
TL;DR
- Clean before you disinfect. Soil deactivates many disinfectants, so a dirty surface cannot be reliably disinfected — cleaning comes first, every time.
- Contact time is the step people skip. The surface must stay visibly wet for the product’s full label time, or the kill claim fails.
- The chemicals are an occupational hazard. Disinfectants cause asthma, dermatitis, and toxic gas when mixed — treat exposure as seriously as the germs.
- Disinfection is risk-triggered, not a default. Most surfaces need only routine cleaning; reserve disinfection for high-touch points, illness, and spills.
- Employers carry legal duties. US HazCom and UK COSHH both require assessment, control, information, training, and records for assigned cleaning staff.
Workplace cleaning and disinfection procedures follow one fixed order: clean visible soil first, then apply an approved disinfectant at the correct dilution and keep the surface wet for the full label contact time. Disinfection is reserved for high-touch surfaces, illness in the space, and blood or body-fluid spills — not applied to every surface as a daily reflex.
A persistent belief on many sites is that a stronger disinfectant, used generously and often, is the safe choice. That belief is wrong on two counts, and both cause real harm.
The disinfectant is itself an occupational hazard, and over-applying it raises exposure without lowering risk on low-touch surfaces. In Great Britain, an estimated 12,000 lung-disease deaths each year are linked to past occupational exposures (HSE, 2025) — a total figure across all causes, but a reminder that what workers breathe at work matters over a lifetime.
This guide sets out workplace cleaning and disinfection procedures for non-healthcare settings — offices, warehouses, retail, and manufacturing common areas. It covers the correct sequence, contact time, product selection, the chemical-health risks competitors ignore, the US and UK legal duties side by side, and the higher-risk procedure for blood and body-fluid spills. Healthcare and food production sit under separate, stricter regimes and are out of scope here.

Cleaning, Sanitizing, and Disinfecting: What’s Actually Different
These three words describe three different outcomes, and confusing them is where most procedures fail. Cleaning removes soil and lowers microbial load but kills nothing; sanitizing reduces germs to a level treated as safe; disinfecting inactivates a wider spectrum, including viruses, on hard non-porous surfaces.
The distinction is not just technical — in the US it is legal. Sanitizers and disinfectants are antimicrobial pesticides registered with the EPA under FIFRA, and their efficacy claims and required contact time are tied to the registered label, not to marketing copy. UK and EU products sit under separate biocidal-product rules, but the same principle holds: the approved label governs what the product can claim.
| Process | What it does | Kills germs? | When to use |
|---|---|---|---|
| Cleaning | Removes dirt, dust, and organic soil with detergent and water | No — physically removes, does not kill | Routine baseline for most surfaces |
| Sanitizing | Reduces bacteria to a level judged safe | Reduces, does not eliminate broadly | Food-contact and some shared surfaces |
| Disinfecting | Inactivates a broad range of microbes, including viruses | Yes, on hard non-porous surfaces | High-touch points, post-illness, spills |
One rule carries the rest of this article: you generally cannot disinfect a dirty surface. Organic soil — grease, food residue, body fluids — physically shields microbes and chemically deactivates many disinfectant actives, which is the technical reason clean-then-disinfect is the correct order rather than a nicety.
A common failure mode follows from misreading this. Teams reach for a “one-step” disinfectant-cleaner on a visibly soiled surface and assume the disinfection claim still holds — but most one-step labels require a separate pre-clean when soil is heavy, and skipping it silently defeats the kill while leaving the paperwork looking compliant.
When Should a Workplace Disinfect Instead of Just Clean?
