

TL;DR
- Group discussions break isolation: Structured substance abuse topics give participants a safe framework to share experiences and challenge denial patterns.
- Topic selection drives engagement: Poorly chosen topics shut groups down; relevant, well-sequenced topics build trust and momentum session by session.
- Coping skills need practice, not lectures: The most effective group topics put participants in active problem-solving mode — not passive listening.
- Mental health and addiction overlap constantly: At least a third of your discussion topics should address co-occurring disorders, trauma, and emotional regulation.
- Facilitators shape outcomes: A strong topic with a weak facilitator fails; preparation, boundaries, and active listening determine whether a session heals or harms.
I sat in on a group recovery session at an occupational rehabilitation center attached to a large logistics operation in the Gulf. Twelve workers — drivers, warehouse crew, two supervisors — sat in a circle. The facilitator opened with “So, does anyone want to talk about their substance use?” Silence. Eleven minutes of silence before one person mumbled something about stress. The session never recovered. Afterward, the facilitator told me the group “just wasn’t ready to open up.” But the group wasn’t the problem. The topic — or rather, the complete absence of a structured one — was.
Substance abuse group discussions are among the most powerful intervention tools available in occupational health, employee assistance programs, and community recovery settings. But their effectiveness depends almost entirely on what you discuss and how you frame it. Vague prompts produce vague silences. Specific, well-chosen substance abuse group topics produce breakthroughs — moments where a participant recognizes a pattern, names a trigger, or commits to a behavior change they’ve been avoiding for months. This article presents 50 field-tested discussion topics organized into practical categories, explains why each one works, and gives facilitators the structure to run sessions that actually change outcomes.
What Are Substance Abuse Group Topics and Why Do They Matter?
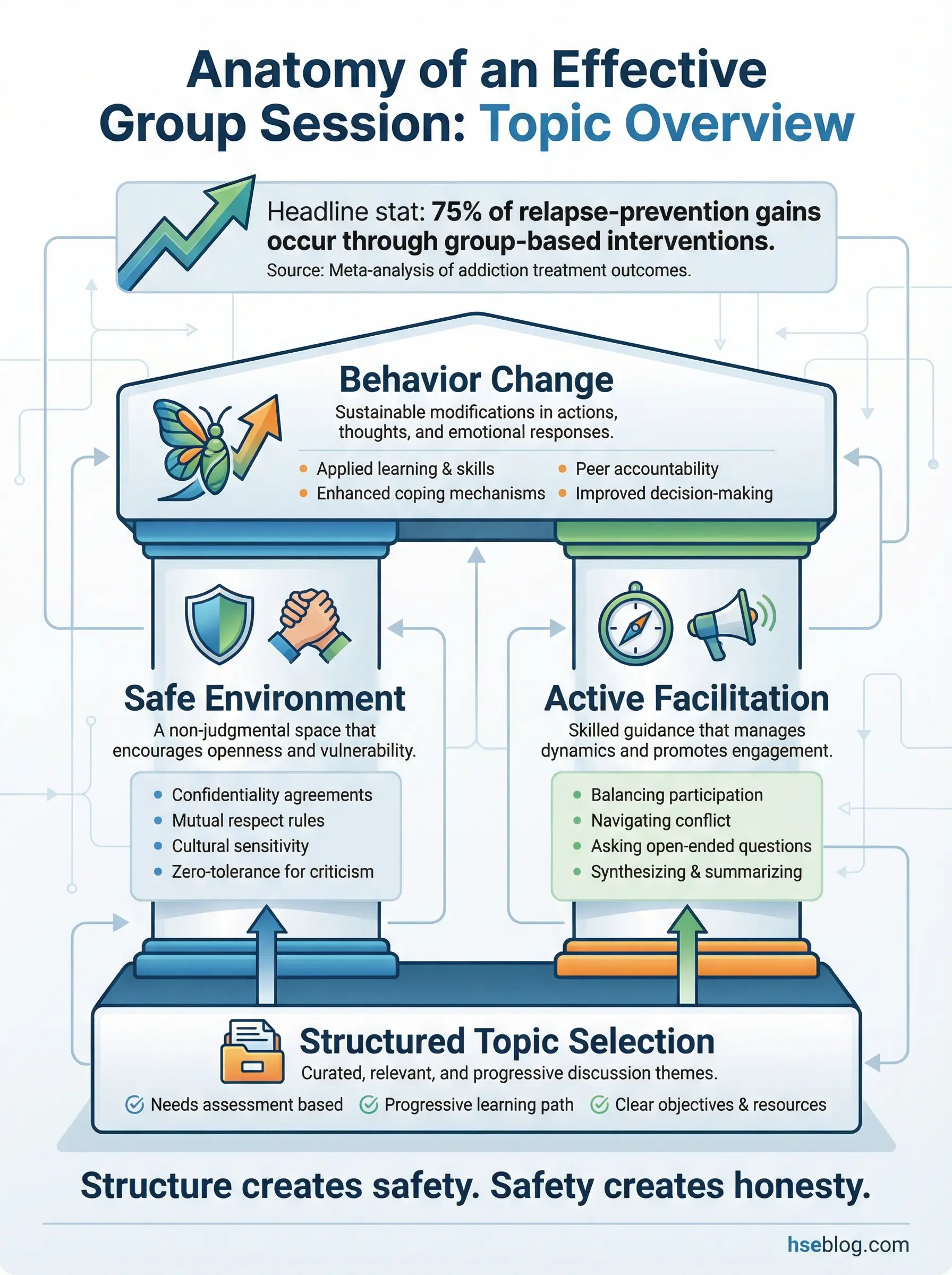
Substance abuse group topics are structured discussion themes designed to guide conversations in group therapy, support groups, workplace recovery programs, and peer counseling sessions. They provide a defined focus for each session, preventing discussions from drifting into unproductive territory or triggering participants without therapeutic support.
The difference between a productive and a damaging group session often comes down to one factor — topic clarity. During my years coordinating employee assistance programs across industrial operations, I watched facilitators struggle most when they walked into a room without a defined discussion topic. Here’s what consistently separates effective groups from ineffective ones:
- Defined topics reduce anxiety: Participants know what to expect, which lowers defensiveness and increases willingness to share. Open-ended sessions feel unsafe for people already carrying shame.
- Sequential topic design builds trust: Starting with low-risk topics like “understanding what addiction is” before moving to high-vulnerability topics like “how my substance use affected my family” mirrors how trust develops naturally.
- Topics create accountability benchmarks: When a participant discusses coping strategies in week three and revisits that same theme in week eight, the group can measure real progress — or honest setbacks.
- Structured discussions prevent facilitator burnout: Without a topic framework, facilitators carry the entire emotional weight of directing conversation. Predefined topics distribute that cognitive load.
The Substance Abuse and Mental Health Services Administration (SAMHSA) identifies structured group therapy as a primary evidence-based treatment modality for substance use disorders, emphasizing that topic-driven sessions produce measurably better engagement and retention than unstructured formats.
Pro Tip: Build your 50-topic roster into a 12–16 week rotation. Map topics from low-vulnerability (education and awareness) to high-vulnerability (trauma, family impact, relapse) so participants’ trust curve matches the emotional intensity curve.
Topics on Understanding Addiction and Its Root Causes (Topics 1–8)
Every group discussion program needs a foundation. Before participants can examine their own behavior, they need a shared language for what addiction is — biologically, psychologically, and socially. I’ve used these as opening-week topics across multiple employee wellness programs, and they consistently produce the highest initial engagement because they feel educational rather than confessional. Nobody is being asked to bare their soul in week one. They’re being asked to learn.
Topic 1: The Brain Science of Addiction
This topic strips away the moral judgment that most participants carry into their first group session. When you explain that substances physically alter the brain’s dopamine reward pathways — that repeated exposure creates neurological changes in the prefrontal cortex and amygdala that impair decision-making and impulse control — the room shifts. I’ve watched participants physically relax when they understand that addiction is not a character flaw but a measurable brain change.
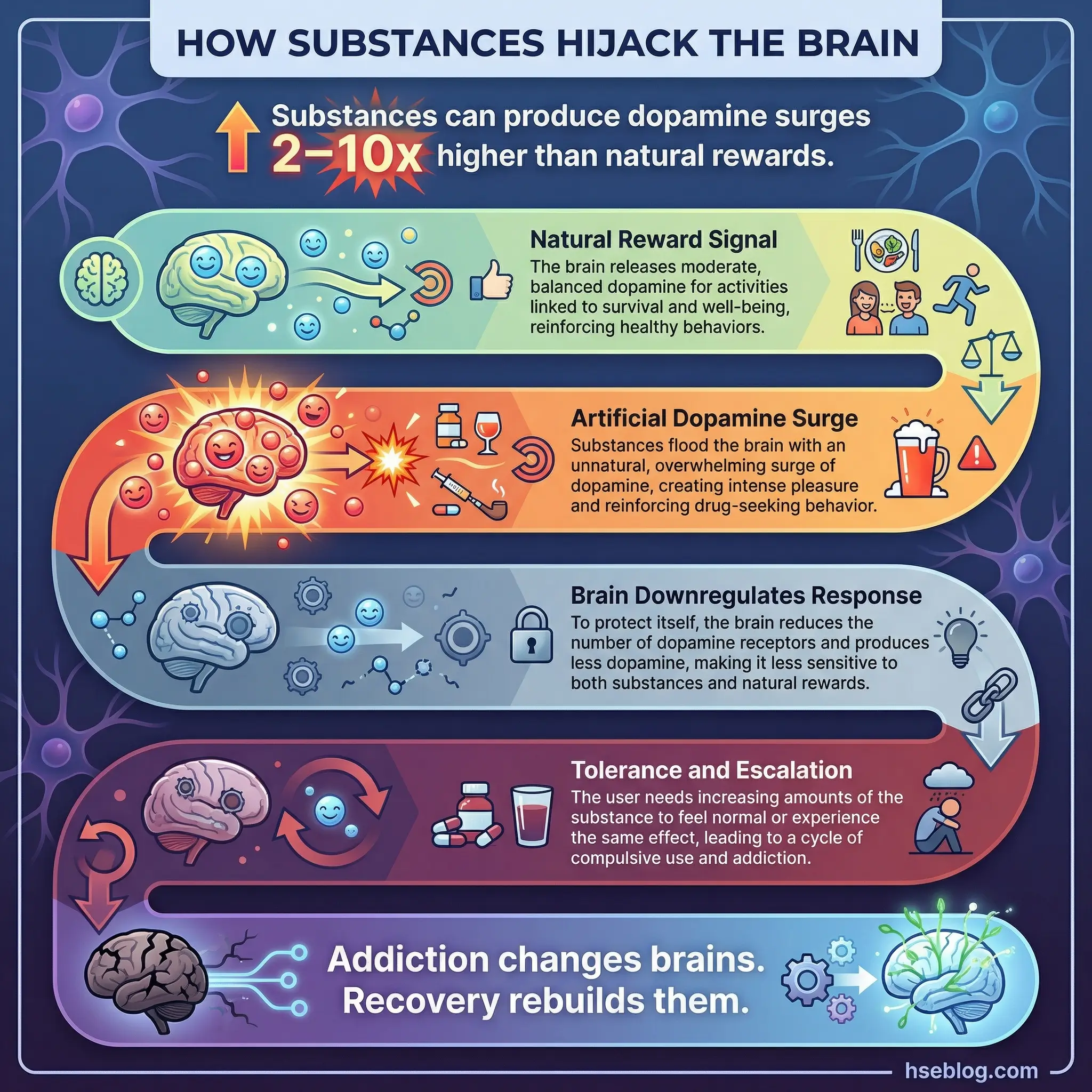
Walk the group through the neuroscience in plain language, using whiteboard sketches rather than clinical slides. The goal is for every participant to leave this session able to explain to someone else why “just stopping” is a neurological challenge, not a willpower shortcut.
- Dopamine hijacking: Explain how substances produce dopamine surges 2–10 times higher than natural rewards, and why the brain downregulates its own production in response.
- Tolerance and escalation: Connect the neuroscience to the lived experience — why the same amount stops working and why doses increase over time.
- Prefrontal cortex impairment: Describe how repeated substance exposure weakens the brain’s decision-making center, making rational choices physically harder.
- Neuroplasticity and recovery: End on the critical positive — the brain can rewire. Recovery is literally the brain rebuilding pathways that addiction damaged.
Topic 2: The Disease Model vs. the Choice Model
This topic generates more debate than any other in the opening sessions — and that’s exactly why it works. Present both perspectives fairly. The disease model, supported by the American Medical Association and most addiction medicine bodies, frames addiction as a chronic, relapsing brain disease requiring medical treatment. The choice model, still common in public perception and some policy frameworks, holds that substance use involves a series of voluntary decisions and that framing it as a disease removes personal accountability.
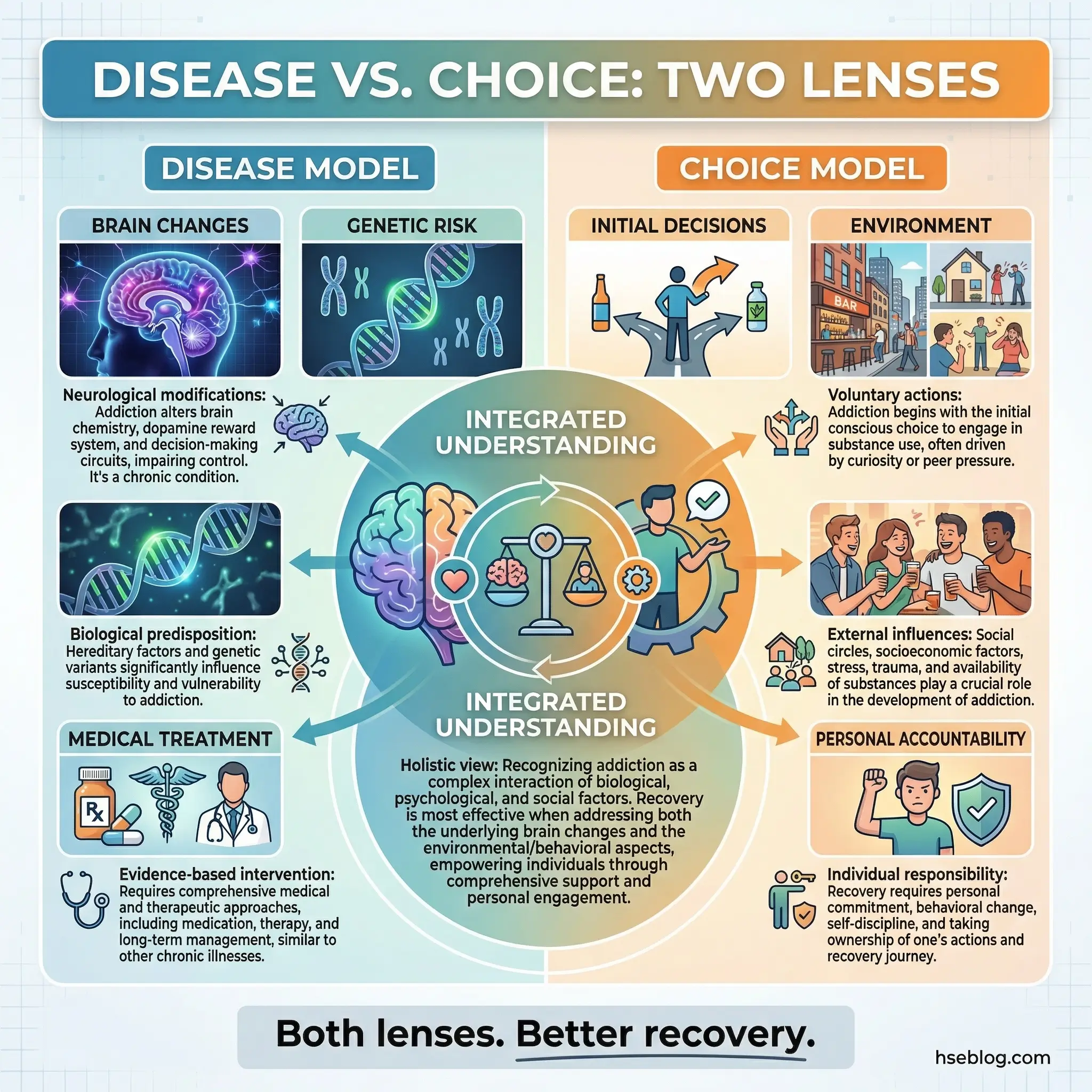
Run this as a structured debate, not a lecture. Let participants argue both sides. Most arrive firmly in the “choice” camp — especially those still carrying guilt — and gradually move toward a more nuanced view that holds both neurological reality and personal responsibility in tension.
- Disease model evidence: Present AMA classification, brain imaging studies, and genetic research that supports addiction as a medical condition with biological markers.
- Choice model arguments: Acknowledge the role of initial decisions, environmental factors, and the reality that many people with risk factors never develop addiction.
- The nuanced middle ground: Guide the group toward understanding that both biology and behavior matter — medical reality doesn’t erase accountability, and personal responsibility doesn’t erase neuroscience.
- Why this debate matters for recovery: How a participant frames their addiction directly affects their treatment engagement, self-concept, and willingness to seek medical support.
Topic 3: Genetic and Environmental Risk Factors
Family history of addiction, adverse childhood experiences, socioeconomic deprivation, early exposure to substances, and living in communities where substance use is normalized — these are not excuses. They are documented, measurable risk multipliers. Research consistently shows that substance abuse risk factors include a genetic component accounting for 40–60% of addiction vulnerability.
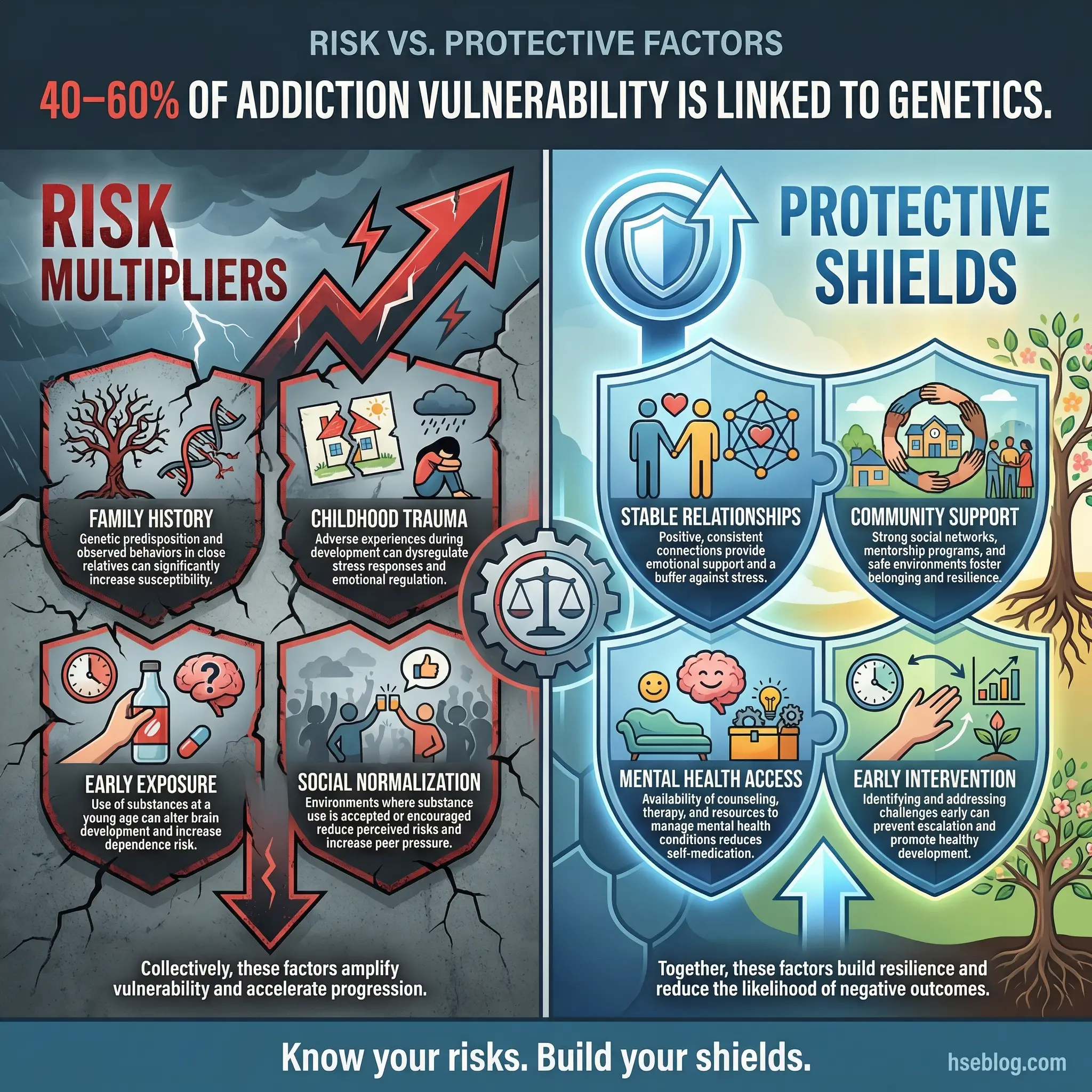
Present this data without letting the group use it as a reason to avoid accountability. The framing matters: “Understanding your risk factors doesn’t remove your responsibility — it helps you understand why your path to addiction was steeper than someone else’s, and what protective factors you need to build deliberately.”
- Genetic predisposition: Explain the 40–60% heritability figure — what it means and what it doesn’t. Having a genetic risk doesn’t guarantee addiction, but ignoring it is reckless.
- Adverse childhood experiences (ACEs): The dose-response relationship between childhood trauma and adult substance use. Higher ACE scores correlate with higher addiction rates across every demographic.
- Environmental normalization: How growing up in households or communities where substance use is routine recalibrates a person’s baseline of “normal.”
- Protective factors: Stable relationships, community connection, early intervention, education, and access to mental health support. Risk factors are not destiny when protective factors are built deliberately.
Topic 4: The Cycle of Addiction
Map the full cycle on a whiteboard: initial use, regular use, risky use, dependence, addiction, and the consequences that either trigger treatment or deepen the cycle. Every participant is somewhere on this cycle, and seeing it drawn out — rather than described in abstract terms — creates recognition.
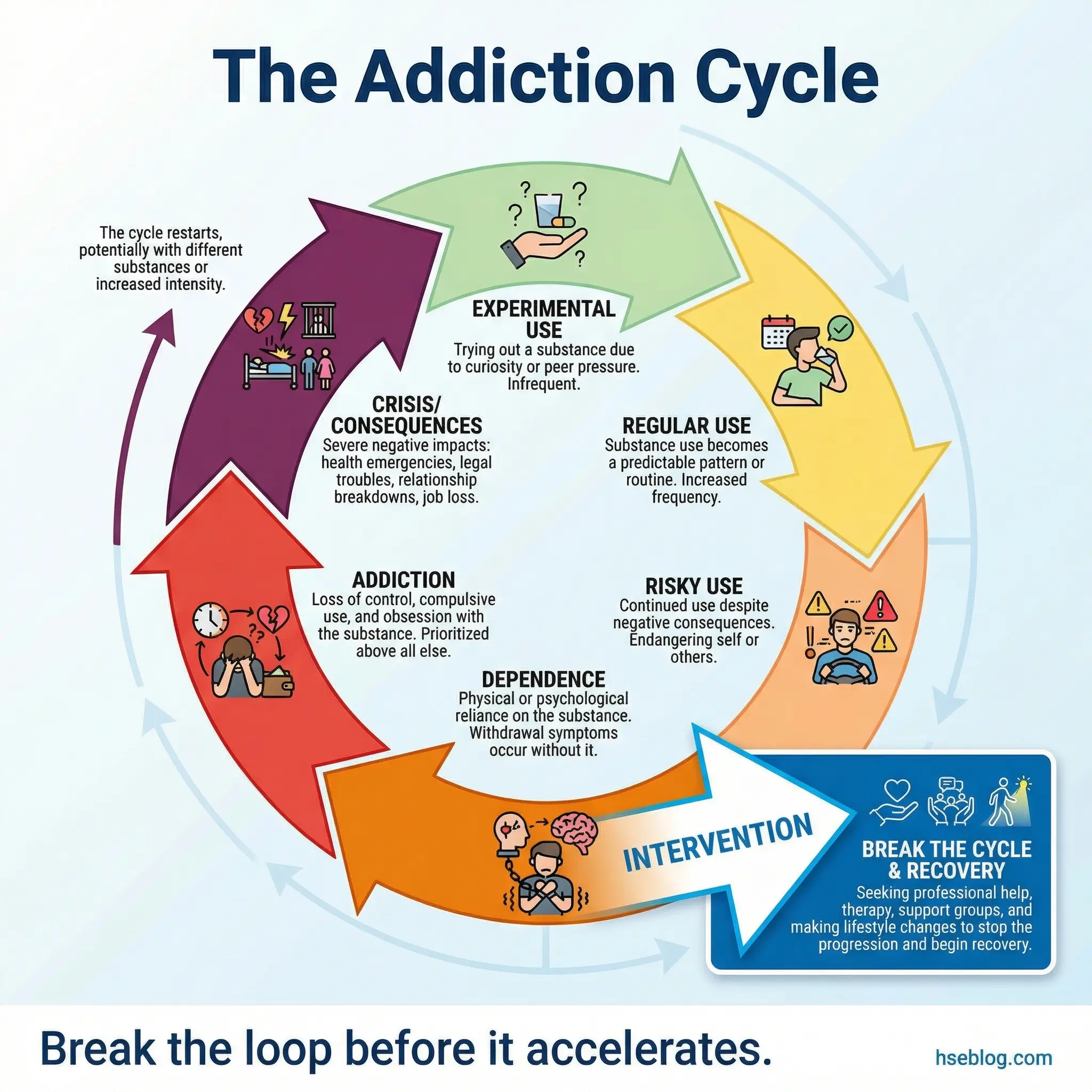
I facilitated this topic at a contractor rehabilitation program for a large energy company, and one electrician pointed at the “risky use” phase and said, “I spent three years right there, telling myself I hadn’t crossed the line.” That moment of recognition is the entire purpose of this topic.
