

TL;DR
- If your welding fume controls were designed before 2019, they almost certainly fail the current HSE enforcement expectation — and may not withstand an OSHA multi-standard citation either.
- If you’re sampling total fume mass and declaring compliance at 5 mg/m³, you’re missing the legally meaningful exposures — Cr(VI) and manganese — that drive enforcement and disease.
- If RPE is your primary welding fume control, expect a citation: both OSHA and HSE treat respiratory protection as residual, not primary, and inspectors check LEV first.
- If you assume mild steel welding is low-risk, IARC’s 2017 Group 1 carcinogen classification was based substantially on mild-steel cohorts — and HSE’s 2019 enforcement change was the direct regulatory response.
Welding fume is classified as a Group 1 human carcinogen by IARC (reclassified 2017, Monograph 118), and since 2019, the UK HSE requires engineering controls — typically local exhaust ventilation — for all indoor welding regardless of duration, with suitable RPE where LEV alone is insufficient. In the US, OSHA regulates welding fume constituents individually, with the hexavalent chromium PEL of 5 µg/m³ under 29 CFR 1910.1026 as the most stringent driver. Effective welding fume control applies the hierarchy of controls: eliminate or substitute the process, install LEV at the arc, then layer administrative controls and respiratory protection as residual measures.
Regulatory content here reflects general HSE professional understanding of US (OSHA), UK (HSE), and EU requirements as of the last-reviewed date. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction. Verify regulatory references against the issuing authority’s current text before acting.
Why Welding Fume Control Is Now a Regulator Priority: The 2017–2019 Shift
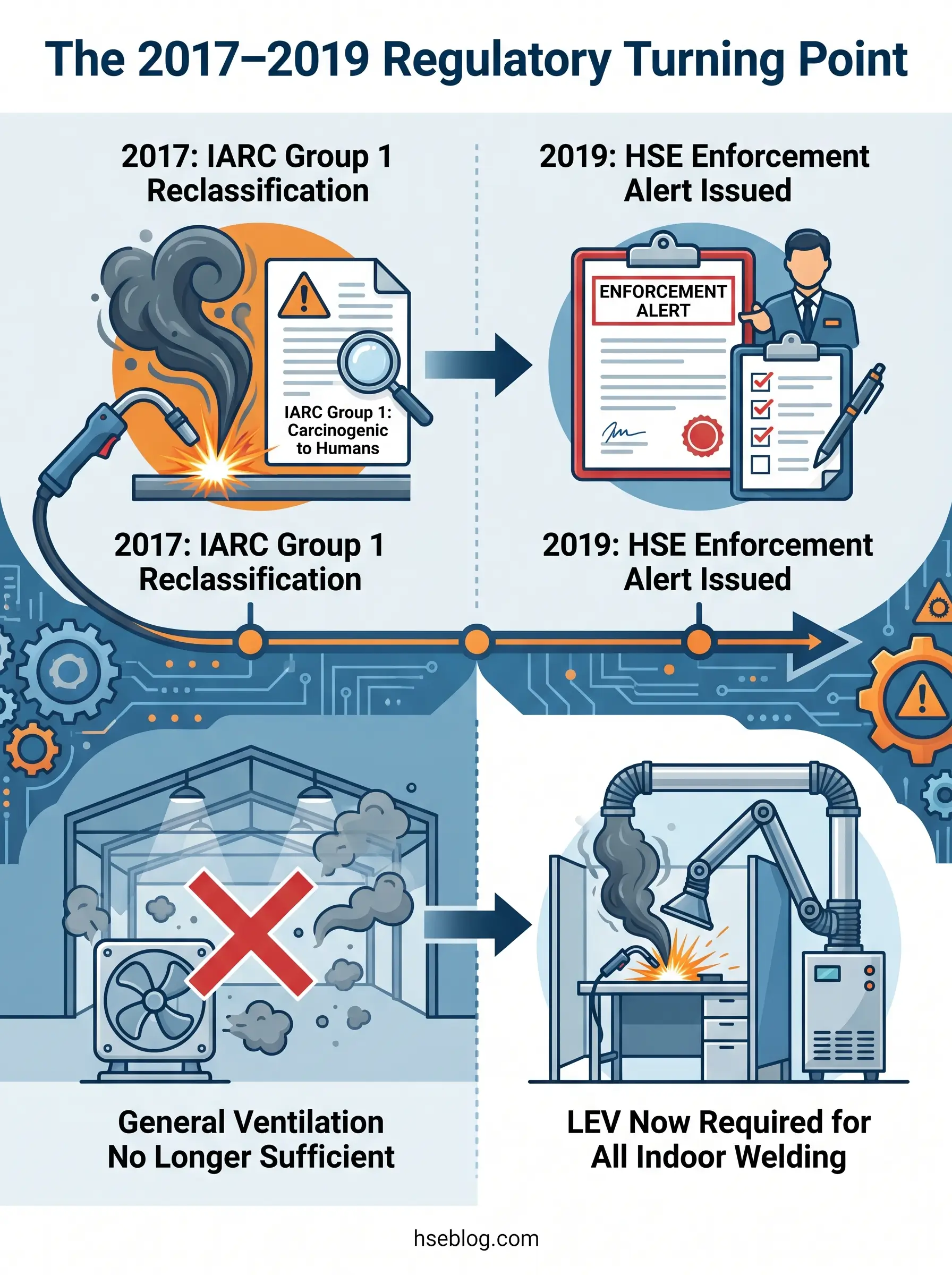
Approximately 11 million workers worldwide hold the job title of welder, with an additional 110 million incurring welding-related exposures (IARC, 2018). For decades, mild steel welding was treated as a nuisance-dust problem on most shop floors — fume was visible, unpleasant, and managed with general ventilation or a door propped open. That assumption collapsed in 2017.
