

TL;DR
- If your workplace generates airborne contaminants (dust, fumes, vapours, gases) through any work activity, then you have a legal obligation under OSHA 29 CFR 1910.1000 (US) or COSHH Regulations 2002 (GB) to assess and monitor worker exposure — not a suggestion, a requirement.
- If you are monitoring CO2, PM2.5, and TVOCs in an office for comfort or certification purposes, then you are conducting indoor environmental quality monitoring — which does not satisfy occupational exposure monitoring obligations for hazardous substances.
- If your monitoring results show exposures at or just below the Permissible Exposure Limit or Workplace Exposure Limit, then that is not a pass — both OSHA and HSE expect employers to reduce exposure further, as low as reasonably practicable.
- If you rely on consumer-grade air quality sensors for regulatory compliance evidence, then your monitoring data will not withstand enforcement scrutiny — compliance monitoring requires validated methods, calibrated instruments, and accredited laboratory analysis.
Workplace air quality monitoring is the systematic measurement of airborne contaminants and environmental conditions in work environments to protect worker health and ensure regulatory compliance. It encompasses both occupational exposure monitoring — measuring personal exposure to hazardous substances against legal limits such as OSHA PELs (US) or HSE WELs (GB) — and indoor environmental quality monitoring for comfort, productivity, and building certification programmes like WELL v2 and LEED.
What Is Workplace Air Quality Monitoring and Why Does It Matter?
An estimated 12,000 people die each year in the UK from lung diseases linked to past occupational dust exposure (HSE/IOSH, 2024). That figure represents exposures that occurred years or decades ago — under monitoring regimes that were either inadequate or absent entirely. Every one of those deaths traces back to air that someone breathed at work, air that should have been measured, evaluated, and controlled.
Workplace air quality monitoring matters because airborne contaminants are the primary route of occupational illness, and the damage they cause is often irreversible by the time symptoms appear. The US EPA estimates that indoor pollutant levels can be 2 to 5 times higher than outdoor levels (EPA, ongoing), and the average person spends roughly 90% of their time indoors (EPA, ongoing). For workers in industrial, manufacturing, and even commercial environments, the air they breathe during a shift is not a background condition — it is an occupational hazard that demands the same systematic assessment as any other workplace risk.
What makes this topic uniquely prone to confusion is that two distinct disciplines operate under the same umbrella term. Occupational exposure monitoring measures a specific worker’s personal exposure to identified hazardous substances — using calibrated sampling equipment in the breathing zone, against legally enforceable limits (OSHA PELs in the US, HSE WELs in Great Britain). This is a regulatory compliance obligation triggered by hazard assessment. Indoor environmental quality (IEQ) monitoring, by contrast, tracks general parameters like CO2, PM2.5, total volatile organic compounds (TVOCs), temperature, and humidity — primarily for ventilation adequacy, occupant comfort, cognitive performance, and building certification programmes such as WELL v2 or LEED.
The convergence of these two disciplines is accelerating. Post-pandemic awareness, wildfire smoke infiltration events (particularly the 2023 Canadian wildfire season, which pushed PM2.5 to hazardous levels across much of North America), and the growth of building performance certifications have moved general IAQ monitoring firmly into employer consciousness. The International WELL Building Institute launched the WELL Operations Rating in January 2026, a data-driven building performance standard where indoor air quality comprises the largest feature category — 9 of 33 features (IWBI, 2026). ASHRAE published Standard 62.1-2025, refining humidity control and adding emergency ventilation provisions (ANSI/ASHRAE, 2025).
A failure pattern I consistently observe across organisations is the assumption that installing consumer-grade IAQ sensors in an office lobby satisfies their COSHH or OSHA monitoring obligations. It does not. These are different regulatory requirements demanding different instruments, different sampling strategies, and different professional competencies. Conflating them creates a compliance gap that looks like diligence on the surface but collapses under regulatory scrutiny.

Key Workplace Air Pollutants and What to Measure
The scope of what to monitor should never be dictated by what sensors happen to ship in a kit. It must be driven by a hazard assessment — a COSHH assessment under GB law, or a workplace hazard assessment under OSHA — that identifies which airborne substances the work activity actually generates.