- Six stages visualized: Initial/experimental use → regular use → risky/hazardous use → dependence → addiction → crisis/consequences. Draw the loop so participants see how each stage feeds the next.
- Acceleration pattern: Discuss how each loop through the cycle tends to be faster and more destructive than the previous one. The time between stages compresses with repetition.
- Intervention points: Identify where the cycle can be broken — and be honest about why earlier intervention produces better outcomes than crisis-driven treatment.
- Self-placement exercise: Ask participants to privately identify where they currently sit on the cycle. No sharing required — the internal recognition is what matters.
Topic 5: Workplace Culture and Substance Use
Every industry has its own relationship with substance use, and pretending otherwise insults the participants’ intelligence. Long-haul transport drivers use stimulants to meet delivery deadlines. Oil rig crews binge-drink during rotational leave. Construction workers self-medicate chronic pain from physically demanding labor. Healthcare professionals have access to controlled substances that the general population doesn’t.
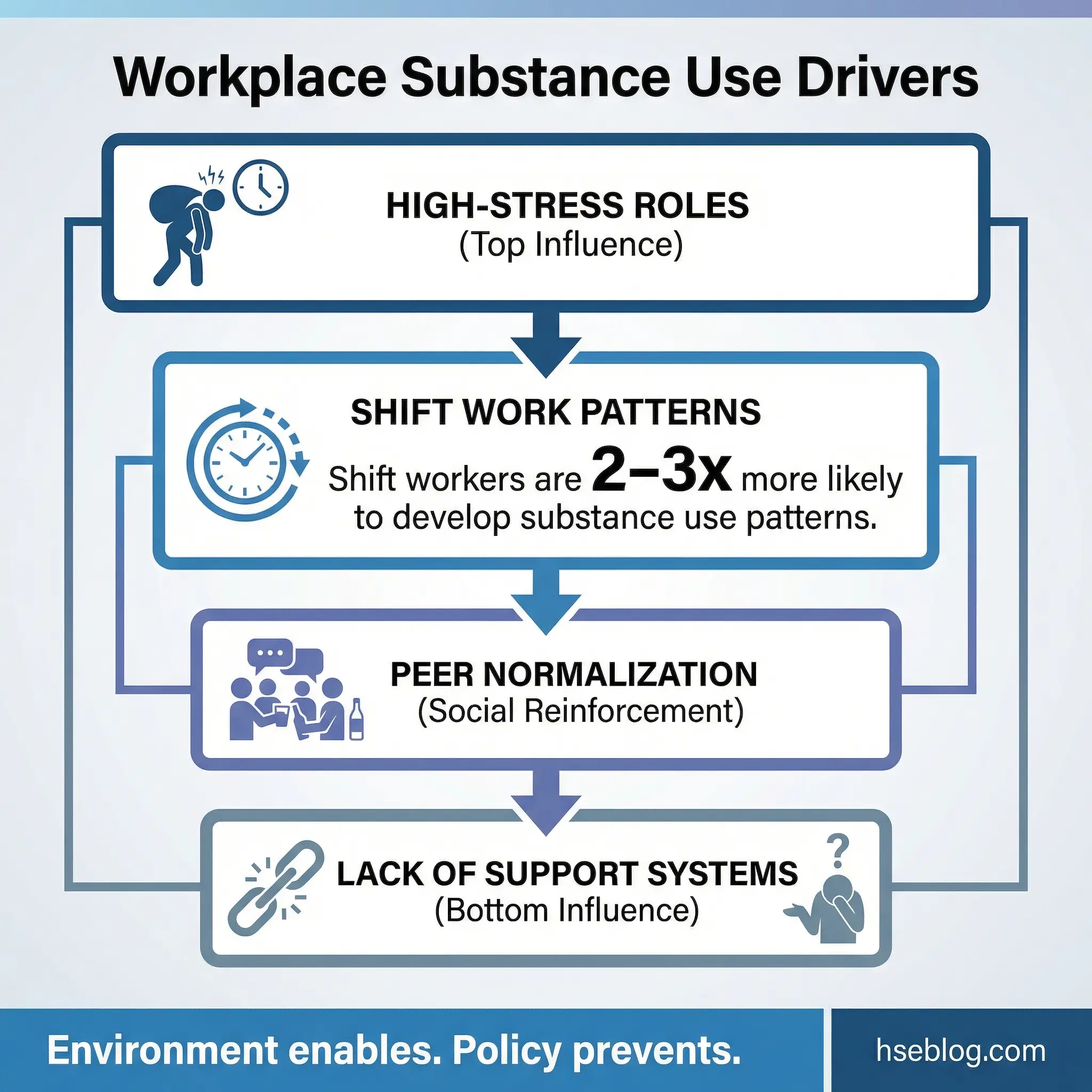
I’ve facilitated this discussion in mining camps in Western Australia where alcohol was the default social activity, and the most powerful moments came when participants realized the environment wasn’t neutral — it was actively enabling.
- Industry-specific patterns: Each sector has its own high-risk substance profile. Stimulants in transport, alcohol in resource extraction, opioids in physically demanding trades, prescription misuse in healthcare.
- Shift work and binge patterns: Rotational rosters, long-haul schedules, and irregular hours create feast-or-famine social cycles that normalize binge behavior during off-periods.
- Peer pressure masquerading as culture: “Everyone drinks after shift” isn’t culture — it’s normalization. Help participants distinguish between genuine camaraderie and substance-centered social pressure.
- Organizational responsibility: Discuss what systemic changes reduce substance use risk — shift schedule redesign, peer support programs, rehabilitation-focused substance abuse policies, and accessible mental health services.
Topic 6: Types of Substance Abuse
Many participants enter recovery focused narrowly on their primary substance — “I’m here for alcohol” or “My problem is opioids.” This topic broadens their understanding of the full spectrum and, critically, stops the dangerous comparison game where someone minimizes their own use because “at least I’m not using something harder.”
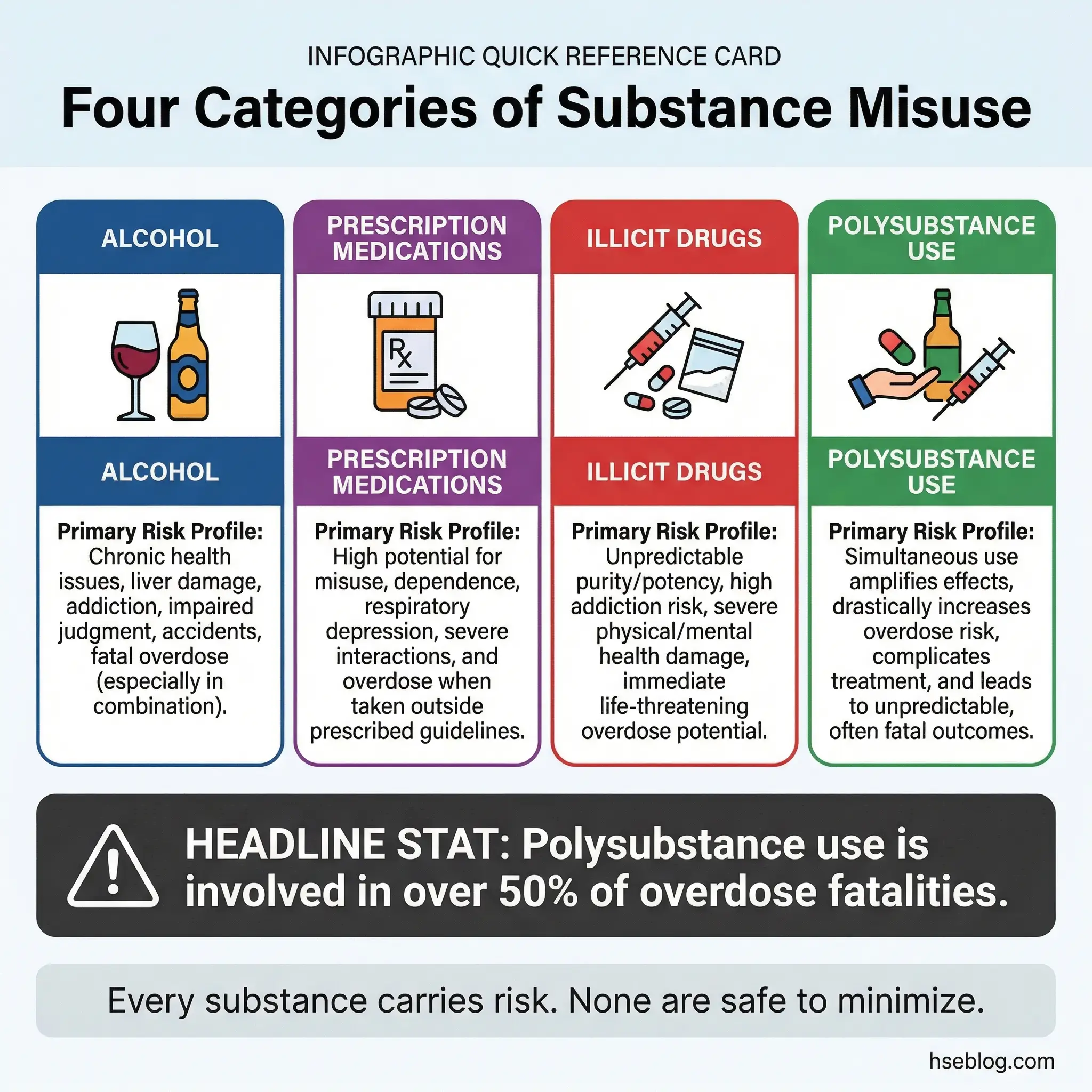
Understanding types of substance abuse matters because it helps participants recognize cross-addiction risks. I’ve seen participants in opioid recovery dismiss their escalating alcohol consumption as “not a real problem” because it wasn’t the substance that brought them into treatment. That blind spot kills people.
- Alcohol: The most socially accepted and widely abused substance globally. Its legality makes it the easiest to minimize and the hardest to avoid in social settings.
- Prescription medications: Opioid painkillers, benzodiazepines, stimulants (ADHD medications), and sleep aids. The “prescribed by a doctor” perception delays recognition of misuse.
- Illicit drugs: Methamphetamine, cocaine, heroin, synthetic cannabinoids, and MDMA. Discuss without moral hierarchy — each substance carries its own dependency profile and health risks.
- Polysubstance use: The increasingly common pattern of combining two or more substances simultaneously. Polysubstance use exponentially increases overdose risk and complicates treatment.
Topic 7: Stigma and Its Role in Preventing Help-Seeking
Stigma is the single largest barrier between a person who needs help and the help itself. During an employee assistance program I helped design for a multinational logistics company, we surveyed 400 workers anonymously. Over 60% said they would not seek help for a substance problem through company channels because they feared career consequences. That statistic drove the entire program redesign.
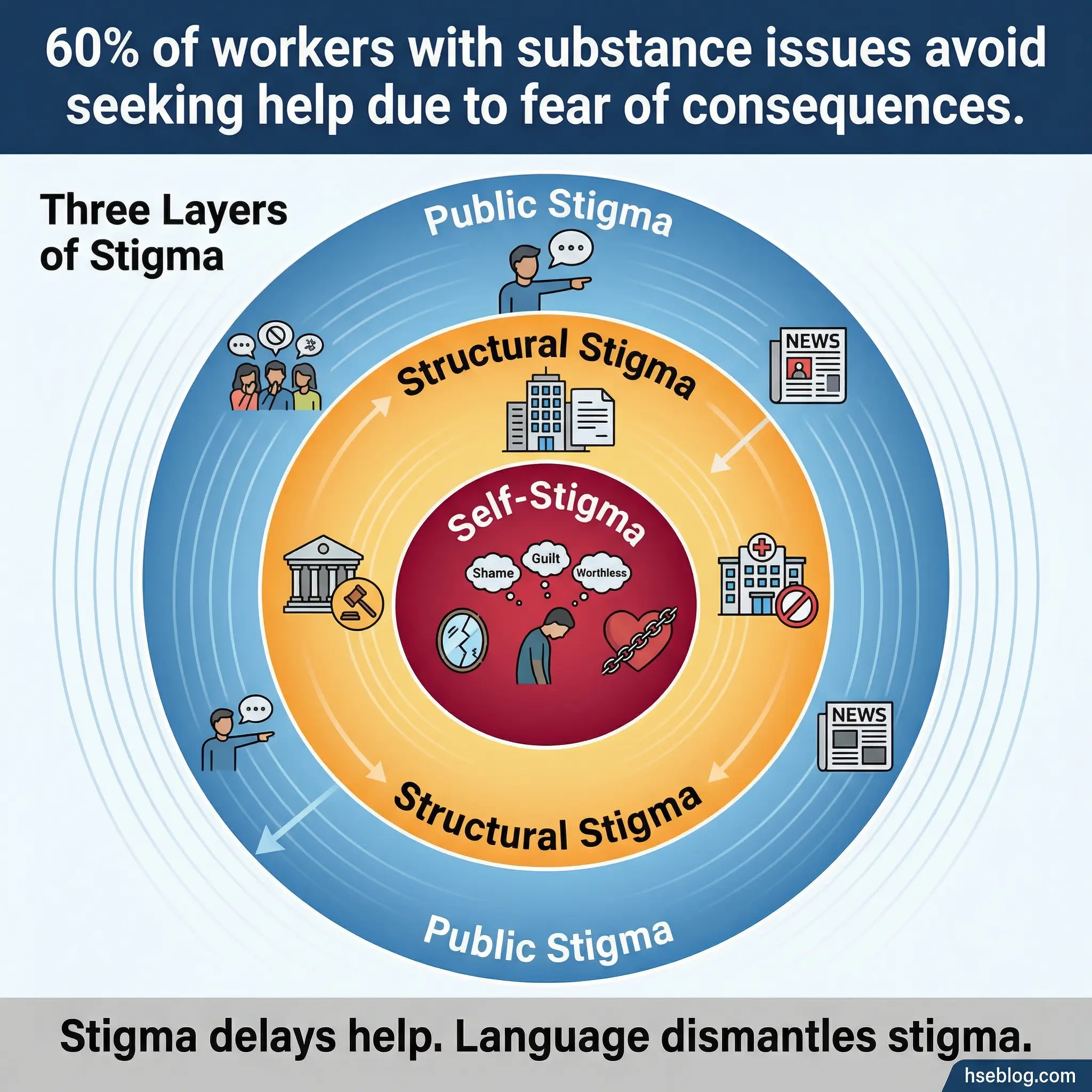
This topic examines three layers of stigma, and it’s one of the most emotionally charged discussions in the early program stages. Set clear ground rules before opening it.
- Public stigma: Society’s judgment — the “junkie” label, media portrayals, community exclusion. Discuss how public stigma creates shame that drives substance use underground instead of into treatment.
- Structural stigma: Policies and systems that punish rather than treat. Zero-tolerance termination policies, criminal records that follow people for decades, insurance systems that limit treatment access.
- Self-stigma: The internalized shame that convinces people they don’t deserve recovery, that they’re fundamentally broken, or that asking for help is weakness.
- Language as intervention: Specific shifts — “substance use disorder” instead of “addict,” “person in recovery” instead of “former junkie” — are not political correctness. They are tools that change how participants think about themselves.
Topic 8: The Economic and Social Cost of Addiction
Numbers land harder than moral arguments. The International Labour Organization estimates that substance use disorders cost employers 3–5% of GDP in lost productivity, absenteeism, healthcare costs, and workplace incidents. At the individual level, the financial trajectory of addiction follows a predictable and devastating curve.
I present this topic using a simple worksheet: participants estimate their personal financial cost of substance use over the past year. The total usually shocks them. It’s not a guilt exercise — it’s a clarity exercise. Understanding what addiction has already cost makes the investment in recovery feel rational rather than emotional.
- Employer-level costs: Lost productivity, increased absenteeism, higher healthcare claims, workplace incidents attributed to impairment, and recruitment costs from turnover driven by substance-related terminations.
- Individual financial damage: Escalating cost of the substance itself, lost wages, legal fees from DUI or possession charges, medical costs from health complications, and compounding credit damage.
- Social capital erosion: Damaged relationships, lost professional reputation, community standing decline, and the cost of rebuilding trust measured not in money but in years.
- The cost-of-inaction calculation: Compare the financial cost of treatment and recovery support against the projected cost of continued use over 5 and 10 years. Recovery is the cheaper option by every measure.
Topics on Recognizing Warning Signs and Triggers (Topics 9–16)
Awareness without recognition is incomplete. These eight topics train participants to identify the behavioral, emotional, and situational cues that precede substance use — both in themselves and in colleagues. During a toolbox talk adaptation I developed for a mining operation in Western Australia, we called this section “reading the dashboard before the engine fails.” The metaphor stuck because every participant understood machines. Learning to read their own warning indicators required the same discipline.
Topic 9: Personal Trigger Mapping
This is one of the most practically valuable exercises in the entire 50-topic program. Each participant creates a written map of their personal triggers — the specific situations, emotions, people, places, and physical sensations that precede their substance use. Addiction feels chaotic from the inside, but trigger mapping reveals patterns that are remarkably consistent.
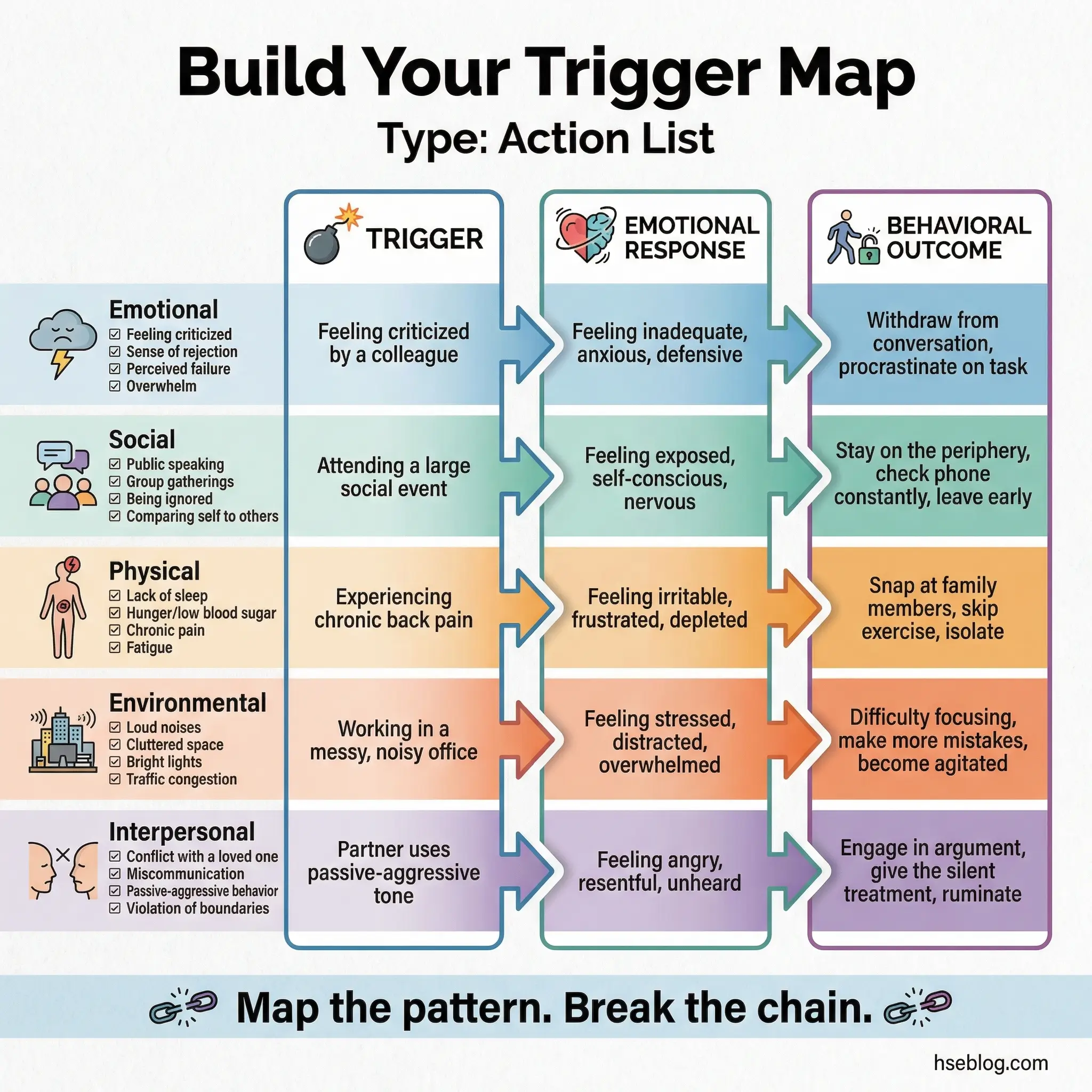
The mapping follows a three-column format: the trigger itself, the emotional or physical state it produces, and the behavior it typically leads to. Do the exercise in writing first, then share voluntarily.
- Five trigger categories: Emotional states, social situations, physical sensations, environmental cues (locations, times of day), and interpersonal conflicts. Each participant identifies their top triggers across all five categories.
- Three-column worksheet: Trigger → Feeling It Produces → Behavior It Leads To. Example: “Argument with partner → helplessness and anger → drive to the bar.”
- Pattern recognition: Most participants discover that 2–3 triggers account for 80% of their substance use. That concentration is what makes targeted coping strategies possible.
- Living document: The trigger map isn’t a one-time exercise. Participants update it as self-awareness deepens throughout the program. What they identify in week two will be more refined by week ten.
Pro Tip: Give each participant a blank trigger map template to keep. Completed maps become personal relapse-prevention tools they carry after the program ends.
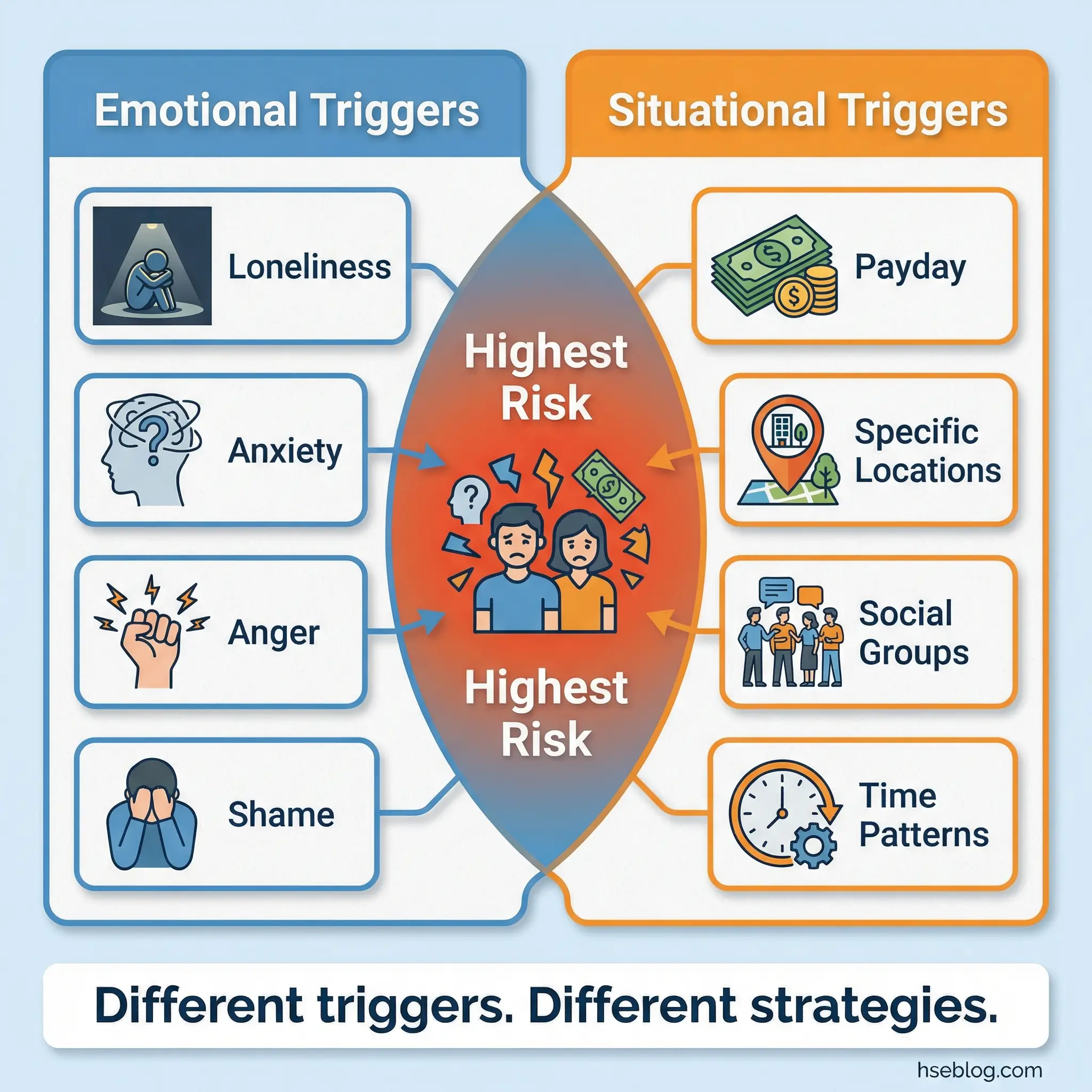
Topic 10: Emotional Triggers vs. Situational Triggers
This distinction matters because each type requires a different response strategy. Emotional triggers — loneliness, boredom, anxiety, anger, shame, grief — live inside the person and travel everywhere. Situational triggers — payday, a specific bar, a friend’s house, the end of a work shift — are external and can be partially controlled through avoidance or restructuring.