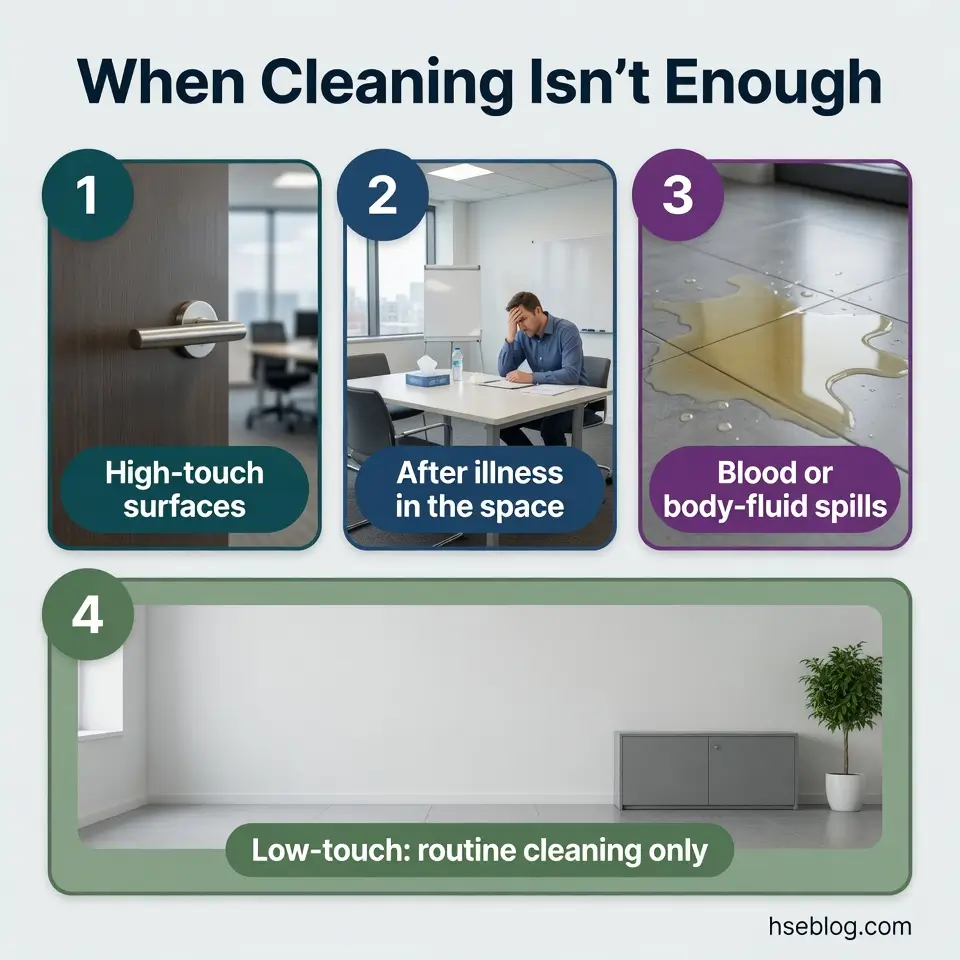
Most workplace surfaces only need routine cleaning. Disinfection is warranted for high-touch surfaces, after someone in the space has been ill, and after spills of blood or body fluids — a risk-based trigger, not a blanket daily habit.
This is the recalibration that post-pandemic guidance made explicit. Updated CDC facility guidance on when to clean versus disinfect reflects a 2024 shift away from the 2020 “disinfect everything” posture, as surface (fomite) transmission of respiratory viruses was reassessed as lower than once assumed.
A consistent pattern in workplaces is the blanket “disinfect all surfaces hourly” rule adopted in 2020 and never revisited. Treating a control as set-and-forget ignores its cost.
Over-disinfection is not a free safety margin. It carries real downsides:
- Higher chemical exposure for staff. More applications mean more inhalation and skin contact for the people doing the work.
- Surface and equipment damage. Repeated disinfectant contact corrodes metals and degrades porous materials over time.
- No proportional benefit on low-touch areas. A rarely-touched ceiling or back-of-store shelf gains little from daily disinfection.
The judgment call is between convenience and proportionality. In most non-healthcare contexts the balance favours routine cleaning as the default, with disinfection documented in the cleaning plan and tied to surface touch-frequency and the setting’s actual transmission risk.
Step-by-Step Workplace Cleaning and Disinfection Procedure
The procedure runs in a fixed order, and contact time is its centrepiece because it is the single most-violated step. Work through it in sequence:
- Ventilate and put on PPE. Open airflow and don the gloves and eye protection specified for the product before you start.
- Remove visible soil. Clean the surface with detergent first; this is the step that makes disinfection possible.
- Apply the disinfectant at the correct dilution. Mix to the label ratio — guessing in either direction undermines the result.
- Keep the surface visibly wet for the full label contact time. This is non-negotiable; if it dries early, re-apply.
- Rinse if the label requires it. Food-contact surfaces typically need a potable-water rinse; general surfaces often do not.
- Dispose of materials and remove PPE in the correct order. Bag used cloths; doff gloves last to avoid contaminating clean hands.
- Wash your hands. Hand hygiene closes the loop regardless of glove use.
