

TL;DR
- If your building has a hot and cold water system → you have a Legionella risk that requires a documented risk assessment, regardless of business size or sector.
- If hot water storage is below 60°C or cold water sits above 20°C → you are operating inside the temperature zone where Legionella pneumophila proliferates, and your primary control has failed.
- If your water management programme documents what to monitor but not what to do when a result exceeds the action level → your programme has the single most common gap that enforcement investigations expose.
- If you commission your Legionella risk assessment from the same contractor providing your water treatment → you have a conflict of interest that may compromise the assessment’s independence and inflate remedial costs.
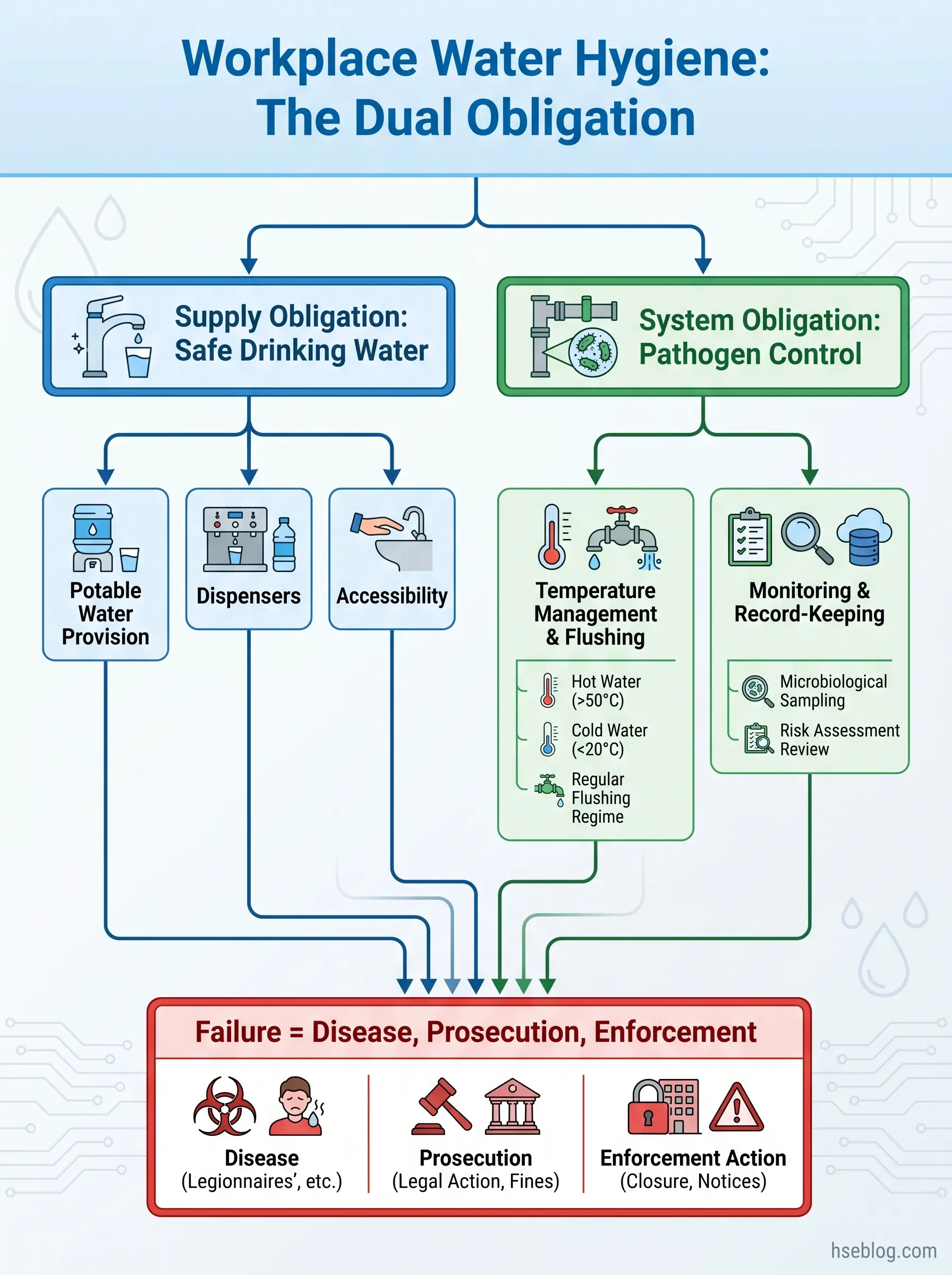
Water hygiene in the workplace is the management of all building water systems to achieve two employer obligations: providing safe potable drinking water for every worker and controlling waterborne pathogens — primarily Legionella pneumophila — within stored and distributed water. Compliance requires a written risk assessment, temperature controls (hot water stored at ≥60°C, delivered at ≥50°C, cold water below 20°C), a documented water management programme, and a competent responsible person with authority to act.
In 2024, a global surge in Legionnaires’ disease outbreaks hit four continents simultaneously — 114 cases and 2 deaths in Melbourne, 53 cases and 4 deaths in Lombardy, 30 cases and 2 deaths in London, and multiple clusters across the United States (The Lancet Microbe, 2024). These were not exotic exposures. They traced back to cooling towers, building water systems, showers, and taps — the same infrastructure present in every workplace. Legionnaires’ disease kills approximately one in ten people who contract it (CDC), and the organisms responsible thrive in precisely the water conditions that poor maintenance creates.