I teach this distinction early because participants who don’t understand it build coping strategies aimed at the wrong target. Avoiding a bar is useless if the real trigger is the loneliness that drives you there.
- Emotional triggers identified: Loneliness, boredom, anxiety, anger, shame, grief, frustration, and feelings of inadequacy. These are internal states that travel with the person regardless of environment.
- Situational triggers identified: Payday, specific locations, particular social groups, time-based patterns (Friday evenings, end of shift), celebrations, and post-conflict moments.
- Why the distinction matters: Emotional triggers require internal coping skills (mindfulness, cognitive reframing, emotional regulation). Situational triggers can be partially managed through environmental modification and planning.
- The combined trigger effect: The highest-risk moments occur when emotional and situational triggers converge — payday (situational) combined with work stress (emotional), for example.
Topic 11: High-Risk Situations in the Workplace
Every industry has its own high-risk windows for substance use, and those windows are often predictable. End-of-project celebrations, work travel with per diem allowances, overnight shifts with minimal supervision, post-incident stress, and shutdown or turnaround periods where work intensity spikes and then abruptly stops — these are the moments where workplace substance use concentrates.
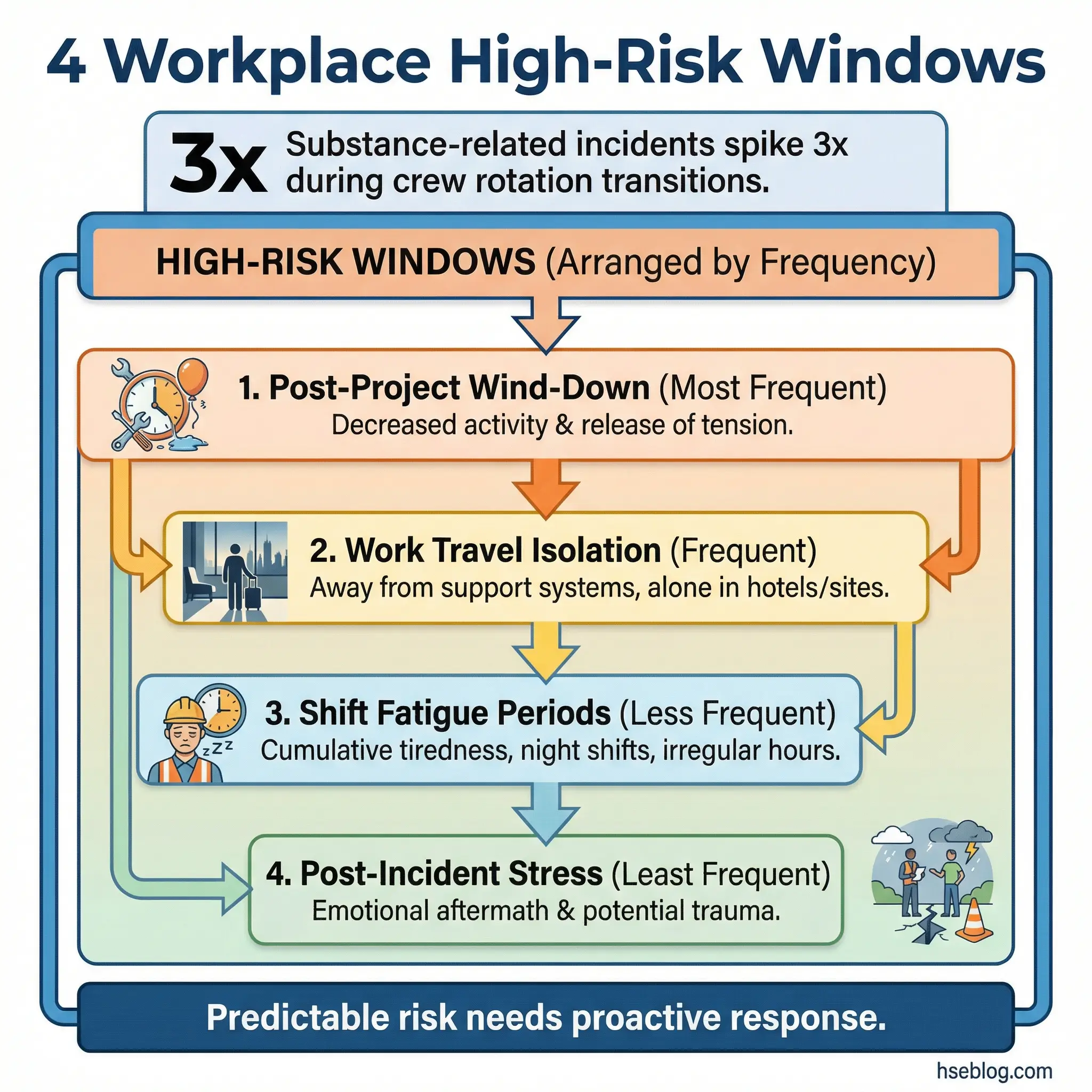
During a pipeline construction project in the Middle East, I tracked incident data and found that substance-related incidents clustered in two specific windows: the first 48 hours after crew rotation arrival, and the final week before demobilization. Both periods shared a common factor — disrupted routine.
- Post-project wind-down: The abrupt shift from high-intensity work to unstructured downtime creates a vulnerability window. Workers who’ve been operating under pressure for weeks suddenly have no structure.
- Work travel and isolation: Hotels, per diem allowances, separation from family and accountability structures, and the anonymity of being in an unfamiliar city.
- Shift transitions and overnight work: Fatigue impairs judgment. Occupational stress compounds with sleep deprivation. Night shift workers have fewer social support resources available during their active hours.
- Post-incident stress: After a workplace accident, near-miss, or fatality, the emotional load on crews is massive. Without structured psychological first aid, self-medication fills the void.
Topic 12: The Role of Stress and Fatigue in Relapse
Occupational stress and substance use share a documented feedback loop. Stress drives use, use worsens performance, poor performance increases stress, and the loop tightens. Fatigue compounds this by impairing the prefrontal cortex — the same brain region already compromised by addiction — making rational decision-making physically harder.
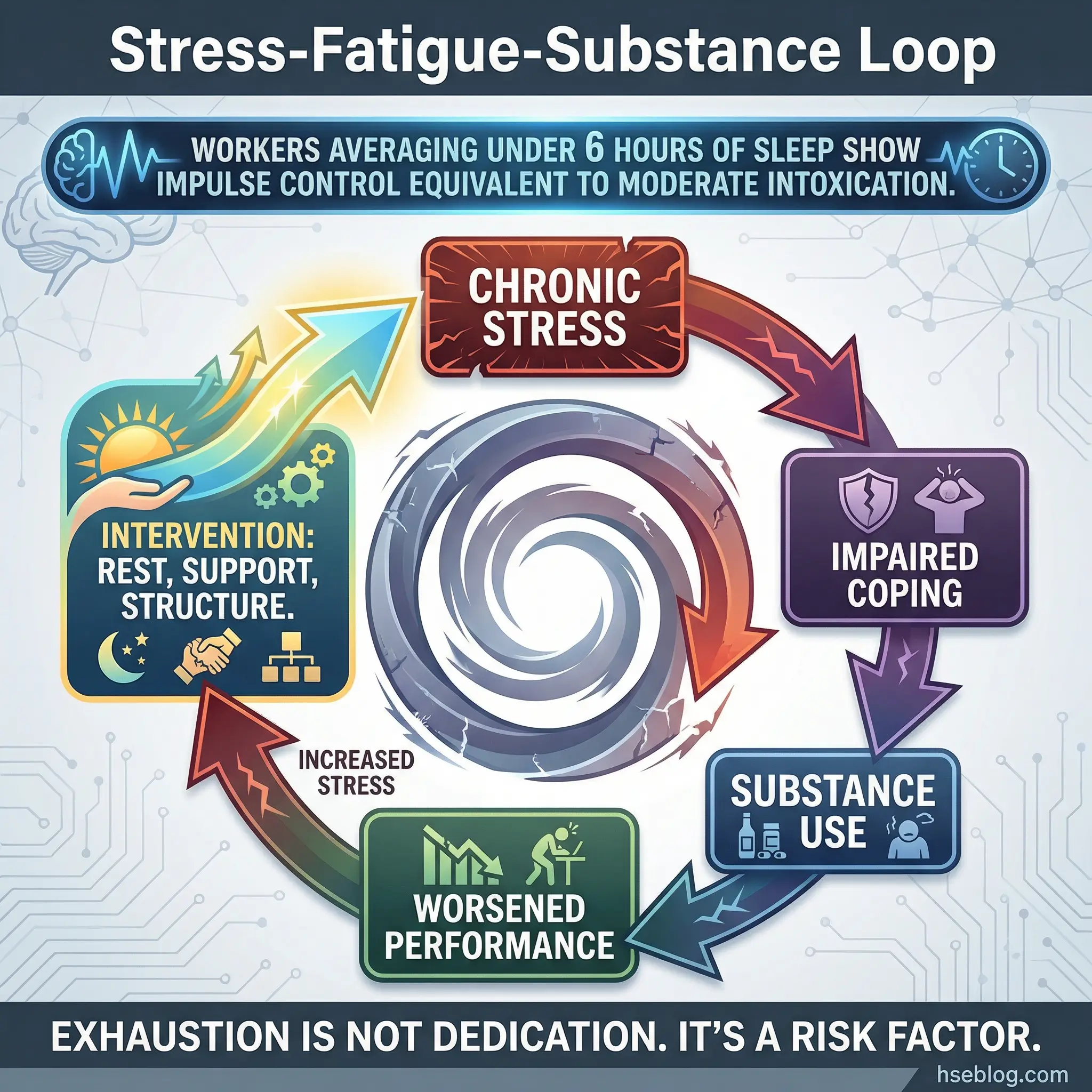
I’ve seen this cycle play out in every high-demand industry I’ve worked in. The workers most at risk aren’t the disengaged ones — they’re the overcommitted ones. The ones who say yes to every extra shift and manage their exhaustion chemically.
- Stress-substance feedback loop: Chronic stress elevates cortisol, which increases cravings. Substance use provides temporary cortisol relief, reinforcing the cycle. The relief is chemical, not psychological — it solves nothing and worsens everything.
- Fatigue and impaired decision-making: Sleep deprivation under 6 hours per night reduces impulse control to levels comparable to moderate alcohol intoxication. Exhausted people make the same poor decisions as intoxicated ones.
- Chronic vs. acute stress: A single bad day (acute stress) is manageable with basic coping tools. Months of sustained overwork (chronic stress) erode coping capacity until the path of least resistance is the substance.
- Recovery-protective work practices: Adequate rest periods, enforced maximum working hours, access to psychological support, and workload monitoring are not luxuries — they’re relapse prevention infrastructure.
Topic 13: Warning Signs Others Can See
This topic flips the perspective. Instead of asking “what are my triggers,” it asks “what do other people notice before I notice it myself?” The observable behavioral changes that precede a relapse or active substance use are often visible to colleagues, supervisors, and family members weeks before the person themselves acknowledges a problem.
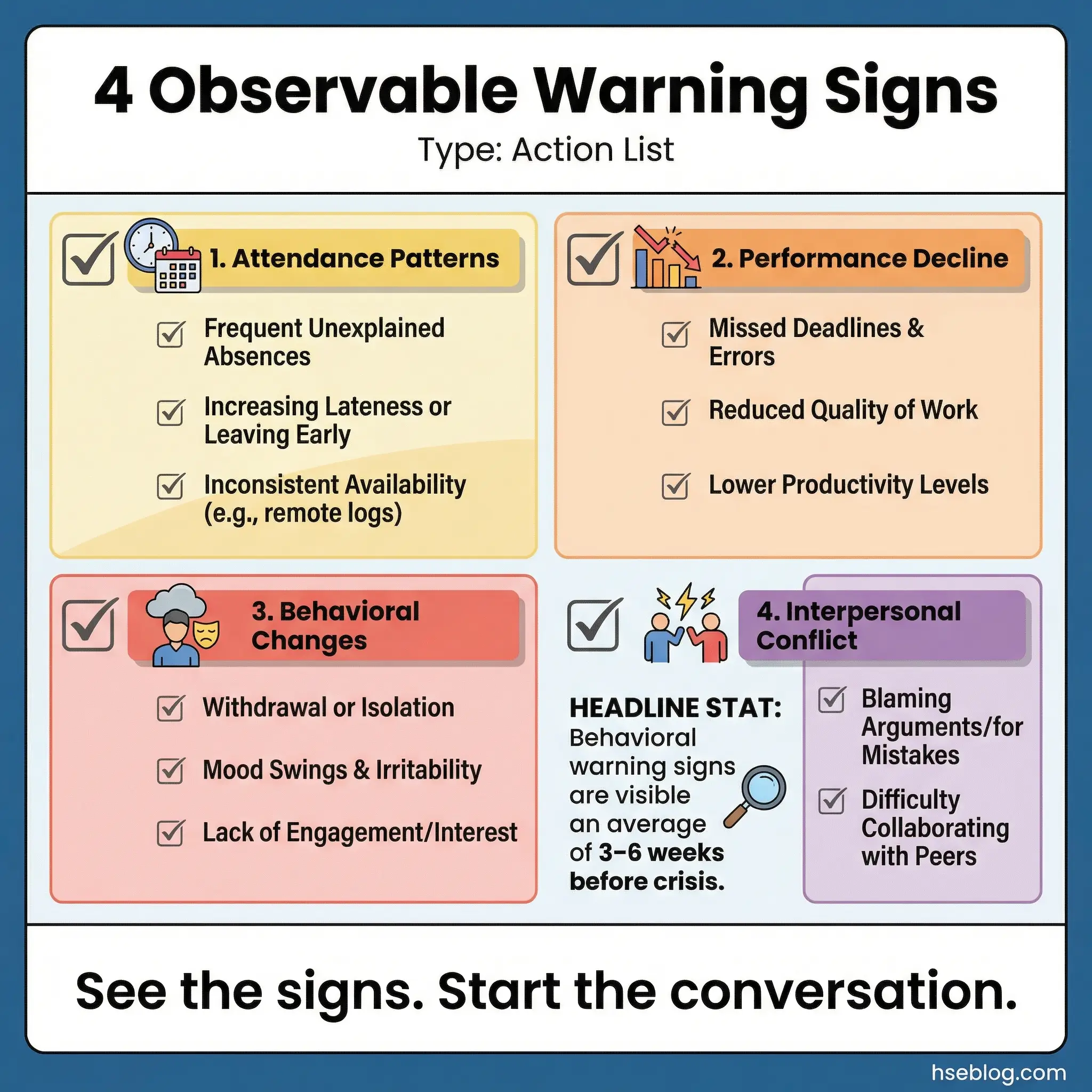
Training participants to recognize these signs in peers isn’t about policing — it’s about early intervention. During a behavioral safety program I delivered for a refinery in Southeast Asia, we trained crew supervisors to recognize the behavioral markers. Within six months, three early interventions were initiated — all before any safety incident occurred.
- Attendance patterns: Unexplained absences, Monday/Friday absenteeism patterns, frequent late arrivals, extended break periods, and leaving early without clear reason.
- Performance decline: Missed deadlines, increased errors, decreased output quality, difficulty concentrating, and uncharacteristic carelessness with safety procedures.
- Behavioral changes: Withdrawal from team activities, increased irritability, mood swings, defensiveness when questioned, secretive behavior, and changes in personal hygiene.
- Interpersonal conflict escalation: Increased arguments with coworkers, overreaction to minor issues, blaming others for personal errors, and deteriorating relationships with previously close colleagues.
Topic 14: Denial and Minimization Patterns
“I only drink on weekends.” “It’s just to take the edge off.” “I can stop anytime I want.” “Plenty of people use more than I do.” “It’s not affecting my work.” Every facilitator has heard these phrases hundreds of times, and every participant in the room has said at least one of them. Denial is not lying — it’s a psychological defense mechanism that protects the person from the full weight of what they’d have to confront if they admitted the truth.
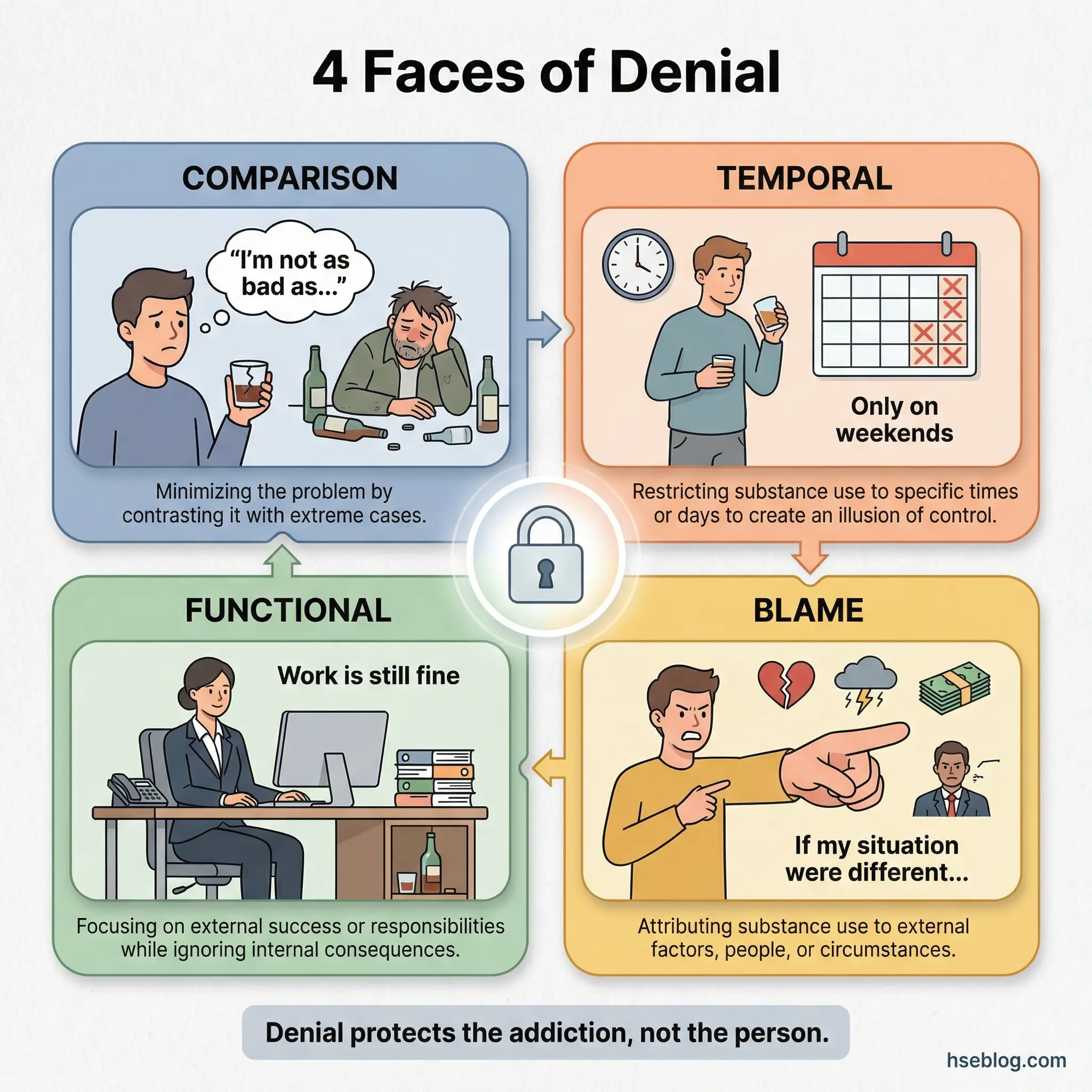
This topic works best when the group catalogs the phrases collectively, without attribution, and then examines the logic beneath each one.
- Comparison minimization: “I’m not as bad as…” — Measuring substance use against someone worse to avoid confronting one’s own reality. The question isn’t whether someone else is worse. The question is whether your use is harming you.
- Temporal minimization: “I only use on weekends / after work / during holidays” — as if scheduling substance use around obligations makes it controlled rather than dependent.
- Functional denial: “My work performance is fine, so it’s not a problem” — using functionality as proof of control while ignoring deteriorating relationships, health, and emotional wellbeing.
- Blame externalization: “If my job / spouse / situation were different, I wouldn’t need this” — shifting the cause of substance use onto external circumstances to avoid personal ownership.
Topic 15: Cross-Addiction and Substitution Behaviors
When someone stops one substance and unconsciously shifts to another — or to gambling, compulsive eating, excessive shopping, or workaholism — the underlying issue hasn’t been addressed. Only the delivery mechanism changed. This topic surprises many participants who assumed that stopping their primary substance was the entirety of recovery.
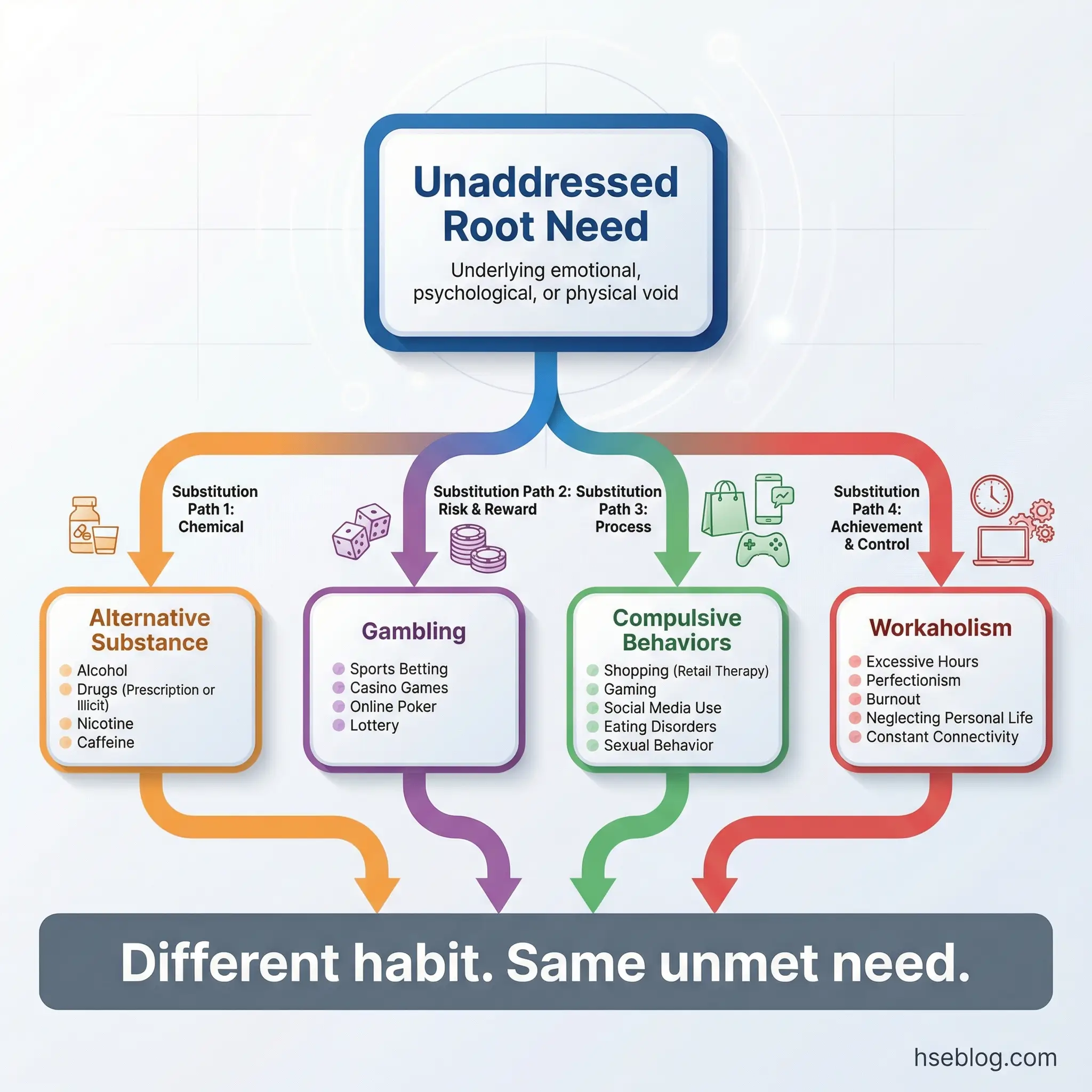
I encountered this pattern repeatedly in return-to-work programs. A worker successfully completed alcohol treatment, passed all follow-up screenings, and was celebrated as a recovery success. Eighteen months later, they were terminated for performance issues related to a gambling addiction that had consumed their finances and mental health. The addiction had migrated, not disappeared.
- Substance substitution: Stopping alcohol but increasing marijuana use. Ending opioid dependence but escalating benzodiazepine use. The brain seeks the reward pathway through whatever substance is available.
- Behavioral substitution: Gambling, compulsive eating, excessive exercise, workaholism, compulsive shopping, and pornography addiction. Each activates the same reward circuitry that substances targeted.