Contact time varies enormously by product — from seconds to roughly ten minutes — and that figure lives on the registered label, not in habit or memory. A product wiped dry after twenty seconds when its label demands four minutes has not disinfected anything, however well it foamed.
Dilution matters in both directions. Under-dilution wastes product and raises exposure for no benefit; over-dilution can drop the active below its efficacy threshold, so the surface looks treated but isn’t.
The recurring habit that defeats all of this is “spray-and-wipe-in-one-motion” — staff spray and immediately wipe the surface dry to save time. It is the most common reason a technically-compliant, correctly-chosen product still fails to disinfect.
Reading the Label and Safety Data Sheet (SDS) Before You Start
Two documents govern every product, and they answer different questions. The label tells you dilution, contact time, and approved use sites; the Safety Data Sheet tells you the hazards, the PPE required, first-aid steps, and — critically — what the product must never be mixed with.
Treat the SDS as a working document consulted before first use of a new product, not a binder produced only when an inspector asks. The gap between having SDSs and using them is exactly where avoidable exposures happen.

Selecting the Right Disinfectant for the Surface and the Threat
Stronger is not better, and bleach is not the universal answer. The right disinfectant is the one matched to the target organism and the surface material — broad-spectrum power you don’t need is just extra exposure and extra corrosion.
Three variables drive the choice: the pathogen you’re targeting, the surface you’re treating, and the contact time the workflow can realistically hold. Each common active-ingredient family trades these off differently:
| Active family | Strengths | Trade-offs |
|---|---|---|
| Sodium hypochlorite (bleach) | Broad-spectrum, inexpensive | Corrosive to metals; deactivated by organic soil; never mix with acids or ammonia |
| Quaternary ammonium (quats) | Common, surface-friendly, residual action | Recognised respiratory sensitisers (asthmagens); soil reduces efficacy |
| Alcohols (≥70%) | Fast-acting, leave no residue | Evaporate quickly, so the required wet contact time is hard to hold; flammable |
| Hydrogen-peroxide-based | Broad-spectrum, breaks down to water and oxygen | Can affect some surfaces; check material compatibility |
In the US, confirm the product is EPA-registered and approved for your use site before relying on any claim. Where a specific pathogen matters, verify the claim against EPA’s published lists rather than the front label — the EPA’s registered-disinfectant listings exist precisely so claims can be checked.
Procurement is where this goes wrong. Products are frequently selected on price or smell rather than on contact time and surface compatibility — which is how a site ends up with corroded fixtures and a disinfectant no one keeps wet long enough to do its job.
The Hidden Hazard: Health Risks of Cleaning and Disinfectant Chemicals
The disinfectant chemicals are themselves an occupational hazard, and this is the part most cleaning guidance leaves out entirely. Respiratory sensitisation, skin disease from wet work, and toxic gas from mixing are documented, foreseeable harms — not rare freak events.
Medical disclaimer: This section covers chemical exposure for HSE practitioner reference. It is not medical advice. Workers with breathing difficulty, persistent cough, skin reactions, or any exposure concern should consult an occupational physician or qualified medical professional. We recommend this content be medically reviewed before publication.
Respiratory: sensitisation and occupational asthma
Several disinfectants — quaternary ammonium compounds among them — are recognised respiratory sensitisers, and HSE lists cleaning chemicals among documented causes of occupational asthma. Once sensitisation is established, the airways can flare at exposures far below the level that first caused the problem, which is why prevention beats management.
Skin: contact dermatitis from wet work
Frequent wet work combined with disinfectant contact is a leading driver of work-related contact dermatitis. Broken or cracked skin then raises both infection risk and chemical absorption, compounding the original problem.
The deadly mixing reactions
Some combinations produce toxic gas almost instantly. Two must never happen:
- Bleach + ammonia → chloramine gas. Many glass and surface cleaners contain ammonia.
- Bleach + acid → chlorine gas. Acidic descalers and some toilet cleaners are the usual culprits.
Both reactions have caused workplace injuries and fatalities. No reliable count exists for non-healthcare workplaces specifically, but public-health hazard alerts repeatedly document serious harm from exactly this improvisation.
Never combine cleaning products. If fumes are produced, leave for fresh air immediately, do not re-enter, and seek medical attention. Detailed emergency response is on the product SDS.
The single most dangerous habit in this whole domain is “boosting” a slow-working product by combining two bottles to clear a tough job faster. Training repeatedly fails to extinguish it, which is why the instruction has to be blunt and repeated: one product, one task, never mixed.