IARC Monograph 118, published in 2017 and formally released in 2018, reclassified welding fumes from Group 2B (“possibly carcinogenic,” a designation held since 1989) to Group 1 (“carcinogenic to humans”), based on sufficient epidemiological evidence for lung cancer and positive associations for kidney cancer. The evidence was not limited to exotic alloys or stainless steel — it drew substantially from mild-steel-dominant cohorts.
The UK Health and Safety Executive responded directly. HSE Safety Alert STSU1 – 2019(1) declared that general ventilation alone is no longer acceptable for any indoor welding, including mild steel, regardless of duration. Suitable engineering controls — typically LEV — are required indoors, with adequate RPE for outdoor welding and wherever LEV proves insufficient. In the US, OSHA has no single welding-fume PEL; instead, constituents like hexavalent chromium, manganese, nickel, cadmium, and ozone are regulated under individual standards, with 29 CFR 1910.1026 (Cr(VI)) the most stringent driver. OSHA inspections increasingly cite multiple standards per welding incident.
A consistent pattern in UK fabrication inspections since 2019 is worth noting: the most common citation is not “no LEV present” but “LEV present but not tested, not positioned correctly, or used only when convenient.” Many sites assume a pre-2019 control posture remains compliant because no one in management has read the updated alert.
What’s Actually in Welding Fume — and Why Composition Drives the Control Decision
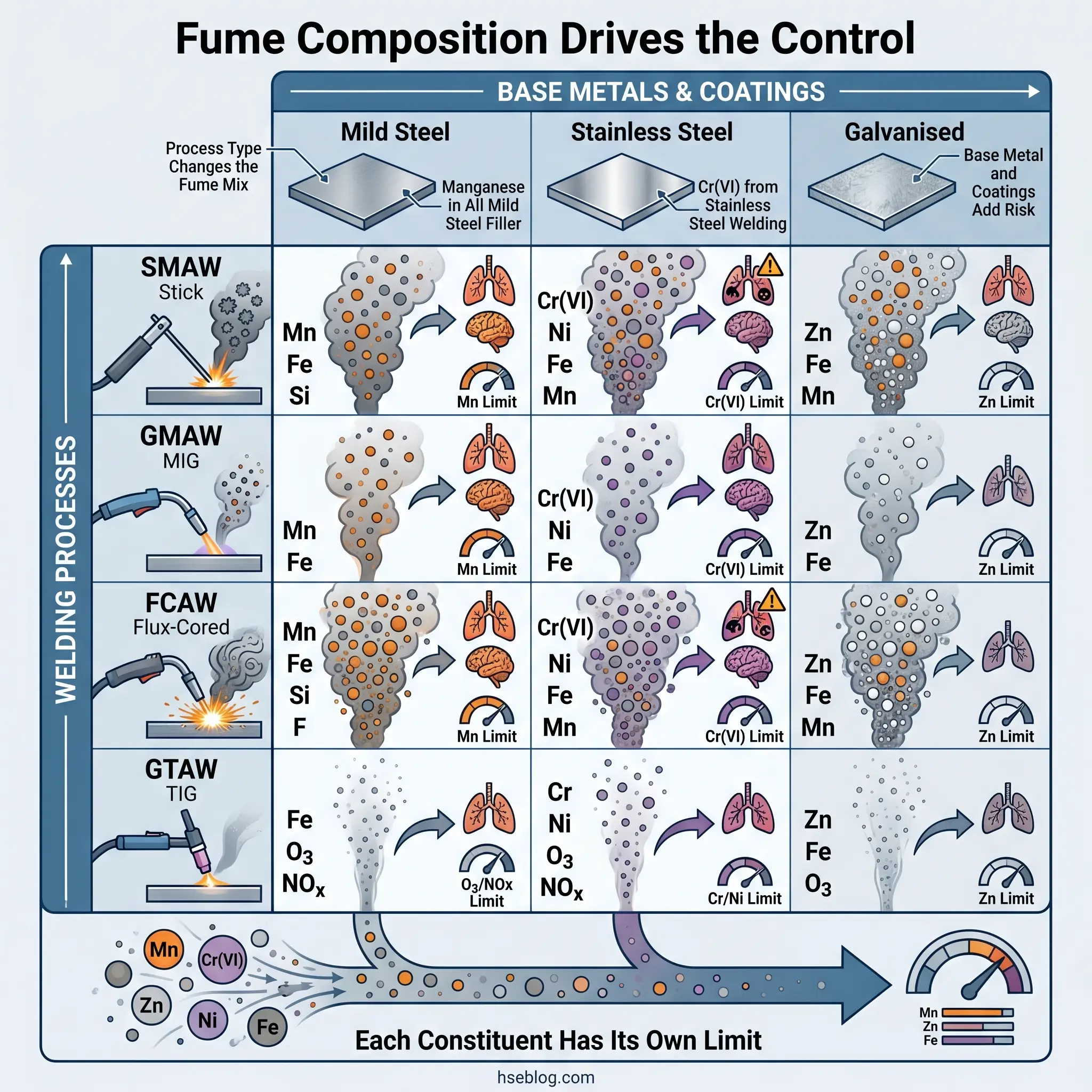
The most consequential misjudgment in welding fume risk assessment is treating “welding fume” as a single substance with a single exposure limit. It is not. The composition of the plume dictates which regulations apply, which health endpoints are at stake, and which controls are defensible.
Particulate Constituents
The metal particulate fraction varies with the base metal, filler wire or electrode, flux, and any surface coating. Key constituents include iron oxide, manganese, hexavalent chromium (Cr(VI)), nickel, lead, cadmium, zinc, copper, molybdenum, and — in specialised applications — beryllium. The regulatory consequence is direct: each metal carries its own PEL, WEL, or TLV, and the strictest applicable limit governs the control design.
