

TL;DR
- Match equipment to hazard type first — personal air sampling pumps with laboratory analysis remain the standard for formal compliance; direct-reading instruments serve screening and real-time awareness but rarely satisfy regulatory compliance requirements on their own.
- Personal beats area — breathing-zone sampling is required for compliance determinations under both OSHA and COSHH; area monitoring alone cannot demonstrate that individual workers are protected.
- Calibration makes or breaks your data — pre- and post-sampling pump calibration within ±5% drift tolerance is non-negotiable; skipping post-calibration invalidates samples after they’ve already been collected.
- Biological monitoring fills the gaps — for skin-notated substances, mixed-route exposures, and RPE-dependent work, air monitoring alone cannot capture total body burden.
- Use the most protective limit — OSHA PELs for many substances have not been updated since 1971; ACGIH TLVs and NIOSH RELs reflect current health science and should be the operational benchmark.
Workplace exposure monitoring is the systematic measurement of worker exposure to chemical, physical, and biological hazards using calibrated sampling equipment and validated analytical techniques. It serves three purposes: verifying regulatory compliance against occupational exposure limits (OELs), confirming that engineering controls are performing as designed, and characterizing baseline health risk. Equipment ranges from personal air sampling pumps with laboratory-analyzed media to direct-reading instruments providing real-time data, with selection driven by hazard type, monitoring purpose, and jurisdictional requirements.
What Is Workplace Exposure Monitoring and Why Does It Matter?
Approximately 13,000 workers die each year in the UK alone from diseases caused by exposure to chemicals or dusts at work (HSE UK, ongoing estimate). In the EU, occupational cancer accounts for over 100,000 deaths annually (ETUI/WHO/ILO, 2022). These are not sudden catastrophic events — they are slow-onset diseases caused by exposures that accumulated over years, often because no one measured what workers were actually breathing.
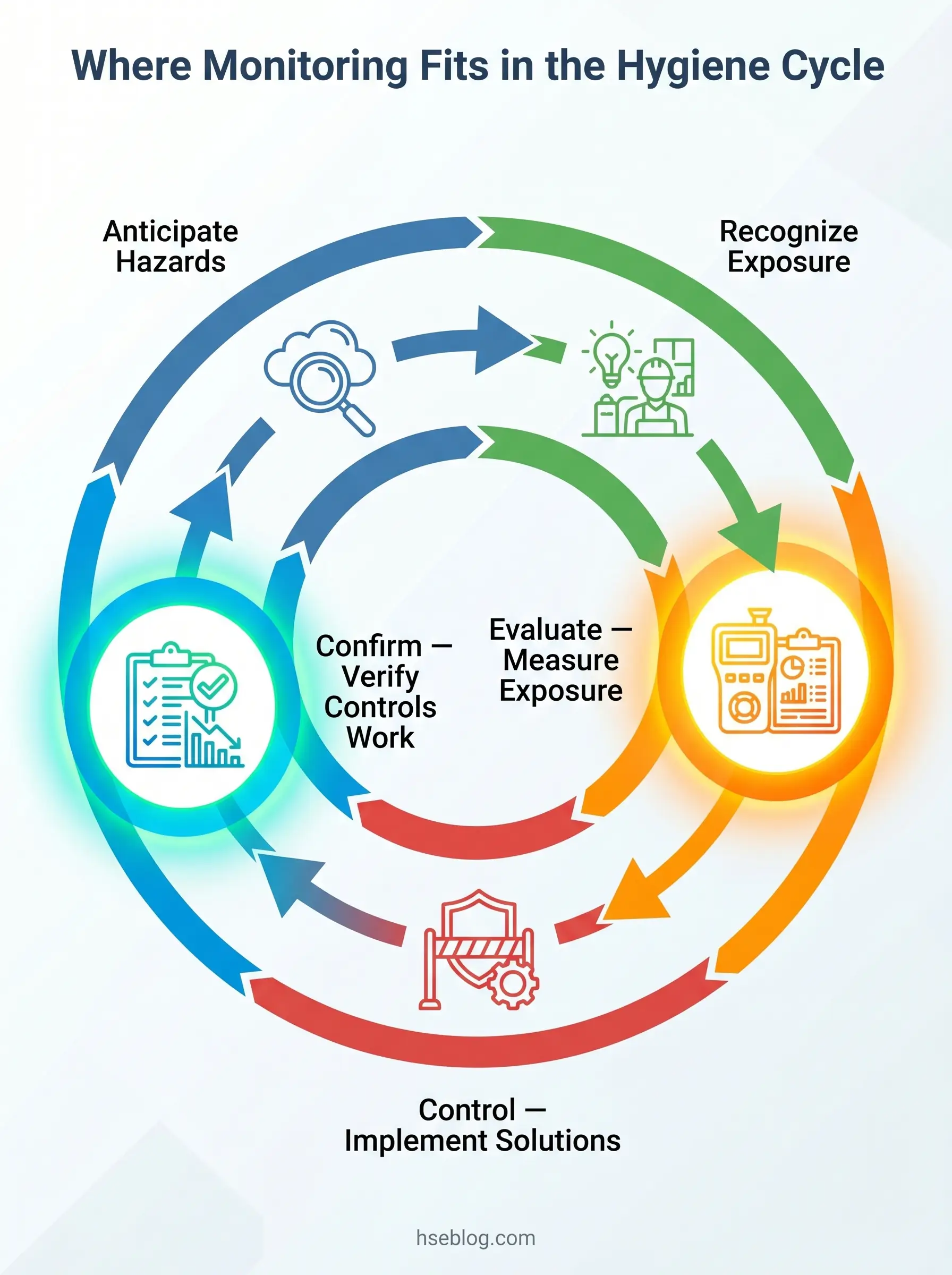
Workplace exposure monitoring is the systematic process of measuring the concentration of hazardous agents in a worker’s breathing zone or work environment, then comparing those measurements against established occupational exposure limits. It is distinct from environmental monitoring, which measures ambient outdoor air quality, and from biological monitoring, which measures substances or metabolites within the worker’s body. Exposure monitoring sits within the broader industrial hygiene cycle — Anticipate, Recognize, Evaluate, Control, Confirm — as the primary tool for the “Evaluate” and “Confirm” stages.