- Why substitution happens: The substance was solving a problem — numbing pain, managing anxiety, filling emptiness. Remove the substance without addressing the underlying need, and the brain finds another solution.
- Cross-addiction awareness in treatment: Every relapse prevention plan should include a cross-addiction check. “What has increased since I stopped my primary substance?” is a question participants should ask themselves monthly.
Topic 16: The Relapse Warning Timeline
Relapse rarely starts with the substance. It starts weeks or even months earlier — with emotional withdrawal, routine disruption, isolation, and rationalization. By the time someone picks up the substance again, they’ve already been in relapse mode for a considerable period. The substance use is the final symptom, not the starting event.
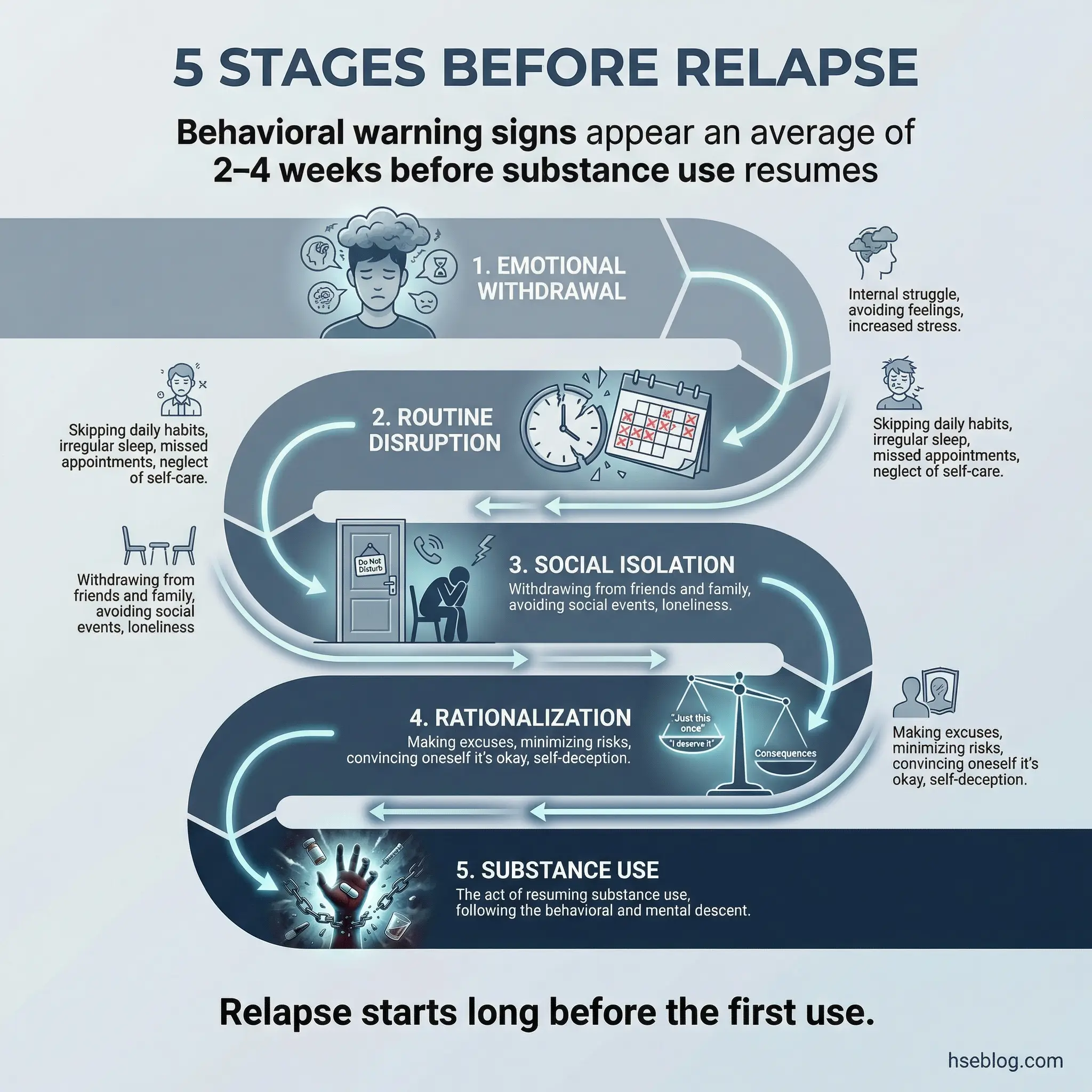
This topic works best as a backward mapping exercise. Start with the moment of substance use and walk backward through the behavioral, emotional, and social changes that preceded it. Most participants can trace the chain back 2–4 weeks.
- Stage 1 — Emotional withdrawal: Increased internal stress, unprocessed emotions, withdrawal from honest communication. The person stops sharing what’s really going on — in group, with their sponsor, with family.
- Stage 2 — Routine disruption: Skipped meetings, abandoned exercise routines, irregular sleep, missed meals. The structural scaffolding of recovery starts to erode.
- Stage 3 — Social isolation: Pulling away from recovery-supportive relationships. Spending more time alone. Reconnecting with pre-recovery social circles or environments.
- Stage 4 — Rationalization: “One drink won’t hurt.” “I’ve been clean for six months — I can handle it.” “Things are different now.” The internal narrative shifts from “I don’t use” to “I could use, and it would be fine.”
- Stage 5 — Substance use: The act itself. By this point, the internal and external safeguards have already been dismantled across weeks of behavioral drift.
Pro Tip: Have participants create their own personal warning timeline using past relapses as data. What happened at each stage? Who noticed? What could have been different? This exercise turns past failure into future prevention intelligence.
Topics on Coping Skills and Relapse Prevention (Topics 17–25)
This is where group discussions shift from understanding to doing. Coping skills discussed in a group setting carry more weight than those taught in one-on-one counseling, because participants see real people — their peers — practicing and struggling with the same tools. I learned this distinction on a rehabilitation-to-work program for a petrochemical contractor workforce in Southeast Asia. The facilitator ran a coping skills session where each participant had to teach one strategy to the group. The peer-teaching model tripled engagement compared to previous lecture-style sessions.
Topic 17: Healthy Stress Management Techniques
This is the foundational coping skills topic, and it needs to be practical — not philosophical. Every participant will nod along to “manage your stress better.” Nobody changes behavior because of that sentence. Behavior changes when someone practices a specific technique in the room and then uses it successfully once outside that room.
Dedicate at least 15 minutes of this session to live practice. Talk about a technique for 5 minutes. Practice it for 15. Debrief for 10.
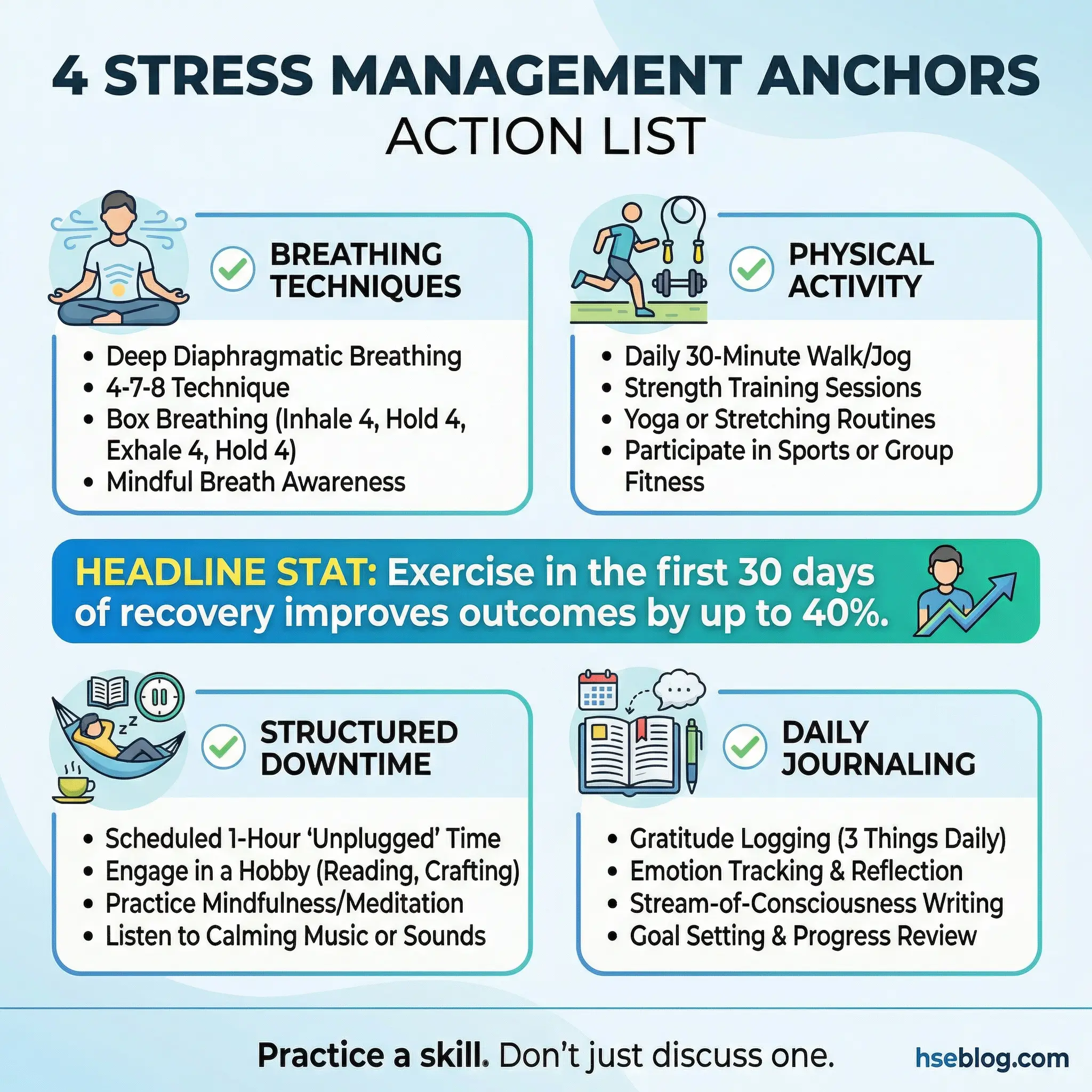
- Physiological regulation: Box breathing (4-4-4-4), diaphragmatic breathing, progressive muscle relaxation. These are not wellness trends — they are nervous system interventions that reduce cortisol within minutes.
- Physical activity as medicine: Walking, weightlifting, swimming, team sports. Exercise produces natural dopamine and endorphins. Participants who build an exercise routine in the first 30 days of recovery show measurably better outcomes.
- Structured downtime: Not scrolling a phone — actual restorative activities. Reading, cooking, building something, spending time outdoors. Unstructured time is a relapse risk. Structured leisure is a recovery asset.
- Journaling for pattern recognition: Five minutes of daily writing about emotional states, triggers encountered, and coping responses used. Over weeks, the journal reveals patterns that real-time awareness misses.
Topic 18: Urge Surfing and Craving Management
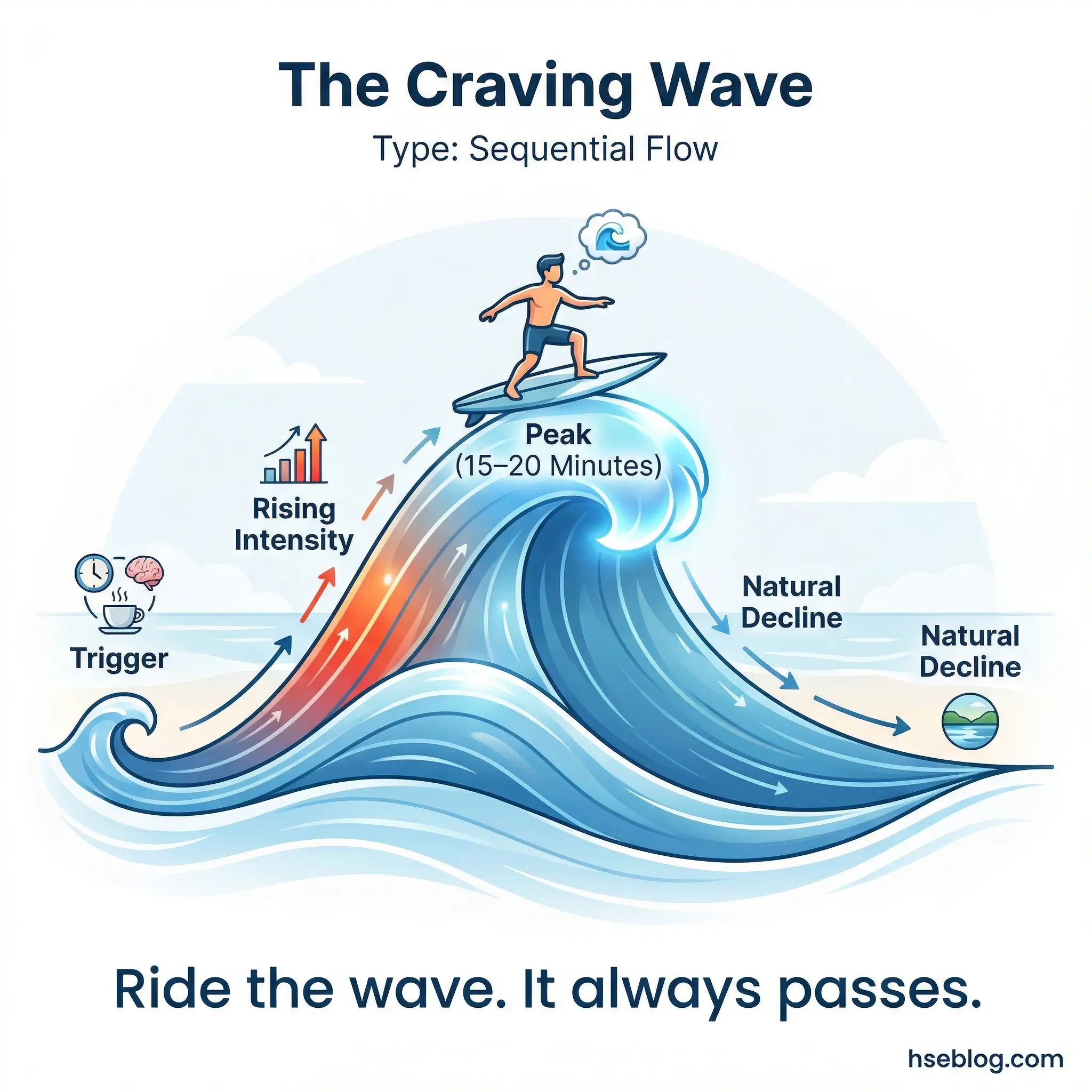
The concept is simple but counterintuitive: cravings are time-limited. They peak and pass within 15–20 minutes if the person does not act on them. Most participants have never experienced a craving passing naturally because they’ve always responded to it before it had the chance. Urge surfing teaches participants to observe the craving — notice it rising, acknowledge its intensity, and ride it out without taking action.
This is cognitive-behavioral therapy translated into plain language, and it works in group settings because participants practice it together.
- The 15–20 minute window: Every craving has a lifespan. It rises, peaks, and subsides. Most participants don’t know this because they’ve never waited long enough to observe the full arc.
- Observation without action: Notice the craving. Name it. Describe its physical sensations — tightness in the chest, restlessness in the hands, a specific taste memory. Naming the sensation externalizes it and reduces its power.
- Delayed response protocol: “I’ll wait 20 minutes before I decide.” Not “I’ll never use again” — just a 20-minute commitment. That manageable interval is more psychologically achievable than a lifetime promise.
- Group practice exercise: Facilitate a guided visualization where participants mentally enter a craving scenario and practice observing it without acting. Debrief the experience afterward.
Topic 19: Building a Daily Routine That Supports Recovery
Recovery doesn’t survive in chaos. Every relapse I’ve investigated in occupational rehabilitation programs traces back, at least partially, to the collapse of daily structure. When sleep, meals, social contact, and activity lose their predictable rhythm, the brain defaults to familiar patterns — and for someone in recovery, the most familiar pattern is substance use.
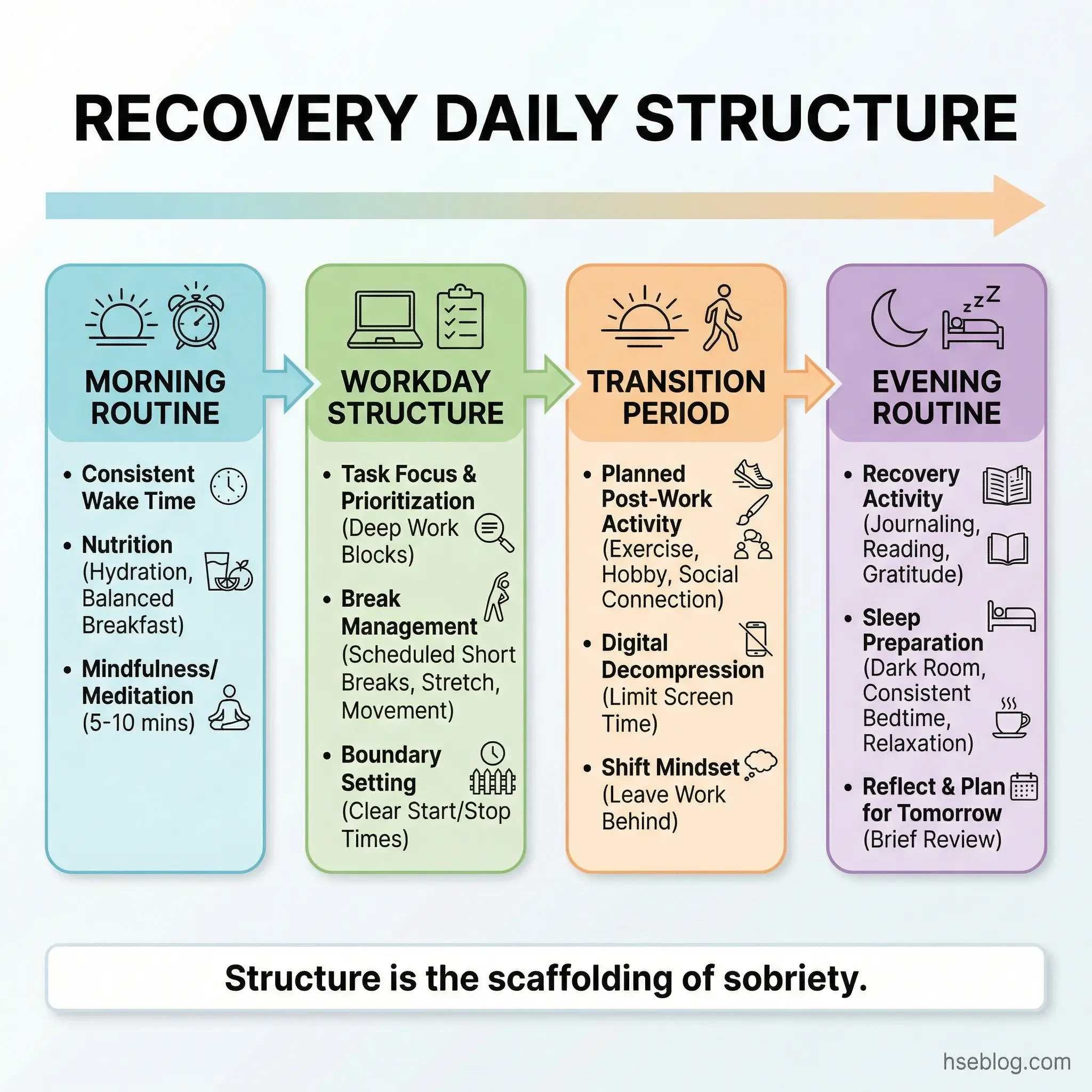
This topic asks participants to design a concrete daily schedule that builds recovery infrastructure into their ordinary day.
- Sleep hygiene as priority one: Consistent bedtime and wake time. No screens 60 minutes before sleep. No caffeine after 2 PM. Sleep disruption is the single most underrated relapse risk factor.
- Meal timing and nutrition: Regular meals stabilize blood sugar, which stabilizes mood. Skipped meals produce irritability and impulsive decision-making — both relapse risk factors.
- Scheduled recovery activities: Meetings, check-ins with accountability partners, exercise — these need fixed time slots, not “when I get around to it.” If it’s not on the schedule, it won’t happen.
- Structured transitions: The highest-risk moments are transitions — end of workday, arrival home, weekends. Build a specific activity into each transition point that replaces the former substance use pattern.
Topic 20: Saying No — Refusal Skills Practice
Knowing you should say no is worthless without practicing how. Most participants can articulate their commitment to sobriety in the safety of a group room. When a colleague slides a beer across the table at a post-project dinner, the articulation vanishes. What remains is whatever refusal script the person has actually rehearsed out loud.
This topic must include live role-play. No exceptions. Talking about refusal skills is not practicing refusal skills.
- Script development: Each participant writes three refusal responses: a direct one (“No thanks, I don’t drink”), a deflecting one (“I’m driving”), and a firm boundary one (“I’ve asked you not to offer me that. Please stop.”). The third script is the one most people never practice — and the one they most frequently need.
- Role-play scenarios: A colleague offering a drink after work. A friend pressuring at a social event. A family gathering where alcohol is central. A dealer contacting via phone. Practice each scenario with a partner.
- Body language and tone: Refusal isn’t just words. Maintain eye contact. Don’t laugh nervously or apologize. Deliver the refusal with the same calm confidence you’d use to decline a business proposal.
- Post-refusal planning: What happens after you say no? The conversation doesn’t end. Have a follow-up ready — change the subject, leave the situation, or contact an accountability partner for support.
Topic 21: Mindfulness and Grounding Techniques
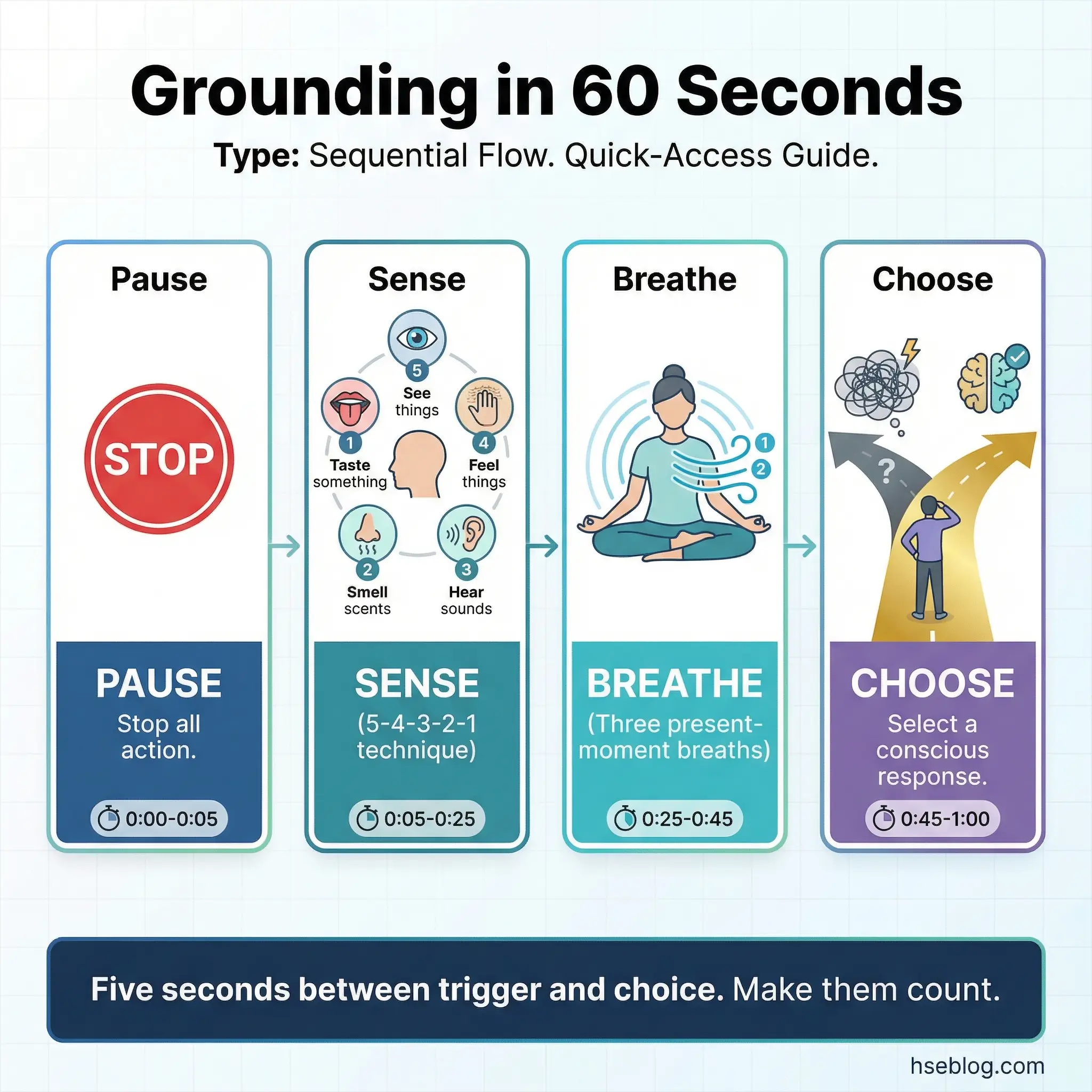
These are survival tools for the space between trigger and action. When a craving hits, when anxiety spikes, when anger floods the body — the person has approximately 5–10 seconds before autopilot takes over. Mindfulness and grounding techniques extend that window long enough for the rational brain to engage.
