

TL;DR
- Most wellbeing programs fail because they target symptoms, not systems. Free fruit and yoga sessions look good in annual reports but do nothing when the real problem is chronic overtime, toxic supervision, or zero recovery time between shifts.
- The 10 initiatives in this article have been field-tested across heavy industry, construction, and EPC projects — each one selected because it produced measurable reductions in absenteeism, incident rates, or voluntary turnover within 12 months of implementation.
- Psychosocial risk is now a regulatory obligation, not a corporate perk. ISO 45003, EU psychosocial directives, and updated HSE UK guidance all require organizations to identify and control psychological hazards the same way they control physical ones.
- Wellbeing works only when leadership owns it operationally — not when it’s delegated to HR as a side project with a wellness poster budget.
- Start with two or three initiatives that address your site’s actual stressors, measure them against leading indicators, and expand only after you see traction. Breadth without depth is the number one reason wellbeing programs collapse.
I was reviewing incident investigation summaries for a pipeline construction project in Central Asia when a pattern jumped off the page. Eleven recordable injuries over eight months — and nine of them involved workers who had been on rotation for more than 28 consecutive days without a proper rest break. Two of those workers had flagged fatigue and stress concerns through informal channels weeks earlier. Nobody acted on it. The safety management system had every physical hazard covered — excavation permits, energy isolation, lifting plans — but there was nothing, not a single documented control, addressing the fact that people were mentally and physically exhausted before they even picked up a tool.
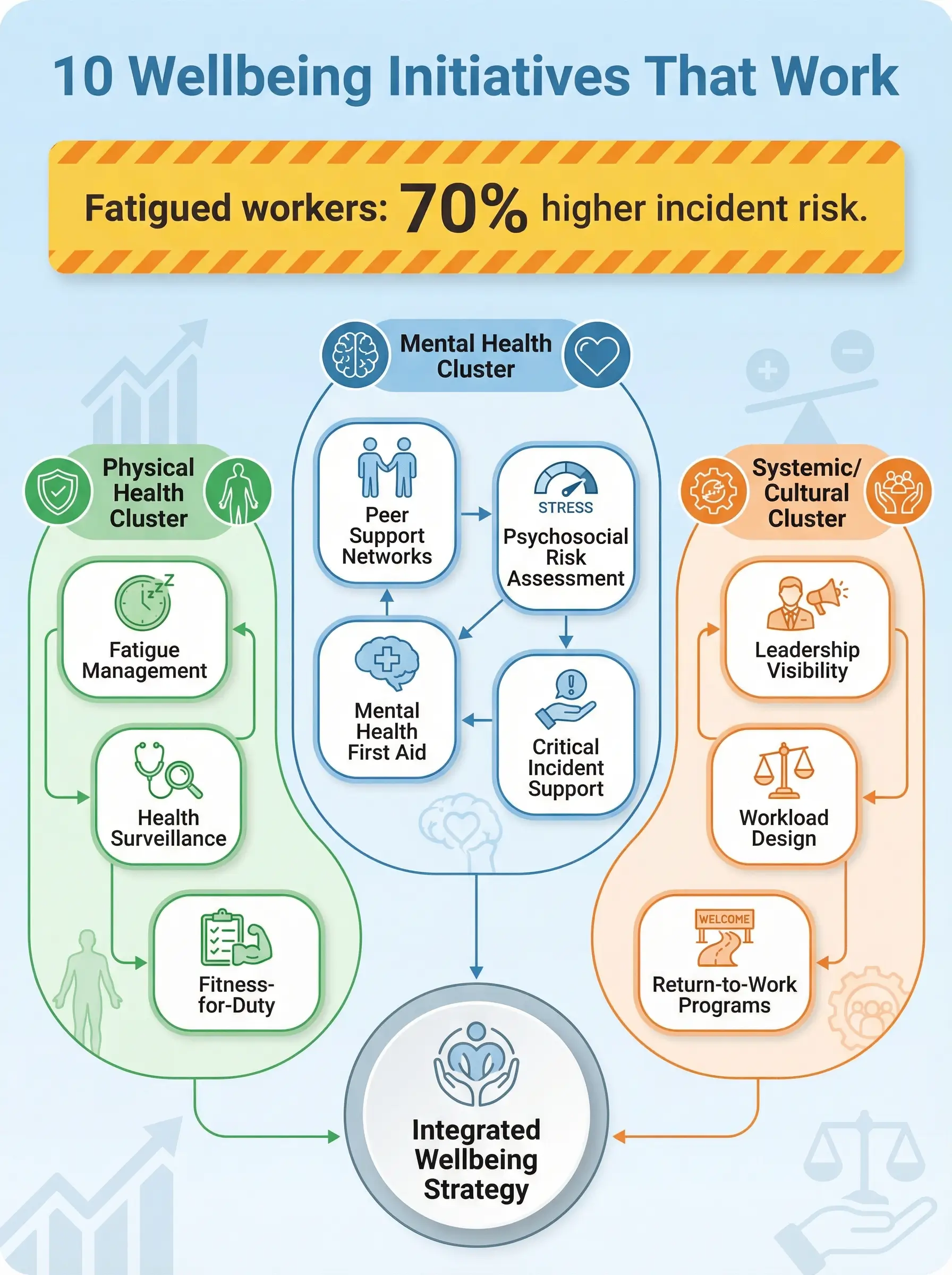
That project became a turning point for how I approach occupational health and safety management. Workplace wellbeing initiatives are not an HR luxury or a feel-good corporate add-on. They are operational controls — and when they are missing, people get hurt. The data backs this up consistently: fatigued workers are 70% more likely to be involved in a workplace incident, and sites with unmanaged psychosocial risks see injury rates two to three times higher than comparable operations with active wellbeing programs. This article covers ten workplace wellbeing initiatives that I have seen work — not in theory, not in a wellness brochure, but on active construction sites, offshore platforms, refinery turnarounds, and mining operations where the consequences of getting it wrong are measured in stitches, fractures, and fatalities.
What Makes a Wellbeing Initiative “Work” in High-Risk Industries
Before listing specific programs, it is worth defining what “actually works” means in an operational HSE context — because the corporate wellness industry has spent two decades selling initiatives that look impressive on dashboards but change nothing on the ground.
A wellbeing initiative works when it produces at least one of these measurable outcomes within a defined period:
- Reduction in absenteeism or sick leave rates directly linked to the targeted health stressor — not a vague “improvement in morale”
- Decrease in incident frequency or severity rates among the population covered by the initiative, particularly for incidents with human factors as a contributing cause
- Improved leading indicator scores such as safety observation participation, near-miss reporting rates, or toolbox talk engagement — signals that workers are more present, more alert, and more willing to speak up
- Lower voluntary turnover in operational roles, particularly among skilled workers whose departure creates competency gaps and increases risk for replacement crews
- Reduction in workers’ compensation claims or occupational health referrals for conditions directly addressed by the initiative
I have watched companies spend six-figure budgets on wellness apps, ergonomic assessments, and motivational speakers — then wonder why their TRIR stayed flat. The reason is always the same: they treated wellbeing as a benefit instead of a control. The ten initiatives below are different because every one of them addresses a root cause, not a symptom.