Legal Duties: Hazard Communication (US) and COSHH (UK)
Legal disclaimer: This regulatory content reflects general HSE professional understanding of US and UK requirements as of 2026. It is not legal advice. Specific compliance, enforcement, or prosecution questions should go to qualified legal counsel in the applicable jurisdiction. Regulatory content here was last reviewed at the date shown in the byline.
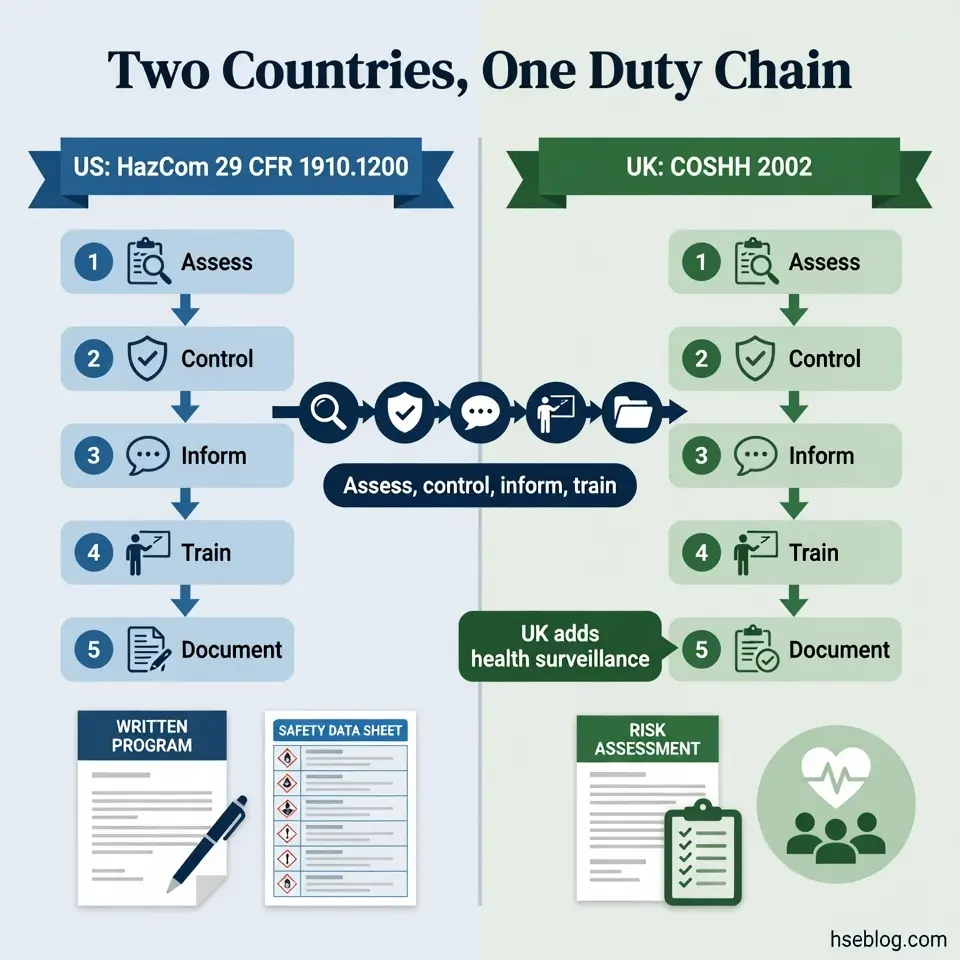
When staff are assigned to clean and disinfect the workplace, the employer carries enforceable duties in both countries. The two regimes share one logic — assess, control, inform, train, document — but differ in mechanics.
In the US, the OSHA Hazard Communication Standard (29 CFR 1910.1200) requires a written program, container labels, accessible Safety Data Sheets, and training for employees exposed beyond typical consumer use. The practical reading of the consumer-product exemption is where sites get caught: an employee occasionally wiping their own desk may be exempt, but staff assigned to clean and disinfect are not — that routine, work-related exposure triggers the full HazCom duties.
This standard is also changing. The 2024 HazCom final rule, aligning primarily with GHS Revision 7, is estimated to affect more than 265,000 workplaces and roughly 1.5 million employees (US OSHA / Federal Register, 2024), and it alters disinfectant-product labels and SDSs. In January 2026 OSHA extended the phased compliance deadlines by four months, so updated documentation will keep arriving through 2026–2028.
