financial damage of their substance use — debt accumulated, income lost, assets damaged or sold, legal costs, medical bills — and begin building a basic recovery budget.
This activity is uncomfortable. Money is a topic most treatment programs avoid entirely. But financial stress is one of the most potent relapse triggers, and ignoring it leaves a critical vulnerability unaddressed.
The workshop covers ground that emotional and psychological work cannot:
- Honest financial accounting reduces shame. The number — whatever it is — has been avoided, estimated, and feared. Writing it down and sharing it with a group that responds with empathy rather than judgment reduces the shame that keeps financial problems hidden and growing.
- A basic recovery budget provides structure. Participants build a simple monthly budget covering essentials — rent, food, transportation, debt minimum payments — and identify where their current income falls short. This clarity, even when the picture is bleak, is preferable to the anxiety of not knowing.
- Money as a trigger is discussed openly. Having cash on hand, receiving a paycheck, experiencing a financial windfall, or facing a bill collector are all trigger situations. Naming them and building coping plans (from Activity 23) reduces their power.
- Practical referrals are provided. The facilitator should have a list of local free financial counseling services, debt management programs, and income assistance resources available for participants who need professional support beyond what the group can offer.
- Session length: 50–60 minutes.
Activity 43: Resume and Interview Practice
Resume and interview practice addresses the employment barrier that makes sustained recovery functionally difficult. Participants who are unemployed or underemployed draft resumes that address employment gaps honestly but strategically. Mock interviews are conducted by group members who play the role of hiring manager.
Employment provides income, structure, purpose, and social connection — four factors that directly support recovery. This activity removes practical barriers to obtaining it:
- Employment gaps are addressed honestly. The group practices framing recovery-related gaps in truthful but professional language — “I took time to address a health issue and am now fully ready to commit to a professional role” — without disclosure of specific diagnosis unless the participant chooses otherwise.
- Mock interviews build confidence. Many participants have not interviewed in years. The anxiety of job searching can itself become a relapse trigger. Practicing in a safe environment reduces that anxiety to manageable levels.
- Group feedback improves presentation. Group members provide feedback on body language, eye contact, handshake, voice tone, and answer quality — the same elements that the Refusal Skills Tournament (Activity 24) addresses in a different context.
- It addresses internalized unemployability. Participants who believe they are unhireable carry that belief as evidence of permanent damage. A successful mock interview challenges that belief with direct experience.
- Session length: 50–60 minutes for 3–4 mock interviews with feedback.
Activity 44: Goal Ladder Exercise
The goal ladder exercise is a structured goal-decomposition activity where each participant identifies one long-term recovery goal and breaks it into weekly, achievable steps arranged as “rungs” on a drawn ladder. The visual format makes the path from current position to desired outcome concrete and navigable.
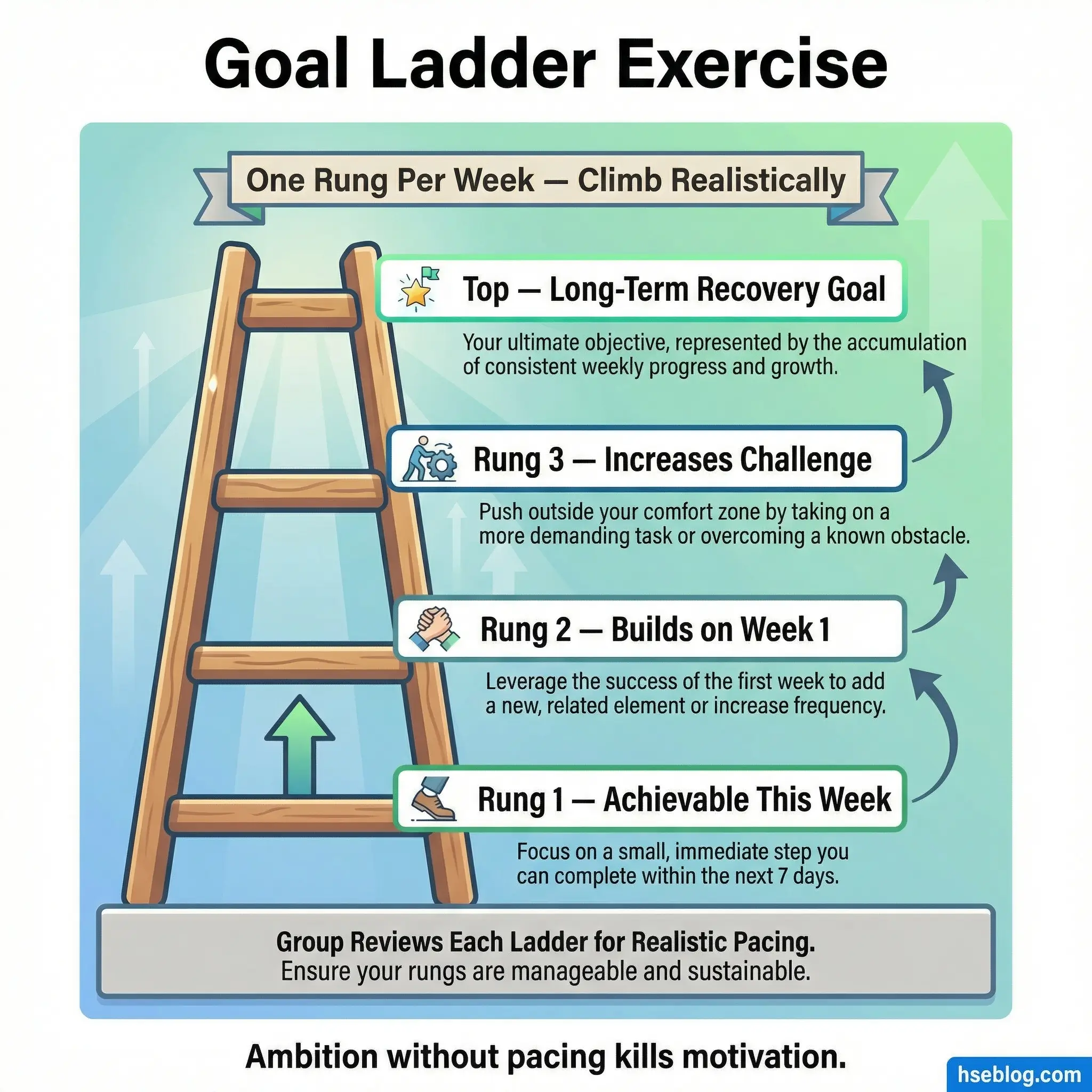
The group reviews each ladder for realistic pacing. Overly ambitious goals are the silent killer of early recovery motivation — a participant who sets a goal of “rebuild my relationship with my children” as a single step will feel failed by next week. Breaking it into first-rung steps like “write a list of what I want to say” makes progress possible.