This guide covers both dimensions of workplace water hygiene that most resources treat separately: the obligation to provide clean drinking water and the obligation to manage building water systems so they do not become incubators for waterborne disease. It spans UK, US, and EU regulatory frameworks with clear jurisdictional attribution, walks through the risk assessment and water management programme process, and flags the practitioner failure patterns that enforcement investigations consistently expose. Whether you manage a single office or a multi-site portfolio, the controls are the same — and the consequences of neglecting them are criminal, not just operational.
What Is Water Hygiene in the Workplace and Why Does It Matter?
Water hygiene in the workplace is not limited to whether the drinking fountain works. It encompasses the full management of every water system within a building — hot and cold distribution networks, storage tanks, cooling towers, showers, decorative features, emergency eyewash stations — to ensure that the water supplied is safe to drink and that the systems storing and distributing it do not harbour organisms capable of causing serious illness.
The distinction matters because the two obligations require different controls. Providing potable drinking water is primarily a supply-chain question: is the water from an approved source, is it dispensed hygienically, is it accessible? Managing building water systems for pathogen control is an engineering and operational question: are temperatures maintained outside the growth range, is stagnation prevented, are biofilm and scale controlled, is monitoring conducted and acted upon?
A common practitioner error — one I encounter repeatedly in site audits — is treating “water hygiene” as synonymous with keeping drinking water dispensers clean. The reality is that the most dangerous waterborne exposure in a workplace almost never comes from the drinking water supply. It comes from the building’s hot and cold water distribution system, where Legionella pneumophila colonizes pipework, storage vessels, and dead legs, then transmits to workers through aerosols from showers, taps, and cooling towers. In 2017, approximately 230,000 work-related deaths globally were attributed to communicable diseases, many linked to poor water, sanitation, and hygiene conditions (ILO / UN DESA, 2017). Legionella is consistently identified by the WHO as the waterborne pathogen causing the highest health burden in the EU.
The consequences of failure span disease (Legionnaires’ disease, Pontiac fever, gastrointestinal illness from coliform contamination), criminal prosecution of duty holders, regulatory enforcement action, civil liability, and reputational damage that can outlast the illness itself.
What Are the Legal Requirements for Workplace Water Hygiene?
Workplace water hygiene sits under overlapping legal frameworks that impose duties on employers, building owners, and persons in control of premises. The obligations are not optional, and in most jurisdictions they carry criminal — not merely civil — liability. What follows is a jurisdiction-by-jurisdiction breakdown of the primary duties.
One pattern that enforcement investigations consistently reveal: organisations appoint a “responsible person” on paper to satisfy the regulatory requirement, but never verify that person’s competence, never give them budget authority, and never empower them to shut down a non-compliant system. The appointment becomes a liability shield on paper and a compliance gap in practice.