That said, workplace air pollutants fall broadly into categories that span both industrial and commercial environments. Understanding these categories is essential for designing a monitoring programme that measures the right things for the right reasons.
Particulate matter covers a range of airborne solids and liquid droplets classified by size. PM2.5 (particles ≤2.5 micrometres) and PM10 (≤10 µm) are general IAQ metrics relevant to every indoor environment. In industrial settings, the relevant fractions are respirable dust and inhalable dust — with specific substances like respirable crystalline silica, asbestos fibres, and lead dust carrying their own dedicated OSHA standards and HSE WELs with mandated monitoring triggers.
Volatile organic compounds (VOCs) include hundreds of individual chemicals. In office environments, TVOCs originate from furniture off-gassing, cleaning products, and building materials. In industrial settings, specific VOCs such as benzene, toluene, and formaldehyde arise from solvents, coatings, and adhesives — each with substance-specific PELs and WELs that require individual measurement, not just a bulk TVOC number.
Carbon dioxide serves as a universal ventilation adequacy indicator. At typical office concentrations (400–1,500 ppm), it is not a toxicant — its value lies in signalling whether enough outdoor air is being supplied. Research from the Harvard T.H. Chan School of Public Health has associated CO2 levels above 1,000 ppm with measurable declines in cognitive performance, making it a productivity metric as much as a health one.
Carbon monoxide, nitrogen dioxide, sulfur dioxide, and ozone enter workplaces through combustion processes, vehicle exhaust infiltration, welding, and outdoor air intake. Each has specific occupational exposure limits.
Biological contaminants — mould spores, bacteria, and airborne pathogens — became a heightened concern post-COVID and remain relevant for facilities with HVAC systems that can harbour microbial growth.
Substance-Specific Versus General IAQ Parameters
The regulatory distinction is critical. Substances like silica, lead, asbestos, formaldehyde, and hexavalent chromium have dedicated OSHA substance-specific expanded health standards — each with mandated exposure monitoring triggers, action levels, medical surveillance requirements, and specific analytical methods. These are not optional monitoring decisions. When the work activity involves these substances, the monitoring obligation is automatic.
General IAQ parameters — CO2, temperature, relative humidity, bulk TVOCs — sit under ventilation standards and guidelines (ASHRAE 62.1-2025, WELL v2) rather than substance-specific health regulations. Monitoring them is best practice for occupant comfort and productivity, but it is not a substitute for the substance-specific monitoring that hazardous work activities legally require.
Watch For: The biggest monitoring error in practice is measuring only what a sensor kit happens to include rather than what the work activity actually generates. A COSHH assessment or OSHA hazard assessment should drive monitoring scope — not the equipment catalogue.
Regulatory Standards and Exposure Limits for Workplace Air Quality
Navigating workplace air quality regulations requires constant awareness of which jurisdiction’s limits apply. Conflating US, GB, and international frameworks is the most common compliance error in multi-site organisations — and in competitor guidance documents that omit jurisdiction labels entirely.
United States — OSHA
The primary enforcement mechanism is 29 CFR 1910.1000, which establishes Permissible Exposure Limits (PELs) through Tables Z-1, Z-2, and Z-3 as 8-hour time-weighted averages (TWAs), ceiling values, and peak exposure limits. Beyond PELs, OSHA enforces substance-specific expanded health standards for high-hazard substances (lead, asbestos, silica, benzene, formaldehyde, and others) with more protective limits and mandated monitoring schedules. Where no specific standard exists — as with general IAQ — OSHA relies on the General Duty Clause, OSH Act Section 5(a)(1), which requires employers to furnish a workplace free from recognised hazards likely to cause death or serious physical harm. OSHA’s indoor air quality guidance applies this clause to IAQ complaints.