This exercise prevents the all-or-nothing thinking that sabotages recovery goals:
- Each rung is one week of work. The time constraint forces specificity. “Get healthier” is not a rung. “Walk for 20 minutes on Monday, Wednesday, and Friday” is.
- The bottom rung must be achievable this week. If the first step is not doable within seven days, the goal is still too abstract. This rule prevents aspirational planning that never converts to action.
- The group challenges unrealistic pacing. Participants in the energized early weeks of recovery often overcommit. Group members who have experienced this pattern firsthand provide reality checks that a facilitator’s caution often cannot.
- Ladders are revisited monthly. Progress is marked. Rungs that were not reached are examined for obstacles. New rungs are added as circumstances change.
- Session length: 40–50 minutes including individual drafting, group review, and revision.
Activity 45: Healthy Routine Challenge
The healthy routine challenge is a group-designed, week-long behavioral experiment. The group collectively designs a seven-day challenge incorporating four domains of daily wellness: sleep hygiene (consistent bedtime, screen-free hour before sleep), nutrition (three structured meals, hydration), physical activity (minimum 20 minutes of movement daily), and social connection (one meaningful interaction per day).
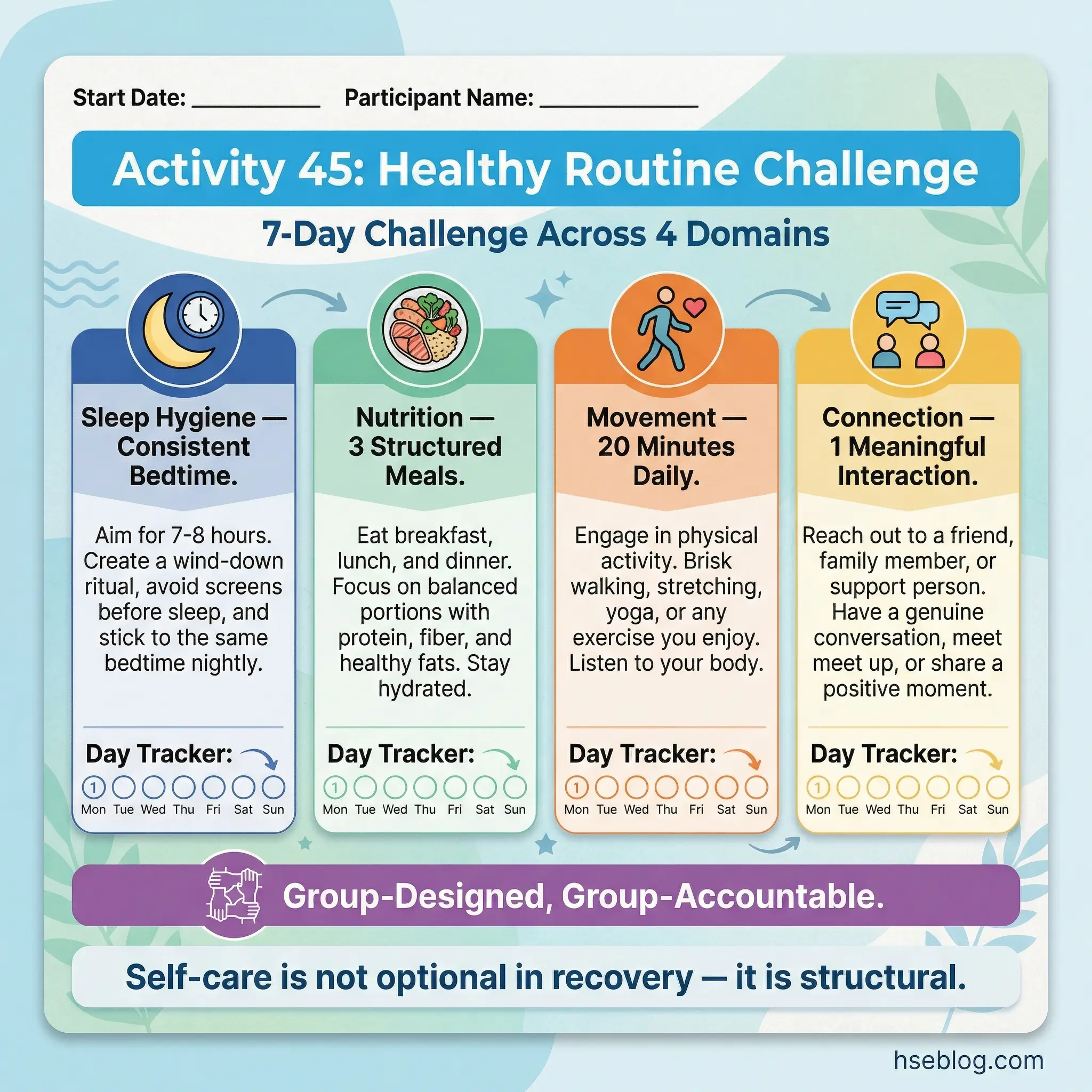
Participants commit to the challenge in front of the group and report results at the next session. The group format creates social pressure that individual goal-setting lacks.