ISO 45003:2021 — Psychological health and safety at work requires organizations to identify psychosocial hazards, assess the risks they create, and implement controls using the same hierarchy of controls framework applied to physical hazards. Wellbeing is no longer discretionary — it is a management system requirement. [External Link: ISO 45003:2021 — https://www.iso.org/standard/64283.html]
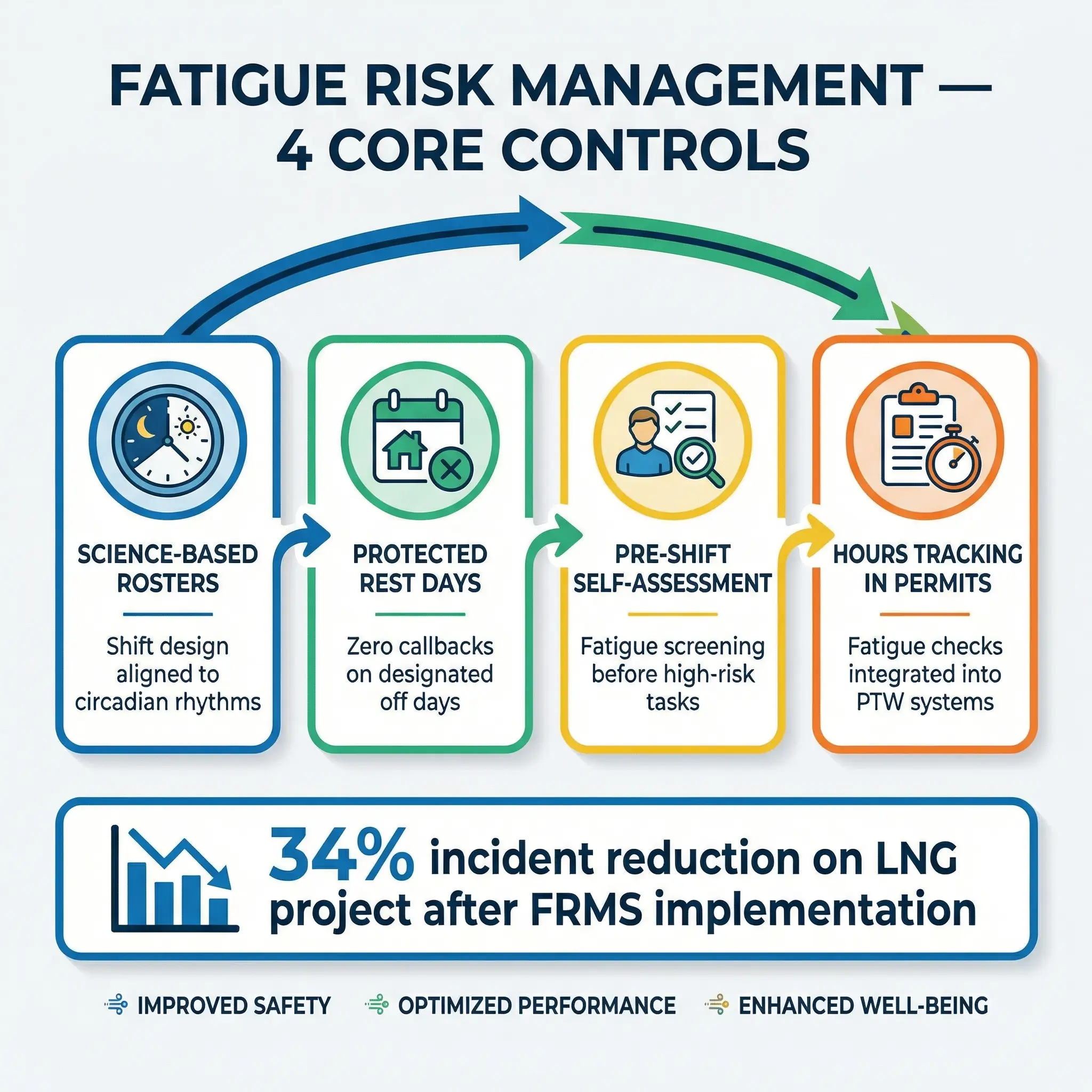
1. Fatigue Risk Management Systems (FRMS)
Fatigue is the single most undercontrolled hazard in heavy industry. I have investigated more incidents where fatigue was a root cause or major contributing factor than almost any other human factors issue — and in most cases, the organization had no formal system for identifying, assessing, or controlling fatigue risk. They had a “maximum hours worked” policy buried in a manual somewhere. That is not a fatigue management system.
A proper FRMS treats fatigue the same way a process safety system treats pressure or temperature — as a variable that must be monitored, controlled, and managed through engineering and administrative controls:
- Roster design based on circadian science. Shift patterns should limit consecutive night shifts to two or three maximum, provide at least 11 hours between shifts, and avoid the “quick changeover” pattern where workers rotate from nights to days with less than 24 hours off. The evidence on this is overwhelming — yet I still see 14/14 and 28/28 rotations on remote projects where nobody has reviewed the roster against fatigue science in years.
- Mandatory rest-day enforcement. Rest days must be genuinely protected — no callbacks, no “voluntary” overtime requests, no administrative tasks. I worked on a mining operation in Western Australia where the fatigue policy looked excellent on paper, but supervisors routinely called workers on their rest days for “quick” tasks. The policy was meaningless.
- Fatigue self-assessment tools at shift start. Brief, standardized checklists completed before high-risk tasks — not as a bureaucratic exercise, but as a genuine decision gate. If a worker scores above the threshold, they are reassigned to lower-risk duties or stood down with no penalty.
- Hours-of-work tracking integrated with permit-to-work systems. Before issuing a permit for confined space entry, working at height, or energized electrical work, the permit issuer checks whether the entrant has exceeded fatigue thresholds. This is a simple administrative control that prevents the most dangerous combination: high-risk task plus exhausted worker.
Pro Tip: The biggest resistance to FRMS comes from operations managers who see rest-day enforcement as a productivity loss. Present it as a risk control with incident cost data. On one LNG project, implementing a proper FRMS reduced recordable incidents by 34% in the first year — the productivity “loss” from enforced rest was recovered three times over in reduced incident costs and avoided schedule disruption.
2. Structured Peer Support Networks
Mental health programs that rely solely on external Employee Assistance Programs fail in field environments. The reasons are practical — workers on remote sites, offshore platforms, or construction camps often cannot access a phone counselor during the narrow windows when they actually need support. And the cultural barrier is real: in male-dominated heavy industry, calling a helpline feels like an admission of weakness to many workers. Peer support networks solve both problems.
The model that I have seen deliver consistent results is based on trained peer supporters — workers who volunteer, receive accredited mental health first aid training, and are identified on site as approachable, confidential points of contact:
- Selection matters more than training. Peer supporters must be respected, trusted workers — not people appointed by management. On one offshore platform in the North Sea, the company initially appointed supervisors as peer supporters. Nobody used them. When they switched to worker-nominated volunteers, engagement tripled within two months.
- Confidentiality is absolute and non-negotiable. Peer supporters do not report individual conversations to management — ever. They report trends anonymously (“three workers this rotation have raised concerns about sleep disruption”) without identifying anyone. The moment confidentiality is breached, the program dies.