United States — NIOSH and ACGIH
The National Institute for Occupational Safety and Health publishes Recommended Exposure Limits (RELs), which are not legally binding but represent more current health-based science than most OSHA PELs. The American Conference of Governmental Industrial Hygienists publishes Threshold Limit Values (TLVs) — health-based recommendations updated annually, required on Safety Data Sheets, and widely referenced by occupational hygienists. Neither RELs nor TLVs carry the force of law, but they represent the standard of professional practice.
Great Britain — COSHH and EH40
The Control of Substances Hazardous to Health Regulations 2002, enforced with legally binding Workplace Exposure Limits (WELs) published in EH40/2005 (4th Edition, 2020, with 2023 amendments). WELs are expressed as 8-hour TWAs (Long-Term Exposure Limits) and 15-minute Short-Term Exposure Limits. For carcinogens, mutagens, and asthmagens, HSE requires exposure reduction to as low as reasonably practicable (ALARP), regardless of whether the WEL is met.
International: The WHO Global Air Quality Guidelines 2021 tightened the annual PM2.5 guideline from 10 µg/m³ to 5 µg/m³ (WHO, 2021), reflecting evidence that health effects occur at lower concentrations than previously assumed. These are ambient air guidelines, not occupational limits, but they are increasingly referenced as indoor benchmarks by building certification programmes and progressive employers.