The challenge framework leverages group accountability to build healthy habits:
- Group design increases buy-in. Because the group designs the challenge together — negotiating what is realistic, debating standards, and agreeing on commitments — participants feel ownership rather than compliance.
- Four domains prevent imbalance. Many participants in recovery address one wellness domain (exercise) while neglecting others (sleep, nutrition, social connection). The four-domain structure ensures comprehensive self-care.
- Reporting at the next session drives follow-through. Knowing that the group will ask about compliance next week is a more powerful motivator than internal resolve alone.
- Challenges escalate over time. The first challenge is deliberately modest — achievable for almost everyone. Subsequent challenges add complexity, duration, or intensity based on group readiness.
- Session length: 30–40 minutes for design and commitment, plus 20 minutes at the following session for reporting.
Activity 46: Relapse Response Drill
The relapse response drill is the most operationally important activity in this entire list and the most underused across treatment programs. Structured identically to a fire drill, this exercise walks participants through exactly what to do in the first 60 minutes after a slip — who to call, where to go, what to do, and critically, what not to do.

Responses are written on wallet-sized cards that participants carry at all times. The drill format replaces panic and shame with automatic, pre-planned action.
Every treatment program practices what to do to prevent relapse. Almost none practice what to do when relapse happens:
- The first 60 minutes determine trajectory. A slip does not automatically become a full relapse. The actions taken in the first hour — calling a support person, leaving the environment, not using again — determine whether the episode is contained or escalates.
- Pre-planned responses bypass shame paralysis. The most common response to a slip is shame-driven isolation — hiding, avoiding calls, skipping meetings. A rehearsed, automatic response plan interrupts this pattern before it takes hold.
- The wallet card format is intentional. A relapse prevention plan in a binder at home is useless at the moment of crisis. A laminated card in a wallet with three phone numbers and four action steps is immediately accessible.
- Drilling reduces stigma. Treating relapse response as a practiced skill — like a fire drill — normalizes preparation without endorsing relapse. It communicates that preparation is responsible, not defeatist.
- Session length: 40–50 minutes including drill, card creation, and discussion.
Pro Tip: Activity 46 — the relapse response drill — is the most underused activity in this entire list. Given that the majority of individuals in recovery experience at least one slip, this preparation is not pessimism. It is operational readiness.
Activity 47: Mentorship Pairing
Mentorship pairing is a structured relationship exercise where longer-term group members are paired with newer participants in a formal mentorship format. The pairing is intentional — the facilitator matches based on compatibility, complementary needs, and recovery stage rather than random assignment.