- Visible but not forced. Peer supporters wear a discreet identifier — a wristband, a helmet sticker — so workers know who to approach. But they never cold-approach someone or ask probing questions uninvited. The power of the model is that it normalizes help-seeking without creating pressure.
- Regular debriefs and supervision for the supporters themselves. Peer supporters absorb heavy emotional content. Without structured supervision from a qualified psychologist or counselor, they burn out or carry secondary trauma. Budget for this from day one.
Pro Tip: Measure peer support effectiveness through proxy indicators — not by counting conversations (which violates confidentiality). Track voluntary near-miss reporting rates, toolbox talk participation, and anonymous wellbeing survey scores before and after implementation. On a pipeline project in the Gulf, near-miss reporting increased by 41% within six months of launching a peer support network — a direct signal that workers felt safer speaking up across the board, not just about mental health.
3. Psychosocial Risk Assessment — Integrated into HIRA
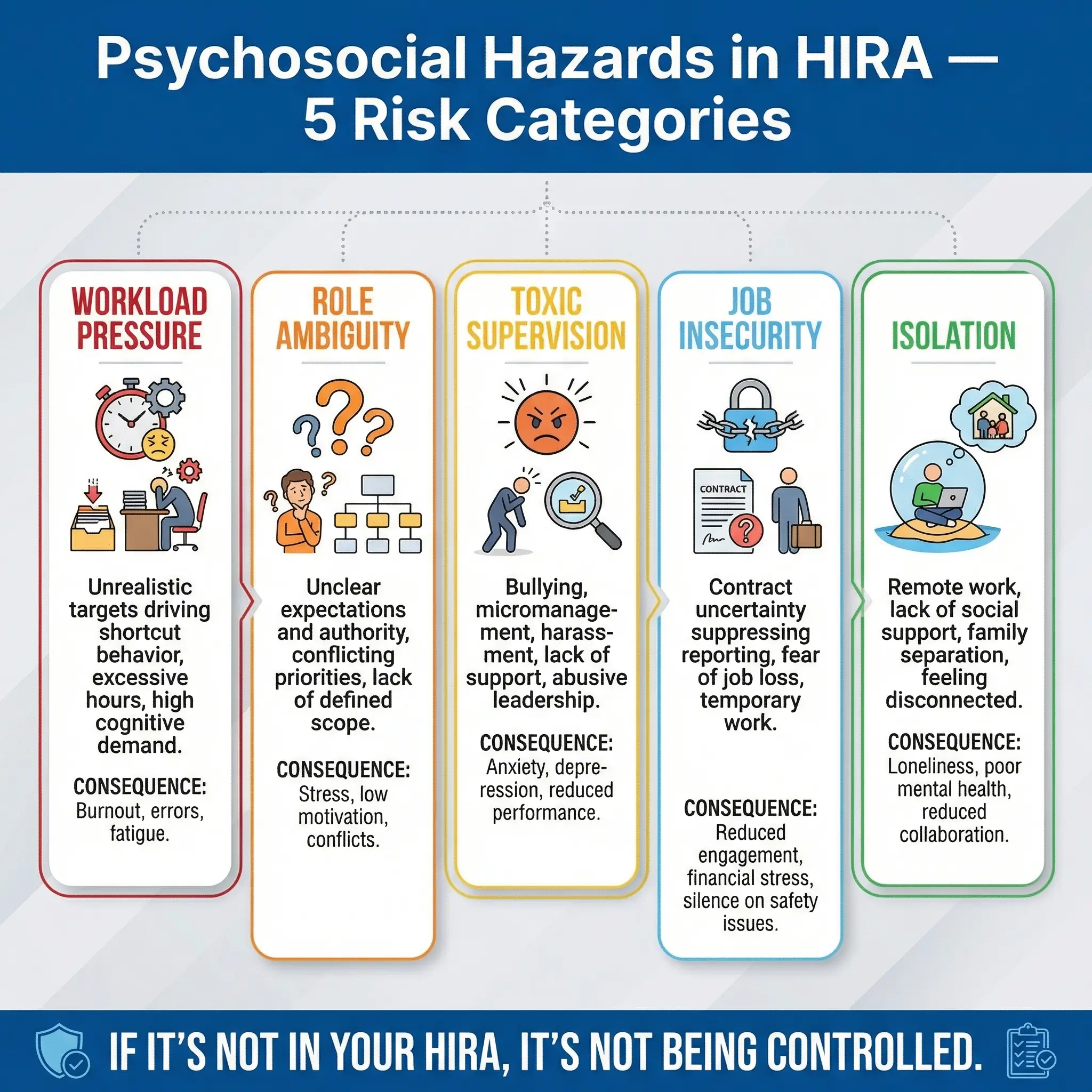
Most organizations conduct thorough Hazard Identification and Risk Assessment for physical hazards — fall from height, chemical exposure, struck-by incidents — but completely ignore psychosocial hazards. The result is a HIRA register that covers half the risk landscape and leaves the other half invisible. I have audited dozens of management systems where the risk register contained 200+ physical hazards and zero psychosocial entries. That is a system gap, not an oversight.
Psychosocial risks are workplace factors that can cause psychological harm, and they are well-defined in the literature and in ISO 45003. Integrating them into your existing HIRA process does not require a separate system — it requires adding a category:
- Workload and pace pressures. Are production targets creating chronic time pressure that forces workers to skip safety steps? This is the most common psychosocial hazard I find on construction sites — and it directly drives incident rates.
- Lack of role clarity. Do workers know exactly what is expected of them, who they report to, and what authority they have to stop work? Ambiguity creates stress and hesitation — both of which are precursors to incidents.
- Poor supervisor behavior. Bullying, micromanagement, public humiliation, and favoritism are psychosocial hazards with measurable health consequences. They must be assessed and controlled the same way you would control a noisy work environment or a poorly guarded machine.
- Job insecurity and contract uncertainty. Workers on short-term contracts who fear non-renewal are significantly less likely to report hazards, refuse unsafe work, or raise concerns. This is a systemic risk that affects safety culture at its foundation.
- Remote and isolated work conditions. Fly-in-fly-out workers, offshore crews, and remote site personnel face separation from family, limited social connection, and disrupted routines — all clinically recognized stressors.
The controls follow the standard hierarchy. Elimination means redesigning the work system to remove the stressor — for example, adjusting unrealistic production schedules. Substitution means replacing a high-stress work arrangement with a lower-stress alternative. Engineering controls might include redesigning shift patterns or providing dedicated rest facilities. Administrative controls include supervisor training, workload monitoring, and grievance procedures. PPE in the psychosocial context means individual coping resources — EAP access, resilience training — which should always be the last line of defense, not the first.
HSE UK Management Standards identify six primary psychosocial risk factors: demands, control, support, relationships, role, and change. These are the framework I use when integrating psychosocial hazards into any HIRA register. [External Link: HSE UK Management Standards — https://www.hse.gov.uk/stress/standards/]
4. Mental Health First Aid (MHFA) Training for Supervisors
Supervisors are the first point of contact for workers in distress — whether they realize it or not. A worker who is struggling with anxiety, depression, substance use, or a personal crisis will show behavioral changes on site long before they ever call a helpline. They become withdrawn, irritable, distracted, or start making uncharacteristic errors. Supervisors see this daily. The question is whether they have the skills to respond appropriately.