UK: ACoP L8, COSHH, and the Workplace Regulations 1992
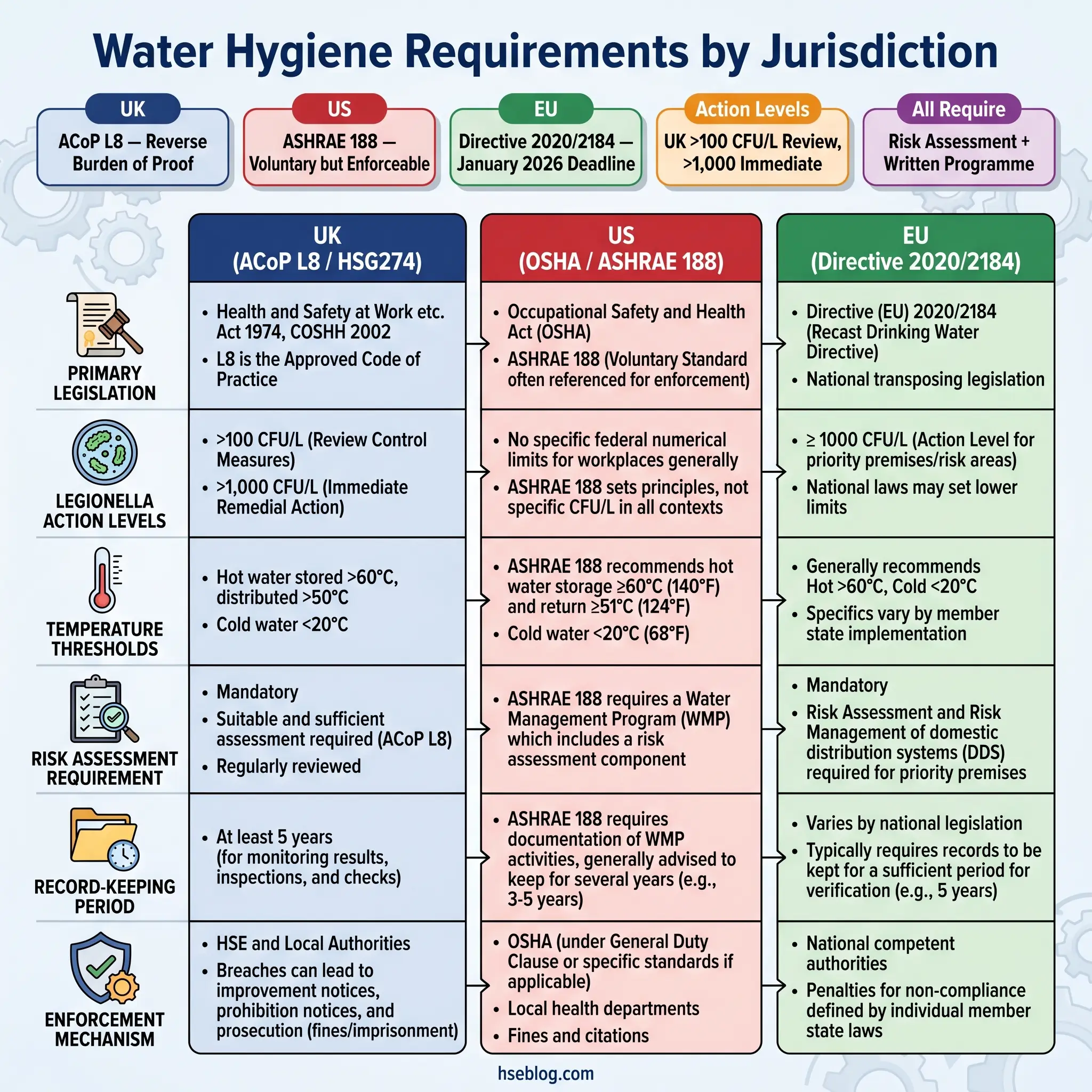
The UK framework is the most prescriptive and carries the strongest enforcement teeth. The legal chain runs from the Health and Safety at Work Act 1974 through the COSHH Regulations 2002 (which classify Legionella as a biological agent hazardous to health under Regulations 6, 7, 8, 9, and 12) to the Approved Code of Practice L8 — “Legionnaires’ disease: The control of legionella bacteria in water systems” (4th edition, 2013).
ACoP L8 has what UK law calls “special legal status.” Non-compliance does not automatically constitute a criminal offence, but in prosecution proceedings, the burden shifts: the duty holder must prove that they complied in an equally effective or better way. This reverse burden of proof makes ACoP L8 the de facto mandatory standard.
Under ACoP L8, duty holders must identify and assess sources of Legionella risk, prepare a written scheme to prevent or control that risk, implement and manage precautions, keep records for at least five years, and appoint a responsible person with sufficient authority, competence, and knowledge.
Separately, Regulation 22 of the Workplace (Health, Safety and Welfare) Regulations 1992 requires employers to provide an adequate supply of wholesome drinking water, readily accessible and conspicuously marked. HSG274 Parts 1–3 provide the technical guidance that supports ACoP L8 in practice — covering cooling towers (Part 1), hot and cold water systems (Part 2), and other risk systems (Part 3).
US: OSHA Sanitation Standards and ASHRAE 188
The US framework splits into two components. The potable water obligation sits under OSHA 29 CFR 1910.141 (General Industry), with parallel provisions in 1926.51 (Construction) and 1915.88 (Maritime). These require employers to provide potable water meeting EPA/US Public Health Service standards, dispensed from fountains or closed containers with taps. Open containers and common drinking cups are prohibited.
For Legionella, OSHA does not have a specific Legionella standard. Instead, enforcement relies on the General Duty Clause (Section 5(a)(1) of the OSH Act) and OSHA’s published guidance on Legionella hazard recognition. The voluntary standard that increasingly fills this gap is ANSI/ASHRAE Standard 188-2021, which establishes minimum risk management requirements for building water systems. While ASHRAE 188 is not itself law, it is referenced in building codes, used as the benchmark in enforcement actions, and recommended by the CDC’s Water Management Program toolkit.
The practical implication: US employers face a less prescriptive but no less enforceable landscape. OSHA can cite employers for Legionella exposures under the General Duty Clause, and ASHRAE 188 provides the standard of care against which “feasible” controls are measured.
EU: Drinking Water Directive 2020/2184
The EU Drinking Water Directive 2020/2184 represents the most significant update to European drinking water standards in over two decades. It introduces a risk-based approach from catchment to tap and, critically for workplace water hygiene, mandates Legionella risk assessments for “priority premises” — hospitals, hotels, care homes, and other buildings with large or complex water systems.
By January 2026, EU Member States must meet new parametric values for contaminants including PFAS, bisphenol A, and lead, and implement the Legionella action level of less than 1,000 CFU/L. This implementation milestone is the most significant regulatory change currently on the horizon for workplace water hygiene in Europe.