Ventilation: ASHRAE Standard 62.1-2025 specifies minimum ventilation rates and defines acceptable indoor air quality. The 2025 edition adds humidity control requirements, including maximum dew-point temperatures, and provisions for emergency ventilation during atypical operating modes (ANSI/ASHRAE, 2025). It is not an occupational health regulation, but it is adopted by building codes and referenced by OSHA in IAQ enforcement.
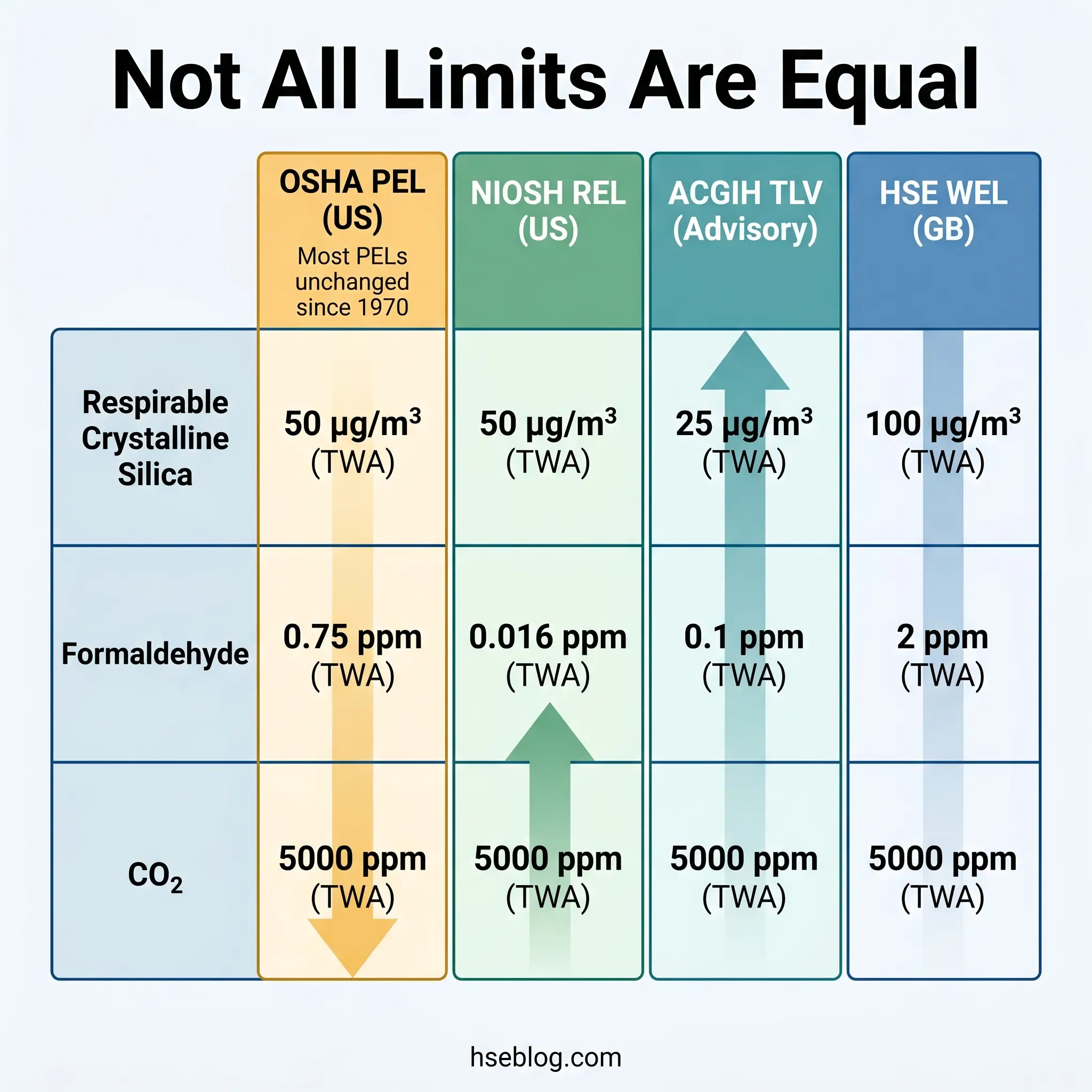
The OSHA PEL Problem: Why Outdated Limits Require Professional Judgment
Most OSHA PELs were adopted directly from 1968 ACGIH TLV values and have not been substantively updated since. OSHA itself acknowledges this — its annotated PEL comparison tables place PELs alongside NIOSH RELs and current ACGIH TLVs, explicitly directing employers to consider these more protective benchmarks.
The practical consequence for monitoring strategy is significant. Measuring against OSHA PELs alone and declaring compliance when exposures fall below them is technically legal but professionally inadequate. A competent occupational hygienist will reference NIOSH RELs or ACGIH TLVs as the health-protective benchmark and recommend controls accordingly. When the ACGIH TLV for respirable crystalline silica sits at 25 µg/m³ while the OSHA PEL allows 50 µg/m³, the judgment call is clear: the more protective limit better reflects current toxicological evidence.
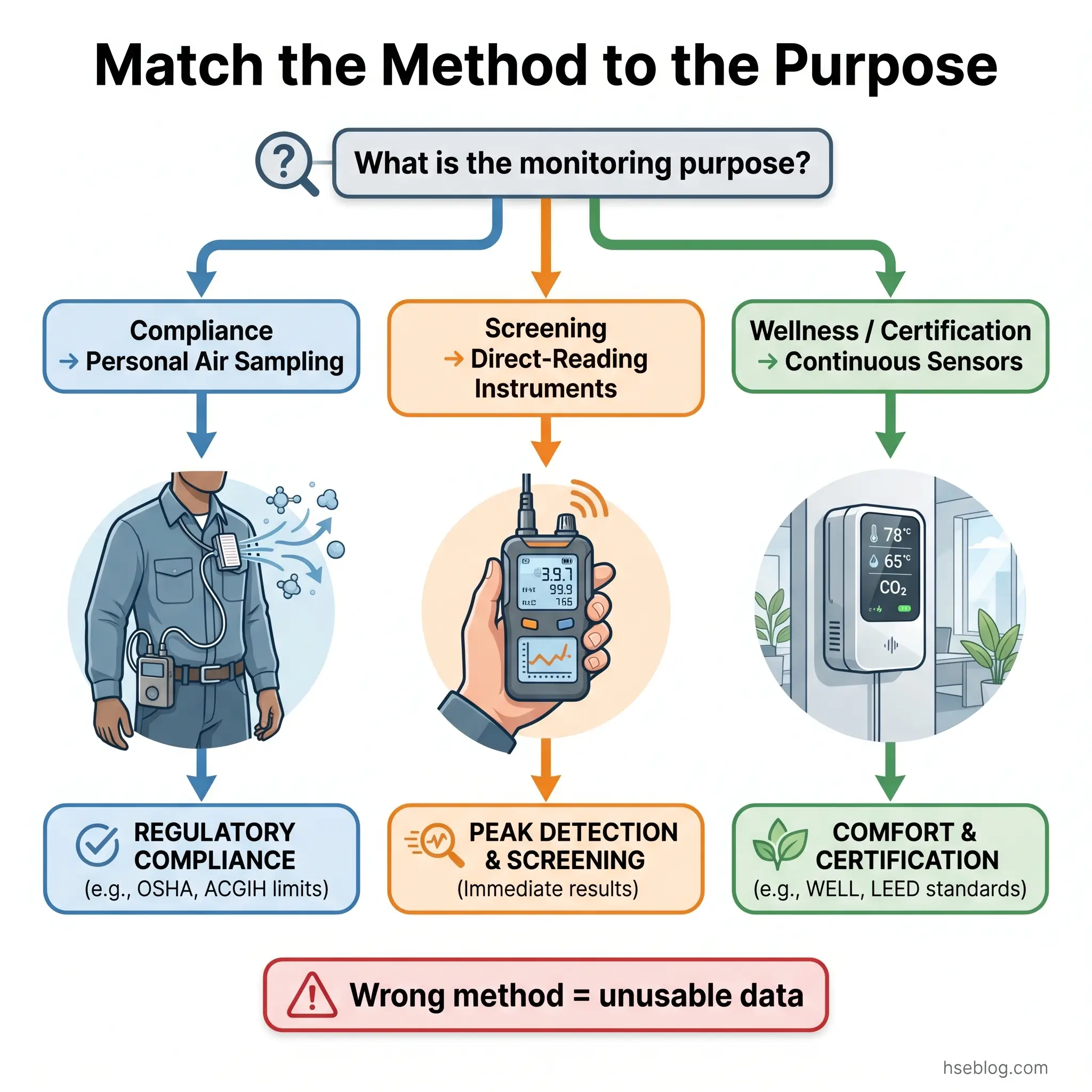
How Is Workplace Air Quality Monitored? Methods and Equipment
The method used to monitor air quality determines whether the results can answer a compliance question, a comfort question, or a certification question — and these are not interchangeable.