Mental Health First Aid training gives supervisors a structured framework for recognizing distress, initiating a conversation, and connecting the worker to appropriate support — without attempting to be a therapist:
- Recognition of warning signs. Changes in behavior, appearance, work quality, attendance patterns, social withdrawal, increased conflict with coworkers, or sudden risk-taking. MHFA training teaches supervisors to notice patterns — not diagnose conditions.
- The approach conversation. How to have a private, non-judgmental, one-on-one conversation that opens with concern rather than accusation. “I’ve noticed you seem different lately — is there anything I can do to help?” is fundamentally different from “Your performance has been slipping and I need you to sort it out.”
- Knowing the boundaries. MHFA-trained supervisors are not counselors. They learn exactly where their role ends and professional support begins. The goal is to be a bridge, not a solution.
- Immediate risk assessment. If a worker expresses suicidal ideation or intent to harm, the supervisor needs a clear, rehearsed protocol — not a panicked phone call to HR. MHFA covers this specifically.
I made supervisor MHFA training mandatory on a refinery turnaround project in Southeast Asia after two separate incidents where workers in clear distress were told to “toughen up” by their foremen. Both workers were subsequently involved in safety incidents within 48 hours. After the training rollout, supervisors referred 14 workers to professional support over the following six months — workers who would previously have been invisible to the system until something went wrong.
Pro Tip: Do not make MHFA a one-time training event. Include a refresher module in every supervisor competency cycle and run scenario-based practice sessions quarterly. Skills decay fast when they are not used — and the first time a supervisor needs to have a crisis conversation should not be the first time they practice one.
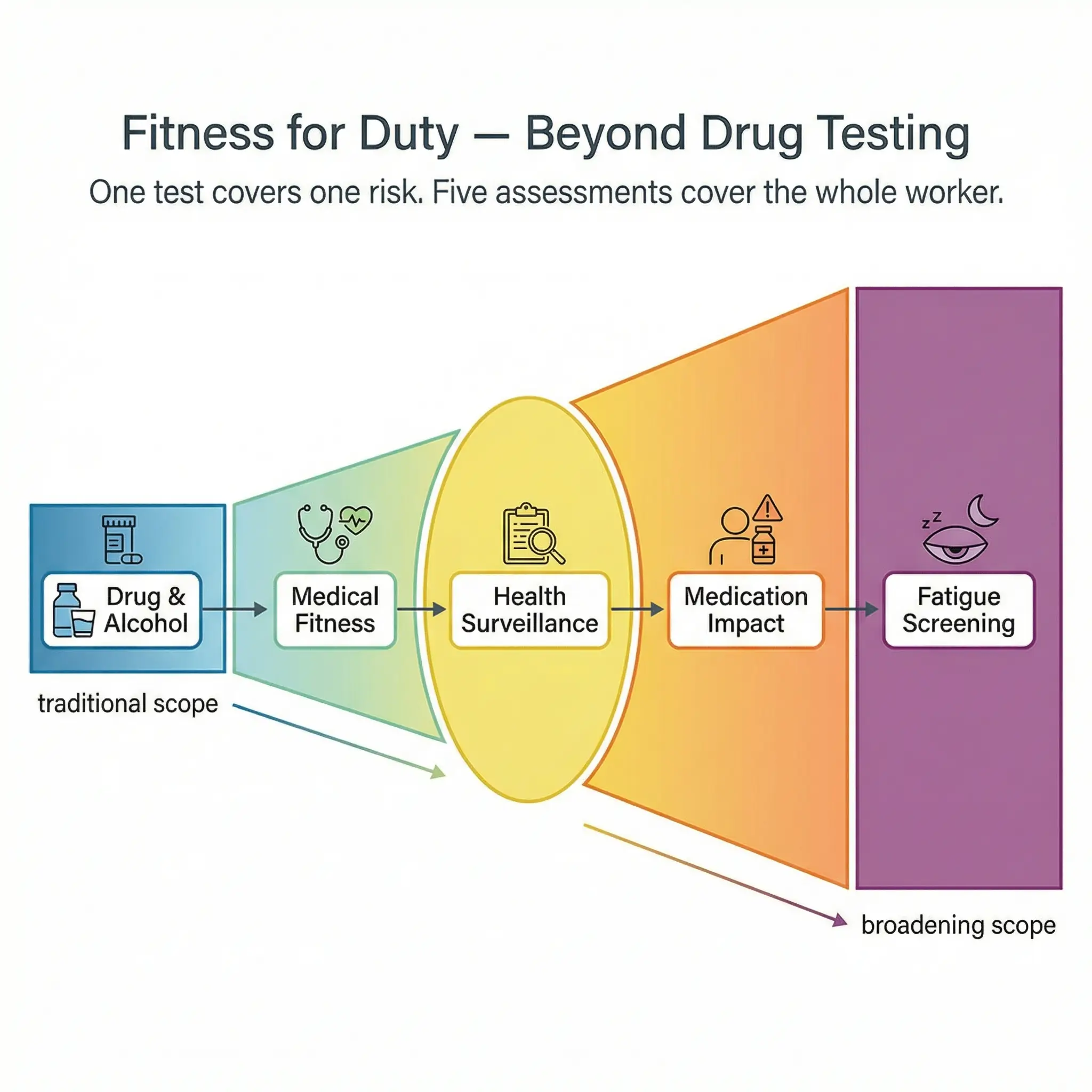
5. Fitness-for-Duty Programs Beyond Drug and Alcohol Testing
Most fitness-for-duty programs in heavy industry begin and end with drug and alcohol testing. That is one narrow slice of fitness for duty. A worker can pass a urinalysis and still be completely unfit to operate a crane, work at height, or enter a confined space because they slept three hours, are managing an uncontrolled medical condition, or are taking prescription medication that impairs reaction time.
A comprehensive fitness-for-duty program assesses the whole person — not just their toxicology results:
- Pre-employment medical assessments aligned to job demands. The medical assessment must be task-specific. A worker who will spend eight hours in a harness at height needs cardiovascular and musculoskeletal screening that is different from someone working in a control room. Generic “fit for work” certificates from a local clinic are not sufficient for high-risk roles.
- Periodic health surveillance for ongoing exposures. Noise audiometry, respiratory function testing, skin surveillance for chemical handlers, and vision testing on a schedule determined by exposure risk — not by calendar convenience.
- Medication disclosure and assessment protocols. Workers taking opioid pain medication, sedating antihistamines, or certain psychiatric medications may be genuinely unfit for safety-critical tasks. A fitness-for-duty program needs a confidential process for assessing medication impacts without stigmatizing the worker or violating medical privacy.