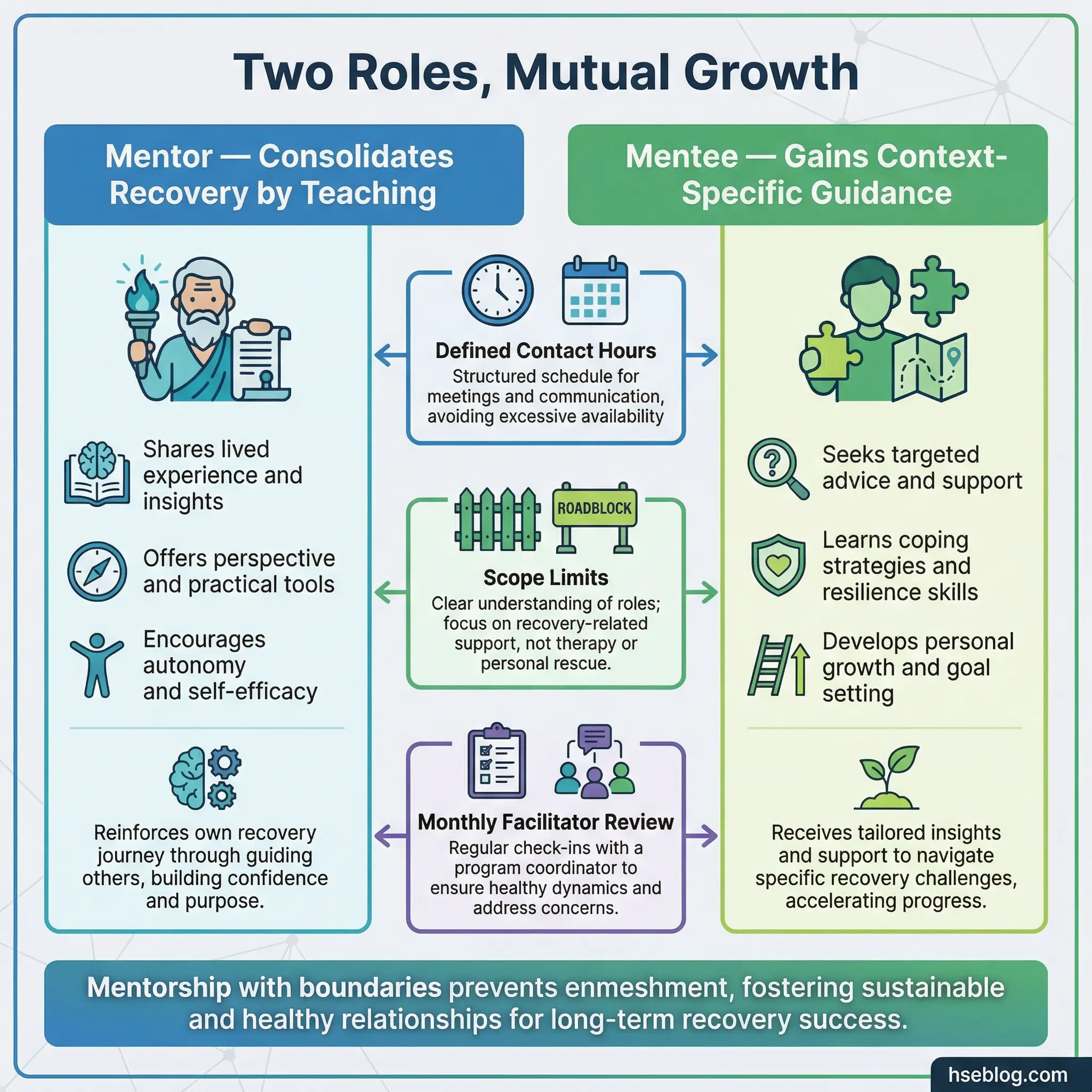
Clear boundaries are established to distinguish mentorship from sponsorship and to prevent the codependency dynamics that unstructured helping relationships can create in recovery settings.
The activity benefits both roles in the pairing:
- Mentors consolidate their recovery by teaching. Articulating recovery principles to someone else requires clarity that internal knowledge does not. Teaching solidifies learning. Mentors also benefit from the accountability of being observed as a role model.
- Mentees gain access to experience. A mentor who has navigated the same treatment program, the same group dynamics, and the same early-recovery challenges provides context-specific guidance that a counselor — no matter how skilled — cannot replicate.
- Boundaries prevent enmeshment. The mentorship agreement includes specific limits — contact hours, topics within scope, and protocols for when to refer back to the facilitator or counselor. These boundaries protect both parties.
- Pairing is reviewed monthly. Not every pairing works. The facilitator checks in with both parties and reassigns when the dynamic is unproductive or unhealthy.
- Session length: 30–40 minutes for initial pairing, boundary discussion, and goal-setting.
Activity 48: Community Resource Scavenger Hunt
The community resource scavenger hunt is a research-based activity where participants work in small teams to compile a comprehensive group directory of local recovery resources — meeting locations and schedules, crisis hotlines, sober recreation options, job training programs, food assistance, housing support, legal aid, and free counseling services.

The collaborative research process itself is therapeutic. It builds initiative, reduces learned helplessness, and produces a practical tool the entire group benefits from.
This exercise addresses the information gap that undermines recovery sustainability:
- It transforms participants from passive recipients to active researchers. The shift from “someone should tell me about resources” to “I found these resources and am sharing them with the group” builds self-efficacy that transfers to other recovery domains.
- The directory has practical value. A compiled, group-verified resource directory with addresses, phone numbers, hours, and member notes about quality is more useful than any list a facilitator could produce alone.
- Teamwork builds connection. Working together on a research task creates the kind of natural, purpose-driven social interaction that many participants have not experienced since before their addiction escalated.
- It reveals resource deserts. If the scavenger hunt reveals that local resources are limited — few meetings, no free counseling, no sober recreation options — that information itself is valuable for advocacy and planning.
- Session length: Typically spans two sessions — one for research assignment and one for compilation and presentation.
Activity 49: Boundary Mapping at Home and Work
Boundary mapping at home and work is a visual assessment exercise where participants draw a “boundary map” of their two primary environments — home and workplace — identifying specific people, spaces, and situations where boundaries need to be established or strengthened.