In the UK, the duties sit under COSHH 2002. The structure runs through specific regulations:
| Duty | US — OSHA HazCom (29 CFR 1910.1200) | UK — COSHH 2002 |
|---|---|---|
| Assess | Identify hazardous chemicals present | Risk assessment under Reg 6 |
| Control | Hierarchy of control before PPE | Control of exposure under Reg 7 |
| Inform & train | Written program, labels, SDS access, training | Information, instruction, and training |
| Health checks | Not specified under HazCom | Health surveillance under Reg 10 where asthma/dermatitis is foreseeable |
| Exposure limits | OSHA PELs (separate standards) | EH40 Workplace Exposure Limits |
Both regimes share hierarchy-of-control logic: eliminate or substitute and apply engineering controls before relying on PPE. And both treat the SDS as something staff must be able to act on — the binder that exists for the inspector but is never read before using a new product is precisely the failure point.
PPE, Ventilation, and Engineering Controls for Cleaning Staff
A frequent and false reassurance is that gloves and a mask make any product safe to use. PPE is the last line of defence, not the first — under both OSHA and COSHH logic, ventilation and safer-product choices come before it.
Working down the hierarchy of control for cleaning tasks:
- Substitution first. Choosing lower-hazard products or formats — for example, ready-to-use solutions over decanting concentrates — cuts exposure at the source before any PPE is needed.
- Ventilation second. Adequate fresh air dilutes vapours, and UK HSE guidance addresses fresh-air supply rates explicitly; apply disinfectants where there is genuine airflow, not in sealed cupboards.
- PPE last, and matched to the product. Use the gloves and eye protection the SDS specifies, with splash protection where splashing is possible, and follow a deliberate don/doff/dispose sequence.
Glove selection is where reassurance turns false. A single bulk-bought box is usually issued for every task, yet the SDS often specifies a particular glove material for a given chemical — and the OSHA hand-protection standard (29 CFR 1910.138) requires employers to select protection appropriate to the substance. A mismatched glove gives confidence while the chemical permeates through it.
Blood and Body-Fluid Spill Cleanup: A Higher-Risk Procedure
Competent-person caveat: This is general HSE knowledge. Blood and body-fluid spill cleanup is an exposure-critical procedure that must be planned and supervised by a competent person, with relevant training, jurisdiction-specific authorization, and a site-specific exposure control plan. The summary below does not replace that training. Recognized pathways include NEBOSH, IOSH, and OSHA outreach training, or regional equivalents.
In the US, this work falls under the OSHA Bloodborne Pathogens Standard (29 CFR 1910.1030) wherever occupational exposure is reasonably anticipated — and that explicitly includes general cleaning staff who clean up blood, not only healthcare workers. The standard requires an exposure control plan, PPE, surface decontamination, and regulated-waste handling.
Apply universal precautions: treat all blood and body fluids as infectious, regardless of the apparent source. At summary level, the procedure runs:
- Restrict the area. Keep people away from the spill.
- Put on PPE. Gloves, eye protection, and any protection the exposure control plan specifies.
- Contain and absorb. Use the spill kit to soak up fluid without spreading it.
- Clean the area. Remove visible contamination before disinfecting.
- Disinfect with an appropriate product. Use a listed, suitable disinfectant at the correct dilution and full contact time.
- Dispose as regulated waste. Bag and label per the plan, not in general waste.
- Decontaminate reusable equipment, then wash hands. Act as soon as feasible throughout.
The pattern that creates real risk is quiet expectation: general cleaning teams told to handle blood spills with no bloodborne-pathogens training and no exposure control plan, because “it’s just cleaning.” That is a serious compliance and safety gap. Large or unknown-source contamination may warrant specialist remediation rather than in-house staff.