- Fatigue and sleep quality screening. This links directly to FRMS. Workers reporting to a safety-critical shift should have a mechanism to flag that they are impaired by fatigue — with a clear, no-penalty pathway for reassignment.
| Assessment Type | What It Screens | Frequency | Applicable Standard |
|---|---|---|---|
| Pre-employment medical | Task-specific physical and mental fitness | Before deployment | OSHA 1910.120, client specs |
| Drug and alcohol testing | Substance impairment | Random + for-cause | 49 CFR Part 40 (US), client policy |
| Periodic health surveillance | Noise, respiratory, skin, vision | Annual or per exposure risk | OSHA 1910.95, COSHH (UK) |
| Medication review | Prescription impairment risk | At disclosure or change | Occupational physician protocol |
| Fatigue self-assessment | Sleep quality, hours of rest | Pre-shift for high-risk tasks | FRMS policy, ICAO/IMO adapted |
6. Leadership Visibility and Safety Engagement Walks
Every wellbeing initiative in this article will fail without visible leadership commitment. Not written commitment — visible commitment. Workers judge an organization’s real priorities by what leaders do on site, not by what they sign in a policy document. I have seen million-dollar wellbeing programs collapse because the project director never once walked the site, spoke to a crew, or asked a worker how they were doing.
Safety engagement walks — sometimes called Visible Felt Leadership (VFL) or leadership safety tours — are structured site visits where senior leaders interact directly with frontline workers about safety and wellbeing:
- Structured but not scripted. Leaders should have a framework (topics to explore, questions to ask) but never read from a checklist. Workers detect rehearsed performances instantly, and it destroys credibility.
- Focused on listening, not inspecting. The purpose is not to find violations. It is to understand working conditions, hear concerns, and demonstrate that leadership cares about the worker’s experience — including their mental and physical wellbeing.
- Consistent and predictable. A single walk per quarter is performative. Leaders should be on site weekly on active projects, and workers should expect to see them. Consistency builds trust; sporadic appearances feel like audits.
- Action follow-through is mandatory. If a worker raises a concern during an engagement walk and nothing changes, the program becomes actively harmful — it teaches workers that speaking up is pointless. Every concern raised must receive a documented response within a defined timeframe, even if the response is “we investigated and here’s why we can’t change this right now.”
Pro Tip: Train leaders to ask open-ended wellbeing questions during walks — not just safety compliance questions. “How’s your rotation going?” and “Are you getting enough rest between shifts?” open conversations that “Is your harness inspected?” never will. The best safety intelligence I have ever received came from a five-minute conversation with a scaffolder during a walkthrough — he told me three members of his crew were working through illness because they feared losing their contract. That single conversation triggered a fitness-for-duty review that identified two workers genuinely unfit for the tasks they were performing.
7. Workload Design and Job Demand-Control Balance
This is the initiative that most organizations skip because it requires them to challenge production assumptions. Workload design means deliberately structuring job demands, task variety, autonomy, and recovery time so that work is sustainable over the duration of a project or rotation — not just survivable.
The demand-control model, well-established in occupational health research, shows that high demands combined with low control is the most harmful work configuration for both psychological and physical health. Workers who face relentless pressure with no ability to influence how, when, or in what order they complete tasks are at significantly elevated risk for stress-related illness, musculoskeletal injury, and safety incidents.
Practical workload design controls that I have implemented on projects include:
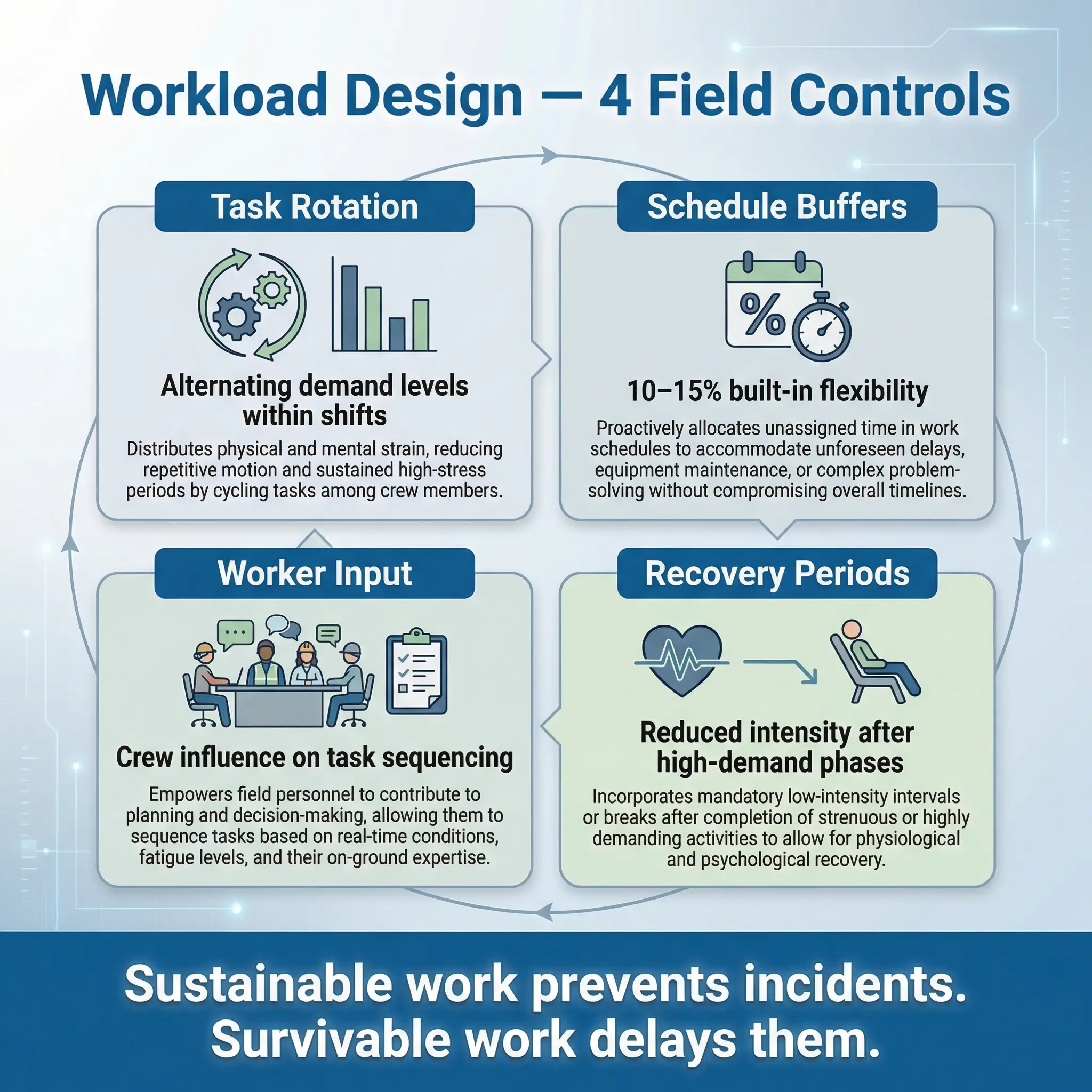
- Task rotation within crews. Alternating between physically demanding and lighter tasks across a shift reduces cumulative fatigue and repetitive strain exposure. On a steel erection project in Northern Europe, rotating ironworkers between connecting, bolting, and material staging cut musculoskeletal injury reports by 28% over a six-month period.
- Buffer time in schedules. Building 10–15% schedule buffer into daily work plans so that unexpected complications do not automatically trigger overtime or shortcut pressure. This is a leadership decision — and one that most project managers resist until they see the incident data from compressed schedules.