Surface coatings change the risk profile entirely. Galvanised steel introduces zinc fume (causing metal fume fever acutely). Cadmium-plated surfaces generate cadmium fume — acutely lethal at high concentrations. Painted, primed, or coated steel can release lead, isocyanates, or phosgene (the last from chlorinated degreaser residues on the metal surface). Even short tacking operations on coated steel can produce dangerous exposures.
Gaseous Constituents
The arc generates ozone (from UV acting on atmospheric oxygen), nitrogen oxides, carbon monoxide, and carbon dioxide. Shielding gases — argon, helium, CO₂ — are simple asphyxiants that accumulate in low or enclosed areas.
Why the Welding Process Matters
SMAW (stick) and FCAW produce significantly more fume mass than GMAW (MIG) and GTAW (TIG). Stainless steel welding with chromium-containing filler generates Cr(VI) exposures that can cross the OSHA action level of 2.5 µg/m³ within minutes of arc-on time.
| Welding Process | Dominant Fume Constituents | Primary Governing Standard (US) | Key Health Endpoint |
|---|---|---|---|
| SMAW on mild steel | Iron oxide, manganese | 29 CFR 1910.1000 (Table Z-1) | Lung cancer (IARC Group 1), manganism |
| GMAW on stainless | Cr(VI), nickel, manganese | 29 CFR 1910.1026 | Lung cancer, kidney cancer, nasal cancer |
| FCAW on mild steel | Iron oxide, manganese, fluorides | 29 CFR 1910.1000 | Lung cancer, neurological effects |
| Any process on galvanised | Zinc oxide, base-metal fume | 29 CFR 1910.1000 | Metal fume fever (acute), plus base-metal risks |
| Any process on Cd-plated | Cadmium fume | 29 CFR 1910.1027 | Pulmonary oedema (acute), kidney damage, lung cancer |
Watch For: Mild-steel filler wire contains manganese — typically 0.9–1.4% in ER70S-6. The Racette et al. (2016) cohort study of 886 US welders observed progressive parkinsonian signs at an estimated mean exposure of 0.14 mg Mn/m³, well below the OSHA PEL of 5 mg/m³. Treating mild steel as “low risk” because the base metal looks benign ignores the filler’s neurological hazard.
The Hierarchy of Controls Applied to Welding Fume
Every HSE professional knows the hierarchy of controls. The challenge with welding fume is not knowing the hierarchy — it’s understanding where each real-world control actually sits and why regulators no longer accept the substitutions that most shops make.
Elimination and Substitution (The Under-Used Top Tier)
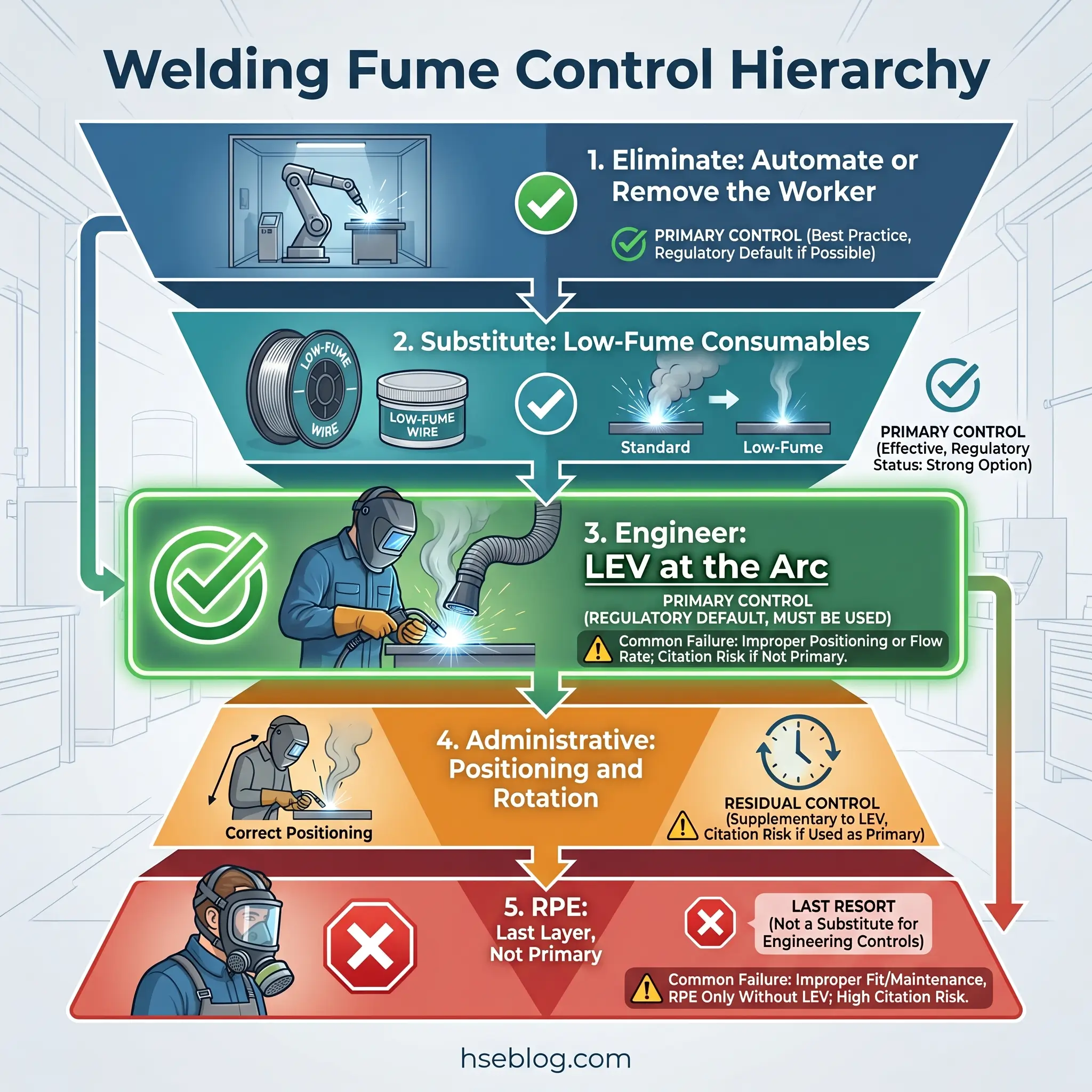
Elimination means removing the worker from the fume entirely. Robotic or automated welding achieves this for repetitive joints — the operator works outside the plume. Where automation is not feasible, process substitution offers measurable reductions: GMAW with optimised shielding gas produces less fume than SMAW where joint quality permits the switch. Low-fume and low-manganese consumables — such as ER70S-3 in place of ER70S-6 where mechanical requirements allow — reduce the manganese fraction at source.