The purpose extends beyond checking a regulatory box. Monitoring answers three operational questions: Are we compliant with the applicable exposure limit? Are the controls we installed actually reducing exposure to acceptable levels? And what is the baseline risk profile for this workforce, this process, this substance?
Several overlapping regulatory frameworks govern what must be measured, how, and against which limits. In the US, OSHA establishes legally enforceable Permissible Exposure Limits (PELs) under 29 CFR 1910.1000 and substance-specific standards. In Great Britain, the Control of Substances Hazardous to Health Regulations (COSHH) require monitoring under Regulation 10 where there is a risk of workplace exposure limits (WELs) being exceeded, as published in EH40/2005. The EU sets Binding Occupational Exposure Limits (BOELs) under the Carcinogens, Mutagens, and Reprotoxic Substances Directive (CMRD — Directive 2004/37/EC as amended through Directive (EU) 2024/869). ACGIH publishes Threshold Limit Values (TLVs) and NIOSH publishes Recommended Exposure Limits (RELs) — neither is legally enforceable, but both reflect more current health science than many decades-old OSHA PELs.
| Framework | Jurisdiction | Legal Status | Basis |
|---|---|---|---|
| OSHA PEL | US | Legally enforceable | Regulatory (many unchanged since 1971) |
| NIOSH REL | US | Recommended | Health-based, regularly updated |
| ACGIH TLV | International | Advisory guideline | Health-based, annually reviewed |
| UK WEL | Great Britain | Legally enforceable under COSHH | Health-based with feasibility consideration |
| EU BOEL | EU Member States | Binding minimum, transposed nationally | Health-based under CMRD |
A persistent failure mode across industries: teams treat monitoring as a one-off compliance exercise. Controls get installed, an initial monitoring round shows acceptable results, and no one re-verifies. Exposure conditions change — ventilation degrades, process parameters shift, maintenance windows get extended — but monitoring stays frozen in the baseline report.
Types of Workplace Hazards That Require Exposure Monitoring
Before selecting any monitoring equipment, the hazard must be identified and classified. Each hazard category demands fundamentally different sampling media, analytical methods, and instrumentation — measuring noise with an air sampling pump is obviously impossible, but subtler mismatches are far more common and equally destructive to data quality.
Chemical Agents
Chemical hazards subdivide by physical state, and each state determines the sampling approach:
- Gases and vapors — substances that exist in gaseous form at ambient temperature and pressure (carbon monoxide, hydrogen sulfide, solvent vapors). Captured using sorbent tubes, passive badges, or detected with direct-reading instruments such as PIDs and electrochemical sensors.
- Respirable dust — particles small enough to penetrate the gas-exchange region of the lungs (below approximately 4 μm aerodynamic diameter). Collected using cyclone-equipped sampling heads. This is the fraction relevant to silicosis and coal workers’ pneumoconiosis.
- Inhalable dust — the fraction that enters the nose and mouth (up to approximately 100 μm). Collected using IOM or conical inhalable samplers. Relevant for substances with upper-airway or systemic toxicity.
- Fumes — solid particles formed by condensation from the gaseous state, typically from welding or metal processing. Collected on membrane filters.
- Mists — liquid aerosols generated by spraying, machining with metalworking fluids, or condensation processes.
- Fibers — asbestos, man-made mineral fibers, ceramic fibers. Collected on membrane filters, analyzed by phase contrast microscopy (PCM) or transmission electron microscopy (TEM).
The most costly monitoring errors occur when the wrong hazard fraction is measured. Measuring total inhalable dust when the applicable WEL or PEL refers to the respirable fraction produces a number that is analytically correct but regulatory meaningless. Approximately 2.3 million workers in the US are potentially exposed to respirable crystalline silica (OSHA, 2016) — and every one of those exposure assessments must use a respirable-fraction sampler with a validated cyclone, not a total dust cassette.
Physical Agents
- Noise — measured using noise dosimeters (personal) or integrating sound level meters (area). OSHA 29 CFR 1910.95 requires a monitoring program when any employee’s exposure may equal or exceed 85 dBA as an 8-hour TWA.
- Vibration — hand-arm vibration (HAV) and whole-body vibration (WBV) measured with accelerometers mounted per ISO 5349 and ISO 2631 respectively.
- Heat stress — assessed using Wet Bulb Globe Temperature (WBGT) meters, combining dry bulb, wet bulb, and globe temperature.
- Radiation — ionizing radiation monitored with dosimeters (TLD, OSL); non-ionizing radiation (RF, UV, laser) with field-strength meters and spectroradiometers.
Biological Agents
Bioaerosol sampling uses impaction samplers, impingers, or cassette-based collection for bacteria, fungi, and viruses. Analysis is culture-based or molecular (PCR). This is the least standardized area of exposure monitoring, with no universally agreed OELs for most biological agents.
Routes of Exposure
Inhalation is the primary route that air monitoring captures. But substances with a “skin” notation in OSHA, ACGIH, or COSHH lists — isocyanates, organophosphate pesticides, some solvents — absorb through the skin, meaning air monitoring alone underestimates total body burden. Ingestion exposure (hand-to-mouth transfer of surface contamination) further complicates the picture. Recognizing these routes before designing a monitoring program prevents collecting data that answers the wrong question.
What Are the Main Types of Exposure Monitoring Equipment?