- Worker input on task sequencing. Allowing experienced workers to influence the order and method of task completion — within safety boundaries — increases their sense of control and reduces stress. It also tends to improve efficiency because experienced workers know the most practical sequence better than a planner sitting in an office.
- Recovery periods after high-demand phases. After a major shutdown, turnaround, or construction push, the immediate next rotation should have reduced intensity. Workers who go from a 60-hour turnaround week straight into another high-intensity phase accumulate fatigue debt that no amount of coffee can repay.
8. Critical Incident Stress Management (CISM)
When a serious incident occurs on site — a fatality, a major injury, a near-miss that could have killed someone — the psychological impact on witnesses, coworkers, and emergency responders is immediate and significant. Yet most emergency response plans cover medical treatment, incident investigation, and regulatory notification while completely ignoring the mental health of the people who were present.
Critical Incident Stress Management is a structured program for supporting workers psychologically after traumatic workplace events:
- Immediate defusing within hours. A brief, facilitated conversation within 4–8 hours of the event — not a formal debrief, but a structured check-in that normalizes acute stress reactions, provides basic coping information, and identifies anyone who may need immediate professional support.
- Formal psychological debrief within 48–72 hours. A longer, facilitated group session led by a trained CISM practitioner — not a supervisor, not an HR representative. The debrief follows a structured protocol that allows participants to process the event cognitively and emotionally in a safe, confidential environment.
- Follow-up screening at 2 weeks and 6 weeks. Most acute stress reactions resolve naturally within two weeks. Those that persist may indicate developing post-traumatic stress disorder or other conditions requiring clinical intervention. Structured follow-up catches this transition point.
- No mandatory participation. CISM sessions must be offered, strongly encouraged, and facilitated at convenient times — but never mandatory. Forcing traumatized workers into a group debrief can cause harm. The option to access individual support must always be available.
I coordinated CISM after a crane collapse on a construction project that killed one worker and seriously injured two others. Thirty-seven workers witnessed the event. Without the CISM program, the project would have expected those workers to return to their tasks the next day after a brief safety stand-down. Instead, the defusing session identified eight workers in acute distress, four of whom were stood down for 72 hours with full pay while receiving professional support. Two of those four were later diagnosed with acute stress disorder and received treatment that prevented chronic PTSD. The cost of the CISM program for that incident was less than 1% of the crane damage cost — and it preserved the mental health of eight workers who would otherwise have been expected to simply carry on.
9. Return-to-Work and Rehabilitation Programs
The way an organization handles injured or ill workers when they return to work is one of the clearest indicators of its genuine commitment to wellbeing. A good return-to-work program protects recovery, prevents re-injury, and demonstrates to every worker on site that the company values people beyond their productive output. A bad one — or the absence of one — sends the opposite message.
Effective return-to-work programs share several common elements that I have seen work consistently across industries:
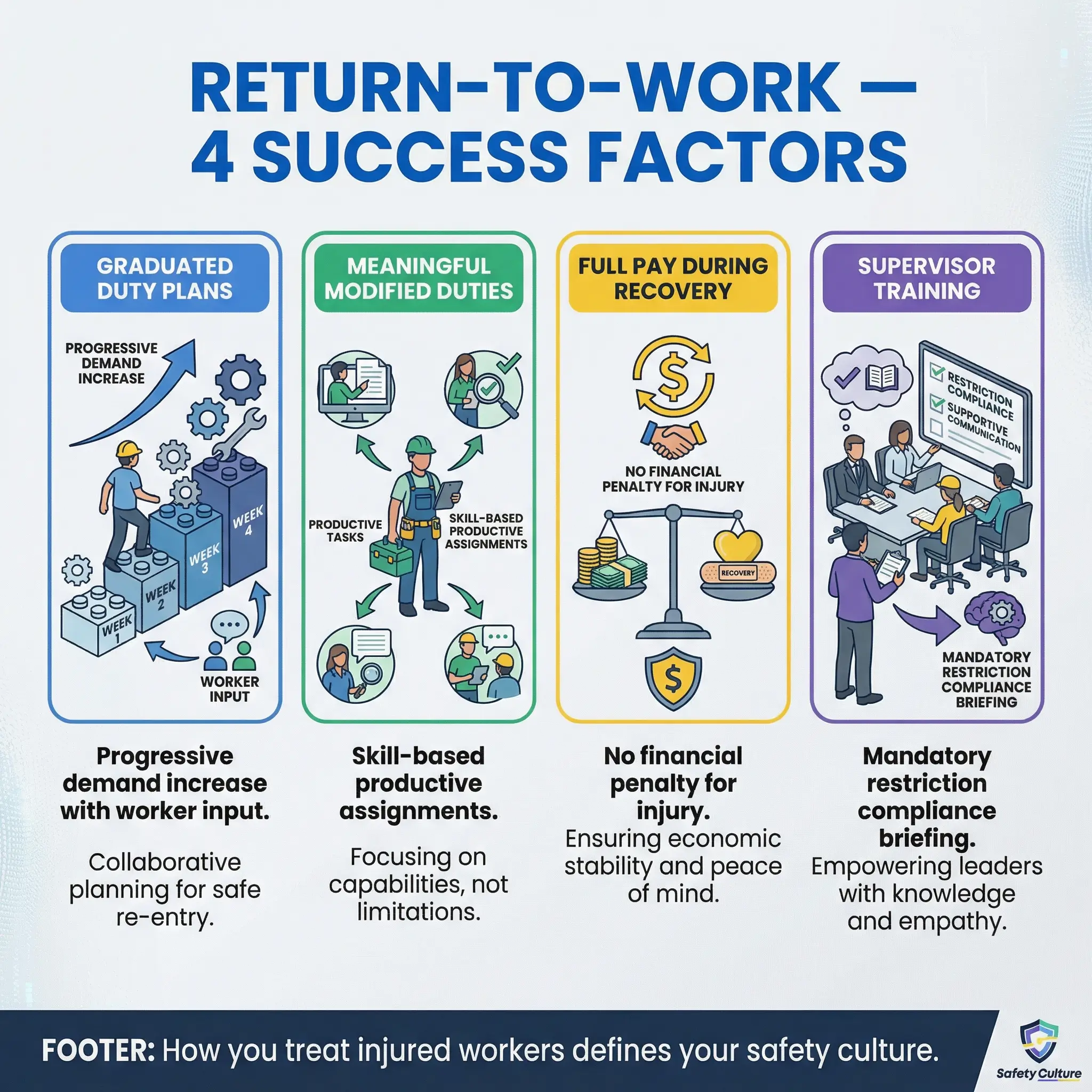
- Graduated duty plans developed with the worker. The returning worker, their treating physician, and the site HSE team jointly develop a task plan that progressively increases physical and cognitive demands over a defined period. The worker’s input is not optional — they know their body and their recovery better than anyone.
- Modified duties that are meaningful. Light duty must never mean humiliation. Giving an injured ironworker a chair and telling them to watch a gate destroys dignity and discourages other workers from reporting injuries. Modified duties should use the worker’s skills in a genuinely productive capacity — documentation review, toolbox talk delivery, quality inspections, mentoring.
- No financial penalty during recovery. Workers who lose income during return-to-work phases learn that getting injured has financial consequences — and the next time, they will hide the injury. Full pay during graduated return is a safety investment, not a cost.