These options are under-used because they require engineering involvement in welding procedure specifications (WPS), which on many sites is treated as outside the HSE function’s remit. The judgment call here is between accepting the existing process and engaging the welding engineer early. The balance favours engagement, because every percentage of fume reduced at source is a percentage the LEV system does not need to capture.
Engineering Controls: LEV as the Regulatory Default
Under both OSHA and HSE frameworks, engineering controls — primarily LEV — are the expected primary control for welding fume. HSE’s 2019 alert made this explicit: LEV is required for all indoor welding. OSHA’s position under 29 CFR 1910.1026 requires engineering controls as the primary compliance mechanism for Cr(VI), with RPE permitted only where engineering controls alone are demonstrably insufficient.
The recurring failure pattern at this tier: a site installs a capture-arm LEV system, but the hood is positioned more than one hood diameter from the arc, where capture velocity collapses. The equipment was specified correctly — the problem is that nobody trained the welder to reposition the hood as the work moves. A £15,000 LEV rig controls nothing at 18 inches when it was sized for 6.
Administrative Controls and Work Practices
Welder positioning — keeping the head out of the plume by working upwind or to the side of the arc — reduces personal exposure but does not satisfy the engineering-controls-first requirement. Arc-off time management, job rotation, and housekeeping (vacuum cleaning, not compressed air) are supplementary layers.
One critical regulatory point: OSHA does not permit job rotation to achieve compliance with the Cr(VI) PEL under 29 CFR 1910.1026. Rotation can reduce individual cumulative exposure for other constituents, but it cannot substitute for engineering controls where Cr(VI) is present.
Respiratory Protective Equipment (RPE) as Residual Control
RPE is the last layer under every major framework — OSHA 29 CFR 1910.134, HSE HSG53, and ANSI/AWS Z49.1:2021. Selection depends on the assigned protection factor (APF) needed: half-mask APF 10, full-face APF 50, powered air-purifying respirator (PAPR) APF 25 or 1000 depending on configuration, and supplied-air for high-exposure and confined-space work. A written RPE programme, annual fit testing for tight-fitting facepieces, medical clearance, and the clean-shaven rule for tight-fitting RPE are regulatory requirements, not best practices.
Audit Point: The most common inspection finding at this tier is a site relying on a PAPR welding helmet as the primary control while skipping LEV entirely. RPE fails when the seal fails, the filter expires, or the welder lifts the visor — and regulators treat it as a residual control, not a primary one.
Welding Fume Exposure Limits: OSHA vs HSE vs ACGIH vs NIOSH
No single competitor article synthesises the cross-jurisdictional exposure limits that actually govern welding fume control decisions. This table does.
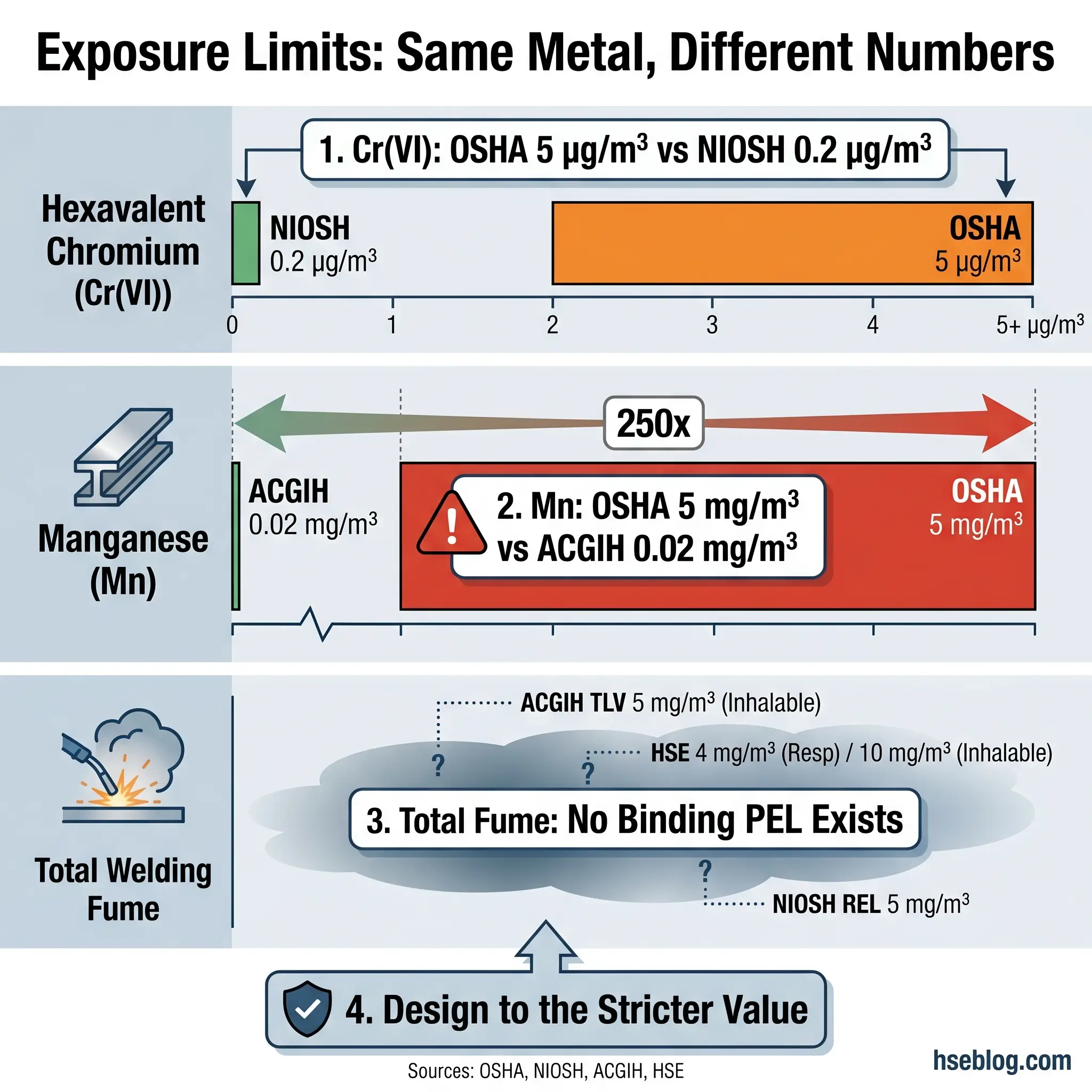
The practical consequence of conflicting standards: where OSHA, NIOSH, ACGIH, and HSE disagree on the same substance, the stricter value is the defensible design target — not the easier-to-meet legal minimum. HSE’s post-2019 position explicitly rejects the argument that “meeting the WEL is sufficient” because, for a carcinogen, there is no known safe level.
| Substance | OSHA PEL (US) | NIOSH REL (US) | ACGIH TLV | HSE/EU Position | Legal Status |
|---|---|---|---|---|---|
| Hexavalent Chromium (Cr VI) | 5 µg/m³ TWA (29 CFR 1910.1026, 2006) | 0.2 µg/m³ TWA | Follows NIOSH REL direction | WEL applies under COSHH carcinogen provisions; EU CMRD BOELV | OSHA PEL legally binding (US); NIOSH REL advisory; EU BOELV binding on member states |