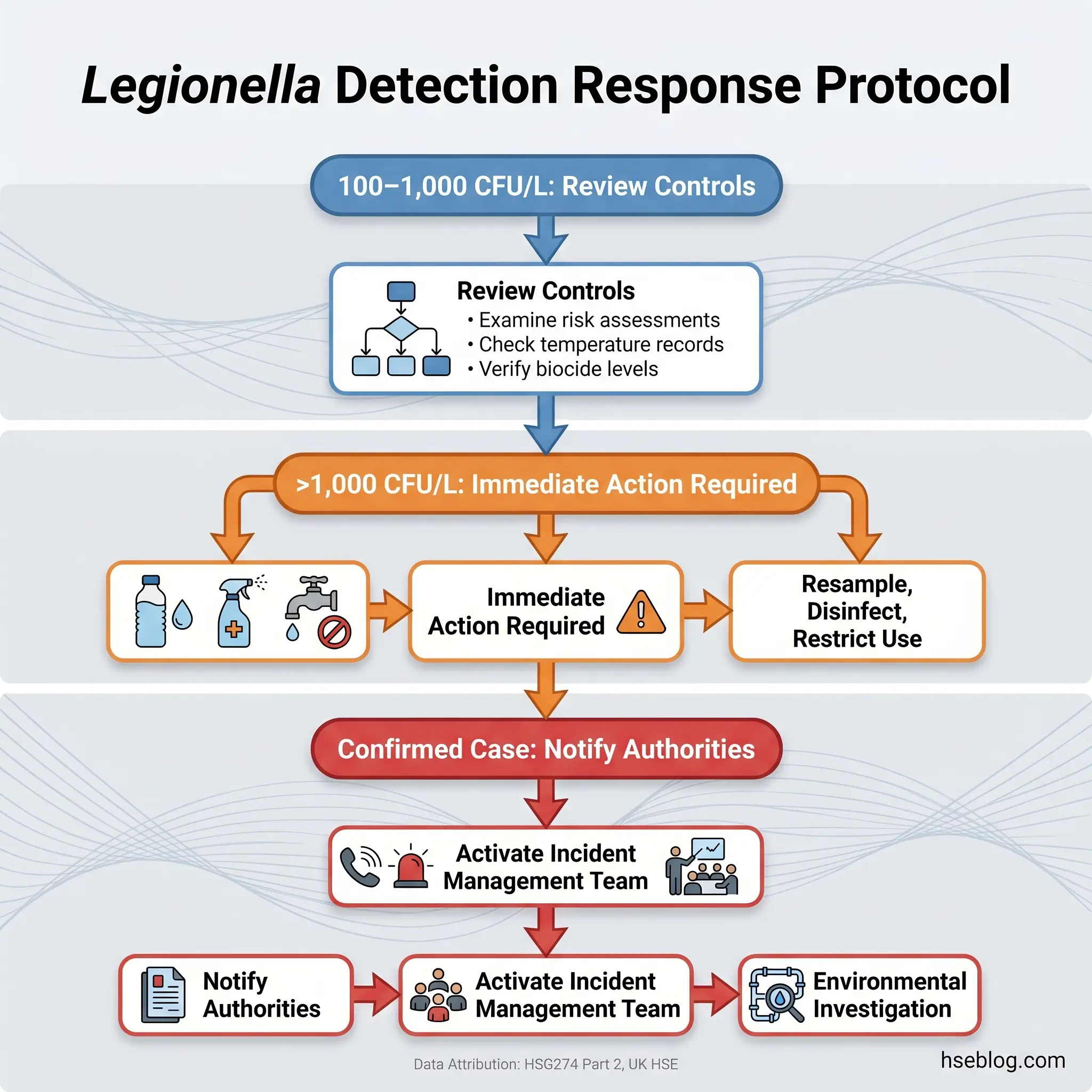
Jurisdiction Note: The UK’s tiered Legionella action levels (HSG274 Part 2: review controls at >100 CFU/L, immediate action at >1,000 CFU/L) are more conservative than the EU Directive’s single action level of <1,000 CFU/L. Some researchers have questioned whether the EU level is sufficiently protective. When managing multi-jurisdiction portfolios, adopt the UK tiered approach as the more protective reference.
What Are the Main Water Hygiene Risks in the Workplace?
The hazards in building water systems fall into three categories, and understanding their mechanisms is essential before designing any control programme.
Biological risks dominate. Legionella pneumophila is the primary concern — it colonizes water systems in the 20–45°C temperature range, with peak proliferation between 35–42°C. Transmission occurs through inhalation of contaminated aerosols (water droplets small enough to reach the lungs), not through drinking. Other biological hazards include Pseudomonas aeruginosa (a particular concern in healthcare settings), coliform bacteria indicating faecal contamination, and biofilm — the slimy matrix of microorganisms that coats internal pipe surfaces and provides both nutrients and protection for Legionella.
Chemical risks include lead leaching from older pipework, disinfection by-products from chemical treatment, and contaminant ingress through cross-connections or backflow failures. The EU Directive 2020/2184 now sets parametric values for PFAS and bisphenol A, reflecting growing awareness of these contaminants.
Physical risk factors create the conditions in which biological hazards thrive. These are the ones practitioners can most directly control: temperature excursions into the growth zone, water stagnation in underused sections of pipework, dead legs (sections with no flow or very infrequent flow), scale and sediment build-up providing nutrients, and inadequate system design that creates mixing zones where hot and cold water blend into the danger range.
The workplace water systems that create the highest risk include cooling towers (high-volume aerosol generation), hot and cold water distribution systems (showers and taps), decorative fountains, emergency eyewash stations that are tested infrequently, humidifiers, and spa pools.
One risk factor that facilities managers in partially occupied buildings consistently underestimate is stagnation in pipework serving unoccupied areas. When a floor or wing of a building sits empty, the water in those distribution lines reaches ambient temperature — often squarely within the Legionella growth zone — and remains static for days or weeks. Without a flushing regime for these outlets, the stagnant sections become colonization sites that can seed the entire system. This risk intensified during COVID-19 building shutdowns and remains relevant wherever buildings operate below full occupancy.