Personal air sampling remains the regulatory gold standard for demonstrating compliance with PELs and WELs. A calibrated air sampling pump draws workplace air through a filter cassette or sorbent tube positioned in the worker’s breathing zone for a representative period (typically a full shift for 8-hour TWA measurement). The collected sample is sent to an AIHA-accredited laboratory for gravimetric, chemical, or microscopic analysis. The method is validated, legally defensible, and specific to the substance of concern. Its limitation is that it provides a single time-weighted result after the fact — it tells you what the exposure was, not what it is right now.
Direct-reading instruments provide real-time data for screening, supplementary assessment, and emergency response. Photoionisation detectors (PIDs) measure total VOC concentrations; electrochemical sensors detect specific gases (CO, NO2, H2S); optical particle counters and light-scattering nephelometers give instantaneous particulate readings. These instruments are invaluable for identifying exposure patterns, peak events, and spatial variation — but most are not validated as standalone compliance tools for PEL/WEL assessment. They complement, rather than replace, laboratory-analysed sampling.
Continuous IAQ monitoring systems use networks of fixed sensors measuring CO2, PM2.5, TVOCs, temperature, and humidity at representative locations throughout a building. Data feeds into building management systems or dedicated dashboards. This is the monitoring method driving WELL v2 certification, RESET Air verification, and corporate wellness programmes. The WELL v2 Performance Verification Guidebook specifies sensor density, placement, and calibration requirements for certification credit.