| Manganese (inhalable) | 5 mg/m³ ceiling (legacy, 1970s) | 1 mg/m³ TWA | 0.02 mg/m³ inhalable; 0.1 mg/m³ respirable (2013) | ALARP under COSHH; effectively requires working below ACGIH where practicable | OSHA PEL legally binding but widely regarded as inadequate for neurological protection |
| Total Welding Fume | No dedicated PEL | No dedicated REL | Former 5 mg/m³ TLV withdrawn; PNOS ~3 mg/m³ as general guide | Carcinogen under COSHH — no safe level; ALARP | No binding limit in any jurisdiction specifically for “welding fume” as a category |
The OSHA hexavalent chromium PEL of 5 µg/m³ was itself a ten-fold reduction from the previous 52 µg/m³, enacted in 2006 (71 FR 10099). Even at 5 µg/m³, NIOSH considers residual cancer risk unacceptable and recommends 0.2 µg/m³. For manganese, the mismatch is starker: the OSHA PEL of 5 mg/m³ predates modern understanding of neurological endpoints entirely. The Racette et al. (2016) study documented progressive parkinsonism at exposures around 0.14 mg/m³ — 250 times below the OSHA PEL. ACGIH’s TLV of 0.02 mg/m³ inhalable, set in 2013, is designed for neurological protection and should be the reference for control design.
Jurisdiction Note: Exposure monitoring programmes frequently measure total fume mass and declare compliance with a 5 mg/m³ figure, while never speciating for Cr(VI) or Mn. The legally meaningful exposures never get measured. The competent-person check is: does your sampling strategy speciate for the metals your consumables actually contain?
Regulatory Requirements by Jurisdiction
Understanding which regulation applies is different from understanding what it requires you to do. This section translates obligations into practical requirements.
United States: OSHA Framework
The US regulatory structure for welding fume is not a single standard but a matrix of overlapping obligations:
- 29 CFR 1910 Subpart Q (general industry) and parallel 29 CFR 1926 Subpart J (construction) and 29 CFR 1915 Subpart D (shipyards) set baseline welding safety requirements including ventilation, fire prevention, and personnel protection.
- 29 CFR 1910.1026 (Cr(VI)) is the most stringent driver for stainless steel welding: exposure assessment, regulated areas, engineering-controls-first hierarchy, medical surveillance triggered at the 2.5 µg/m³ action level, and 30-year exposure record retention.
- 29 CFR 1910.134 requires a written respiratory protection programme with medical clearance, annual fit testing, training, and a designated programme administrator.
- 29 CFR 1910.1000 (Table Z-1) provides PELs for individual metal constituents, and 29 CFR 1910.1200 requires hazard communication including access to Safety Data Sheets for all consumables.
- 29 CFR 1910.146 governs permit-required confined spaces — directly applicable when welding inside tanks, vessels, and enclosed structures.
OSHA civil penalty maximums increased significantly in 2024, with serious violations reaching $16,131 per violation and willful or repeated violations exceeding $161,323 per violation (OSHA, 2024). Multi-standard citations on a single welding operation can accumulate rapidly.
United Kingdom: HSE Framework Post-2019
UK obligations flow from the Control of Substances Hazardous to Health (COSHH) Regulations 2002. Regulation 7(5) imposes stricter duties for carcinogens and mutagens — minimisation and enclosure where reasonably practicable. The 2019 enforcement change via HSE Safety Alert STSU1 – 2019(1) hardened this: general ventilation is not acceptable; LEV is required indoors; suitable RPE is required outdoors.