I teach these not as meditation practices but as emergency interventions. The participants who use them most successfully are the ones who practiced them repeatedly in non-crisis moments so they were available automatically during crises.
- 5-4-3-2-1 sensory grounding: Name 5 things you see, 4 you hear, 3 you can touch, 2 you smell, 1 you taste. This technique forces the brain out of the craving loop and into present-moment sensory reality.
- Body scan awareness: Slow attention from head to feet, noticing tension, temperature, and sensation in each body region. This interrupts the stress response by shifting focus from emotional intensity to physical observation.
- Present-moment breathing: Not “deep breathing” — present-moment awareness of the breath as it is. Notice the air entering the nostrils, the chest expanding, the exhale. No modification, just observation.
- Practice frequency: These techniques fail in crisis if they haven’t been practiced in calm. Participants should practice at least once daily — ideally twice — for 2–3 minutes each time, building automatic access.
Topic 22: Creating a Personal Relapse Prevention Plan
This is the single most important written document any participant will produce during the entire program. A relapse prevention plan is not an aspirational statement — it’s an emergency protocol. Like a workplace emergency response plan, it exists because the person who needs it will be in a state of impaired judgment when the moment arrives.
Every participant should leave this session with a draft plan. The group reviews each other’s plans and offers feedback — because an untested plan is no plan at all.
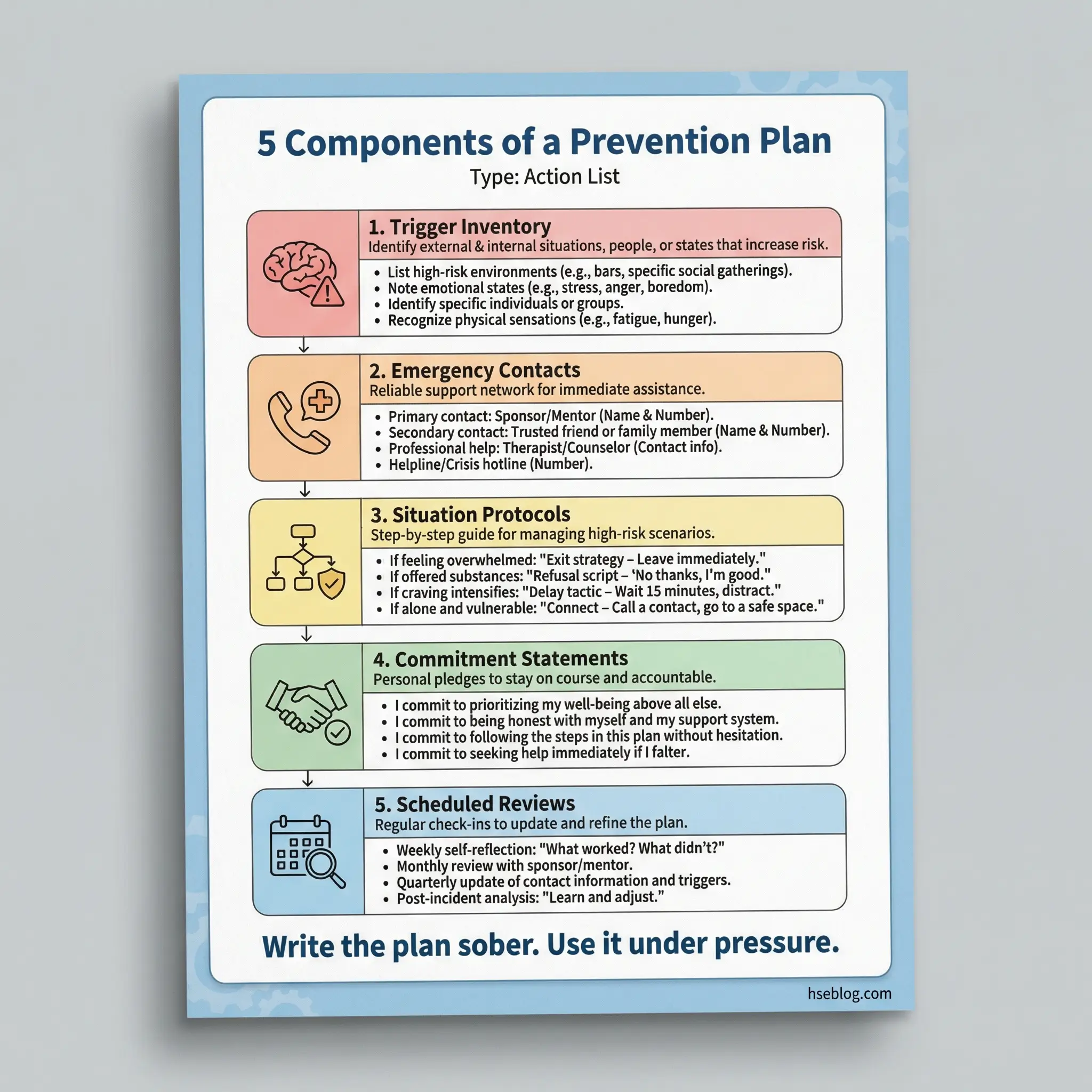
- Trigger inventory: The top five personal triggers from the trigger mapping exercise (Topic 9), with specific coping responses assigned to each one.
- Emergency contact list: Three people the participant can call at any hour — not just names, but actual phone numbers written down. Include at least one who is not a family member to avoid reliance on a single support system.
- High-risk situation protocols: For each identified high-risk situation, a specific pre-planned response. “If I’m invited to a work function with alcohol, I will [specific action].”
- Commitment statements: Written commitments that the participant signs and shares with the group. “If I experience a craving lasting more than 20 minutes, I will call [name] before taking any other action.”
- Plan review schedule: The plan isn’t static. Schedule reviews at 30, 60, and 90 days post-program, with the accountability partner involved in each review.
A relapse prevention plan is an emergency response plan for recovery. Write it when you’re clear-headed because you’ll need it when you’re not.
Topic 23: What to Do in the First 24 Hours After a Lapse
This topic removes the shame spiral that turns a single lapse into a full-blown relapse. The distinction between a lapse (a single use) and a relapse (a return to sustained use patterns) is clinically critical and psychologically lifesaving. Most participants who experience a lapse believe they’ve failed entirely — and that belief drives them back into the full addiction cycle.
I’ve seen this topic literally save lives. One supervisor in a refinery program told me that remembering the “first 24 hours” protocol from group was the only reason his single beer at an airport lounge didn’t become a three-week bender.
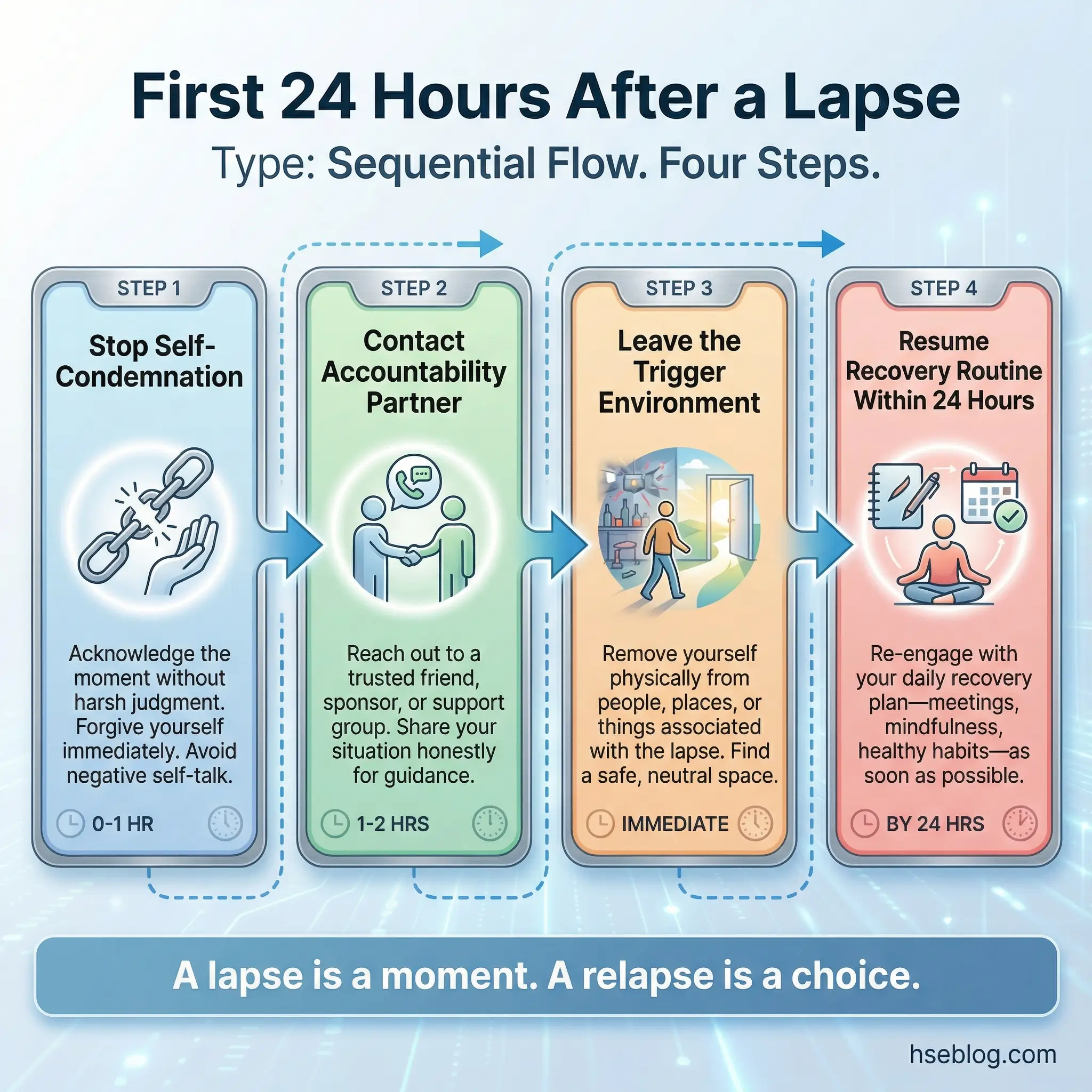
- Eliminate self-condemnation: A lapse is data, not a death sentence. The first internal response should be observation (“What triggered this? What coping mechanism failed?”) — not judgment (“I’m worthless and recovery is impossible”).
- Immediate contact: Call the accountability partner or sponsor within 60 minutes of the lapse. Silence is the enemy. The longer the lapse stays a secret, the more likely it becomes a relapse.
- Environmental removal: Leave the situation where the lapse occurred. Change location, change activity, change company. Break physical proximity to the trigger environment.
- Same-day plan restart: Don’t wait until Monday or next week. Resume the recovery routine — meeting attendance, exercise, structured schedule — within 24 hours. Momentum is recovery’s oxygen.
Topic 24: Building a Sober Support Network
Recovery happens in relationships. The quality and structure of a participant’s social network after treatment is one of the strongest predictors of sustained sobriety. This topic forces an honest evaluation of current relationships — which ones support recovery and which ones actively undermine it.
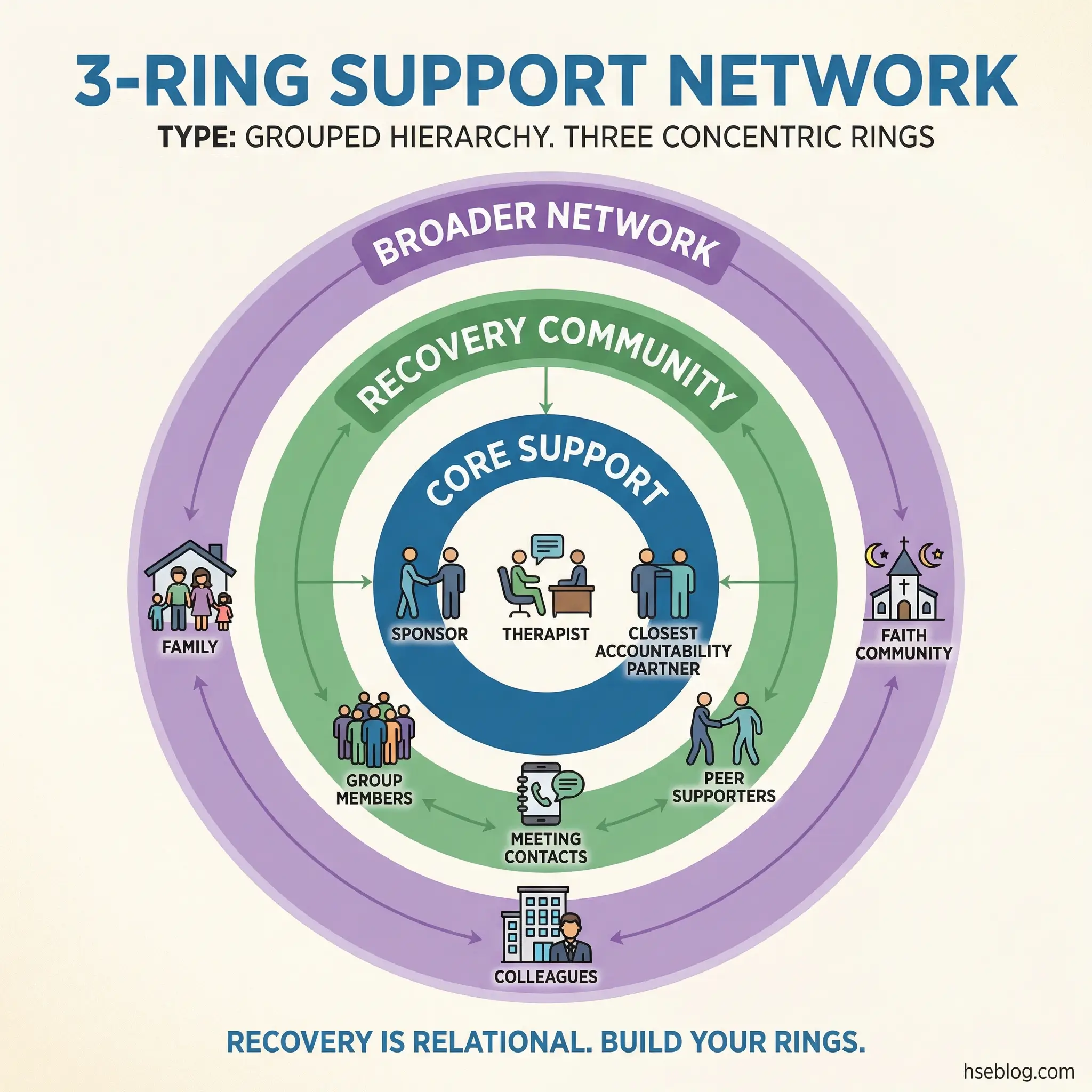
The exercise is uncomfortable. Some participants will realize that their entire social circle is organized around substance use, and that sobriety requires building an entirely new network from scratch. That reality is better confronted in a group setting than discovered alone.
- Network audit: List every person the participant spends regular time with. Categorize each as “recovery-supportive,” “neutral,” or “recovery-threatening.” Be honest — a drinking buddy who says “I support your sobriety” but always invites you to the bar is not supportive.
- Recovery community integration: 12-step meetings, SMART Recovery, Refuge Recovery, workplace peer support groups, faith-based recovery communities. Each offers a different model — participants should try multiple formats to find fit.
- Rebuilding family connections: Family members who survived the addiction period may be willing to reconnect but unsure how. Discuss how to initiate those conversations without expecting immediate forgiveness or trust.
- Professional support structures: Therapists, substance abuse counselors, occupational health professionals, and employee assistance program contacts. These are not substitutes for personal relationships — they are specialized support that personal relationships cannot provide.
Topic 25: Long-Term Recovery Milestones and Realistic Expectations
Recovery is not linear, and the timeline doesn’t match the motivational posters. The first 90 days are often called the “honeymoon phase” — high motivation, visible progress, strong support. The 6-month wall hits when motivation fades but the hard work of sustained change remains. The one-year mark brings reassessment — “Is this really my life now?” These phases are predictable, and preparing participants for them prevents the devastating surprise that derails many otherwise solid recoveries.
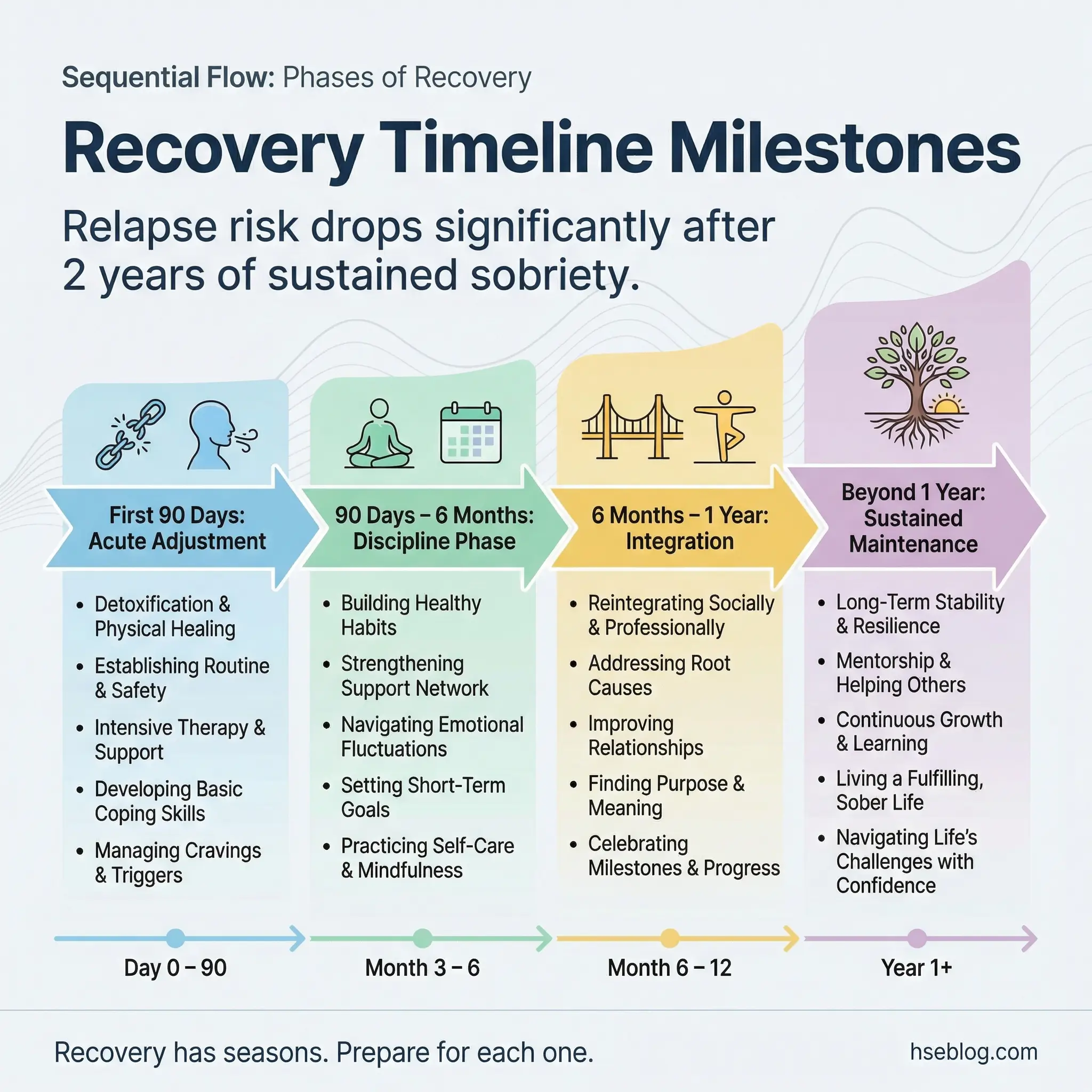
Understanding the long-term effects of substance abuse helps participants stay committed when the motivation dips, because they can see what continued use would cost them across years, not just days.
- First 90 days — the acute adjustment phase: Physical recovery, sleep normalization, emotional volatility, intense cravings. This period requires the highest level of external support and the most rigid daily structure.
- 90 days to 6 months — the discipline phase: Initial motivation fades. Routines feel boring. The novelty of sobriety wears off. This is where daily discipline — the unglamorous, repetitive work of recovery — matters more than inspiration.
- 6 months to 1 year — the integration phase: Identity begins to shift from “person trying not to use” to “person building a new life.” Relationships, career, health, and purpose start to restructure around sobriety.
- Beyond 1 year — sustained maintenance: Recovery becomes lifestyle rather than project. The vigilance never completely disappears, but it becomes integrated rather than effortful. Complacency is the primary risk at this stage.
Topics on Mental Health and Co-Occurring Disorders (Topics 26–32)
Substance abuse rarely exists in isolation. In my experience across occupational health programs on multiple continents, at least 40–50% of participants in any substance abuse group carry an undiagnosed or undertreated mental health condition alongside their substance use. Ignoring this overlap doesn’t simplify treatment — it guarantees failure. These seven topics address the intersection directly, giving facilitators the framework to open conversations about mental health without overstepping into clinical territory.
The World Health Organization estimates that approximately 50% of individuals with a substance use disorder also meet criteria for at least one other mental health condition, reinforcing the clinical necessity of integrated dual-diagnosis discussion within group treatment settings.
Topic 26: The Link Between Anxiety and Substance Use
Self-medication is the entry point for a significant portion of substance users, and anxiety is the most common driver. The person doesn’t start with a desire to get intoxicated — they start with a desperate need to quiet the noise in their head. Alcohol dampens generalized anxiety. Benzodiazepines eliminate panic attacks. Cannabis reduces social anxiety. Each substance provides temporary relief that creates a dependency loop.
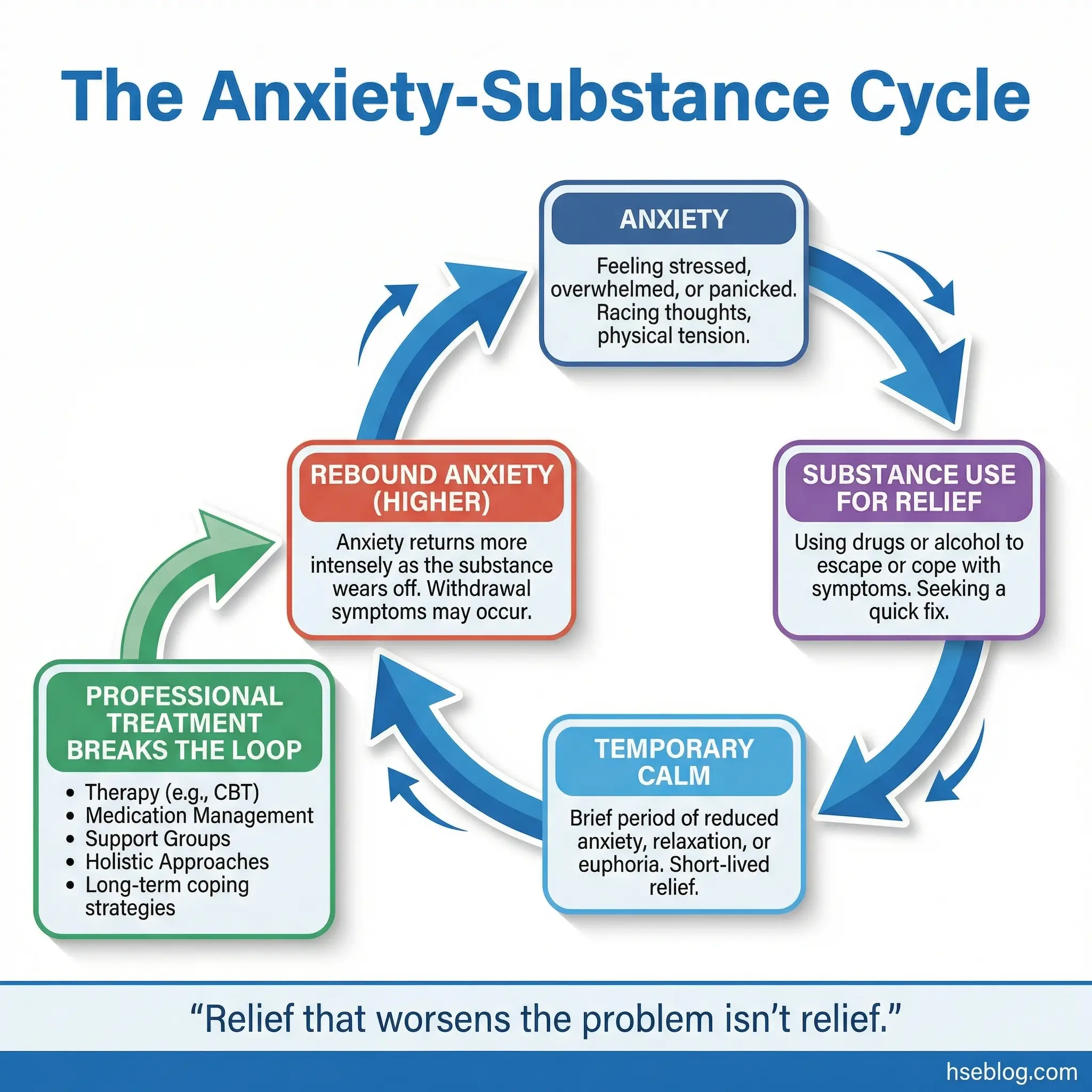
The critical insight for participants is that substance use worsens anxiety over time. The relief is a loan, not a gift — and the interest rate compounds ruthlessly.