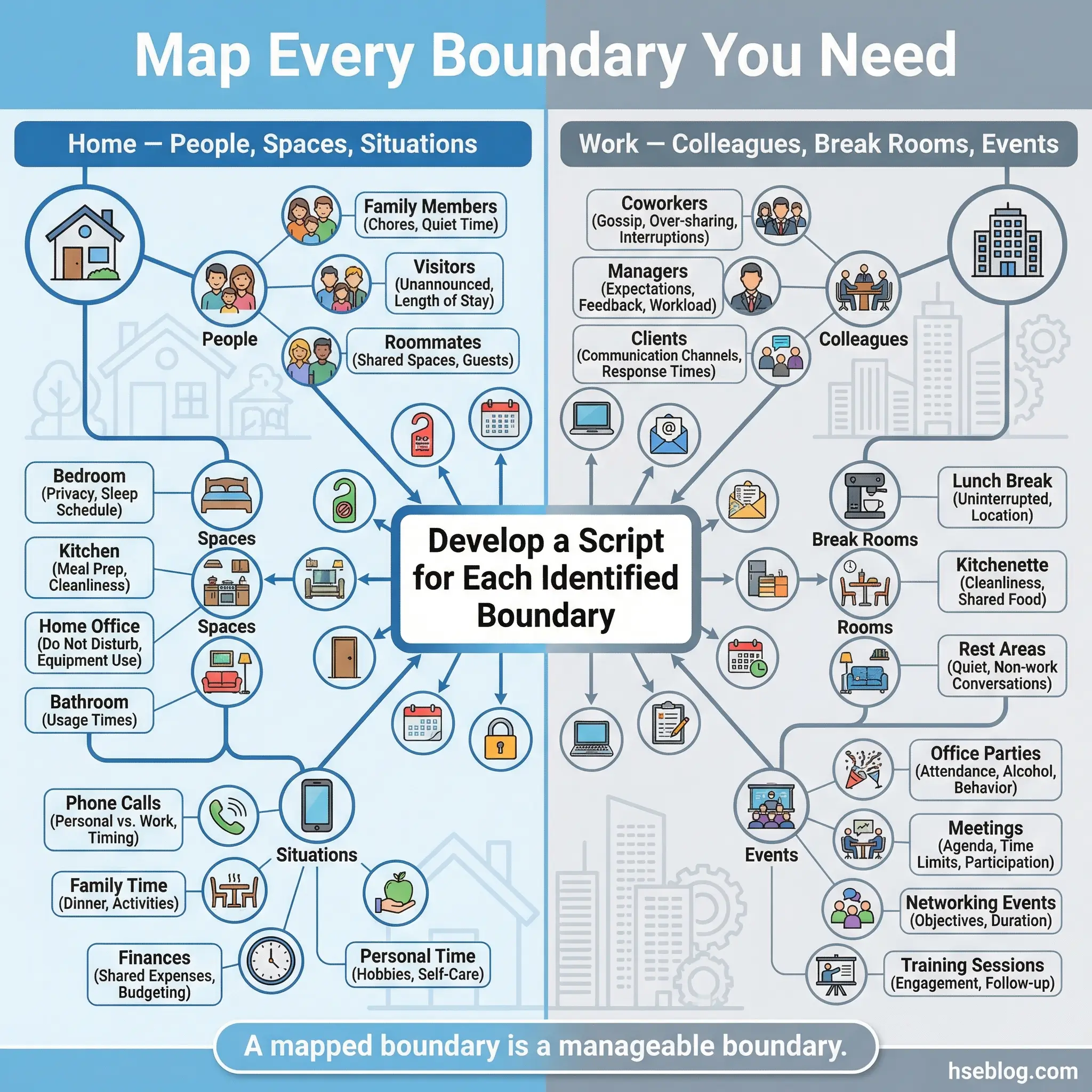
Maps are reviewed by the group, and specific boundary-setting scripts are practiced for each identified area. The exercise connects the interpersonal skills from Activities 11–20 with the practical realities of daily recovery.
This activity moves boundary work from abstract concept to concrete, environment-specific application:
- Physical environments carry triggers. A kitchen where drinking occurred, a break room where colleagues discuss weekend parties, a neighbor who enables — these environmental factors require specific boundary responses that generic “set boundaries” advice does not address.
- Maps identify relationship-specific risks. A participant’s boundary map might reveal that they have strong boundaries with strangers but none with family members — or the reverse. The specificity of the map reveals patterns that general discussion misses.
- Scripts are rehearsed for each boundary. For each identified boundary area, the group develops and practices a specific script — what to say, how to say it, and how to respond to pushback. This preparation converts intention into capability.
- Maps are updated as circumstances change. A new roommate, a job change, or a family event creates new boundary requirements. Periodic map updates keep the tool relevant.
- Session length: 50–60 minutes including mapping, group review, and script practice.
Activity 50: Recovery Vision Board — 90-Day Edition
The recovery vision board — 90-day edition — closes the activity library with a forward-looking planning exercise that differs from traditional vision boards in one critical way: it focuses strictly on the next 90 days. No five-year dreams. No abstract aspirations. Ninety days of specific, measurable, achievable goals across four domains — health, relationships, employment or purpose, and recovery milestones.