Watch For: Emergency eyewash stations and safety showers are legally required to be available but are often tested only during annual inspections. The water sitting in their supply lines between tests is stagnant, warm, and an ideal Legionella habitat. Weekly activation — flushing for at least three minutes — should be part of any water management programme.
How to Conduct a Water Hygiene Risk Assessment
A water hygiene risk assessment is the foundation document from which every other control flows. Without it, temperature monitoring, flushing regimes, and sampling programmes have no rational basis — you are managing controls without knowing what you are controlling against.
The process outlined in ACoP L8 and HSG274 Part 2 (UK) and the ASHRAE 188 / CDC Water Management Program toolkit (US) follows a consistent logic, even though the terminology differs between jurisdictions.
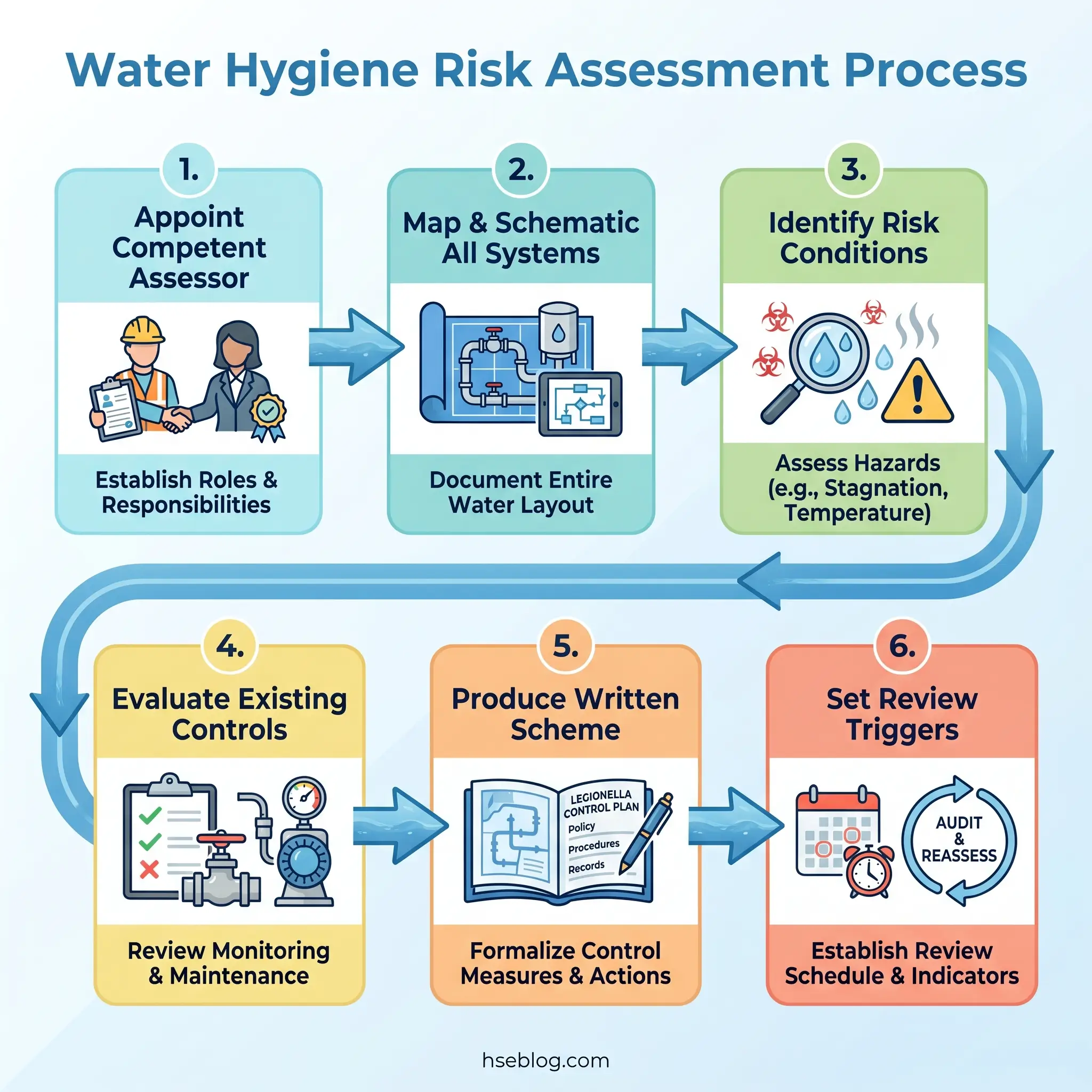
Step 1 — Appoint the assessor and verify competence. The person conducting the assessment must have demonstrable competence in water hygiene risk management. In the UK, ACoP L8 requires the duty holder to ensure the assessor has “appropriate training and knowledge.” There is no single mandatory qualification, but training aligned with HSE UK’s expectations (typically covering microbiology, system design, and control strategies) is the practical standard. A critical judgment call: organisations that commission their risk assessment from the same contractor providing their ongoing water treatment services create a conflict of interest. The contractor has a financial incentive to identify risks that generate treatment revenue. Independent assessment is a best-practice principle worth the additional cost.