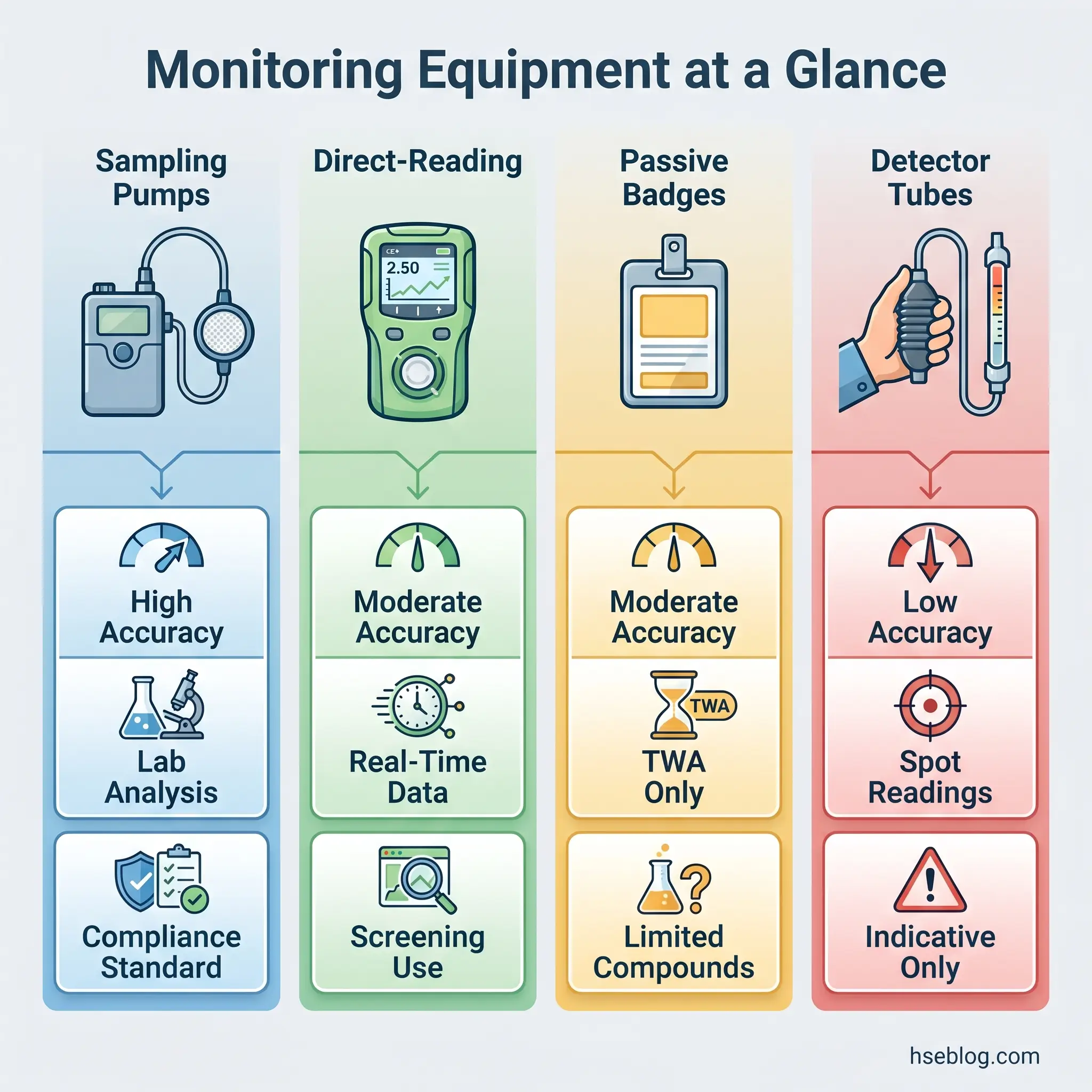
The equipment landscape divides into three broad categories based on how samples are collected and analyzed. Each serves different monitoring purposes, and confusing their roles is a reliable source of bad data and worse decisions.
Personal Air Sampling Pumps and Media
The personal air sampling pump paired with appropriate collection media is the backbone of regulatory compliance monitoring worldwide. The principle is straightforward: a calibrated, battery-powered pump draws a known volume of air through a collection medium positioned in the worker’s breathing zone (within 30 cm of the nose and mouth, typically clipped to the lapel). After sampling, the medium goes to an accredited laboratory for analysis.
Collection media selection depends entirely on the target analyte:
- Filter cassettes — 37 mm or 25 mm cassettes with membrane filters (PVC, MCE, PTFE, glass fiber) for particulates, metals, asbestos fibers, crystalline silica.
- Sorbent tubes — glass tubes packed with activated charcoal, silica gel, Tenax, or XAD-2 for organic vapors and gases. The analyte adsorbs onto the sorbent, then is desorbed in the lab (solvent desorption or thermal desorption).
- Impingers and bubblers — air bubbled through a liquid reagent for reactive compounds, aldehydes, or high-humidity situations where sorbent tubes underperform.
- Canister-based whole-air samplers — evacuated canisters (SUMMA, MiniCan) that collect a whole-air sample for laboratory GC-MS analysis, particularly useful for complex VOC mixtures at low concentrations.
The NIOSH Manual of Analytical Methods (NMAM) provides validated methods specifying exactly which media, flow rate, sample volume, and analytical technique to use for each substance. Using the wrong method — the wrong sorbent for a particular solvent, the wrong filter substrate for a metal — produces results that no laboratory accreditation can salvage.
Flow rates must be calibrated before and after each sampling period using a primary standard such as a soap-bubble meter or electronic mass-flow calibrator. Acceptable drift tolerance is typically ±5%. Exceeding this invalidates the sample.
Direct-Reading Instruments
Direct-reading instruments (DRIs) provide real-time concentration data without laboratory analysis. They are indispensable for screening surveys, emergency response, confined-space entry, and identifying exposure-driving tasks — but their role in formal compliance monitoring is limited.
Key instrument types include:
- Photoionization detectors (PIDs) — detect volatile organic compounds by ionizing them with UV light. Broad-spectrum but non-specific; a PID reading tells you total VOC concentration, not which compounds are present. Response factors vary by compound.
- Flame ionization detectors (FIDs) — detect organic compounds through hydrogen flame ionization. More uniform response across hydrocarbons than PIDs but less portable.
- Electrochemical gas sensors — substance-specific sensors for common toxic gases (CO, H₂S, NO₂, SO₂, Cl₂). Used in multi-gas monitors. Cross-sensitivity between gases is a documented limitation.
- Infrared analyzers (NDIR) — detect gases by infrared absorption. Used for CO₂, methane, and specific compounds with characteristic IR absorption spectra.
- Real-time aerosol monitors — photometric instruments (such as the TSI DustTrak or pDR series) that estimate particulate concentration by light scattering. Useful for trending and source identification but require gravimetric correction factors for regulatory comparison, because the optical response varies with particle size, shape, and refractive index.
OSHA provides detailed guidance on direct-reading instruments through its DRI program, covering proper operation, calibration protocols, and appropriate applications. The critical practitioner understanding: DRIs excel at answering “is there a problem?” and “where is the source?” They are generally unsuitable for answering “are we in compliance?” — because the validated accuracy required for compliance determinations comes from laboratory-analyzed samples collected by methods published in NMAM or equivalent references.
Some regulatory frameworks do specify DRIs: OSHA’s confined-space standard (29 CFR 1910.146) requires direct-reading atmospheric testing before entry. In those specific contexts, DRIs are not just acceptable — they are mandatory.