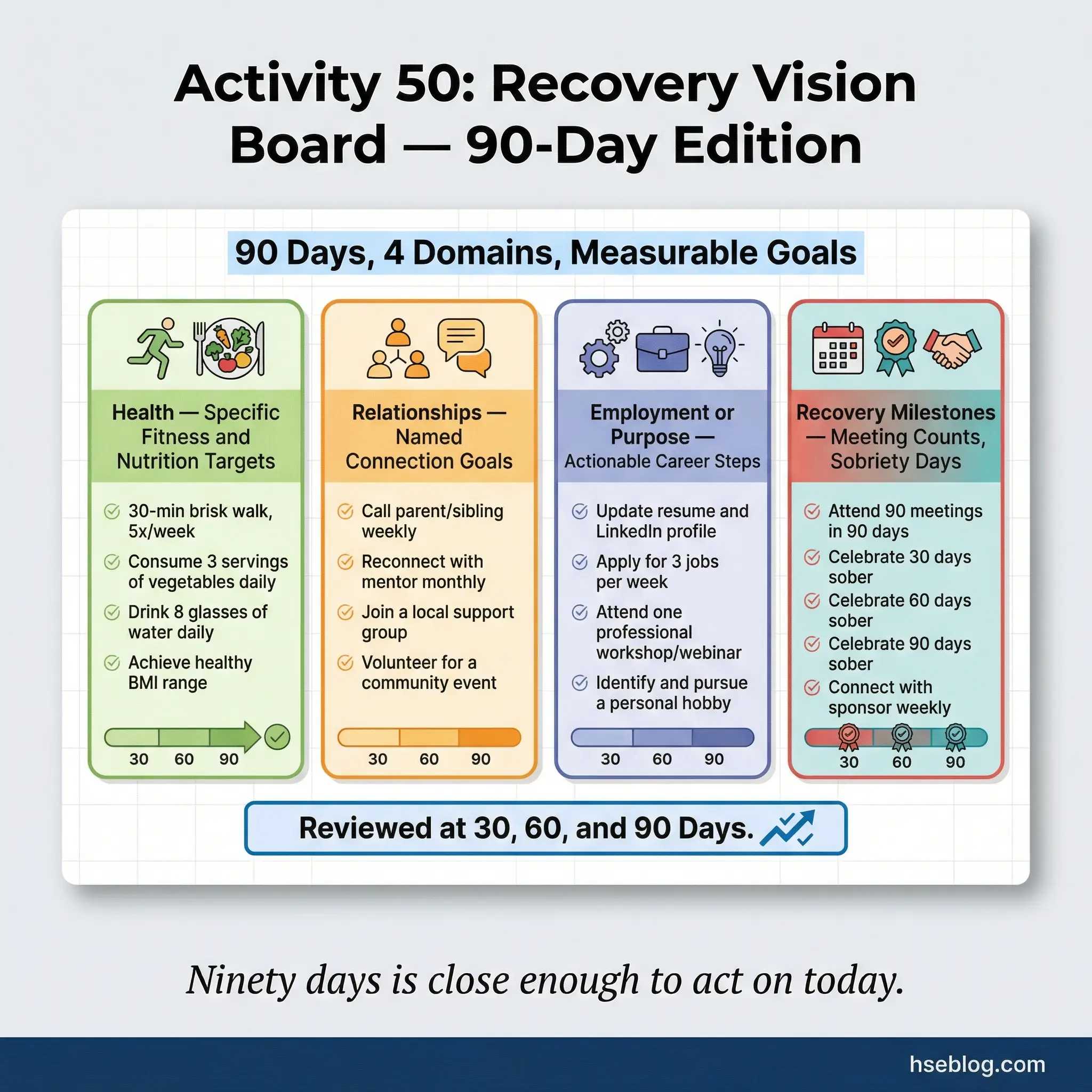
Participants create a visual plan using images, words, timelines, and specific targets. Goals are reviewed monthly, and boards are physically updated to reflect progress, adjustments, and completed milestones.
The 90-day constraint is what makes this activity effective where traditional vision boards fail:
- Ninety days is far enough to be meaningful and close enough to be actionable. A five-year vision board allows infinite procrastination. A 90-day board demands action this week.
- Goals must be measurable. “Get healthier” is not a 90-day goal. “Attend 12 recovery meetings, walk 30 minutes four times per week, and cook meals at home five nights per week for 90 days” is a goal. The measurement criteria are displayed on the board.
- Monthly check-ins create accountability. The board is reviewed at 30, 60, and 90 days. Completed goals are visibly marked. Missed goals are examined for obstacles and revised — not abandoned.
- The four-domain structure prevents tunnel vision. Participants who focus exclusively on one recovery area (often sobriety milestones) while neglecting health, relationships, and employment build an unstable recovery. The board requires attention to all four domains.
- It produces a physical artifact of progress. At 90 days, a board covered in completed milestones provides concrete evidence that recovery works. That evidence is more motivating than any speech or slogan.
- Session length: 50–60 minutes for creation, plus 20–30 minutes for each monthly review session.
How to Choose the Right Substance Abuse Group Activities
Selecting the right activity for the right group at the right time is the skill that separates effective facilitators from those who run through a checklist. The wrong activity at the wrong stage does not just waste time — it damages group trust and can trigger participants who are not ready.
Activity selection should follow a structured assessment that accounts for where the group is in its development, not just what the session plan says:
- Assess group stage first. New groups (first 1–4 sessions) need structured, low-disclosure activities from the Self-Awareness and Communication categories. Attempting a Mask Making exercise (Activity 33) or an Empty Chair exercise (Activity 10) with a group that has not yet established psychological safety will backfire.
- Match emotional intensity to group capacity. After a session that involved heavy emotional disclosure, the next session should use a lighter-intensity activity — a Sober Fun Brainstorm (Activity 28) or a Weekly Schedule Building (Activity 41) — to prevent emotional fatigue.
- Rotate across all five domains. Groups that spend all their time on coping skills without addressing self-awareness produce participants who can manage triggers but cannot identify them. Rotate deliberately across all five domains over any four-week cycle.
- Let the group inform your selection. If energy is low, use a Movement and Rhythm Circle (Activity 40). If conflict is surfacing, use a Fishbowl Conversation (Activity 17). If a participant just experienced a slip, use the Relapse Response Drill (Activity 46). Rigid adherence to a pre-planned sequence ignores what the group actually needs.