Step 2 — Describe and schematic the system. The assessment must map every water system in the building — supply source, storage tanks, calorifiers/water heaters, distribution pipework (including dead legs), outlets, cooling towers, and any ancillary systems. A schematic drawing is not optional; it is the reference document that makes monitoring and remedial work possible.
Step 3 — Identify risk conditions. Walk the system against known risk factors: temperature excursions, stagnation points, biofilm potential, aerosol-generating outlets, scale and sediment, system age and material. Identify susceptible persons — immunocompromised workers, visitors to healthcare or care settings, anyone exposed to aerosol sources.
Step 4 — Evaluate existing controls. Document what controls are already in place — temperature settings, flushing schedules, treatment regimes — and assess whether they are adequate, consistently implemented, and recorded.
Step 5 — Determine residual risk and produce the written scheme. The output is a written scheme of control (UK) or water management programme (US) specifying: what must be monitored, at what frequency, by whom, what the acceptable parameters are, and — critically — what action must be taken when a parameter is exceeded. This last element is the one most programmes leave vague.
Step 6 — Set review triggers. The assessment is not a one-time exercise. UK guidance under ACoP L8 states it must be reviewed “regularly” and specifies trigger events: any change to the water system, after a reported case of Legionnaires’ disease, after any incident suggesting the controls have failed, and periodically regardless. ASHRAE 188 builds ongoing review into the programme cycle. A two-year periodic review is a widely adopted benchmark, but event-driven reviews should not wait for the calendar.
Records from the risk assessment and all subsequent monitoring must be retained for at least five years under UK guidance. Under ASHRAE 188, indefinite retention is best practice.
Water Temperature Control: The Primary Defence Against Legionella
Temperature control is the single most effective measure for preventing Legionella colonization in hot and cold water systems. Every other control — chemical treatment, flushing, filtration — is either supplementary or compensatory. If the temperatures are right, the risk is fundamentally managed. If they are wrong, no amount of sampling will make the system safe.
The critical thresholds are broadly consistent across jurisdictions:
- Hot water storage (calorifier/boiler): ≥60°C
- Hot water at outlets: ≥50°C within one minute of running the tap
- Cold water: ≤20°C, with ≤24°C as the absolute maximum tolerable after stagnation periods
- Legionella growth zone: 20–45°C, with peak proliferation at 35–42°C
- Thermal kill point: Above 60°C, Legionella is killed; above 70°C, it is killed almost instantly
The practical challenge is maintaining these thresholds at every point in the distribution system, not just near the heat source. A pattern that appears repeatedly in enforcement investigations: temperature monitoring records show “compliant” readings at sentinel outlets near the calorifier — the easy-to-access taps that the monitoring technician checks every month — while distant outlets, dead legs, and infrequently used fixtures on remote floors have never been tested. Those distant points are exactly where temperatures decay into the growth zone, and they are exactly where colonization begins.
Monitoring frequency under HSG274 Part 2 (UK) calls for monthly checks at sentinel outlets (nearest and furthest from the calorifier, plus the return leg) and representative checks at other outlets on a rotating basis to cover all outlets within a defined period. ASHRAE 188 (US) requires monitoring as defined in the building’s water management programme, with frequency determined by the risk assessment.
Audit Point: When reviewing temperature monitoring records, check the furthest outlet from the heat source, the outlet with the longest dead leg, and any outlet on an infrequently occupied floor. If these have never been monitored, the programme is testing convenience, not risk.
The scald-risk trade-off deserves mention. Storing and distributing water at temperatures that kill Legionella creates a scalding hazard at the point of use, particularly in care settings, schools, and facilities serving vulnerable populations. Thermostatic mixing valves (TMVs) are the standard engineering control — they blend hot and cold water to a safe delivery temperature at the outlet while allowing the distribution system to operate at Legionella-lethal temperatures. TMVs themselves require routine maintenance; a stuck or failed TMV can deliver either scalding water or water in the Legionella growth zone.
Developing a Water Management Programme
The risk assessment identifies what must be controlled. The water management programme — called a “written scheme of control” under ACoP L8 (UK) or a “water management programme” under ASHRAE 188 (US) — is the operational document that specifies how those controls are executed, monitored, and maintained on an ongoing basis. It is a living document, not a compliance filing that sits in a drawer.
ASHRAE 188 structures the programme around seven core elements: water management team, system description, control measures, monitoring procedures, corrective actions, verification activities, and documentation. ACoP L8 requires a system schematic, operating procedures, precautions to prevent or control risk, monitoring schedules, and remedial action procedures. The language differs; the substance converges.
Three roles form the governance backbone. The responsible person (UK) or programme leader holds overall accountability and must have authority to commit resources and shut down non-compliant systems. The authorised person executes day-to-day monitoring tasks. In larger organisations, a water safety group — a cross-functional team including facilities, HSE, and occupational health — provides oversight and review.