Building a Workplace Cleaning and Disinfection Program
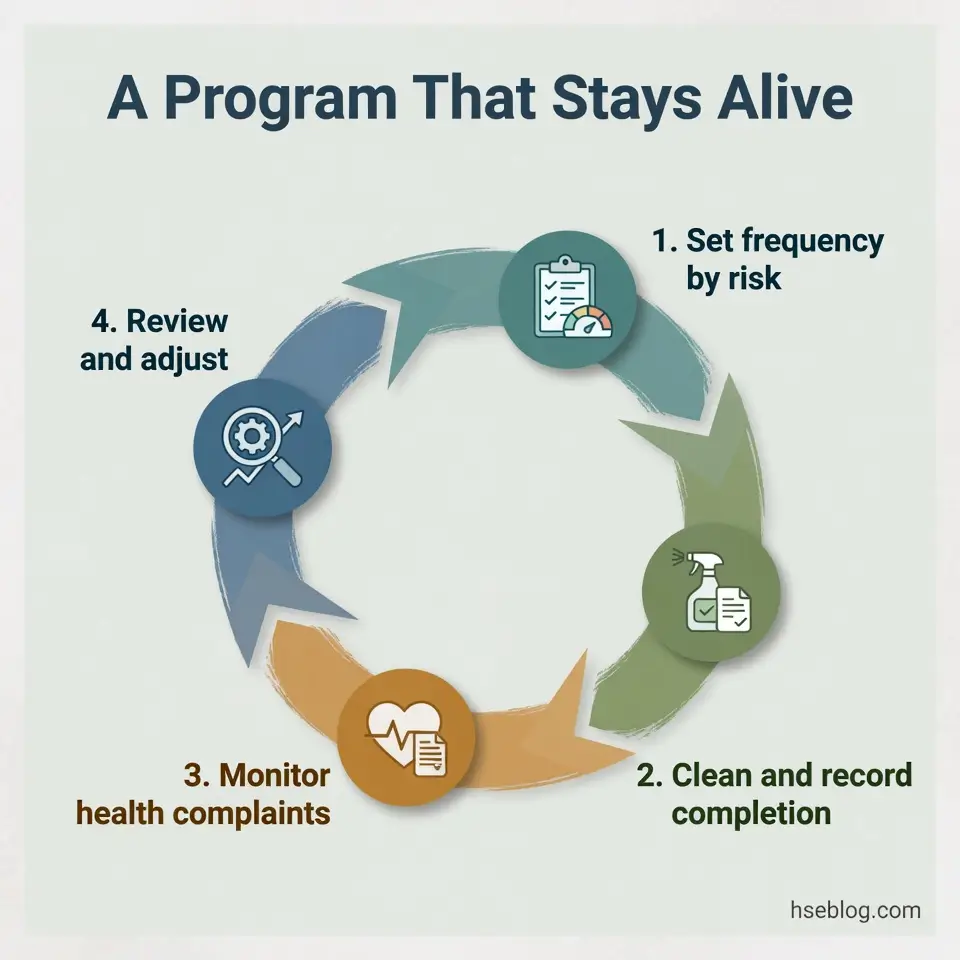
A program is defined by its feedback loop, not its laminated schedule. Moving from task to system means setting frequency by risk, documenting the plan, and reviewing it against what staff actually report.
Set frequencies by surface touch-frequency and the setting’s risk, not by a single blanket rule:
- High-touch surfaces — frequent attention. Door handles, shared keyboards, lift buttons, and taps justify routine disinfection.
- General surfaces — routine cleaning. Desks, floors, and walls usually need cleaning, not daily disinfection.
- Shift operations — clean between or during shifts. Sites running multiple shifts may need cleaning scheduled around handovers.
The documentation is what satisfies both an OSHA and an HSE inspector: the written plan, the product list with SDSs, dilution charts, training records, and a defined review trigger. Auditable evidence — records of completion, not just intentions — is the difference between a real program and a checklist on a wall.
Build in monitoring of whether controls are actually working. Dermatitis or respiratory complaints, sickness absence, and incident reports are early-warning signals that exposure controls are failing — and a glossy schedule that no one checks against those complaints is a program in name only.
Frequently Asked Questions
Conclusion
The industry’s recurring mistake is treating disinfection as the goal and the chemical as harmless — when the chemical is often the larger hazard and the disinfection routinely fails on a skipped step. Most ranking guidance still describes what disinfecting is while ignoring the contact time that makes it work and the exposure that makes it dangerous.
If you change one thing in your workplace cleaning and disinfection procedures, make it this: hold the full label contact time, and stop mixing products to speed the job up. Those two habits — surfaces wiped dry too early, and bottles combined to “boost” a result — account for more failed disinfection and more avoidable chemical injury than any product choice.
The stronger position is also the simpler one. Clean as the baseline, disinfect by risk, match the product to the surface, keep it wet for its time, and document the program so it survives a staff change and an inspector. Competent control here is quiet, repeatable, and measured by what your cleaning team breathes and touches over years — not by how much disinfectant gets sprayed in a shift.