- The anxiety-substance feedback loop: Anxiety → substance use for relief → temporary calm → rebound anxiety (higher baseline than before use) → increased substance use for relief. Each cycle raises the baseline anxiety level.
- Types of anxiety affected: Generalized anxiety disorder, social anxiety, panic disorder, performance anxiety, and health anxiety. Each drives substance use through a different mechanism.
- The withdrawal anxiety trap: When substance use stops, anxiety temporarily spikes — often to levels higher than the pre-use baseline. This rebound anxiety is the primary reason people relapse within the first two weeks.
- Anxiety management without substances: Cognitive-behavioral strategies, exposure therapy concepts, and the importance of professional anxiety treatment as a component of addiction recovery — not an alternative to it.
Topic 27: Depression and Addiction — Which Came First?
The chicken-and-egg question of whether depression causes addiction or addiction causes depression generates genuine interest in every group I’ve facilitated. The clinical answer is that it doesn’t matter which came first — both conditions need treatment simultaneously because each perpetuates the other. But the discussion itself is valuable because it helps participants stop using one condition to explain away the other.

I’ve heard “I drink because I’m depressed” used as a justification, and “I’m depressed because I can’t stop drinking” used as a reason to avoid mental health treatment. Both positions are incomplete and both are dangerous.
- Depression as a driver of substance use: Numbing emotional pain, seeking pleasure when the brain can no longer produce it naturally, using stimulants to counteract the lethargy and hopelessness of depression.
- Substance-induced depression: Chronic alcohol use depletes serotonin. Stimulant crash cycles produce depressive episodes. Opioid withdrawal mirrors major depressive disorder symptomatology.
- The integrated treatment imperative: Treating addiction without addressing depression leaves the underlying driver intact. Treating depression without addressing addiction leaves the coping mechanism intact. Both fail alone.
- Group discussion frame: Ask participants: “If your depression disappeared tomorrow, would you still use substances? If your substance use disappeared tomorrow, would you still feel depressed?” The answers reveal the relationship.
Topic 28: PTSD, Trauma, and Substance Use
This is the highest-vulnerability clinical topic in the entire 50-topic roster. Trauma-informed facilitation is non-negotiable here. Many participants carry unprocessed traumatic experiences — childhood abuse, domestic violence, combat exposure, witnessing workplace fatalities, sexual assault — and substance use has been their primary method of managing the associated hyperarousal, intrusive memories, and emotional flooding.
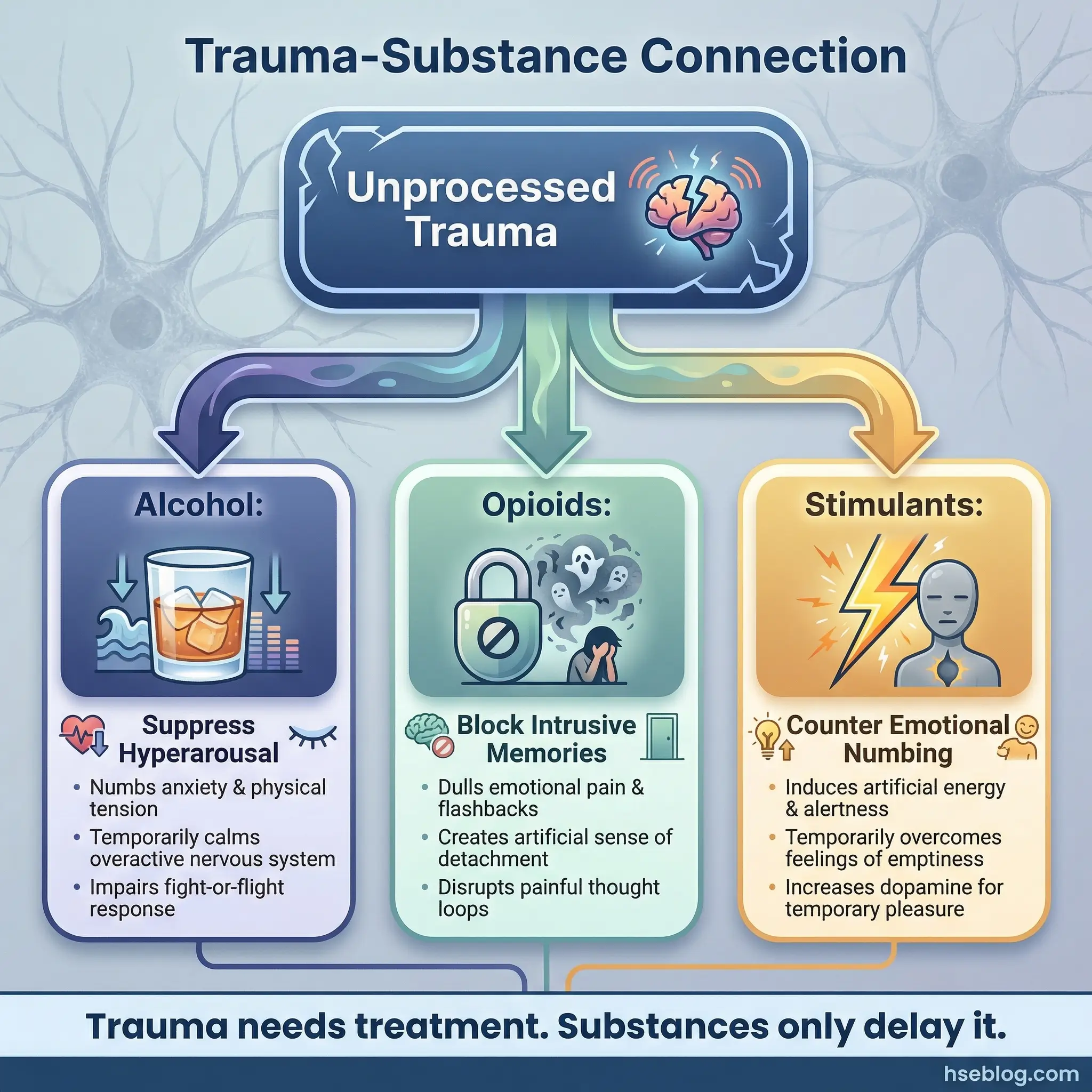
In high-risk occupational settings, this topic carries additional weight. Emergency responders, military veterans, workers who’ve witnessed fatal incidents — these populations carry occupational trauma that directly feeds substance use.
- The self-medication model of PTSD: Substances suppress hyperarousal (alcohol), block intrusive memories (opioids), and reduce emotional numbing (stimulants). The substance becomes a survival tool — removing it without addressing the trauma is clinically dangerous.
- Trauma disclosure ground rules: This session is NOT for detailed trauma narration. Establish clear boundaries: participants can name that they have trauma, identify its connection to their substance use, and discuss what support they need — without retelling the traumatic event itself.
- Occupational trauma recognition: Witnessing a colleague’s death, being involved in a serious accident, prolonged exposure to human suffering — these are occupational traumas that often go unrecognized because “it’s part of the job.”
- Referral pathways: PTSD treatment requires specialized clinical intervention — EMDR, prolonged exposure therapy, or trauma-focused CBT. The group setting can open the door to this recognition, but it cannot provide the treatment itself.
Topic 29: Sleep Disorders and Recovery
Sleep disruption is the relapse risk factor that everyone acknowledges and nobody prioritizes. Insomnia, disrupted circadian rhythms from shift work, substance-withdrawal sleep disturbances, and the temptation to use substances as sleep aids — these form a quiet, persistent threat to every person in recovery.
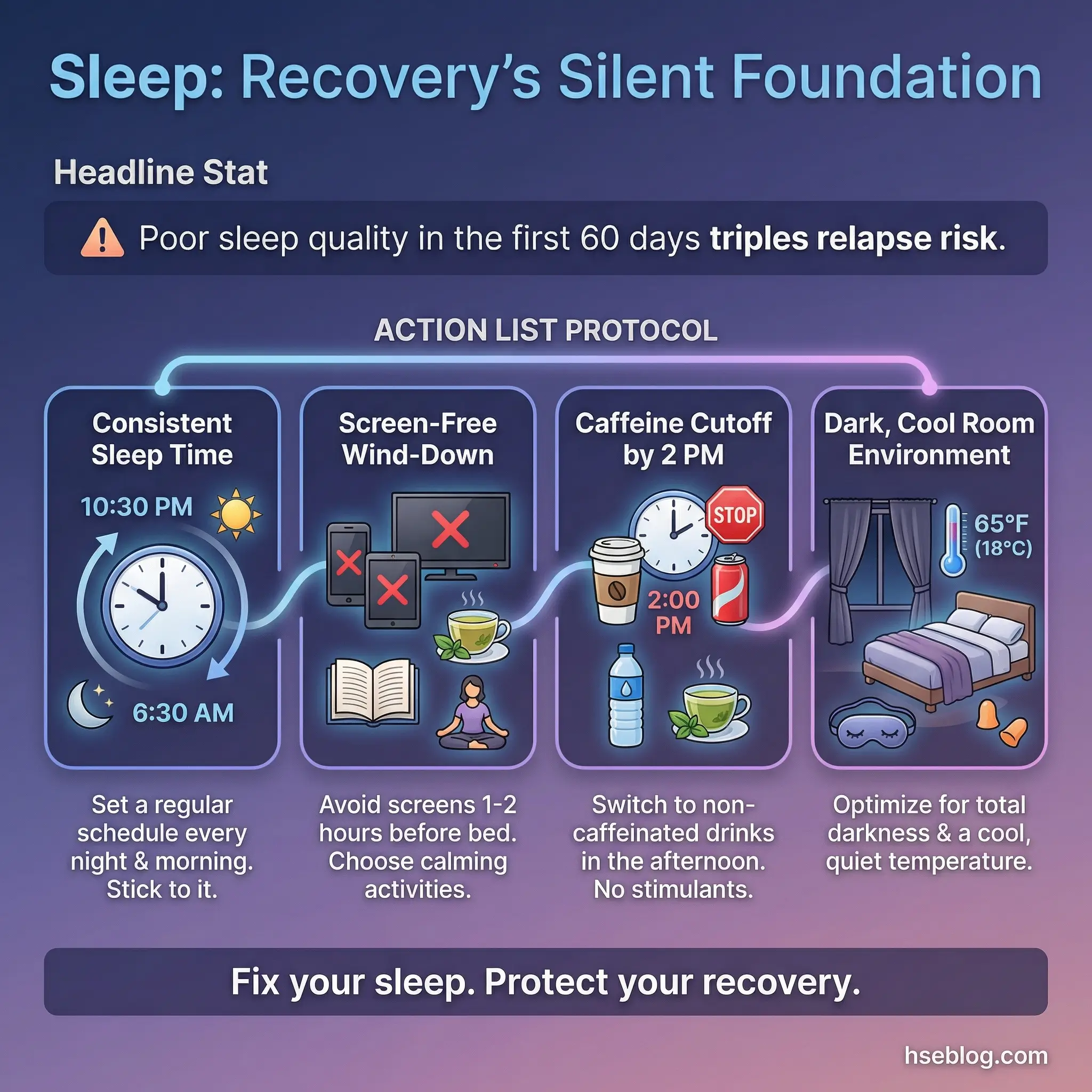
During a fitness-for-duty program I managed at a refinery, sleep quality assessments were added to the return-to-work protocol. The data was striking — participants who reported consistently poor sleep quality in the first 60 days of recovery were three times more likely to relapse than those who achieved stable sleep patterns.
- Substance withdrawal and sleep: Alcohol withdrawal causes rebound insomnia that can last weeks. Stimulant withdrawal produces hypersomnia followed by irregular sleep. Opioid withdrawal disrupts sleep architecture profoundly. Participants need to know that sleep disruption is a temporary withdrawal symptom — not permanent.
- Shift work complication: Workers in recovery who also work rotating shifts face a compounded challenge. Their circadian rhythm is already disrupted by their work schedule, making recovery-standard sleep hygiene harder to implement.
- Sleep hygiene fundamentals: Consistent bedtime, dark room, no screens before sleep, no caffeine after early afternoon, temperature regulation, and a wind-down routine. These are not suggestions — they are recovery infrastructure.
- The sleep-substance substitution risk: Participants must be warned against substituting prescription sleep aids, over-the-counter antihistamines, or cannabis as sleep solutions. Each carries its own dependency risk.
Topic 30: Managing Anger Without Substances
Anger is the trigger most participants underestimate and facilitators most frequently avoid. It’s uncomfortable to sit with someone else’s anger in a group setting — but that discomfort is exactly why the topic matters. Most participants have used substances to manage anger for so long that they have no alternative response pattern. Remove the substance, and the anger has nowhere to go except outward (aggression) or inward (depression).
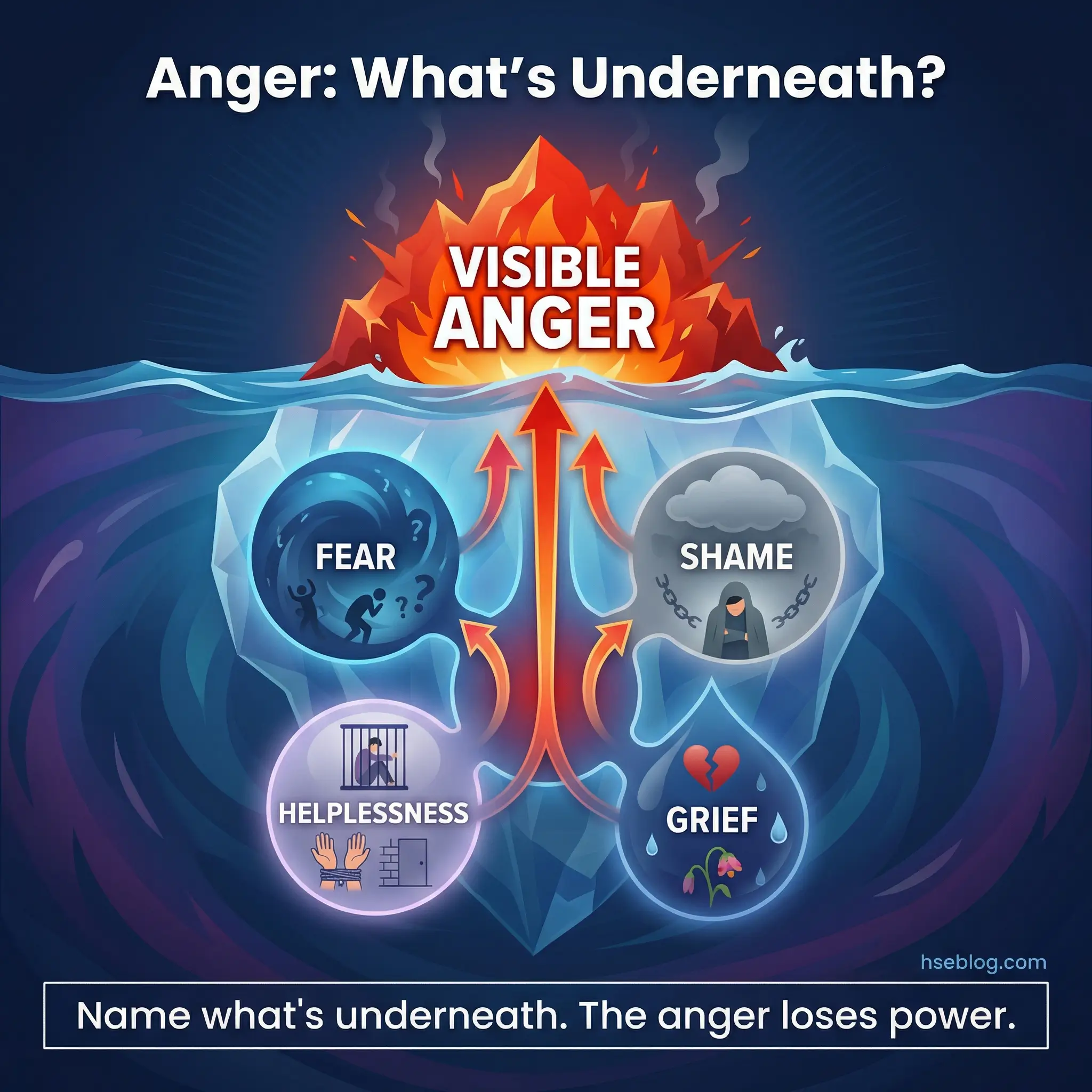
The reframe that changes this conversation: anger is almost always a secondary emotion. Underneath it sits fear, shame, helplessness, or grief. Participants who learn to identify the primary emotion beneath their anger gain access to entirely different coping strategies.
- Anger as secondary emotion: “I’m angry at my boss” is usually “I’m afraid of losing my job.” “I’m angry at my partner” is often “I’m ashamed of what I’ve put them through.” Identifying the emotion under the anger redirects the coping response.
- Physiological anger management: Recognizing the body’s anger signals — elevated heart rate, muscle tension, jaw clenching, heat in the face. Teaching participants to use these signals as cues to implement a pause before responding.
- The time-out protocol: When anger escalates beyond the person’s current coping capacity, leave the situation. Not permanently — for 20–30 minutes. Return when the physiological arousal has subsided enough for rational engagement.
- Anger expression vs. anger suppression: Neither extreme works. Suppressed anger builds pressure. Explosive anger destroys relationships. The goal is regulated expression — naming the anger, identifying its source, and communicating the underlying need.
Topic 31: Self-Worth, Shame, and Identity in Recovery
“I am an addict” versus “I am a person recovering from addiction.” That single linguistic shift carries an enormous psychological weight. The first statement fuses identity with the disorder. The second acknowledges the disorder while preserving personhood. This is not semantic hair-splitting — it’s a foundational principle of identity reconstruction in recovery.

Shame is the most corrosive internal experience a person in recovery carries. It whispers that they are fundamentally broken, undeserving of recovery, permanently damaged. Guilt says “I did something bad.” Shame says “I am something bad.” The difference determines whether a person fights for recovery or surrenders to relapse.
- Shame vs. guilt distinction: Guilt is behavioral (“I made a harmful choice”). Shame is identity-based (“I am a harmful person”). Recovery requires converting shame into guilt — acknowledging harmful actions without internalizing them as permanent identity.
- Language and identity construction: How participants describe themselves shapes how they think about themselves. Encourage language that separates the person from the disorder: “I have a substance use disorder” rather than “I’m an addict.”
- Achievement recognition: Participants in early recovery often cannot name a single thing they’re proud of. This exercise asks each person to identify three accomplishments — any size — since they entered recovery. The group validates each one.
- Shame resilience building: Discuss Brené Brown’s shame resilience framework in practical terms — recognizing shame triggers, practicing critical awareness of shame messages, reaching out to trusted contacts, and speaking shame aloud (which reduces its power).
Topic 32: When to Seek Professional Mental Health Support
Group discussions are not therapy. Peer support is not clinical treatment. This topic draws clear lines around what group sessions can and cannot provide, and teaches participants to recognize when they need professional intervention beyond the group.
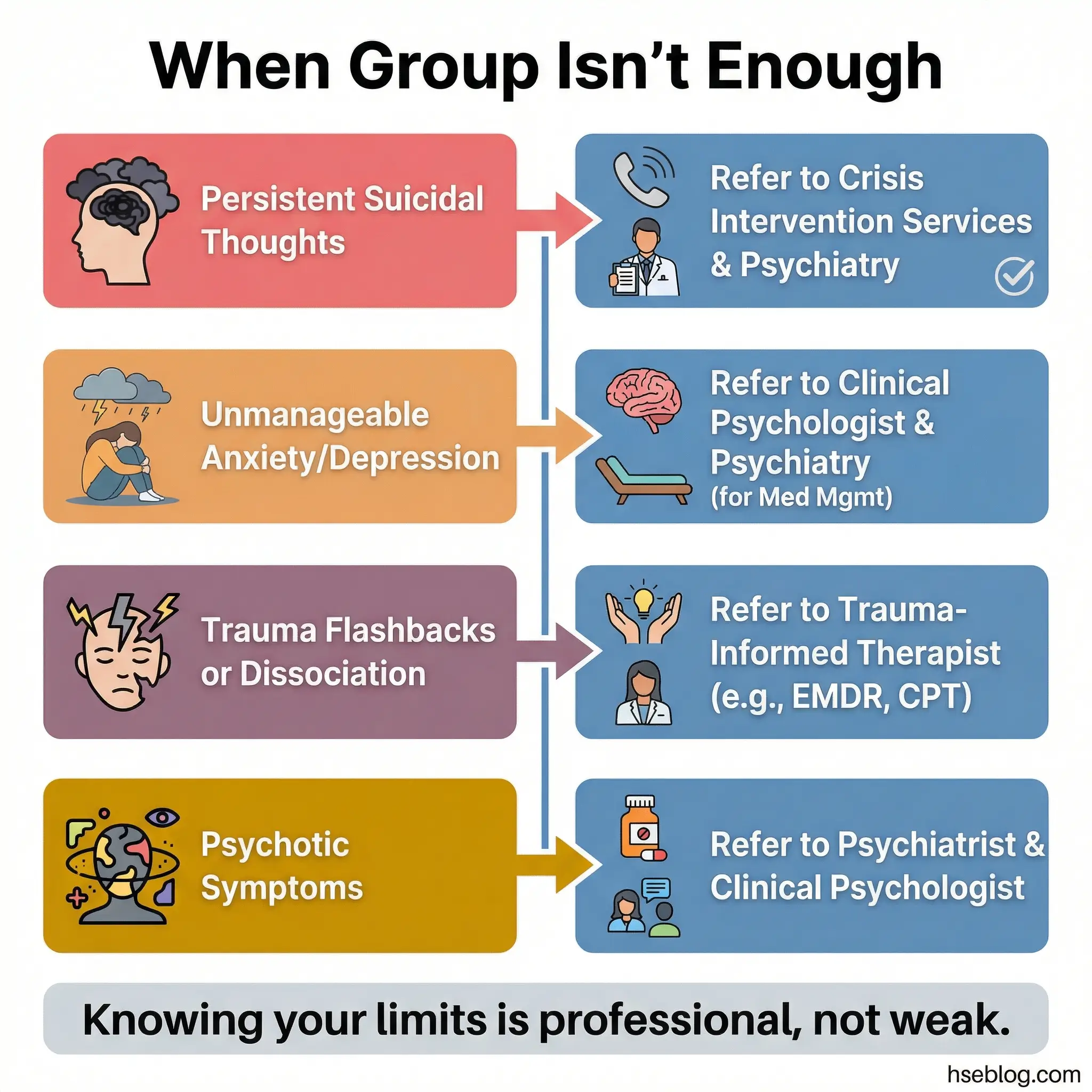
I’ve seen facilitators hesitate to address this topic because they fear it undermines the group’s value. The opposite is true. A group that knows its limitations and actively refers participants to appropriate professional resources is more credible and more effective than one that tries to handle everything internally.
- Clinical red flags that require professional referral: Persistent suicidal ideation, hallucinations or psychotic symptoms, severe depressive episodes lasting more than two weeks, unmanageable anxiety that prevents daily functioning, and trauma responses (flashbacks, dissociation) that the participant cannot stabilize with grounding techniques.
- Types of professionals and their roles: A substance abuse counselor handles addiction-specific treatment. A psychologist provides cognitive-behavioral therapy and assessment. A psychiatrist prescribes and manages medication. Participants need to understand the difference so they seek the right professional for their specific need.
- Normalizing professional help: In many workplace and cultural contexts, seeking mental health support still carries stigma. Frame professional help as a sign of strength and self-awareness — the same way seeking medical treatment for a broken bone is rational, not shameful.
- Access pathways: Employee assistance programs, community mental health centers, telehealth options, sliding-scale clinics, and insurance navigation. Remove logistical barriers by providing concrete pathways, not generic advice.
Pro Tip: Keep a printed resource card with local and international mental health helplines available at every session. Don’t wait for a crisis to distribute contact information. Normalize access from day one.
Topics on Relationships, Family, and Social Impact (Topics 33–40)
Recovery doesn’t happen in a vacuum, and neither does addiction. The people around the participant — family, partners, children, coworkers, friends — are both affected by and influential in the trajectory of substance use. These eight topics are among the highest-vulnerability discussions in any group program.
I’ve watched grown men break down during a family impact session at a construction workforce wellness program in Northern Europe. The facilitator handled it with calm, steady professionalism — no rushing, no minimizing, no platitudes. That’s the standard.