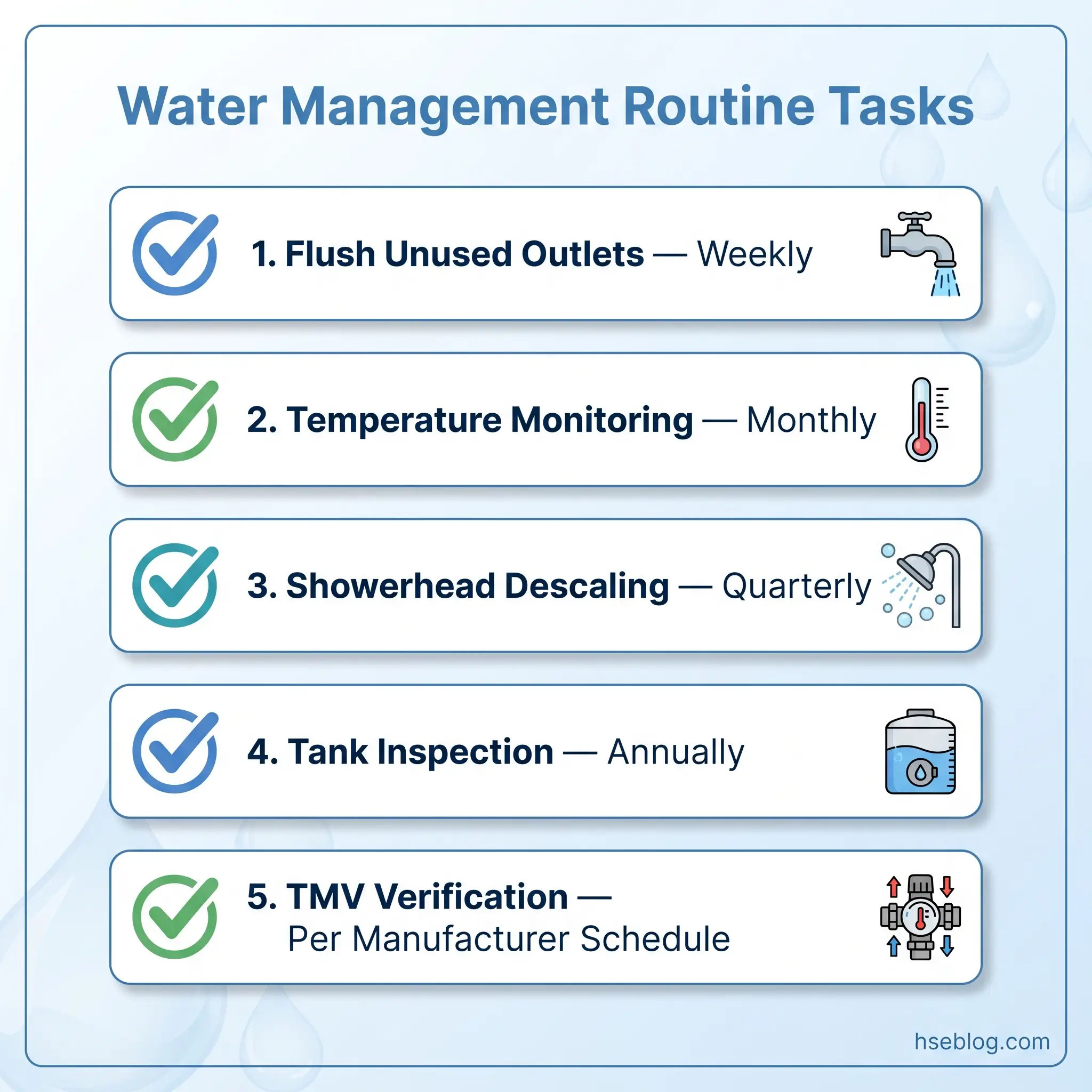
Routine tasks that the programme must schedule, assign, and record include flushing infrequently used outlets (weekly), cleaning and descaling showerheads (quarterly or as specified by the risk assessment), inspecting cold water storage tanks (annually, with attention to lid integrity, insulation, and internal condition), verifying TMV function (at intervals specified by the manufacturer and risk assessment), and temperature monitoring as discussed above.
The biggest gap in most water management programmes is the response protocol. Organisations are generally competent at documenting what to monitor and when. Where they consistently fail is specifying what to do if a result falls outside the acceptable range. A facilities technician who records a cold water temperature of 28°C at a distant outlet needs clear, written instructions: who to notify, what interim measures to implement (increased flushing, restriction of use), what investigation to initiate, and who has authority to escalate to emergency disinfection if the problem is systemic. Without that clarity, the technician logs the reading, nobody acts, and the next month’s reading is 30°C.
The Fix That Works: For every monitored parameter in your water management programme, add a column to your monitoring sheet: “Action if out of specification.” Populate it with named escalation contacts, interim control measures, and investigation triggers. This converts a monitoring form into a response system.
Providing Safe Drinking Water: Employer Obligations
Distinct from the system-safety obligations above, employers carry a straightforward duty to provide workers with safe drinking water. This obligation is simpler in concept but generates a surprising number of compliance failures in practice.
In the UK, Regulation 22 of the Workplace (Health, Safety and Welfare) Regulations 1992 requires an adequate supply of wholesome drinking water, readily accessible and conspicuously marked where necessary. Cups or a drinking jet must be provided. Mains tap water meeting public supply standards satisfies the requirement — employers are not obligated to provide bottled or filtered water. Enclosed refillable containers are acceptable where a mains supply is not reasonably practicable, but they must be refilled at least daily.