HSG258 is the LEV design, commissioning, and thorough-examination-and-test reference that HSE inspectors use as their benchmark. COSHH Regulation 9 requires LEV thorough examination and test at least every 14 months — a specific interval with no flexibility.
HSE continued targeted inspection campaigns on welding fume across UK fabricated-metals businesses through 2024–2026, building on the 2021 declaration exercise (HSE, 2021 onwards). Sites that received a declaration request and never acted remain a priority enforcement population.
European Union
The Carcinogens, Mutagens and Reprotoxic Substances Directive (2004/37/EC, as amended) sets binding occupational exposure limits for Cr(VI) and other welding-relevant carcinogens, plus the minimisation principle. The Chemical Agents Directive 98/24/EC governs non-carcinogenic substances like manganese. Each member state transposes through national regulations; EU limits are minima, and stricter national values apply where set.
International and Consensus Standards
ANSI/AWS Z49.1:2021 is the US consensus reference for welding safety — ventilation, fire prevention, PPE, and work practices. The ISO 21904 series covers LEV equipment for welding: design, testing, and marking. The ACGIH Industrial Ventilation Manual (31st edition, 2024) remains the global practical reference for LEV design, and the ILO provides welding safety guidance for jurisdictions without mature national frameworks.
The most common jurisdictional error in multi-site operations is writing a single global welding procedure against the weakest applicable standard. A procedure that satisfies OSHA 29 CFR 1910.1026 will not satisfy HSE’s post-2019 expectation, because HSE explicitly rejects the “de minimis duration” argument that OSHA’s standard implicitly permits.
Designing an Effective Local Exhaust Ventilation System for Welding
Specifying LEV for welding is where most control programmes succeed or fail — not on paper, but on the shop floor. The design logic matters more than the equipment catalogue.
Hood Selection Hierarchy
Not all LEV configurations perform equally, and the selection should follow a practical capture-effectiveness ranking:
- On-gun extraction — stays with the arc as the welder moves; best sustained capture for GMAW/FCAW. Airflow must balance extraction against shielding gas disruption; manufacturers publish airflow ranges for each gun model.
- Movable capture arm (snorkel) — effective when positioned within the manufacturer’s stated capture distance. Requires welder discipline to reposition as the work moves.
- Fixed hood — suitable for repetitive work with a stationary arc position.
- Enclosing booth — contains the fume but requires adequate make-up air.
- Downdraft table — effective for small parts; struggles with large assemblies.
- Dilution ventilation — rarely sufficient alone under current regulatory expectations.
Capture Velocity and the Distance Problem
Per the ACGIH Industrial Ventilation Manual (31st edition, 2024), welding typically requires approximately 100–150 fpm capture velocity in moderately still air. The critical physics: for an unflanged hood, required volume flow scales with the square of distance. Doubling the hood-to-arc distance requires roughly four times the airflow to maintain the same capture velocity.
Cross-drafts compound the problem. ACGIH notes that cross-drafts can reduce hood performance by up to 75%. Open bay doors, overhead radiant heaters, HVAC supply diffusers, and adjacent process equipment all generate cross-drafts that defeat otherwise well-specified LEV. Site layout assessment is part of LEV design — not an afterthought.
Recirculation and Discharge Rules
OSHA permits recirculation of filtered welding air only where the air-cleaning system provides continuous, reliable collection and specific monitoring/bypass provisions are met. On the discharge side, EPA NESHAP restricts outdoor exhaust where the fume contains cadmium, chromium, lead, or nickel at ≥ 0.1% or manganese at ≥ 1% by weight.
Under COSHH Regulation 9 (UK), LEV requires thorough examination and test at least every 14 months. OSHA does not specify an interval, but 29 CFR 1910.94 and 1910.1026 require demonstrable effectiveness — most well-managed US sites follow annual or semi-annual testing.
Field Test: Walk behind the welder during arc-on time. If you can smell the fume or see a visible plume drifting past the hood, the capture velocity at the arc is insufficient — regardless of what the design specification says.
Controlling Welding Fume in Confined Spaces
Confined-space welding is where fatalities and severe exposures cluster. It warrants treatment as a distinct control problem, not a footnote.