- Never repeat an activity without variation. The Trigger Mapping exercise (Activity 1) can be repeated if the second iteration adds new dimensions — mapping emotional triggers versus situational triggers, for example. Exact repetition signals laziness to participants.
| Group Stage | Recommended Activity Types | Activities to Avoid |
|---|---|---|
| Forming (Sessions 1–4) | Feelings Check-In, Trust Walk, Values Sort, Active Listening | Empty Chair, Mask Making, Poetry Slam, Conflict Simulation |
| Storming (Sessions 5–8) | Boundary Setting, Assertiveness Continuum, HALT Check-In | High-intensity role-plays without prior trust-building |
| Norming (Sessions 9–14) | Collage, Thought Record, Accountability Contracts, Mentorship | Activities below the group’s current depth level |
| Performing (Sessions 15+) | Stress Inoculation, Relapse Drill, Vision Board, Full creative exercises | Reverting to icebreaker-level activities without purpose |
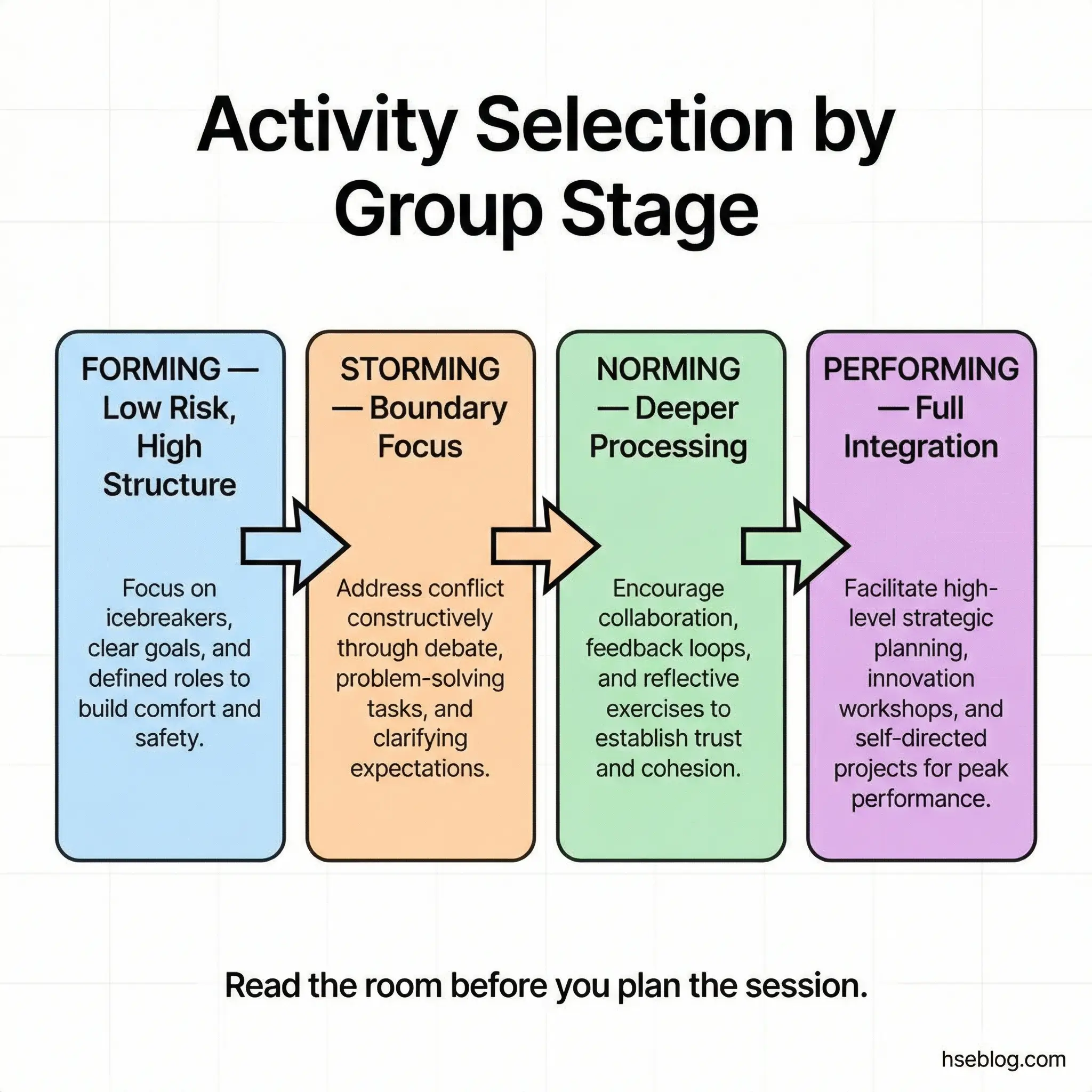
Common Mistakes Facilitators Make with Group Recovery Activities
Even well-intentioned facilitators undermine their own group activities through predictable errors. I have observed these mistakes across dozens of programs, and every one of them is preventable with awareness and preparation.
The following errors consistently reduce the effectiveness of substance abuse group activities — and in some cases, actively harm participants:
- Forcing disclosure too early. Asking participants to share deep personal content before trust is established creates resistance, not breakthroughs. Disclosure must be voluntary, and activities must be sequenced from low to high emotional risk.
- Using activities as entertainment, not treatment. Group activities are clinical tools with specific therapeutic objectives. When a facilitator cannot articulate why a particular activity is being used and what outcome it targets, the activity becomes a time-filler. Participants sense this immediately.
- Skipping the debrief. The activity itself is half the intervention. The debrief — where participants process what they felt, noticed, and learned — is the other half. Cutting the debrief short due to time constraints negates much of the activity’s value.
- Ignoring cultural context. Activities involving physical touch (Trust Walk), creative expression (Poetry Slam), or emotional disclosure (Letter to My Past Self) carry different weight across cultural contexts. A competent facilitator assesses cultural dynamics before selecting activities, not after a participant shuts down.