- Supervisor training on return-to-work management. Supervisors must understand that a returning worker has medical restrictions that are non-negotiable — not suggestions. I investigated a re-injury case on a pipeline project where a supervisor assigned a returning worker to manual trenching because “he looked fine.” The worker re-ruptured a disc and required surgery. The supervisor had never been briefed on the return-to-work restrictions.
ILO Code of Practice on Managing Disability in the Workplace establishes that return-to-work programs should be initiated as early as medically appropriate, involve the worker in planning, and provide workplace accommodations that enable productive participation during recovery. [External Link: ILO — https://www.ilo.org/global/topics/disability-and-work]
Pro Tip: Track your return-to-work completion rate — the percentage of injured workers who successfully complete their graduated return plan without re-injury or dropout. This is a leading indicator of both wellbeing program quality and safety culture health. Anything below 80% signals a systemic problem in how your organization manages recovery.
10. Health Promotion and Preventive Screening Programs
The final initiative addresses a gap that most safety-focused organizations overlook entirely: the baseline physical health of their workforce. Occupational health surveillance catches work-related exposures, but it does nothing for the cardiovascular disease, diabetes, hypertension, and metabolic conditions that are prevalent in industrial workforces — and that directly affect fitness for duty, fatigue resilience, and incident risk.
Health promotion programs go beyond compliance-driven surveillance to proactively improve worker health through education, screening, and behavioral support:
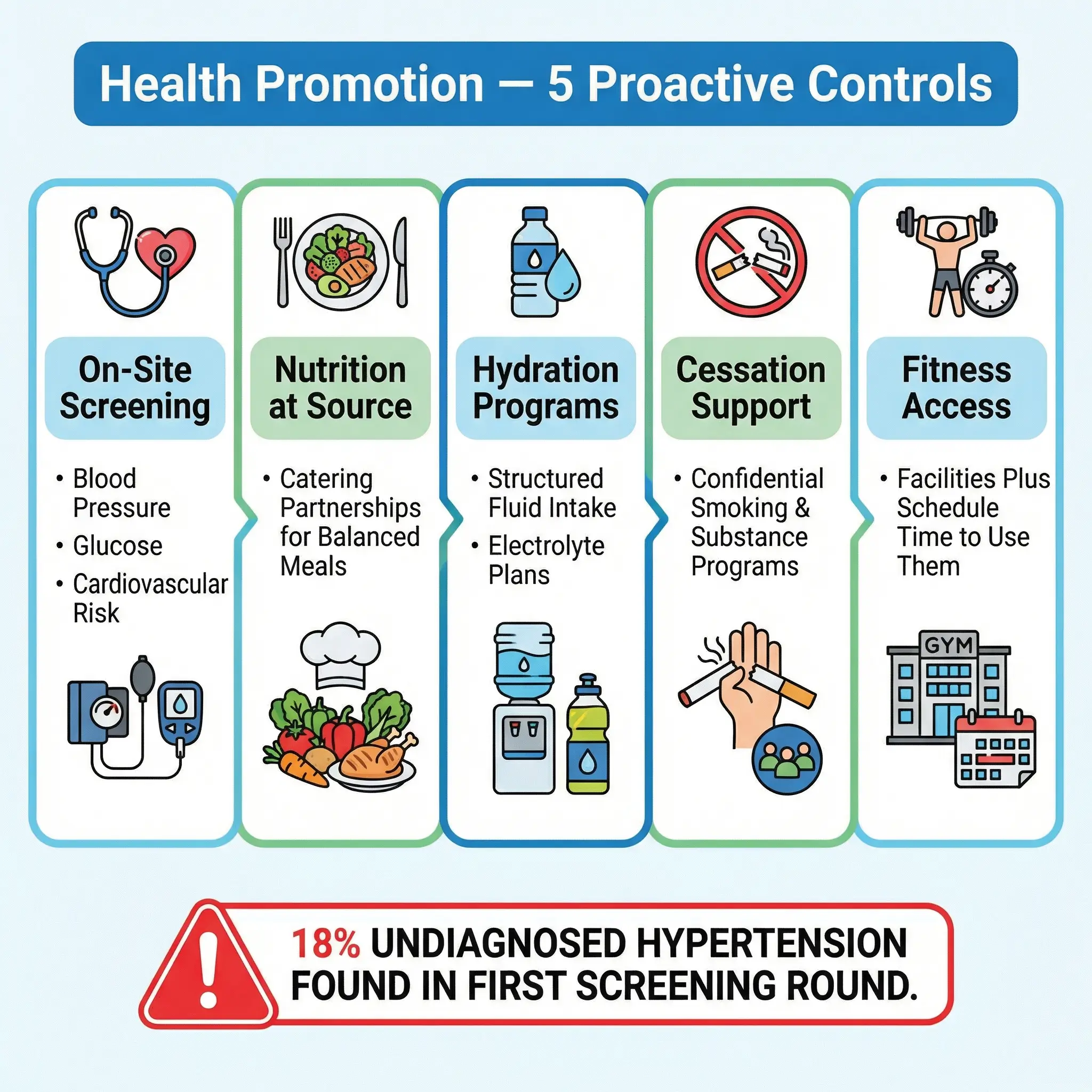
- On-site health screening campaigns. Blood pressure, blood glucose, cholesterol, BMI, and basic cardiovascular risk assessment offered voluntarily on site — during work hours, at no cost to the worker. I ran quarterly screening campaigns on a mining operation in Southern Africa that identified undiagnosed hypertension in 18% of the workforce during the first round. Several of those workers were operating heavy mobile equipment with blood pressure readings that put them at immediate risk of a cardiovascular event behind the wheel.
- Nutrition interventions at site catering facilities. Wellbeing programs that encourage healthy eating while serving deep-fried meals at the camp mess are self-defeating. Partner with catering providers to offer balanced meal options, provide nutritional information, and make healthy choices the easy default — not the hidden alternative at the end of the buffet line.
- Hydration and heat stress prevention programs. In hot climates, structured hydration programs with electrolyte supplementation, shaded rest areas, and work-rest cycle schedules are wellbeing fundamentals. These are not optional comforts — they are physiological controls against heat illness.
- Smoking cessation and substance awareness support. Offer voluntary, confidential programs with professional support — never punitive approaches. Workers who fear disciplinary action for disclosing substance use will never seek help.
- Physical activity facilitation. Provide basic fitness facilities on remote sites, organize voluntary group activities, and — critically — ensure that shift schedules leave enough recovery time for workers to actually use them. A gym that nobody has energy to visit is not a wellbeing initiative.
Why Most Wellbeing Programs Fail — And How to Prevent It
Understanding what works is only half the equation. Knowing why initiatives fail is equally critical, because the failure modes are consistent and avoidable. Every collapsed wellbeing program I have reviewed shares at least two of the same root causes.
The most common reasons wellbeing programs fail in industrial settings include:
- Treating wellbeing as an HR function, not an operational control. When wellbeing sits in HR, it competes with recruitment, payroll, and benefits administration for attention and budget. When it sits inside the HSE management system — integrated into HIRA, reported alongside safety KPIs, and reviewed in management meetings — it becomes part of how the operation runs.