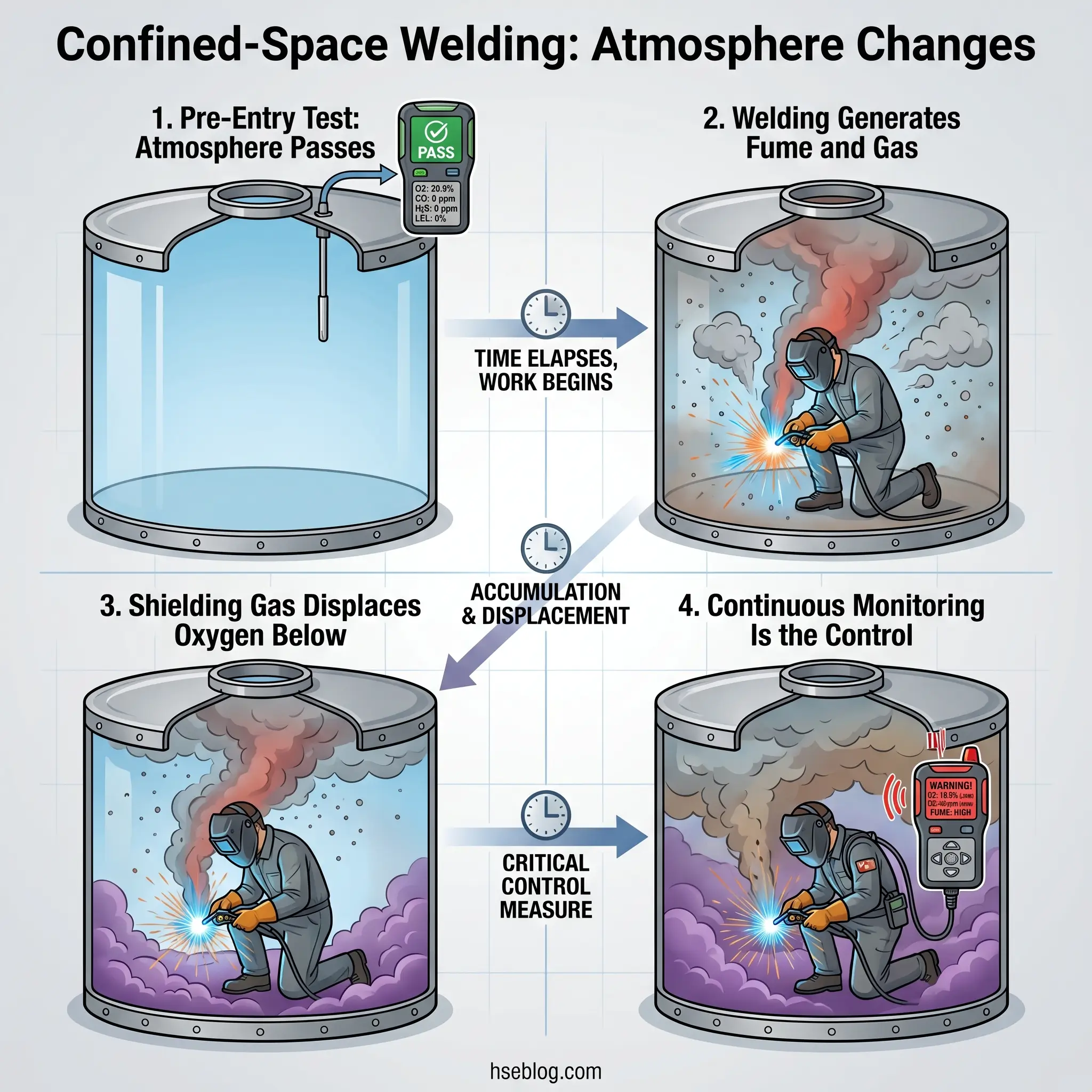
Welding inside tanks, vessels, pipework, or enclosed structures triggers permit-required confined space rules — OSHA 29 CFR 1910.146 in the US, the Confined Spaces Regulations 1997 in the UK. Dilution ventilation alone is not sufficient for hot work in confined spaces. The minimum expectation is LEV positioned close to the arc plus continuous atmospheric monitoring for oxygen, combustibles, carbon monoxide, and nitrogen dioxide.
Shielding gases — argon, helium, CO₂ — are simple asphyxiants that accumulate in low points within enclosed structures. Supplied-air respiratory protection is typically required when engineering controls cannot reduce exposure below the applicable PEL or WEL. The AIHA reference point of 20 air changes per hour is often cited as a practical ventilation target for confined-space welding, though the actual requirement depends on the space geometry, welding process, and atmospheric monitoring results.
A qualified or competent person — a qualified person per OSHA 29 CFR 1910.146, or a competent person per COSHH in the UK — must conduct the risk assessment and specify controls for each confined-space welding task individually.
Watch For: The compounding factor in confined-space welding incidents is rarely a single control failure. Pre-entry atmospheric testing passes. Welding begins. Manganese fume and NO₂ accumulate. The atmosphere is no longer the one that was tested — and continuous monitoring was not set up because “the entry permit said it passed.” The control that fails is always the one that was not planned as continuous.
Health Surveillance and Exposure Monitoring
Engineering controls mean nothing if no one verifies they’re working. The measurement and surveillance programme is the feedback loop that closes the control system.
Exposure Monitoring
Personal breathing-zone sampling is the defensible measurement basis for welding fume. Area sampling supplements but does not replace it — the welder’s exposure is determined by what reaches the breathing zone, not what a wall-mounted monitor detects three metres away.
Analytical methods matter. NIOSH Method 7300/7303 (ICP analysis) is the standard reference for metals; NIOSH Method 7600/7605 is used for Cr(VI) speciation. The sampling strategy must be driven by the Safety Data Sheets of the consumables in use — which metals the filler, electrode, and flux actually contain determines which analytes the laboratory must test for.
Programmes frequently sample only a “typical” shift and miss the high-exposure tasks: tack welding on galvanised steel, grinding stainless welds, welding in a pit or tank, or hot work on painted surfaces. Worst-case task sampling is what defends the control programme during enforcement — average-shift results do not.
Health Surveillance
Under 29 CFR 1910.1026 (US), medical surveillance is required for workers exposed at or above the Cr(VI) action level for 30 or more days per year. Under COSHH (UK), health surveillance is required wherever exposure is likely to produce an adverse health effect — and for carcinogenic fume, HSE expects it as a default.
HSE advises spirometry for welders and periodic respiratory questionnaires. The design and interpretation of any health surveillance programme must be led by an occupational health professional — this is not a function an HSE manager should attempt to self-administer. Referral to NIOSH guidance on welding fumes and manganese provides a solid clinical reference for programme design.
Building a Welding Fume Control Programme: Practical Checklist
The programmes that survive inspections are not the ones with the most paperwork. They’re the ones where the documented controls match what is happening on the shop floor during an unannounced walk. The single most common finding is a current risk assessment referencing control measures no one on site can demonstrate in use.