The following comparison captures the trade-offs practitioners must evaluate when designing a monitoring programme:
| Factor | Personal Air Sampling | Direct-Reading Instruments | Continuous IAQ Monitoring |
|---|---|---|---|
| Primary use | Regulatory compliance (PEL/WEL) | Screening, peak detection, emergency | Comfort, wellness, certification |
| Data type | Time-weighted average per sample | Real-time instantaneous readings | Continuous trend data |
| Accuracy | High (validated analytical methods) | Moderate (cross-sensitivity, drift) | Variable (sensor-dependent) |
| Cost per event | High (lab fees, hygienist time) | Moderate (instrument cost, calibration) | Low per data point (high initial setup) |
| Regulatory acceptance | Full — the compliance standard | Supplementary only for most substances | Not accepted for PEL/WEL compliance |
Audit Point: When monitoring results may determine whether an employer faces enforcement action, three things matter above all else: the instrument’s documented accuracy specification, its calibration record, and the sampling method’s validation status against a recognised standard (NIOSH Manual of Analytical Methods, HSE MDHS series). Consumer-grade sensors meet none of these requirements.
The shift toward continuous monitoring is welcome for data richness and operational awareness. But it creates a new failure mode: organisations deploy networked sensors, generate dashboards full of green indicators, and assume compliance is demonstrated. A dashboard showing CO2 at 650 ppm and PM2.5 at 8 µg/m³ tells you the ventilation system is performing adequately for general occupant comfort. It tells you nothing about a maintenance worker’s personal exposure to isocyanates during a spray-painting task two floors below.
What Are Acceptable Air Quality Levels in the Workplace?
This is the question most readers arrive with, and the honest answer is: it depends entirely on which standard you are monitoring against and why. The gap between occupational toxicity thresholds and health-performance benchmarks for the same parameter is enormous — and understanding that gap is essential for making defensible monitoring decisions.
| Parameter | OSHA PEL (US) | HSE WEL (GB) | ASHRAE 62.1 / WELL v2 Target | WHO 2021 AQG |
|---|---|---|---|---|
| CO2 | 5,000 ppm (8-hr TWA) | 5,000 ppm (8-hr TWA) | ≤700 ppm above ambient / ≤800 ppm (WELL v2) | Not specified |
| PM2.5 | No specific IAQ standard* | No general IAQ WEL** | ≤15 µg/m³ (WELL v2) | 5 µg/m³ (annual mean) |
| Formaldehyde | 0.75 ppm (8-hr TWA) | 2 ppm (8-hr TWA, STEL) | ≤27 ppb (WELL v2) | 0.1 mg/m³ (80 ppb) |
| TVOCs | No general TVOC PEL*** | No general TVOC WEL*** | ≤500 µg/m³ (WELL v2) | Not specified |
*General Duty Clause applies. **Substance-specific WELs apply to individual dusts. ***Individual VOCs have substance-specific limits.
The CO2 comparison is the starkest illustration. The OSHA PEL of 5,000 ppm is an acute toxicity threshold — the concentration at which CO2 itself begins to cause physiological harm. No normally ventilated office will ever approach it. The ASHRAE and WELL targets of 700–800 ppm reflect a fundamentally different concern: cognitive performance and ventilation adequacy. Research consistently associates CO2 above 1,000 ppm with measurable declines in decision-making ability. These two numbers — 5,000 and 800 — are not different opinions about the same question. They answer different questions entirely.
The judgment call for organisations is which standard governs their monitoring programme, documented explicitly. A facility pursuing WELL v2 certification monitors against 800 ppm CO2 and 500 µg/m³ TVOCs. A manufacturing operation with solvent exposure monitors against substance-specific PELs for each identified VOC — a TVOC number is irrelevant for that purpose. Both are “workplace air quality monitoring.” Both require different thresholds, instruments, and actions when exceeded.
How to Implement a Workplace Air Quality Monitoring Programme
A monitoring programme that produces defensible, actionable data follows a structured sequence. Each step has a regulatory anchor, and skipping any of them undermines the entire effort.
1. Conduct a hazard assessment. Under COSHH (GB), this is the legally required assessment of substances hazardous to health before work begins. Under OSHA (US), the General Duty Clause and substance-specific standards create equivalent obligations. The assessment identifies which airborne substances the work activity generates, which workers are potentially exposed, and at what duration and intensity. This step — not a sensor catalogue — determines what gets monitored.