Passive and Diffusive Samplers
Passive samplers — commonly called badges — collect airborne contaminants by molecular diffusion across a defined path length without a pump. The driving force is the concentration gradient between the ambient air and the collection medium inside the badge.
Available types cover organic vapors (charcoal-based), formaldehyde (treated filter), ethylene oxide, mercury vapor, nitrous oxide, and a growing list of specific compounds. Their advantages are significant: no pump noise, no tubing, lightweight, no flow calibration required, and minimal interference with the worker’s tasks.
Limitations are equally real. Sensitivity is lower than active sampling at equivalent durations. Performance degrades at low air velocities (stagnant conditions), high humidity, and temperature extremes. The range of validated compounds is narrower than for sorbent-tube methods. For low-concentration monitoring — such as benzene below the new EU BOEL — diffusive sampler validation data must be scrutinized carefully.
Watch For: Passive samplers assume a stable diffusion coefficient. In environments with intermittent high-concentration bursts followed by clean periods, the time-weighted average may be captured accurately, but the peak-exposure profile is invisible. If STEL compliance is the question, passive samplers cannot answer it.
Colorimetric Detector Tubes
Glass tubes packed with chemical reagent that changes color proportionally to the concentration of a specific gas or vapor. The worker breaks the tube ends, inserts it into a bellows or piston pump, draws a calibrated volume of air through, and reads the concentration from the graduated scale.
They provide a rapid, low-cost indicative measurement — useful for spot checks, leak investigation, and situations where a quick yes/no answer is needed before committing to full analytical sampling. Accuracy is typically ±25% to ±35%, which makes them unsuitable for compliance determinations but adequate for screening purposes. ANSI/ISEA 102 provides performance requirements for these devices.
Personal Monitoring vs. Area Monitoring: When to Use Each Approach
A personal sampling pump clipped to a worker’s belt with the sampling head in the breathing zone measures what that individual actually inhales during a shift. A static area monitor positioned at a fixed point — on a tripod, mounted on a wall, placed on a workbench — measures the ambient concentration at that location. These are not interchangeable measurements, and treating them as such is one of the most persistent errors in occupational hygiene practice.
OSHA’s substance-specific standards and COSHH both require personal breathing-zone sampling for compliance determinations. The PEL and the WEL apply to what the worker breathes, not what the room measures. Area monitors placed at workstation level consistently underestimate peak breathing-zone concentrations during active tasks — grinding, pouring, spraying, decanting — and overestimate exposure during idle periods when the worker has moved away from the source.
Area monitoring has legitimate applications. It is valuable for verifying ventilation performance, identifying emission sources, tracking temporal concentration trends, and characterizing process contributions. When a local exhaust ventilation system is installed, area monitors upstream and downstream of the hood can confirm capture efficiency far more precisely than personal sampling alone. The distinction is operational purpose: area monitoring tells you about the environment; personal monitoring tells you about the worker.
| Characteristic | Personal Monitoring | Area Monitoring |
|---|---|---|
| Measures | Worker breathing-zone concentration | Fixed-point ambient concentration |
| Regulatory acceptance | Required for PEL/WEL compliance | Supplementary; not accepted for compliance |
| Best use | Exposure determination, SEG characterization | Source ID, ventilation verification, trending |
| Limitation | Resource-intensive per worker | Does not represent individual exposure |
Similar Exposure Groups
Monitoring every worker on every shift is rarely practical. The similar exposure group (SEG) concept makes monitoring programs feasible without sacrificing statistical validity. An SEG is a group of workers whose exposure profiles are sufficiently similar — based on job classification, tasks performed, proximity to emission sources, and exposure controls — that monitoring a representative subset characterizes the group.
Forming SEGs requires judgment. Workers with the same job title but different tasks, or the same tasks but different ventilation conditions, do not belong in the same SEG. The AIHA exposure assessment strategy provides a structured approach: define SEGs based on qualitative assessment, then validate with quantitative data. If monitoring results within an SEG show high variability (geometric standard deviation exceeding approximately 2.5–3.0), the group is likely not homogeneous and needs to be subdivided.
Audit Point: Regulators and auditors test SEG assignments by examining the qualitative basis and the statistical homogeneity of available data. A SEG defined solely by job title without task-level analysis rarely survives scrutiny.
Sampling Strategies and Monitoring Techniques
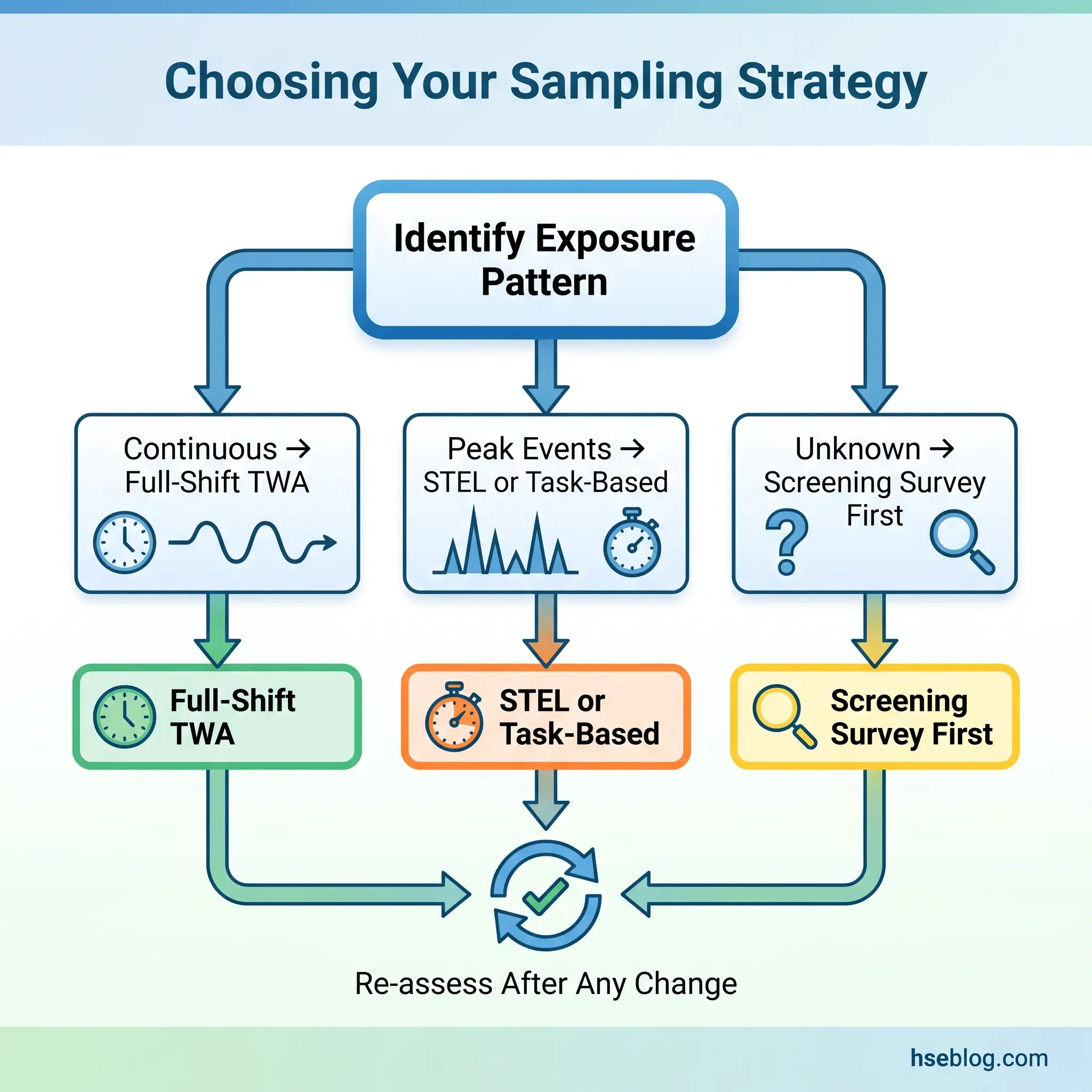