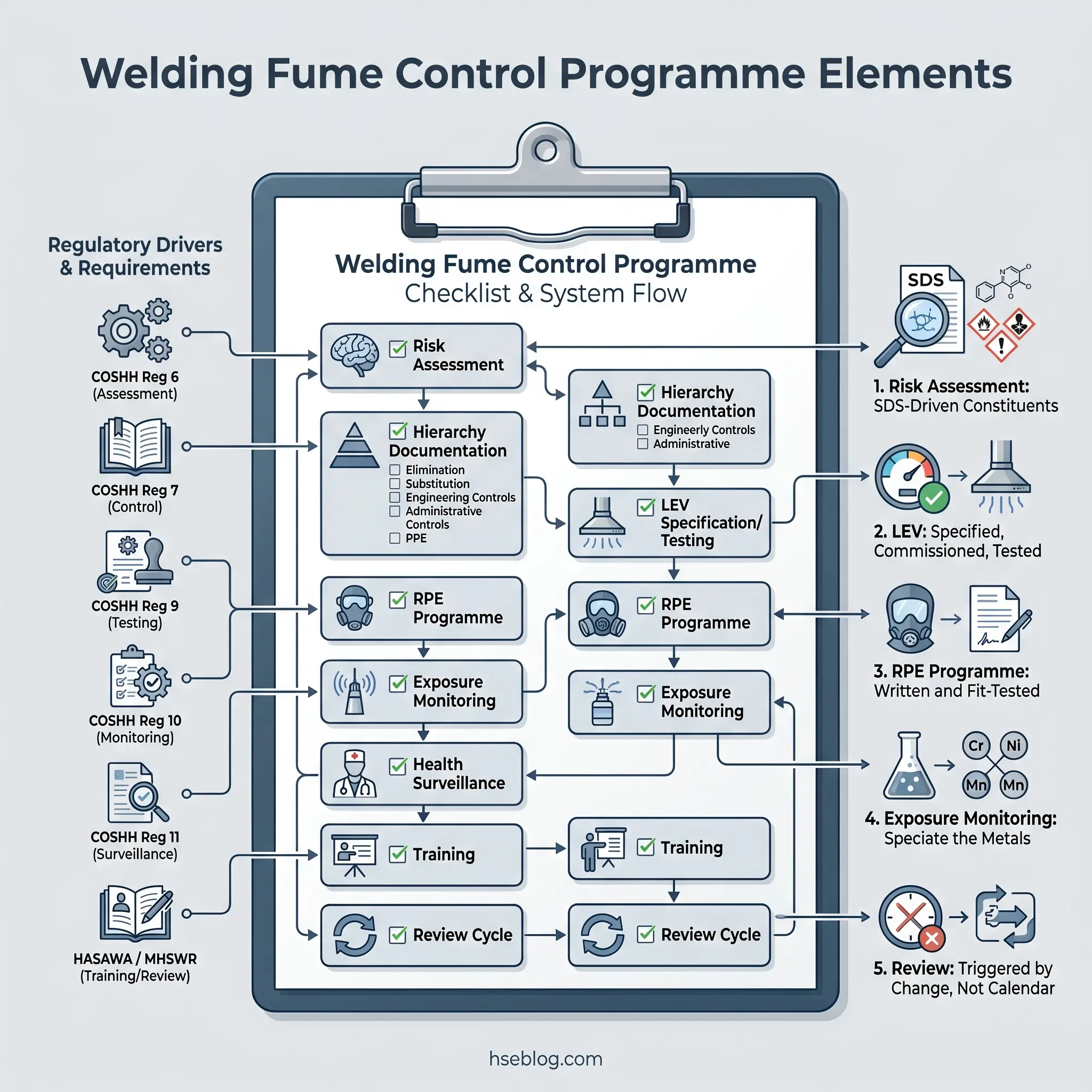
Each programme element below maps to the regulatory driver that requires it:
- Written exposure assessment / risk assessment with process-specific constituent identification based on consumable SDS data — required under COSHH Regulation 6 (UK), 29 CFR 1910.1026(d) (US, for Cr(VI)).
- Documented control hierarchy decisions with justification for each deviation from a higher-tier control — the defensible record for an inspector’s “why not LEV?” question.
- LEV specification, commissioning, user training, and scheduled examination/test — UK: at least every 14 months per COSHH Regulation 9; US: on a defensible schedule demonstrating ongoing effectiveness.
- Written RPE programme with fit-testing, medical clearance, training, maintenance, and cartridge/filter change schedules — 29 CFR 1910.134 (US), HSG53 (UK).
- Exposure monitoring plan with a sampling strategy that speciates for the metals in your consumables, defines sampling frequency, and identifies re-sampling triggers (new consumable, new process, new work location).
- Health surveillance co-designed with an occupational health professional — not self-administered.
- Training records covering welders, supervisors, and bystanders — who is exposed, what controls are in place, how to use them, and what symptoms to report.
- Review cycle tied to process changes, new consumables, new base metals, or regulatory updates — not an arbitrary annual date disconnected from operations.
Frequently Asked Questions
Conclusion
The single biggest lesson the welding industry continues to learn the hard way is that “we’ve always done it this way” is not a control strategy — and since 2017, it is not a defensible one. IARC’s Group 1 reclassification and HSE’s 2019 enforcement response fundamentally changed what constitutes adequate welding fume control. The sites that still operate under a pre-2019 control posture are not sites with an unusual risk tolerance; they are sites where nobody updated the risk assessment.
The highest-impact change any facility can make is not purchasing better equipment — it is aligning the sampling strategy with the consumables actually in use. A programme that measures total fume mass and ignores Cr(VI) and manganese speciation is measuring the wrong thing. The legally meaningful exposures are the ones no one tests for, and the control programme that has never been tested against them has never been validated.
Welding fume control is not a paperwork exercise. It is the difference between a workforce that retires with their neurological function intact and one that does not. The controls exist. The standards are published. The question for every site is whether what is written in the risk assessment matches what is happening under the welding hood right now.