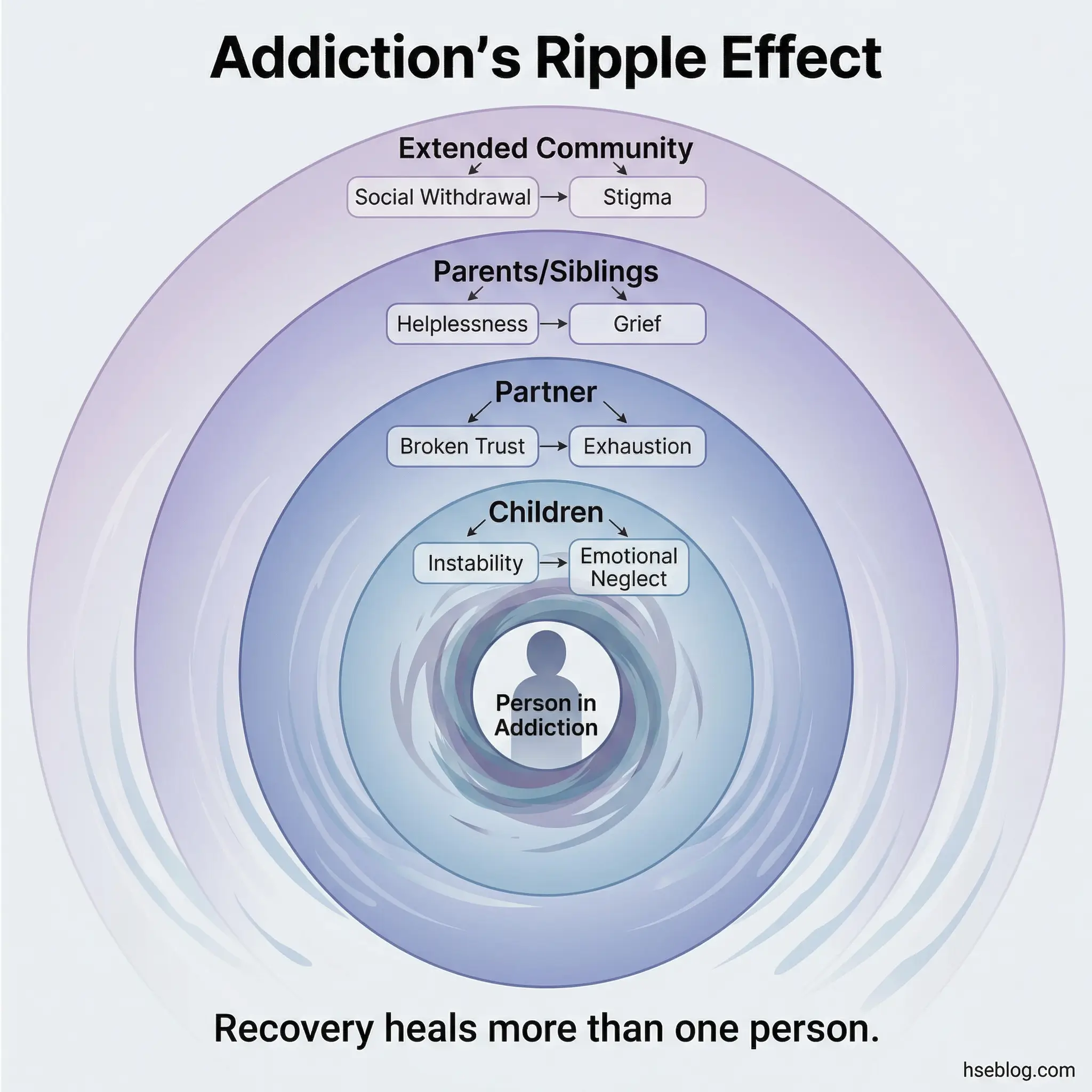
Topic 33: How Addiction Affects Families
This topic opens the door to the ripple effect of addiction — the damage that radiates outward into every relationship the participant holds. Children, spouses, parents, siblings — each relationship carries a different burden and experiences a different kind of harm. The goal is not to weaponize guilt but to build awareness that recovery isn’t just a personal project. It’s a relational one.
Let participants name the specific impacts they’ve observed or caused — without forced confessions. Some will speak. Some won’t. Both responses are acceptable.
- Impact on children: Inconsistent parenting, emotional neglect, broken promises, exposure to substance-related behavior, and the long-term psychological effects on children who grow up in homes where a parent uses substances.
- Impact on partners/spouses: Erosion of trust, emotional exhaustion, financial strain, codependent behavior patterns, and the isolation that partners experience when they can’t discuss the situation without stigma.
- Impact on parents and siblings: Helplessness, enabling behaviors, grief for the person they remember before addiction, and the family system disruptions that occur when one member’s substance use dominates household dynamics.
- Intergenerational transmission: The documented pattern where children of parents with substance use disorders are significantly more likely to develop their own substance issues — not through inheritance alone, but through learned behavior, normalized exposure, and unaddressed childhood trauma.
Topic 34: Codependency and Enabling Behaviors
Codependency is one of the most misunderstood dynamics in addiction. A codependent partner or family member isn’t “loving too much” — they’re caught in a pattern where their own emotional stability depends on managing the addicted person’s behavior. Enabling isn’t helping — it’s removing consequences that the person needs to experience in order to recognize the severity of their situation.
Understanding substance abuse effects on family dynamics is essential here, because codependency and enabling are family-system responses to addiction, not individual character flaws.
- Defining codependency in practical terms: When a person’s sense of worth, purpose, and daily functioning depends on managing someone else’s addiction — making excuses, covering up, controlling situations to prevent consequences — that’s codependency.
- Common enabling behaviors: Calling the boss to report a “sick day” after a binge. Paying off debts caused by substance use. Making excuses to family and friends. Hiding evidence of use. Each action delays the addicted person’s confrontation with reality.
- Why enablers enable: Fear of conflict, fear of abandonment, fear of the addicted person’s escalation, and the genuine — if misguided — desire to protect. Enabling comes from love. It also sustains addiction.
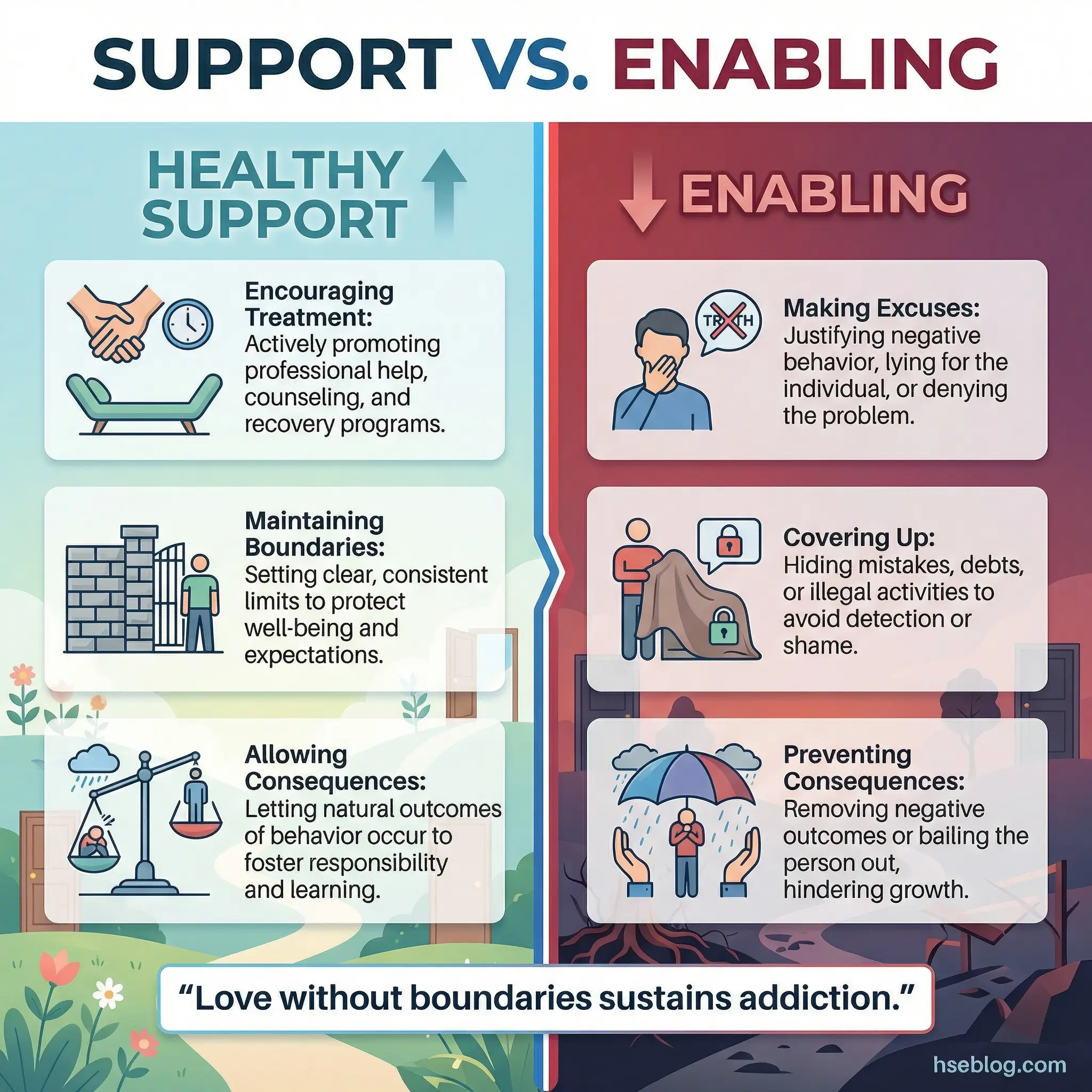
- Healthy support vs. enabling: Supporting someone means encouraging treatment, maintaining boundaries, and allowing natural consequences. Enabling means preventing consequences and doing for the person what they need to do for themselves.
Topic 35: Rebuilding Trust After Addiction
Trust repairs slowly. There is no shortcut, no grand gesture, and no single conversation that restores what addiction dismantled. This topic needs to be delivered with absolute realism — participants who expect quick forgiveness will be devastated when it doesn’t come, and that devastation becomes a relapse trigger.
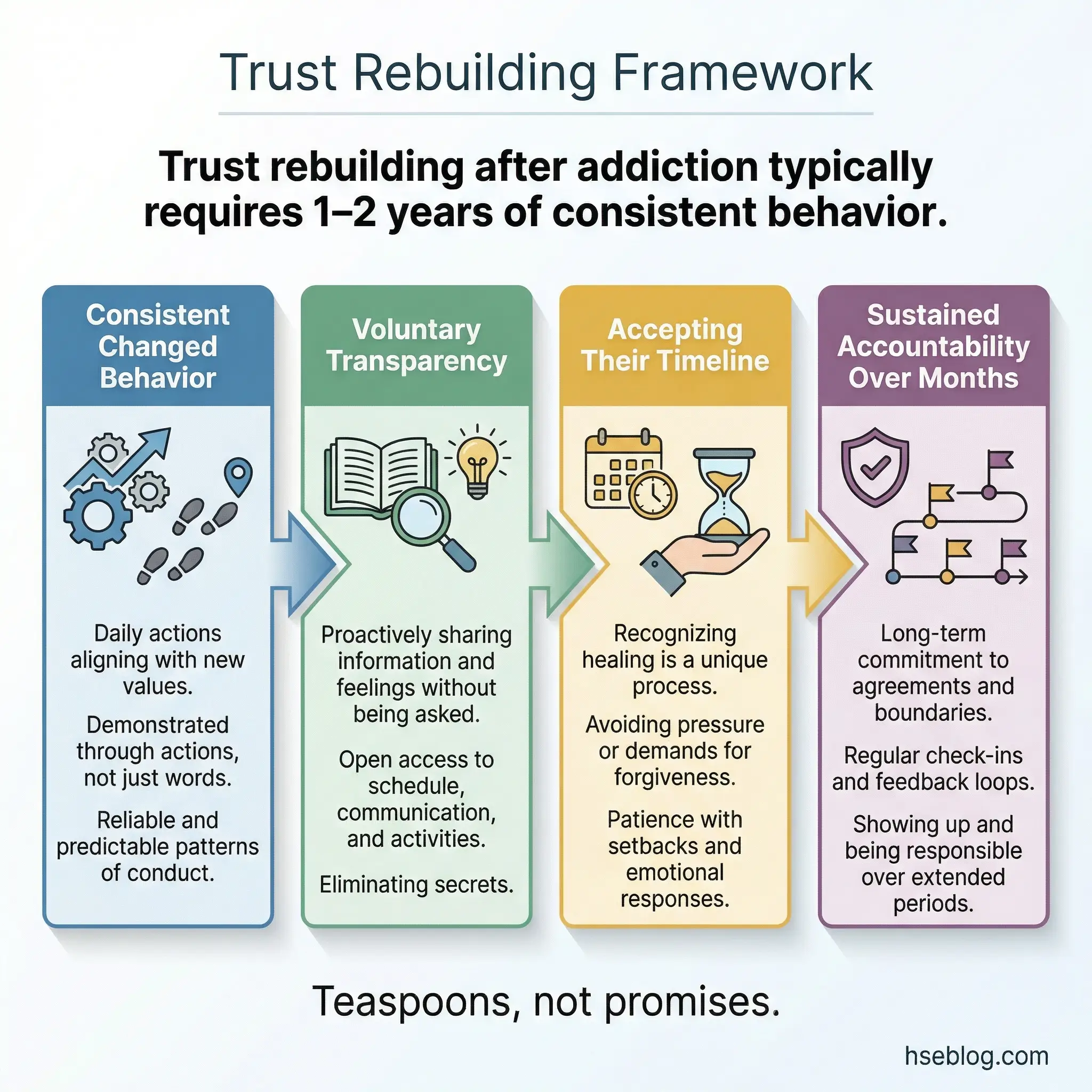
The framing I use: “Trust is rebuilt in teaspoons and destroyed in buckets. You’re working with teaspoons now.”
- Consistent behavior over verbal promises: The addicted person has likely made dozens of promises during active addiction — promises to stop, to change, to do better. Those promises are worthless currency. Only sustained, consistent behavior over time rebuilds trust. Actions over months. Not words over dinner.
- Accepting the other person’s timeline: The person rebuilding trust doesn’t get to decide when the injured party should “get over it.” Trust returns on the other person’s timeline, not the recovering person’s schedule.
- Transparency as a practice: Open phone, open schedule, proactive communication about whereabouts, honest reporting of struggles. Transparency isn’t surveillance — it’s a voluntary demonstration of accountability.
- Handling setbacks: When trust-building efforts hit a wall — a suspicious question, a moment of doubt from a partner, a family member’s continued resentment — the recovering person must not escalate defensively. The defensive reaction confirms the doubt. The calm, accountable response dissolves it.
Topic 36: Setting Boundaries in Recovery
Boundaries are not walls. They’re traffic signals — they tell the people in a recovering person’s life what’s acceptable and what isn’t, not to punish but to protect the recovery itself. Most participants have never set clear boundaries because addiction eroded their capacity to do so. This topic teaches boundary-setting as a learnable skill, not a personality trait.
With family members who still use, with friends who enable, with workplaces that don’t support recovery — every relationship requires recalibrated limits.
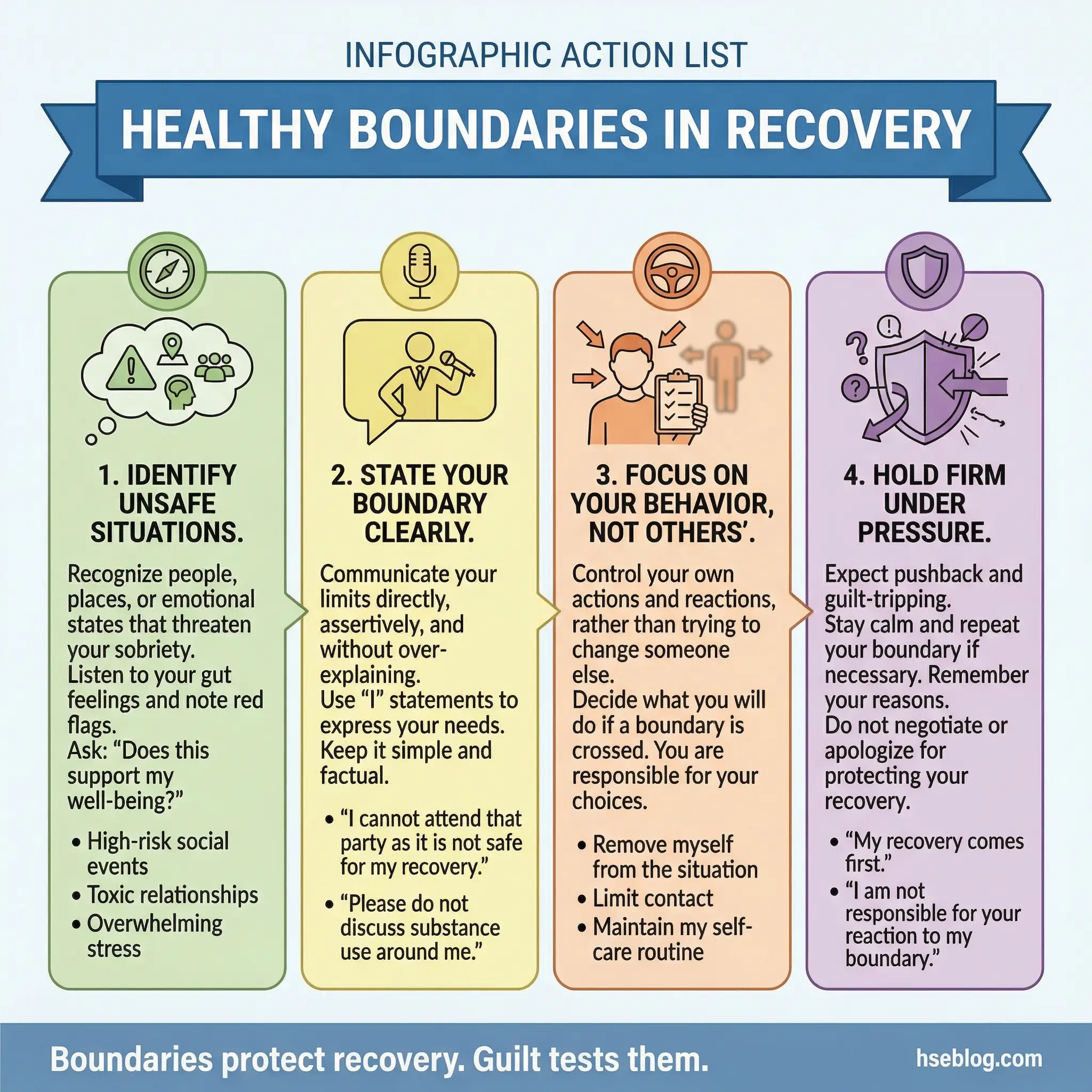
- Identifying where boundaries are needed: Ask participants to name three relationships or situations where they currently feel unsafe, pressured, or pulled toward substance use. Those are the boundary targets.
- Communicating boundaries clearly: “I can’t attend events where alcohol is the central activity” is a boundary. “You shouldn’t drink around me” is an attempt to control someone else. Boundaries govern the participant’s own behavior, not others’.
- Holding boundaries under pressure: Family guilt, social pressure, and workplace expectations will test every boundary. Practice responses: “I understand you’re disappointed. My recovery requires this.”
- Boundaries as relapse prevention: Every boundary that protects recovery is a structural safeguard. Remove the boundaries, and the recovery infrastructure weakens. Participants must understand that boundaries aren’t optional extras — they’re load-bearing walls.
Topic 37: Parenting in Recovery
Guilt about past behavior, anxiety about future capability, and the daily challenge of modeling healthy coping for children who may carry their own trauma from the parent’s addiction period — parenting in recovery is one of the most emotionally complex topics in the entire program. Handle it with directness and compassion.
Many parents in recovery carry a specific fear: that their children will follow their path. That fear is legitimate and statistically supported. But fear alone isn’t useful. This topic converts fear into constructive parenting strategy.
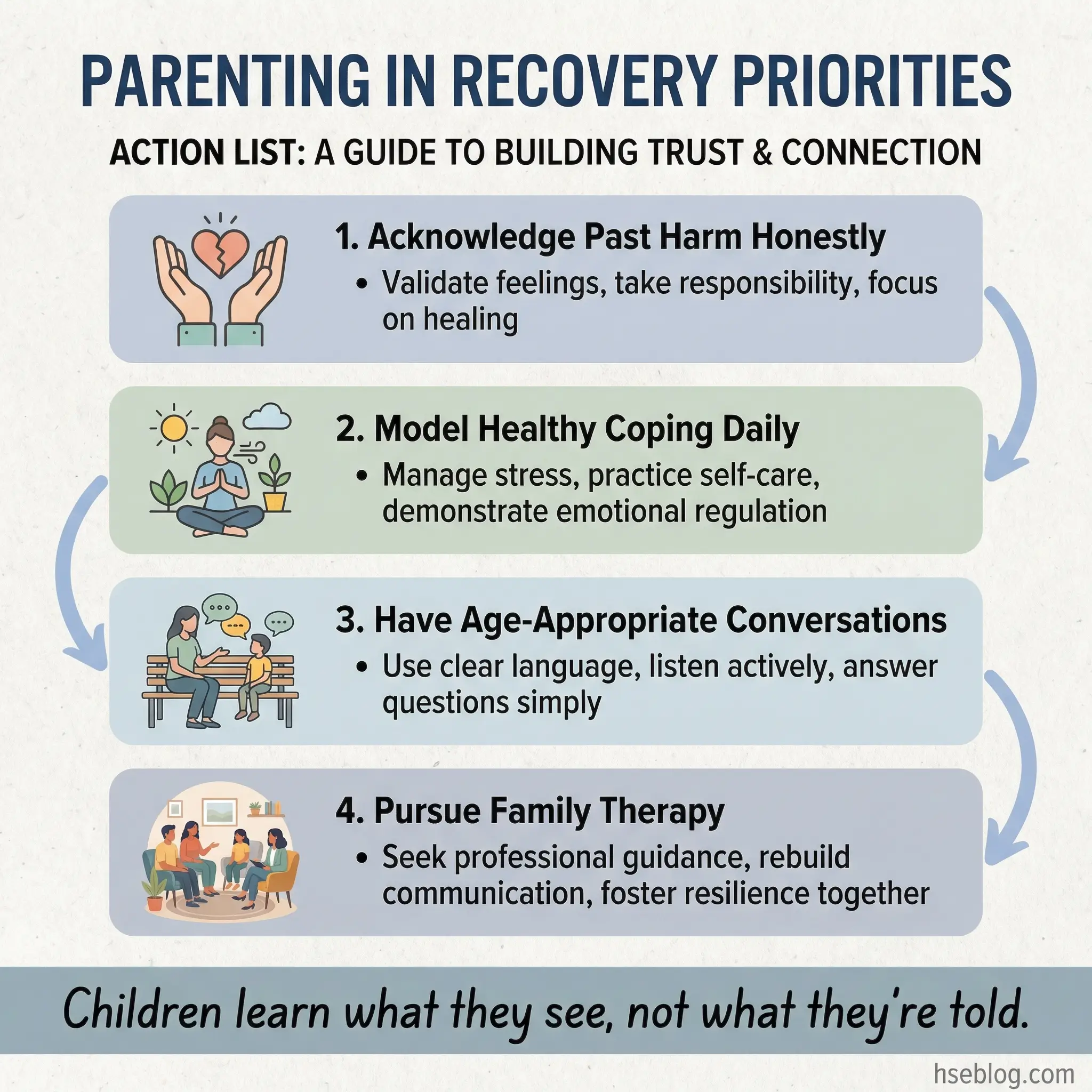
- Addressing guilt without drowning in it: Acknowledge the harm done during active addiction — honestly, specifically. Then pivot to the present: “What kind of parent am I being today? What kind of parent will I be tomorrow?” Guilt about the past is only useful if it drives present action.
- Age-appropriate conversations about addiction: Children deserve honest answers, calibrated to their developmental level. A 6-year-old doesn’t need clinical details. A 16-year-old can handle — and benefits from — a more frank conversation about the parent’s experience.
- Modeling healthy coping: Children learn more from what they observe than what they’re told. A parent who demonstrates stress management, emotional regulation, and accountability teaches these skills without a single lecture.
- Seeking family therapy: Individual recovery is necessary but insufficient when children have been affected. Family therapy provides a structured space for children to express their experience and for the parent-child relationship to be repaired with professional guidance.
Topic 38: Romantic Relationships and Recovery
The common advice to avoid new romantic relationships in the first year of recovery exists for a reason — but simply stating the rule without explaining the reasoning behind it invites defiance. This topic explores why early-recovery relationships are high-risk, how to navigate existing partnerships, and how substance use may have masked intimacy issues that now surface without chemical interference.
I’ve seen early-recovery relationships derail programs that were otherwise progressing well. The emotional intensity of a new relationship — the dopamine, the excitement, the distraction — can substitute for the substance itself, creating a dependency transfer that looks like progress but functions like relapse.
- Why the “no new relationships” guideline exists: Early recovery is a period of intense neurological and psychological recalibration. Adding the emotional volatility of a new relationship overloads a system already operating at capacity.
- Navigating existing partnerships: Partners who stayed through active addiction may carry resentment, trauma, and exhaustion. The relationship dynamic that existed during addiction must be renegotiated — and both parties may need couples counseling to navigate the transition.
- Intimacy without substances: Many people in recovery discover that substances were masking sexual anxiety, emotional vulnerability, or intimacy avoidance. Sober intimacy can feel terrifyingly exposed. Discuss this openly.
- Dependency transfer risk: The same reward-seeking brain patterns that drove substance use can drive relationship dependency. Monitor for signs: obsessive thinking, mood dependent entirely on the partner, neglecting recovery activities for relationship time.
Topic 39: Workplace Relationships After Disclosure
Returning to work after treatment — or continuing to work while in recovery — means navigating a social environment where people may know about the substance use. Supervisors who watched the performance decline. Colleagues who covered extra shifts. HR professionals who processed the leave paperwork. Each relationship carries a different dynamic, and none of them reset automatically because treatment occurred.
A clear substance abuse policy at the organizational level can make or break this transition. Workplaces that treat recovery as a supported process retain talent. Workplaces that treat it as a liability lose people.
- Managing supervisor dynamics: The supervisor may feel betrayed, burdened, or genuinely supportive — often all three simultaneously. Proactive communication about recovery commitments (meeting attendance, schedule needs) reduces uncertainty and builds professional trust.
- Handling colleague awareness: Some colleagues will be supportive. Some will be awkward. Some will gossip. Prepare for all three. Participants don’t owe detailed explanations to everyone — a simple “I took time to address a health issue and I’m doing well” is sufficient.