Equipment selection determines what you can measure. Sampling strategy determines whether the data answers the question you actually need answered. A perfectly calibrated pump collecting a full-shift sample answers the 8-hour TWA question — but if the hazard is a 20-minute task that generates peak concentrations an order of magnitude above the shift average, that TWA result will dilute the exposure into apparent compliance and mask a genuinely dangerous condition.
Full-Shift TWA Monitoring
The standard approach for chronic exposure assessment. The sampler runs for the entire work shift (typically 7–8 hours of sampling time within an 8-hour period), capturing the time-weighted average concentration. The result is compared directly against the 8-hour TWA PEL or WEL.
Full-shift monitoring is appropriate when exposure is relatively continuous throughout the shift — process operators in chemical manufacturing, workers in steady-state production environments, office workers with continuous low-level exposures.
Short-Term Exposure Limit (STEL) Monitoring
STEL monitoring captures peak exposure episodes. The sampling period is 15 minutes, timed to coincide with the anticipated period of highest exposure. Many substances have STELs in addition to 8-hour TWAs — for example, ACGIH publishes STELs for irritants and fast-acting toxicants where the 15-minute ceiling matters more than the shift average.
The challenge is timing. The sampler must be running during the actual peak, which requires advance knowledge of the work cycle. In practice, this means shadowing the worker through the task and activating sampling at the right moment — or using a direct-reading instrument to identify when peaks occur, then targeting STEL sampling to those windows.
Task-Based Monitoring
This is the most underutilized technique in routine monitoring programs. Many exposure profiles are dominated by a single short-duration task — a 30-minute grinding operation, a batch-charging event, a spray-painting cycle. Default full-shift TWA monitoring dilutes these peaks and produces misleadingly low averages.
Task-based sampling isolates the specific activity. The pump runs only during the task, and the result is reported as a task-specific concentration and duration. This data directly informs whether task-specific controls are needed and whether worker rotation, ventilation modification, or RPE upgrade should be applied to that activity.
Monitoring Frequency and Triggers
How often monitoring occurs depends on jurisdiction and exposure level. OSHA’s substance-specific standards generally follow two models:
- Performance option — the employer conducts an initial determination of employee exposure. If exposure is below the action level (typically 50% of PEL), periodic monitoring can be discontinued with documentation.
- Scheduled monitoring option — monitoring at defined intervals (every 3 or 6 months depending on the standard) until two consecutive results below the action level are achieved.
Under COSHH, monitoring is required at intervals appropriate to the risk, and always when controls change. The legal requirement under Regulation 10 to keep monitoring records for 5 years (40 years for substances causing identifiable diseases) means the data trail must be defensible over decades.
Regardless of jurisdiction, any change in process, materials, work practices, or engineering controls should trigger reassessment. This is the point most organizations miss: the monitoring program is not a fixed schedule but a living protocol tied to operational reality.
Biological Monitoring as a Complementary Technique
Content covering biological monitoring and biological exposure indices is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms or exposure concerns should consult an occupational physician or qualified medical professional.
Air monitoring measures what is in the breathing zone. Biological monitoring measures what has actually entered the body — by analyzing blood, urine, or exhaled air for the parent substance, its metabolites, or a biological effect indicator. The two approaches answer different questions, and in several critical scenarios, biological monitoring is the only method that captures the full exposure picture.
Biological monitoring is most valuable precisely where air monitoring is least reliable. Substances with a skin notation — isocyanates, organophosphate pesticides, certain glycol ethers — absorb through intact skin, meaning a worker can receive a significant dose even when air concentrations are well below the OEL. Workers who rely on respiratory protective equipment (RPE) as their primary control present another gap: the air monitor outside the facepiece measures ambient concentration, not what penetrates the seal. Only biological monitoring can confirm whether the RPE is actually protecting the worker.
Several regulatory frameworks mandate biological monitoring for specific substances:
- Lead — OSHA (29 CFR 1910.1025) requires blood lead level monitoring for workers exposed above the action level. COSHH and EU CMRD similarly mandate blood lead surveillance. The EU Directive (EU) 2024/869 reduced the biological limit value for lead, with tighter thresholds taking effect across member states.
- Cadmium — OSHA requires both blood cadmium and urine beta-2-microglobulin monitoring.
- Mercury — urine mercury is the standard biological marker, with ACGIH BEI at 35 μg/g creatinine.
- Organic solvents — urine metabolite analysis (e.g., mandelic acid for styrene, hippuric acid for toluene).