2. Determine the monitoring strategy. Based on the hazard assessment, define the sampling approach: which workers or locations represent worst-case and typical exposures, what sampling duration reflects the exposure pattern (full-shift TWA, short-term task-based, peak), which validated analytical methods apply, and how many samples provide statistical confidence in the results.
3. Select appropriate equipment. Match instruments to purpose. Compliance monitoring requires validated sampling media (NIOSH or HSE MDHS methods), calibrated pumps, and AIHA-accredited laboratory analysis. IAQ wellness monitoring uses continuous sensors with documented accuracy specifications and regular calibration schedules. Using the wrong category of instrument for the wrong purpose produces data that is neither compliant nor useful.
4. Establish baselines and compare against applicable limits. Initial monitoring establishes the exposure profile under normal operating conditions. Compare results against the applicable legal limits (PELs, WELs) and, where the organisation has adopted them, against more protective benchmarks (NIOSH RELs, ACGIH TLVs, WELL targets). Document which limits apply and why.
5. Set action levels and response protocols. Define what happens when readings exceed thresholds. OSHA substance-specific standards define action levels (typically half the PEL) that trigger specific responses — increased monitoring frequency, medical surveillance, worker notification. For general IAQ, establish similar tiered responses: investigate at one threshold, implement controls at another, evacuate if needed.
6. Document, record-keep, and communicate. COSHH requires monitoring records retained for at least 5 years — 40 years where health surveillance is involved. OSHA requires employee notification of monitoring results within 5 working days. Beyond compliance, communicating results to workers builds the trust that makes safety programmes function. Monitoring data locked in a hygienist’s report that no one reads is monitoring data wasted.
7. Review and repeat. A single set of measurements tells you what the air was like on that day under those conditions. It does not tell you what happens during peak production, after a process change, during seasonal HVAC transitions, or when outdoor air quality deteriorates. Monitoring frequency must be driven by risk level, process changes, introduction of new substances, and regulatory requirements — not by a calendar reminder set and forgotten.
The Fix That Works: The most effective monitoring programmes integrate continuous IAQ data (for trend awareness and ventilation management) with periodic professional exposure assessments (for compliance verification). Continuous data identifies when and where to investigate. Professional sampling provides the legally defensible answer.

The Role of Air Quality Monitoring in Building Certifications
Building certification programmes have become a significant driver of IAQ monitoring adoption outside traditional industrial hygiene contexts. For facility managers and corporate real estate teams, these programmes create business-case justification for monitoring investments that regulatory compliance alone may not provide.
WELL v2, administered by the International WELL Building Institute, dedicates its Air concept to IAQ performance. Preconditions A01 (Air Quality) and A03 (Ventilation Design) establish minimum requirements, while optimisations A05, A06, and A08 reward continuous monitoring, enhanced air treatment, and pollutant source management. Continuous IAQ monitoring can satisfy multiple preconditions and earn up to 9 optimisation points. The WELL Operations Rating, launched in January 2026, takes a data-driven approach to building performance verification — with IAQ as its largest feature category, representing 9 of 33 features (IWBI, 2026). This signals a market shift toward ongoing performance evidence rather than point-in-time design verification.
LEED v5 is expected to expand IAQ monitoring requirements with greater emphasis on continuous performance verification and measured outcomes rather than prescriptive design inputs. RESET Air focuses specifically on continuous IAQ data quality, requiring Grade A sensor accuracy and ongoing calibration verification.
The business case extends beyond certification plaques. Research from the Harvard T.H. Chan School of Public Health’s healthy buildings programme has consistently linked improved indoor air quality to measurable cognitive performance gains, with one widely cited finding suggesting that modest ventilation improvements costing approximately $40 per employee could yield thousands of dollars in annual productivity benefits per employee.
Certification monitoring and regulatory compliance monitoring can share sensor infrastructure and data dashboards, but they serve different masters. A WELL audit failure for TVOCs above 500 µg/m³ is a certification setback. The same reading may not trigger any OSHA enforcement action, because OSHA has no general TVOC standard. Organisations pursuing both regulatory compliance and building certification must maintain clarity on which results matter for which purpose — and document that distinction in their monitoring programme.