- Performance as the recovery statement: The most powerful way to rebuild professional credibility is consistent, reliable performance over time. Show up, do the work, meet deadlines, contribute to the team.
- Knowing your rights: Employees in recovery have legal protections under the Americans with Disabilities Act (ADA) in the US and equivalent legislation in other jurisdictions. Participants should understand what their employer can and cannot do regarding their recovery status.
Topic 40: Social Isolation vs. Healthy Solitude
Many people in recovery isolate themselves, calling it “protecting my sobriety.” There’s a critical difference between intentionally choosing solitude for rest, reflection, and recovery — and withdrawing from all human connection because interacting with people feels too risky, too exhausting, or too triggering. The first is healthy. The second is a relapse warning sign.
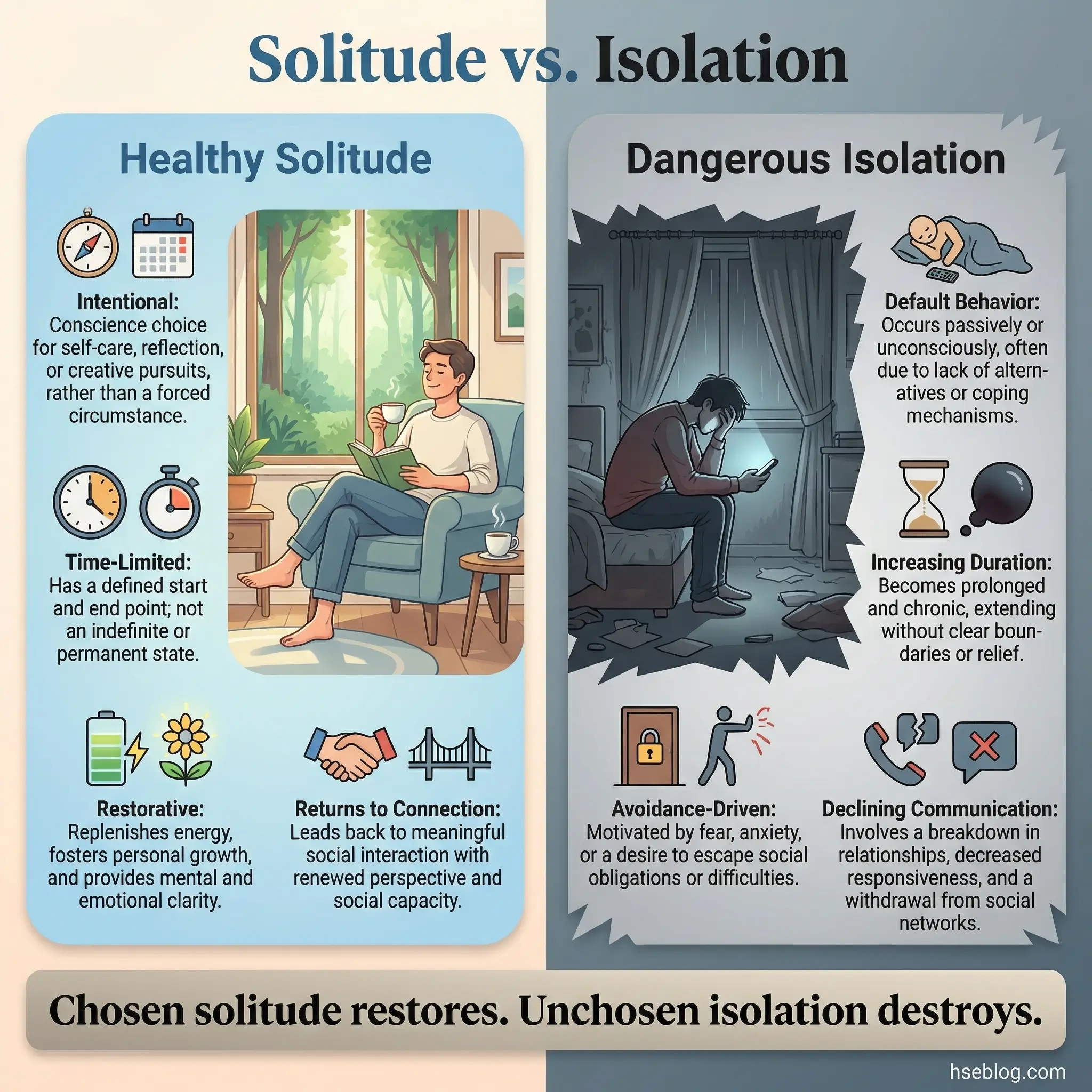
This topic challenges participants to examine their isolation patterns honestly. Is the time alone restorative? Or is it avoidance wearing a recovery mask?
- Healthy solitude characteristics: Chosen intentionally. Time-limited. Used for specific restorative purposes — reading, exercise, meditation, creative activities. The person emerges from it feeling refreshed, not more withdrawn.
- Dangerous isolation characteristics: Default behavior rather than intentional choice. Progressively increasing duration. Accompanied by declining communication with recovery supports. Used to avoid accountability, emotion, or effort.
- The loneliness-relapse pathway: Isolation produces loneliness. Loneliness is one of the most potent emotional triggers for substance use. The pathway from “I just need some space” to “I’m completely alone and craving” can be remarkably short.
- Structured social re-engagement: For participants who recognize isolation patterns, build structured social contact into the weekly schedule — not optional events but committed, scheduled interactions with recovery-supportive people.
Topics on Recovery, Accountability, and Building a New Life (Topics 41–50)
The final ten topics shift the conversation from managing addiction to building a life where substance use no longer fits. This is the aspirational phase — but it must stay grounded. I’ve seen too many recovery programs end on a motivational high that evaporates within 72 hours because participants leave with inspiration but no structure. These topics provide both.
Topic 41: Accountability Partners and Sponsorship Models
The mechanics of having someone who checks in, challenges excuses, and celebrates progress — that’s what accountability looks like in practice. This isn’t about surveillance. It’s about having one person in the world who has permission to ask, “How are you really doing?” and who won’t accept “fine” as an answer.
Discuss what makes a good accountability relationship, what makes a toxic one, and how to choose a partner or sponsor whose recovery maturity matches the participant’s needs.
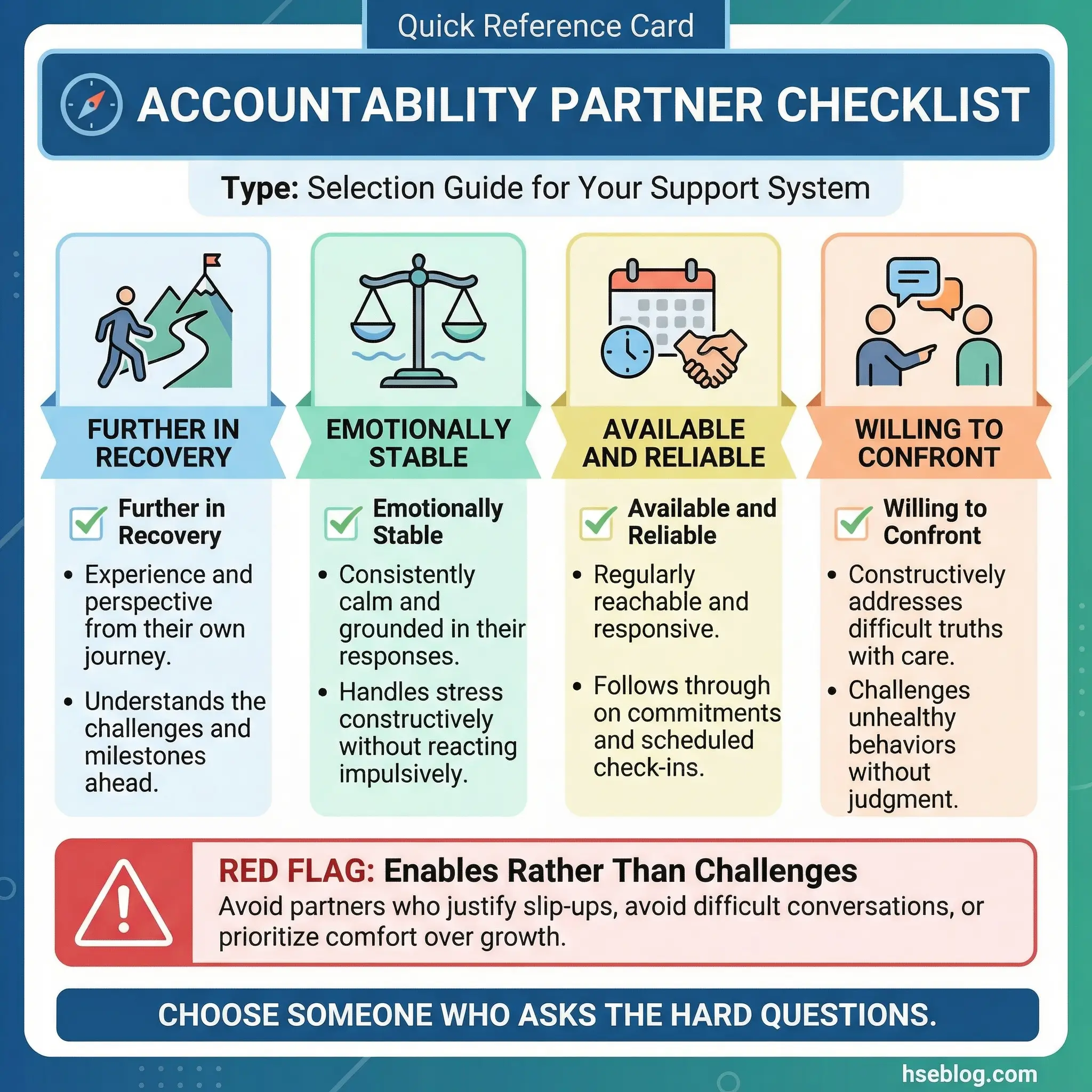
- What an accountability partner does: Regular check-ins (daily in early recovery, weekly thereafter), honest questioning, challenging rationalizations, celebrating genuine milestones, and providing immediate crisis support.
- Characteristics of a good accountability partner: Further along in their own recovery, emotionally stable, available and reliable, willing to confront rather than comfort, and not codependent.
- Sponsorship models: 12-step sponsorship, SMART Recovery peer support, workplace recovery champion programs, and faith-based accountability structures. Each model has strengths and limitations — participants should evaluate which aligns with their needs.
- Red flags in accountability relationships: Over-dependence on a single person, power dynamics that mimic codependency, accountability partners who enable rather than challenge, and sponsors who impose their own recovery model rather than supporting the participant’s.
Topic 42: Honesty as a Recovery Tool
This is not a philosophical topic about the virtue of truthfulness. It’s a practical discussion about how radical honesty — telling the truth about cravings, struggles, and setbacks — functions as a recovery mechanism. Every relapse I’ve investigated started with a lie. Not a dramatic lie. A small one. “I’m fine.” “The craving passed.” “I didn’t go to the meeting, but I was busy.” Small lies create the privacy that relapse needs to operate.
The group setting is the practice ground for honesty that participants then carry into daily life.
- Honesty about cravings: Saying “I’m craving right now” out loud to another person reduces the craving’s power. It breaks the secrecy that feeds the addiction cycle. Participants who normalize craving disclosure relapse less frequently.
- Honesty about setbacks: Missing a meeting, skipping a workout, reconnecting with a pre-recovery contact — these are warning signs that must be reported, not hidden. The group is the safety net for exactly these disclosures.
- Honesty about emotional states: “I’m angry,” “I’m lonely,” “I’m scared” — these statements are the raw material of recovery. Participants who learn to name their emotions accurately gain access to targeted coping responses instead of the blanket response of substance use.
- The cost of dishonesty in recovery: Every hidden struggle is an untreated vulnerability. Every downplayed craving is an unaddressed warning sign. Dishonesty doesn’t protect recovery — it creates the conditions for relapse to operate undetected.
Topic 43: Financial Recovery After Addiction
Debt, lost income, damaged credit, legal costs, and the compounding financial wreckage of years of substance use — this is the recovery topic that nobody finds glamorous and everybody needs. Practical financial planning — not shame-based budgeting lectures — is a recovery support tool that stabilizes one of the most stressful domains a person in recovery faces.
Financial stress is a relapse trigger. Addressing it directly reduces relapse risk. Ignoring it guarantees a persistent source of anxiety that substances will eventually be recruited to manage.
- Financial damage assessment: A structured, non-judgmental inventory of current financial reality — debts, income, expenses, legal obligations, credit status. Most participants have been avoiding this inventory because the numbers are frightening. The group setting provides accountability to face them.
- Basic budgeting for recovery: Income minus essential expenses equals the margin available for debt repayment, savings, and recovery-related costs (meetings, therapy, transportation). Simple, practical, immediate.
- Debt management strategies: Prioritization frameworks — address legal debts first (court-ordered payments, fines), then high-interest consumer debt, then remaining obligations. Small, consistent payments rebuild credit and reduce psychological burden.
- Income rebuilding: Career recovery, job search strategies, interview preparation for people with employment gaps or criminal records. Participants need practical support, not platitudes about “new beginnings.”
Topic 44: Legal Consequences and Navigating the System
DUI records, custody battles, criminal charges, employment background checks, probation requirements — participants in recovery often carry legal burdens that complicate every other aspect of their lives. This topic addresses those realities with information rather than fear. Catastrophizing doesn’t help. Clear-eyed understanding of legal options and obligations does.
Facilitators should bring printed legal resource sheets specific to the jurisdiction where the program operates. Generic legal advice is useless — participants need contact information for legal aid organizations, public defenders, and advocacy groups.
- Understanding legal obligations: Probation requirements, court-ordered treatment, mandatory reporting, driving restrictions, and community service. Non-compliance with legal obligations creates additional consequences that destabilize recovery.
- Employment and background checks: Many participants fear that their criminal record will permanently bar them from employment. Discuss the reality — which industries conduct what level of checks, which records can be expunged, and what legal protections exist for people in recovery.
- Custody and family court: Substance use history in custody proceedings. What courts look for in recovery evidence. How to document treatment completion and ongoing recovery engagement in a format that supports custody claims.
- Advocacy and legal rights: Participants have rights during and after treatment. Anti-discrimination protections, confidentiality of treatment records, and workplace accommodation requirements. Knowledge of these rights empowers participants to navigate systems rather than fear them.
Topic 45: Spirituality and Meaning-Making in Recovery
This is not a religious topic — and facilitators must establish that distinction immediately. Spirituality in the recovery context refers to purpose, connection, meaning, and the existential questions that surface when substances no longer fill the void. For participants who find spiritual frameworks helpful — whether religious, philosophical, nature-based, or humanistic — this topic provides space to explore that dimension of recovery.
Handle with absolute neutrality toward any belief system. No proselytizing. No assumption that everyone needs a spiritual framework to recover. For some participants, this is the most important session. For others, it’s irrelevant. Both responses are equally valid.
- Purpose beyond sobriety: Sobriety removes the substance. Purpose fills the space the substance occupied. Without purpose — whether found in family, work, community service, creativity, or faith — the empty space becomes a vulnerability.
- Connection to something larger: For some, this is God. For others, it’s nature, community, humanity, or an abstract sense of meaning. The specific “what” matters less than the felt experience of being connected to something beyond individual survival.
- Existential questions in recovery: “Who am I without substances?” “What is my life for?” “What do I believe about suffering and redemption?” These questions surface naturally in recovery and deserve a structured space for exploration.
- Respecting diverse frameworks: In a group setting, participants will hold vastly different spiritual and philosophical positions. The facilitator’s role is to hold space for all of them without privileging any. Unity comes from the shared recovery experience, not from theological agreement.
Topic 46: Career Rebuilding and Professional Identity
Many participants define themselves by what they lost — the job, the promotion, the professional reputation. This topic shifts the narrative from loss to construction. What does a professional identity look like when it incorporates — without being defined by — the recovery experience?
Some of the most effective substance abuse counselors, peer support specialists, and occupational health professionals I know built their careers specifically from their recovery experience. The journey itself became the credential.
- Reframing the employment gap: “I took time to address a health condition” is a legitimate, truthful, and sufficient explanation. Participants don’t owe interviewers a clinical history. Practice delivering this explanation with confidence.
- Transferable skills from recovery: Self-awareness, emotional regulation, crisis management, structured routine maintenance, communication skills developed in group settings — these are professionally valuable skills that recovery develops, even if they weren’t acquired through traditional career channels.
- Career exploration and pivoting: Some participants will return to their previous industry. Others may find that their pre-addiction career environment is incompatible with recovery. Discuss career pivoting without framing it as failure.
- Professional development during recovery: Certifications, training courses, volunteer work, and incremental skill-building. Recovery and career development can proceed in parallel — and the discipline required for one supports the other.
Topic 47: Substance Abuse Awareness in Your Community
This topic shifts the participant’s role from recipient of help to provider of help. Becoming a substance abuse awareness advocate — through volunteering, peer mentoring, community education, or simply sharing one’s story when appropriate — is both a service to others and a powerful recovery reinforcement tool.
The principle is well-established in recovery communities: you keep what you have by giving it away.
- Peer mentoring: Supporting someone earlier in their recovery journey. This requires emotional stability and clear boundaries — premature mentoring can burden a person whose own recovery is still fragile.
- Community education: Speaking at schools, community groups, or workplace awareness events about the reality of addiction and recovery. Personal narratives carry more weight than statistics in changing public perception.
- Volunteering with recovery organizations: Recovery community centers, helplines, shelter programs, and aftercare services all rely on volunteers with lived experience. Structured volunteering provides purpose, schedule, and social connection.
- Knowing when you’re ready: Not everyone should become an advocate immediately. Early recovery demands inward focus. Advocacy requires outward energy. Discuss how to recognize when the transition from self-care to service is appropriate — typically after at least 12 months of stable recovery.
Topic 48: Wellness Beyond Sobriety
Sobriety is the foundation, not the ceiling. This topic challenges participants to define what a genuinely fulfilling life looks like beyond the absence of substances — because a life defined only by what it’s missing is not sustainable.
I’ve met people years into sobriety who are technically clean but functionally miserable — no hobbies, no physical activity, no creative outlets, no joy. Sobriety without wellness is survival. Sobriety with wellness is living.
- Physical wellness: Regular exercise, nutrition, preventive healthcare, and body awareness. Many participants neglected their physical health during active addiction. Rebuilding it is both medically necessary and psychologically empowering.
- Intellectual wellness: Learning, reading, taking courses, engaging with ideas. The brain in recovery is rebuilding neural pathways — intellectual stimulation supports that process and provides the engagement that substances used to provide artificially.
- Creative wellness: Art, music, writing, building, cooking, gardening — any creative activity that produces a state of flow. Flow states generate natural dopamine through engagement, not substance use.
- Social wellness: Healthy relationships, community involvement, family connection, and meaningful social participation. Isolation may have defined the addiction period. Connection should define recovery.
Topic 49: Relapse as Data, Not Failure
This topic reframes past or potential relapse as information — a clinical data point to be analyzed, not a moral failure to be condemned. The shame-and-condemnation response to relapse drives people away from recovery. The analytical response drives them back toward it.
Every industrial incident investigation I’ve ever conducted follows the same principle: the event isn’t a failure to moralize about — it’s a data set to learn from. The exact same methodology applies to relapse.
- Root cause analysis of relapse: What triggered it? What coping mechanism failed? What environmental factor wasn’t addressed? What support was absent? Map the chain of events backward from the substance use to the first warning sign — exactly as you would in an incident investigation.
- Systemic vs. individual factors: Was the relapse driven by personal coping failure, or by a system failure — inadequate support, premature program discharge, untreated co-occurring disorder, workplace stress without mitigation? Often it’s both.
- Extracting actionable lessons: Every relapse teaches something specific if analyzed properly. The question is not “why did I fail?” but “what does this event tell me about what I need to change in my prevention plan?”
- Eliminating the shame spiral: Shame drives secrecy. Secrecy sustains relapse. Analytical framing breaks the cycle by treating relapse as a clinical event rather than a moral collapse. This reframe alone can be the difference between a single lapse and a sustained return to active addiction.
Topic 50: Writing Your Recovery Narrative
The final topic is both a closing exercise and a launching point. Each participant writes a one-page story structured around three sections: where they were, what changed, and where they’re headed. This is not a confessional or a memoir. It’s a distillation of the recovery journey into a document that functions as a personal accountability artifact, a reference point during difficult moments, and — for those who choose — a testimony that can help others.
Read aloud voluntarily. No one is compelled to share. But in every group where I’ve facilitated this exercise, at least two-thirds of participants chose to read, and the emotional impact on the room was consistently the most powerful moment of the entire program.
- Section 1 — Where I was: A honest, unflinching account of the person’s experience during active addiction. Not every detail — just the truth that matters. What was the reality? What was the cost?
- Section 2 — What changed: The turning point. Not necessarily a dramatic moment — sometimes it’s a quiet realization, a single conversation, or simply running out of alternatives. What shifted? What made recovery possible?
- Section 3 — Where I’m headed: Forward-looking, concrete, realistic. Not “I’m going to be happy forever” but “I’m going to attend my meetings, rebuild my relationship with my daughter, and complete my certification.” Specific goals anchored in observable behavior.
- The narrative as a living document: This story will evolve. Participants should revisit and revise their recovery narrative at the 6-month and 12-month marks. As recovery deepens, the story becomes richer, more honest, and more useful.
Pro Tip: At the final session, have each participant identify one topic from the 50 that changed their perspective the most, and one topic they want to revisit independently. This creates a self-directed continuation plan that extends the program’s impact well beyond the last meeting.
How to Facilitate Effective Substance Abuse Group Discussions
Having 50 strong topics means nothing if the facilitation fails. I’ve observed and trained facilitators across employee assistance programs, occupational rehabilitation centers, and community-based recovery groups. The patterns of failure are remarkably consistent — and almost always preventable.
Ground Rules and Session Structure
Before any topic is introduced, the group needs a framework that makes honest conversation possible. These structural elements are non-negotiable for effective facilitation:
- Confidentiality agreement: State it at the start of every session, not just the first one. “What’s shared here stays here” must be a living rule, not a one-time announcement.
- Voluntary participation: No one is forced to share. Silence is acceptable. Pressure to disclose creates resistance, not breakthroughs.
- No cross-talk during sharing: When someone speaks, the group listens. Feedback comes after, in structured rounds — not as interruptions.
- Time boundaries: Start on time, end on time. Open-ended sessions create anxiety. A 60–90 minute format with a clear opening, discussion body, and closing reflection works for most groups.
- Emotional safety protocols: If a participant becomes distressed, the facilitator must have a plan — a co-facilitator who can step out with the individual, a grounding exercise for the group, and a clear policy on when to pause or redirect.
Common Facilitation Mistakes
Every facilitator makes errors. The difference between a good facilitator and a harmful one is the ability to recognize and correct them. These are the mistakes I’ve seen cause the most damage:
- Over-sharing by the facilitator: Your role is to guide, not to become the center of the conversation. One brief personal reference per session maximum. The group is not your therapy.
- Allowing one participant to dominate: Redirect with gentle structure: “Thank you for sharing that. Let’s hear from someone who hasn’t spoken yet today.”
- Jumping to solutions: When a participant describes pain, the instinct is to fix it. Resist. Acknowledge first. Solutions come in their own time — often from other group members, not the facilitator.
- Avoiding difficult emotions: If someone cries, gets angry, or sits in uncomfortable silence, don’t rush to fill the space. Discomfort is where growth happens. Your job is to keep it safe, not comfortable.
- Poor topic sequencing: Don’t open with trauma on week one. Don’t save all the practical skills for the final session. Match emotional intensity to group maturity.
| Facilitation Element | Effective Approach | Ineffective Approach |
|---|---|---|
| Topic introduction | Brief context + open question | Reading a definition aloud |
| Participant silence | Allow 10–15 seconds before redirecting | Immediately calling on someone |
| Emotional distress | Acknowledge, ground, offer support | Minimizing or changing the subject |
| Dominant speaker | Structured turn-taking | Letting them continue unchecked |
| Session closing | Reflection + one takeaway per person | Abrupt end without processing |
Pairing discussion topics with hands-on substance abuse group activities increases retention and builds practical skill memory.
Pro Tip: After every session, spend 10 minutes writing facilitator notes: what worked, what didn’t, which participants seemed activated or withdrawn, and what topic adjustments are needed for the next session. These notes are your quality improvement system.
Conclusion
Substance abuse group topics are not a curriculum to check off. They are a carefully sequenced set of conversations designed to dismantle denial, build skills, and reconstruct a life that addiction dismantled. Every topic on this list has been tested in real group settings — employee assistance programs, occupational rehabilitation centers, peer support circles — and each one earns its place by producing the kind of honest, uncomfortable, transformative dialogue that no pamphlet, video, or solo counseling session can replicate.
The 50 topics presented here move from foundation to action: understanding addiction’s root causes, recognizing personal triggers, practicing coping skills, confronting mental health overlap, repairing damaged relationships, and building a recovery identity that extends far beyond sobriety. That sequence matters. Facilitators who skip the trust-building phases and jump to high-vulnerability topics lose their groups. Facilitators who stay in the educational phase too long bore their groups into disengagement. The architecture of the program is as critical as the content.
If you take one thing from this article, let it be this: a well-chosen substance abuse group topic doesn’t just fill 60 minutes. It gives a person sitting in that circle a word for something they’ve never been able to name, a strategy for something they’ve never been able to manage, or the realization that they are not the only one in the room carrying that particular weight. That’s not a discussion topic. That’s an intervention.