Under OSHA 29 CFR 1910.141 (US), potable water must meet US Public Health Service / EPA standards. It must be dispensed from fountains or closed containers with taps. Open containers are prohibited. Common cups are prohibited. Employers cannot charge workers for drinking water.
Both jurisdictions share a “readily accessible” requirement that many workplaces fail to meet in practice. A single water cooler in a distant break room does not satisfy the obligation for workers on a large floor plate or in a spread-out facility. OSHA inspectors enforce the principle that workers should not need to travel an unreasonable distance or leave their work area for an extended period to access water. In hot environments or during physically demanding work, the provision obligation increases — more water, more access points, more frequently restocked.
Non-potable water outlets — industrial process water, recycled water, untreated supplies — must be clearly and conspicuously marked in both jurisdictions to prevent accidental ingestion.
Monitoring, Testing, and Record-Keeping
Routine monitoring is the feedback mechanism that tells you whether your controls are working. Without it, temperature settings, flushing schedules, and treatment regimes operate on assumption rather than evidence.
The monitoring regime for a typical hot and cold water system includes monthly temperature checks at sentinel outlets, quarterly checks at other outlets on a rotating basis to cover all outlets over a defined period, annual visual inspection of cold water storage tanks and calorifiers, and showerhead cleaning and descaling on the schedule specified by the risk assessment.
Whether routine Legionella sampling (microbiological testing of water for Legionella counts) is required depends on the system’s complexity and risk profile. For simple systems — mains-fed hot and cold water only, no cooling tower, no large-volume storage, properly maintained temperature controls — HSG274 Part 2 (UK) does not require routine sampling. The controls are the primary defence, and temperature monitoring verifies them. For complex systems, cooling towers, and systems with a history of colonization, quarterly Legionella sampling is standard practice.
A misconception worth correcting: some organisations test water monthly from low-risk, well-controlled systems purely because their water treatment contractor includes sampling in the service contract and charges for it. They treat sampling as a substitute for operational controls. Sampling is a verification tool. It confirms that the controls are working or reveals that they have failed. It does not itself prevent Legionella growth. Over-sampling from low-risk systems while neglecting temperature control is a misallocation of both effort and budget.
Record retention is a compliance requirement and an evidential necessity. UK guidance under ACoP L8 specifies a minimum of five years. Under ASHRAE 188, indefinite retention is best practice. Records must demonstrate not only what was monitored but what actions were taken when results were unsatisfactory — this is the chain of evidence that prosecutors and regulators examine.
What to Do If Legionella Is Detected or an Outbreak Occurs
The response to Legionella detection depends on the count and the context. HSG274 Part 2 (UK) defines a tiered action framework. Counts between 100 and 1,000 CFU/L trigger a review of the risk assessment, control measures, and water management programme to identify the failure. Counts exceeding 1,000 CFU/L require immediate action: resample, implement corrective measures (which may include thermal disinfection or chemical disinfection), review the entire control scheme, and consider whether the system should be restricted from use until the cause is identified and resolved.
Thermal disinfection — sometimes called pasteurisation — involves raising the hot water system to 70°C or above at the calorifier and flushing all outlets sequentially until each delivers water at 60°C or above for at least two minutes. Chemical disinfection typically uses chlorination to achieve a target concentration throughout the system for a defined contact time. Both procedures require competent execution to be effective and safe.
When a confirmed case of Legionnaires’ disease is linked to a workplace, the situation shifts from maintenance response to incident management. Legionnaires’ disease is a notifiable disease in the UK and a nationally notifiable condition in the US (with state-specific reporting requirements). Public health authorities must be informed. The building’s water system becomes a potential crime scene for environmental investigation.
The critical mistake in outbreak response — and this pattern appears in published investigation after investigation — is treating the situation as a plumbing problem rather than an incident requiring multi-agency coordination. Organisations that respond by dispatching maintenance staff to “flush the system” without involving public health authorities, occupational health, legal counsel, and their insurer are simultaneously increasing their liability, potentially destroying evidence, and likely failing their statutory notification duties.
Field Test: Ask the person responsible for your water management programme: “If you received a Legionella count of 5,000 CFU/L from a cooling tower sample tomorrow morning, what exactly would you do in the first two hours?” If the answer involves hesitation, checking a manual, or calling a contractor to ask what to do — the response protocol needs rewriting.
Frequently Asked Questions
Conclusion
The industry’s persistent error with workplace water hygiene is treating it as two separate, disconnected obligations — a facilities task (keep the water cooler working) and a specialist task (manage Legionella) — rather than a single integrated programme. That fragmentation is how buildings end up with compliant drinking water dispensers on every floor and 32°C water sitting in dead legs behind the walls. The 2024 global surge in Legionnaires’ disease outbreaks, documented across four continents, is a reminder that Legionella exploits exactly the gaps between responsibilities.
The single highest-impact change most organisations can make is not technical. It is completing the response column in their water management programme. Every monitored parameter needs a defined action when it falls outside specification — who to contact, what interim measure to implement, who has authority to escalate. Without that, monitoring is record-keeping theatre: you document the failure but do nothing about it.
Water hygiene in the workplace is not a specialist concern to be delegated and forgotten. It is a duty holder obligation with criminal liability, a public health responsibility in every building where water is stored, heated, cooled, or aerosolised, and — for approximately one in ten people who contract Legionnaires’ disease — a question of survival.