Reference values come from three primary sources: ACGIH Biological Exposure Indices (BEIs), HSE UK Biological Monitoring Guidance Values (BMGVs) published in EH40/2005, and German BAT/EKA values. Sampling timing is critical — most biological markers have a defined sampling window relative to the exposure period (end-of-shift, end-of-workweek, or pre-shift for accumulated substances), and samples collected outside this window are uninterpretable.
| Substance | Biological Marker | BEI / BMGV | Sampling Time |
|---|---|---|---|
| Lead (inorganic) | Blood lead | 20 μg/dL (ACGIH BEI) | Not critical (long half-life) |
| Mercury (inorganic) | Urine mercury | 35 μg/g creatinine (ACGIH BEI) | Pre-shift |
| Toluene | Urine o-cresol | 0.3 mg/L (ACGIH BEI) | End of shift |
| Styrene | Urine mandelic acid | 400 mg/g creatinine (ACGIH BEI) | End of shift |
Calibration, Quality Assurance, and Common Sources of Error
Every piece of monitoring data rests on a chain of technical steps, each of which can introduce error. Calibration and quality assurance are not administrative formalities — they are the difference between data that can defend a compliance determination in court and data that gets thrown out.
Pump Calibration Protocol
The calibration workflow follows a strict sequence. Before sampling, the pump is connected to the sampling media (the exact media that will be used, in the same configuration) and calibrated against a primary standard — a soap-bubble meter, electronic mass-flow calibrator (DryCal, Gilibrator), or equivalent traceable device. The target flow rate is set per the applicable NIOSH or OSHA method (e.g., NIOSH 7500 for silica specifies 1.7 L/min through a 10 mm nylon cyclone).
After the sampling period ends, the pump is calibrated again with the exposed media still in place. If the post-sampling flow rate has drifted more than ±5% from the pre-sampling rate, the sample is invalidated. The average of pre- and post-calibration flow rates, multiplied by sampling duration, gives the total air volume — the denominator in every concentration calculation.
Post-sampling calibration is the step most frequently skipped. In practice, teams pull the sampling media, cap the cassettes, and send them to the lab before checking whether the pump held its flow rate. When the laboratory reports a concentration, there is no way to know whether the volume calculation — and therefore the result — is accurate. The sample is analytically processed but scientifically useless.
Field and Media Blanks
Quality assurance requires blank samples. A field blank is an unopened sampling medium that travels with the field samples through the entire process — transported to the site, handled alongside active samples, and returned to the laboratory for analysis. It detects contamination introduced during transport and handling. A media blank stays in the laboratory to verify that the unused media is clean. Without blanks, any positive result could be an artifact of contamination rather than actual workplace exposure.
Laboratory Accreditation
Samples should be analyzed by laboratories accredited to ISO/IEC 17025, with specific accreditation for the analytes and methods in question. In the US, AIHA Laboratory Accreditation Programs (AIHA-LAP, formerly ELLAP and PAT) provide accreditation specifically for industrial hygiene laboratories. Using a non-accredited laboratory does not necessarily invalidate results, but it significantly weakens their defensibility in enforcement actions or litigation.
Common Error Sources
Recurring errors that undermine monitoring data quality, drawn from published quality assurance literature and audit findings:
- Incorrect flow rate — the most consequential single error, directly affecting the calculated concentration
- Wrong media for the analyte — using activated charcoal when silica gel is specified, or using the wrong filter substrate
- Cassette orientation — open-face versus closed-face configuration matters; the wrong orientation changes the particle-size selection characteristics
- Sampling head placement — the cassette must be in the breathing zone; clipping it to the waist or chest does not satisfy breathing-zone requirements
- Environmental interference on DRIs — humidity, temperature, and cross-reactive gases produce false readings; PID readings in high-humidity environments can be significantly suppressed
- Broken chain of custody — samples that cannot be traced from collection through analysis lack evidentiary value
Field Test: Before deploying for a monitoring campaign, run a calibration check, verify media lot numbers against the method, confirm cassette orientation, and photograph the sampling setup on the worker. Documentation costs minutes; a lost or invalidated sample costs the entire campaign.
Interpreting Monitoring Results and Comparing Against Exposure Limits
Raw laboratory results arrive as mass of analyte collected on the sampling medium. Converting this to an airborne concentration requires the total air volume sampled — which is why calibration accuracy controls everything downstream.
TWA Calculation
The formula is fundamental:
Concentration (mg/m³) = Mass collected (mg) ÷ Volume of air sampled (m³)
For gases and vapors reported in ppm:
Concentration (ppm) = (mg/m³ × 24.45) ÷ Molecular weight
The calculated TWA is then compared against the applicable OEL. But which OEL? For many substances, the OSHA PEL, NIOSH REL, and ACGIH TLV specify different values. The OSHA Annotated PEL Tables provide a side-by-side comparison of OSHA PELs, NIOSH RELs, Cal/OSHA PELs, and ACGIH TLVs — a resource that makes the discrepancies immediately visible.
The Conflicting-Standards Problem
OSHA’s PEL tables (29 CFR 1910.1000, Tables Z-1, Z-2, and Z-3) were last comprehensively updated in 1971. For many substances, the PEL reflects toxicological understanding from the 1960s. NIOSH RELs and ACGIH TLVs are regularly updated based on current epidemiological and toxicological evidence.
The practical consequence: a monitoring result can be below the legally enforceable PEL while exceeding the health-based TLV by a significant margin. For benzene, OSHA’s PEL is 1 ppm (8-hour TWA), while the ACGIH TLV is 0.5 ppm. For crystalline silica, the OSHA PEL is 50 μg/m³ (post-2016 revision), while the ACGIH TLV is 25 μg/m³.