Common Challenges and Mistakes in Workplace Air Quality Monitoring
Published enforcement records and occupational hygiene literature reveal consistent patterns of monitoring failure. These are not hypothetical risks — they are the specific ways programmes produce misleading data or fail to protect workers.
Conflating occupational exposure monitoring with comfort-level IAQ monitoring. This is the foundational error this entire article is built to address. Organisations install continuous CO2 and PM2.5 sensors, generate green-light dashboards, and assume their air quality monitoring obligations are met. Meanwhile, workers handling solvents, welding, cutting stone, or disturbing legacy materials have no personal exposure data against the applicable PELs or WELs. The two systems answer different questions. Neither substitutes for the other.
Using uncalibrated or consumer-grade sensors for compliance-critical measurements. Consumer IAQ monitors are designed for awareness, not enforcement. Their accuracy specifications, if documented at all, are insufficient for determining whether an exposure limit has been exceeded. When monitoring data becomes evidence — in an OSHA citation, an HSE enforcement notice, or a workers’ compensation claim — the instrument’s calibration history and the method’s validation status will be examined. Consumer-grade devices fail that examination.
Monitoring in unrepresentative conditions. Testing during low occupancy, with windows open, outside normal production hours, or in locations distant from actual emission sources produces data that understates real exposures. A monitoring programme must capture worst-case and typical conditions, not best-case ones.
Failing to account for mixed exposures. When multiple contaminants are present simultaneously, OSHA requires additive-effect calculations using the mixture formula (29 CFR 1910.1000(d)(2)(i), US). Individual results below each respective PEL can still represent an overexposure when combined. This calculation is routinely omitted.
Treating monitoring as periodic spot-checks. A single round of sampling captures a snapshot. It does not account for seasonal ventilation changes, process modifications, new substances introduced, or deteriorating extraction equipment. Monitoring must be integrated into management-of-change procedures and operational review cycles.
Not communicating results to workers. Both OSHA and COSHH require that workers be informed of their monitoring results. Beyond legal obligation, workers who understand their exposure data engage more seriously with controls and PPE requirements. Monitoring data locked in a filing cabinet protects no one.
Field Test: Ask this question of any workplace air quality monitoring programme: “If a regulator requested all monitoring records for the past three years, would the data demonstrate a competent, ongoing programme — or a single set of readings filed and forgotten?” The answer reveals whether the programme is real or performative.
The most damaging pattern — across enforcement records and prosecution case files — is what I describe as “monitoring for the file.” Measurements are taken, results are recorded, and no corrective action follows. If monitoring reveals elevated exposures and the employer takes no action, the monitoring data itself becomes prosecution evidence of a known hazard that was identified and ignored.

Frequently Asked Questions
Conclusion
The single most consequential mistake in workplace air quality monitoring is treating it as one discipline when it is two. Occupational exposure monitoring — personal sampling against PELs and WELs — is a legal compliance obligation with prescribed methods, legally binding limits, and enforcement consequences. Indoor environmental quality monitoring — continuous sensor data for CO2, PM2.5, TVOCs, comfort, and certification — is an operational and business-performance tool with advisory thresholds and certification requirements. Both are valuable. Neither substitutes for the other. Organisations that conflate them end up with wellness dashboards that look reassuring and compliance files that contain no defensible data.
The industry pattern that causes the most preventable harm is what the published enforcement record consistently reveals: monitoring data collected, filed, and never acted upon. In 2024, US private industry employers reported 54,000 respiratory illness cases (Bureau of Labor Statistics, 2026). Behind that number are workplaces where airborne contaminants were either never measured, measured inadequately, or measured and ignored. Every stage of that failure chain is a monitoring programme decision.
A workplace air quality monitoring programme earns its value when it changes decisions — when a baseline assessment triggers an engineering control, when a continuous trend triggers an investigation, when a comparison against the ACGIH TLV rather than the outdated OSHA PEL leads to an earlier intervention. The air workers breathe during a shift is not an administrative detail. Monitoring it properly is the difference between an employer who documents compliance and one who actually prevents disease.