- Running the same activities every cycle. Participants who attend long-term groups will disengage if they encounter the same exercises repeatedly. Facilitators need a minimum library of 25–30 activities with variations — drawn from diverse substance abuse group topics — to maintain engagement across a six-month cycle.
- Confusing participation with engagement. A participant who completes every activity as directed but never connects emotionally has not benefited. Facilitators must watch for compliant disengagement — going through motions without internal processing — and address it directly.
Pro Tip: Record your debrief questions before the session, not during it. Improvised debriefs tend to be shallow. Planned debrief questions that target specific recovery domains — “What did this activity teach you about your triggers?” versus “How did that feel?” — produce deeper processing and better outcomes.
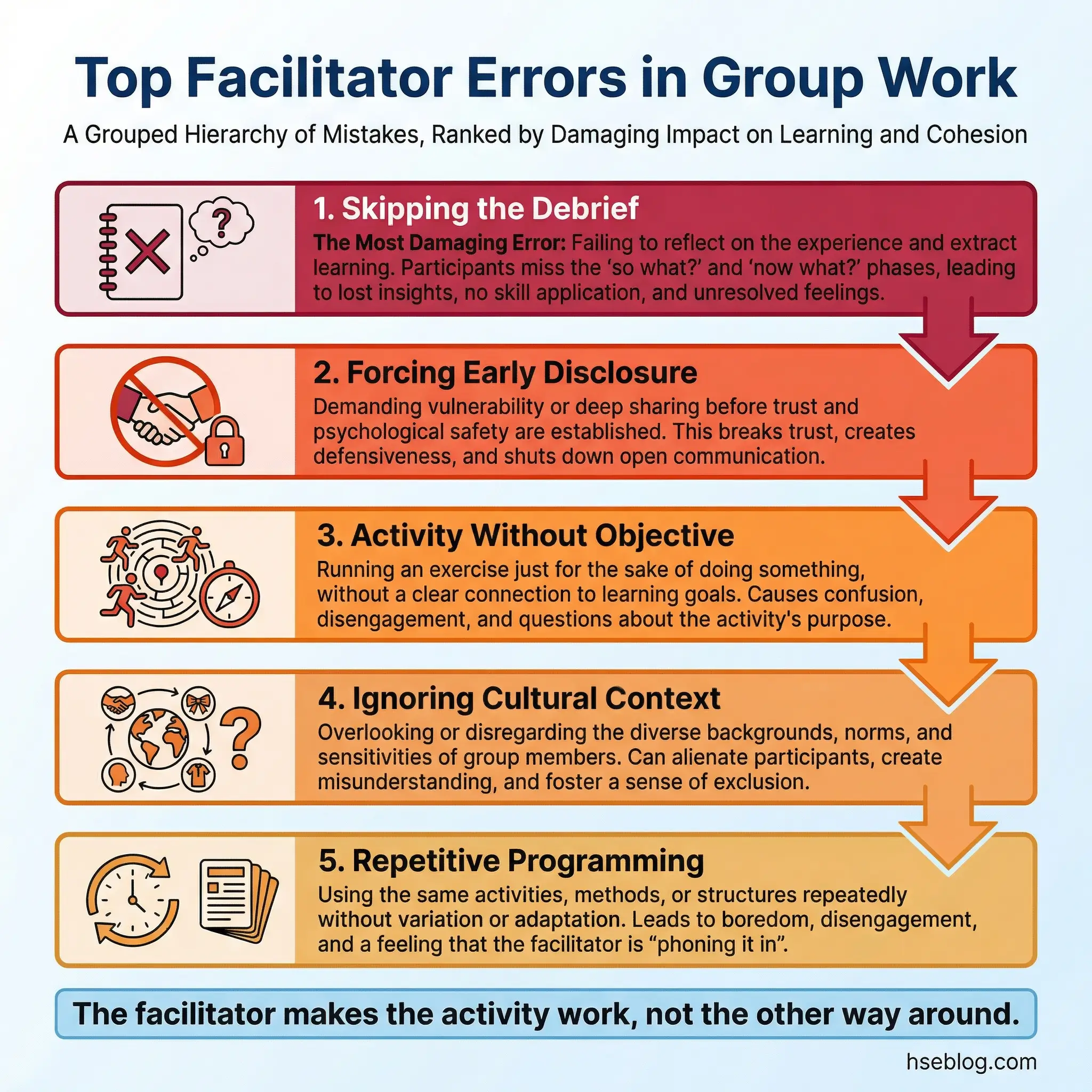
Conclusion
Substance abuse group activities are not supplementary programming. They are the mechanism through which recovery concepts move from abstract ideas into practiced, embodied skills. The 50 activities in this article span the full arc of recovery — from the tentative self-awareness exercises of early sobriety to the structured accountability and life skills work that sustains long-term change. Each one targets a specific domain. Each one requires a facilitator who understands not just how to run the activity, but why it works and when it should be used.
The most important lesson from years of observing these activities in practice is this: the activity is only as effective as the facilitator and the group environment that holds it. A brilliantly designed exercise in the hands of an unprepared facilitator achieves nothing. A simple check-in exercise in the hands of someone who understands group dynamics, reads emotional cues, and knows when to push and when to hold space can change the trajectory of a person’s recovery.
Recovery is not a solo project. It is built in rooms with other people who are willing to be honest, uncomfortable, and accountable. These 50 substance abuse group activities give facilitators the tools to create those rooms — and to fill them with purpose.