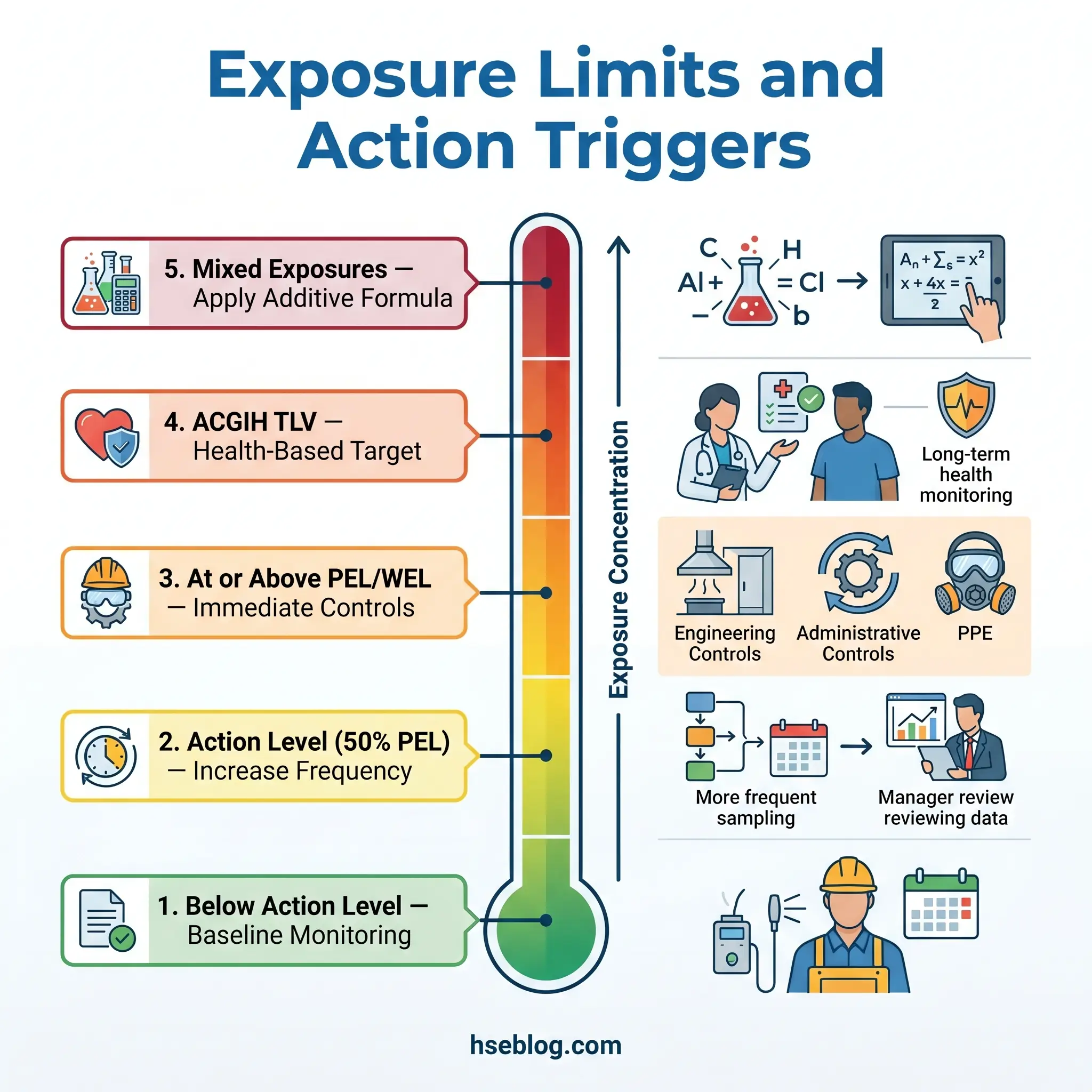
The judgment call for practitioners: compliance with the PEL satisfies the minimum legal requirement, but using the more protective TLV or REL as the operational target aligns with current health science. Many organizations adopt the most protective published limit as their internal standard — not because they are legally required to, but because the health evidence supports it and litigation risk increasingly references the health-based limits.
Mixed-Exposure Calculations
When workers are exposed to multiple substances with similar toxicological effects, the additive formula applies:
Em = C₁/L₁ + C₂/L₂ + … + Cₙ/Lₙ
If Em ≥ 1.0, the combined exposure exceeds the applicable limit, even though individual concentrations may each be below their respective OELs. This calculation is required under 29 CFR 1910.1000(d)(2)(i) and is implicit in COSHH assessments for mixed exposures. It is frequently overlooked.
Action Levels
Many OSHA substance-specific standards establish an action level, typically set at 50% of the PEL. Results above the action level trigger increased monitoring frequency and, in some standards, initiation of medical surveillance. The action level is not a “safe” threshold — it is a management trigger designed to catch upward exposure trends before the PEL is reached.
Jurisdiction Note: In the UK under COSHH, there is no formal “action level” concept equivalent to OSHA’s. The WEL itself is the control target, and employers must reduce exposure as far as reasonably practicable — not merely to the WEL. This means UK-based monitoring programs should interpret any detectable exposure as a trigger for reviewing control adequacy, not just results approaching the WEL.
Emerging Technologies and Future Trends in Exposure Monitoring
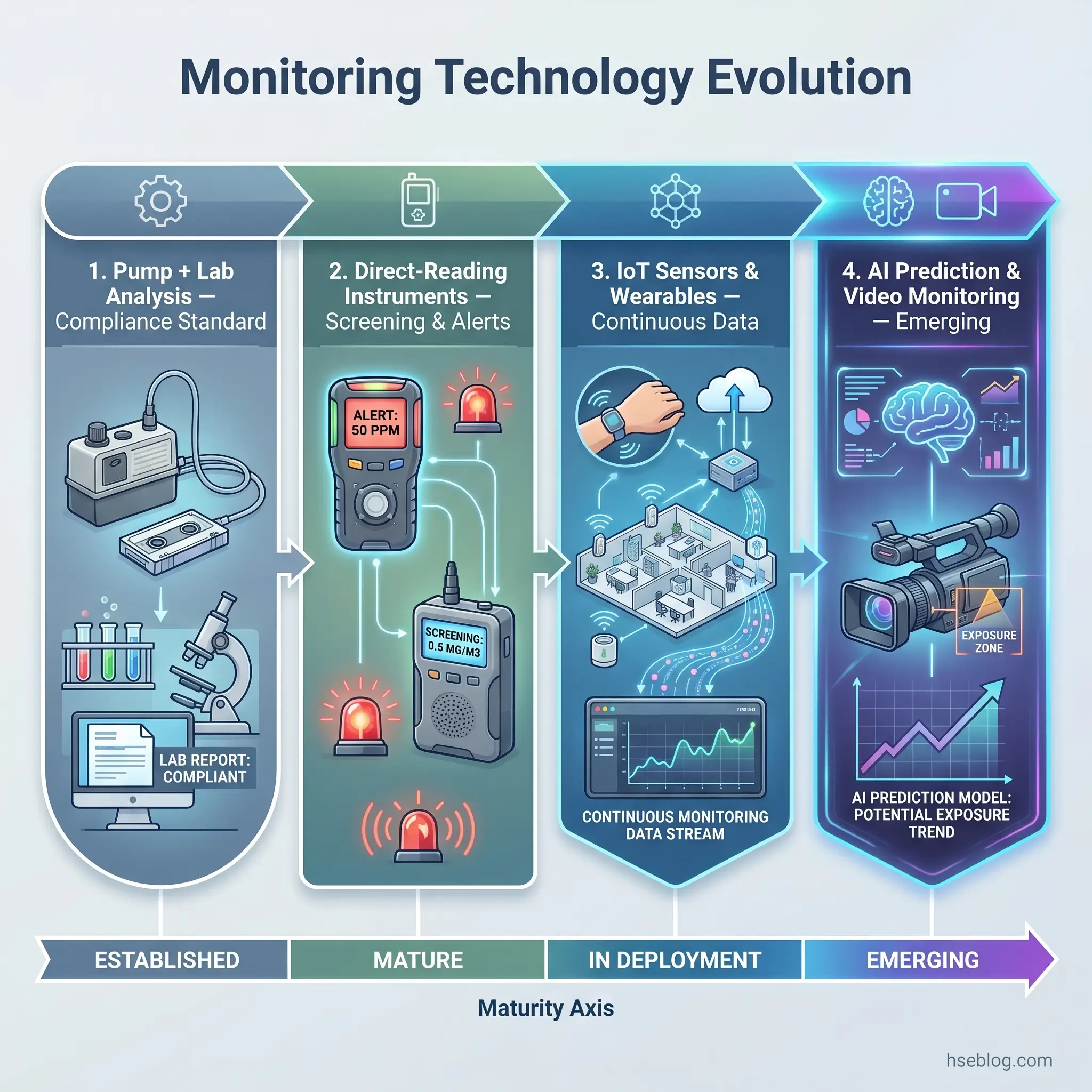
The monitoring equipment landscape is shifting toward continuous, connected, and data-rich approaches. Some developments are already in commercial deployment; others remain in research. The distinction matters for practitioners making purchasing and program-design decisions today.
Real-Time Wireless Sensor Networks
IoT-enabled area monitoring networks deploy multiple direct-reading sensors across a facility, transmitting continuous concentration data to cloud-based dashboards. These systems provide temporal and spatial resolution that periodic grab sampling cannot match — identifying concentration spikes, drift patterns, and source contributions in real time. Their value is operational control and early warning, not compliance documentation.
Wearable Personal Monitors
Compact, Bluetooth-enabled personal monitors are entering the market for gases (VOCs, CO, H₂S), noise, and particulates. They promise continuous personal exposure data with minimal worker burden. The practical question is analytical reliability: how do these devices perform against the validated reference methods over extended shifts, across temperature and humidity ranges, and with the calibration stability that compliance data demands? For most substances, the answer is “not yet equivalent” — but for trending, alerting, and supplementing traditional campaigns, they are increasingly useful.
Video Exposure Monitoring
Video exposure monitoring (VEM) synchronizes real-time instrument readings with video footage of the worker performing tasks. The result is a frame-by-frame correlation of concentration with activity — exposing exactly which movements, positions, or process steps drive exposure peaks. NIOSH has published guidance on VEM methodology. It transforms monitoring from a statistical exercise into a visual diagnostic tool, directly informing control design by showing where and why exposures occur.
AI-Driven Exposure Assessment
Machine learning models are being applied to exposure prediction — using historical monitoring data, job descriptions, process parameters, and environmental variables to predict exposures for unmonitored workers or unmeasured tasks. This is particularly relevant for SEG assignment, where AI can analyze patterns across large datasets to identify exposure groupings that human judgment might miss.
Regulatory Freshness: 2024–2026 Developments
Two regulatory developments are actively reshaping monitoring equipment requirements. The EU adopted Directive (EU) 2024/869, reducing the binding OEL for lead from 0.15 to 0.03 mg/m³ and establishing new limits for diisocyanates at 6 μg NCO/m³ (effective January 2029). These tighter limits demand higher-sensitivity monitoring methods and more frequent biological monitoring for lead across EU member states.
In the mining sector, MSHA published its final rule in April 2024 lowering the silica PEL for all mines to 50 μg/m³ with a 25 μg/m³ action level, requiring ISO-compliant sampling devices and accredited laboratories. While enforcement for coal mines was stayed by the Eighth Circuit Court of Appeals in April 2025, the compliance deadline for metal/nonmetal mining of April 2026 remains in effect (MSHA via J.J. Keller Consulting, 2024–2026), driving demand for upgraded monitoring equipment capable of reliably quantifying silica at lower concentrations.
Practitioners should be cautious about treating data from emerging sensor technologies as equivalent to validated NIOSH or OSHA analytical methods for compliance purposes. The technology is powerful for trending, alerting, and operational decision-making. Formal compliance determinations still require validated sampling and laboratory analysis in most jurisdictions — and this is unlikely to change until the regulatory frameworks themselves are updated to accept real-time sensor data.
Frequently Asked Questions
Conclusion
The pattern that consistently undermines monitoring programs is not equipment failure or laboratory error — it is the disconnect between collecting data and using it to drive decisions. Organizations that invest in calibrated equipment, validated methods, and accredited laboratory analysis but then file the reports without acting on marginal results are spending resources on compliance documentation rather than worker protection. The 2.5 million nonfatal workplace injuries and illnesses reported in 2024 (US Bureau of Labor Statistics, 2026) — while the lowest since 2003 — still represent a burden that effective monitoring programs, properly designed and acted upon, are built to reduce.
The single highest-impact improvement most monitoring programs can make is shifting from default full-shift TWA sampling toward hazard-appropriate strategy selection. Task-based sampling for short-duration high-exposure activities, STEL monitoring timed to peak events, biological monitoring for skin-notated substances — these methods capture the exposures that matter most but are most easily diluted by routine full-shift averaging.
Workplace exposure monitoring is not a measurement exercise. It is a decision tool. The equipment, techniques, calibration protocols, and interpretive frameworks described here exist for one purpose: to produce data reliable enough to answer the question that matters — are the people doing this work protected, or aren’t they?