- Launching too many initiatives at once. Organizations that roll out eight programs simultaneously dilute everything. Start with two or three initiatives that target your site’s most significant stressors, resource them properly, measure them, and expand only after demonstrating results.
- No baseline measurement. If you do not measure wellbeing indicators before launching a program, you cannot demonstrate impact afterward. Absenteeism rates, incident rates involving human factors, voluntary turnover, health surveillance findings, and anonymous wellbeing survey scores all provide baseline data.
- Leadership lip service without follow-through. A CEO who signs a wellbeing policy but never walks the site, never asks about wellbeing metrics, and never allocates budget beyond the minimum has not committed to wellbeing. Workers read actions, not policies.
- Ignoring the systemic causes of poor wellbeing. Yoga classes and meditation apps do not fix 14-hour shifts, abusive supervisors, or contract insecurity. Individual resilience programs layered on top of toxic systems are not wellbeing — they are burden-shifting.
| Failure Mode | What It Looks Like | What to Do Instead |
|---|---|---|
| HR-owned, not ops-integrated | Wellbeing discussed in HR meetings, absent from safety reviews | Integrate into OHSMS, report alongside TRIR/LTIFR |
| Too many initiatives at once | 8 programs launched, none resourced, all abandoned in 12 months | Start with 2–3 targeted programs, measure, then expand |
| No baseline data | “We think morale improved” with no supporting metrics | Establish KPIs before launch: absenteeism, incident rates, survey scores |
| Leadership lip service | Policy signed, zero site visibility, minimum budget | Mandate leadership engagement walks and wellbeing metric reviews |
| Individual focus, systemic ignore | Resilience training offered while rosters remain brutal | Address workload, roster design, and supervision quality first |
Measuring Wellbeing — Leading Indicators That Matter
You cannot manage what you do not measure, and wellbeing is no exception. The challenge is that traditional safety metrics — TRIR, LTIFR, DART — are lagging indicators that tell you about failures after they happen. Wellbeing measurement requires leading indicators that signal risk before incidents occur.
The following indicators have proven reliable across projects I have managed for tracking wellbeing program effectiveness:
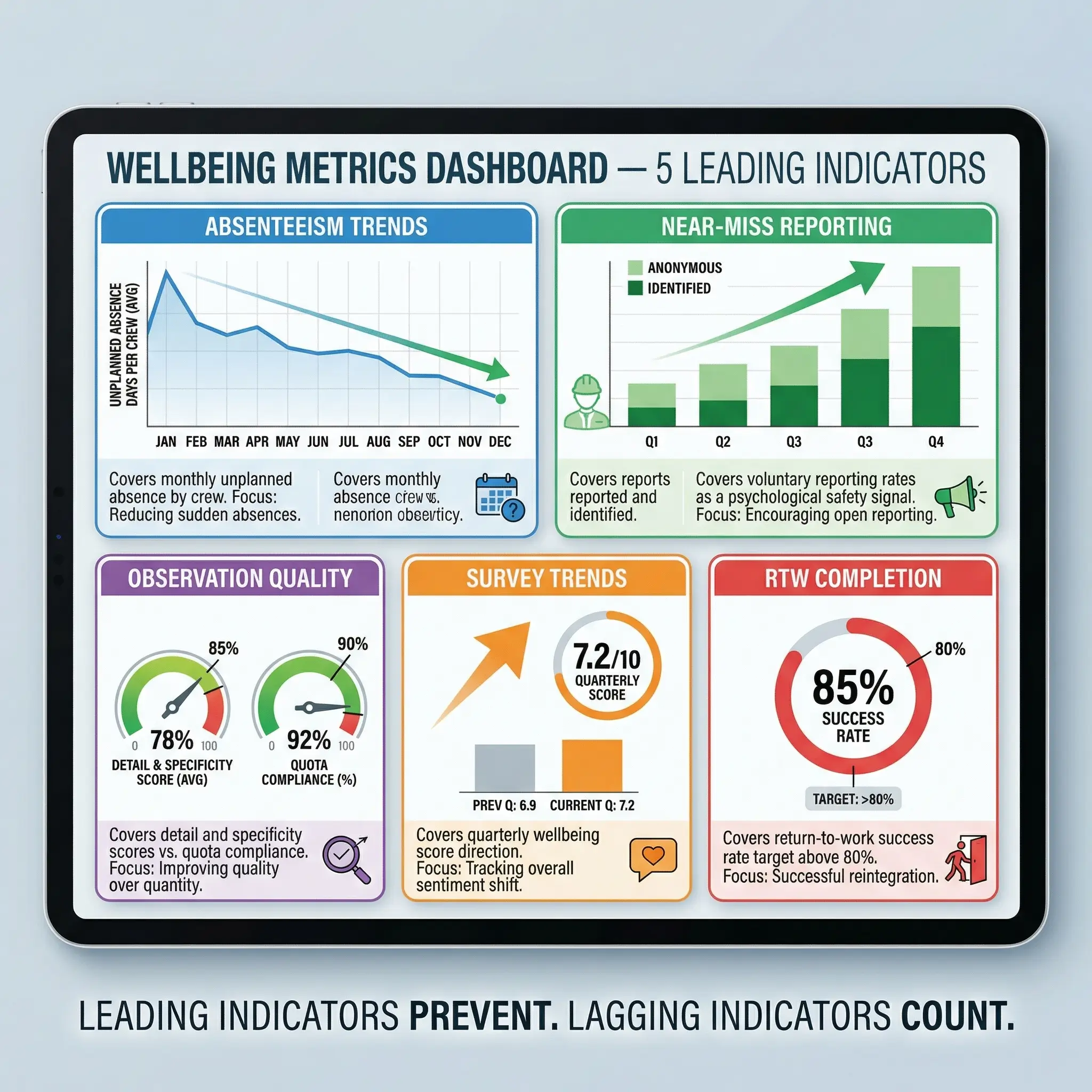
- Absenteeism trend analysis. Track unplanned absence rates monthly, broken down by department, crew, and rotation cycle. Rising absenteeism in a specific crew or during a specific rotation pattern is an early signal of stress, fatigue, or morale breakdown.
- Near-miss and hazard reporting rates. Workers who feel psychologically safe and physically well report more hazards — not fewer. A decline in voluntary reporting is a warning sign, not a success indicator.
- Safety observation quality scores. Not just count — quality. Are observation cards identifying real hazards with specific detail, or are they generic tick-box entries submitted to meet a quota? Quality reflects engagement; quantity reflects compliance pressure.
- Employee wellbeing survey scores. Anonymous, quarterly or biannual surveys covering workload, supervisor support, rest adequacy, mental health, and overall satisfaction. Trend the data over time — single snapshots are less useful than directional movement.
- Return-to-work completion rates. As noted earlier, this is a powerful proxy for how well the organization supports injured workers through recovery.
- Health surveillance findings trends. Are occupational health conditions (hearing loss, respiratory function decline, musculoskeletal complaints) stable, improving, or worsening? Trends in surveillance data reflect both exposure control and overall workforce health.
Pro Tip: Present wellbeing metrics alongside traditional safety metrics in every management review. When the project director sees TRIR, LTIFR, and wellbeing indicator trends on the same dashboard, wellbeing stops being a side conversation and becomes an integrated performance measure.
Conclusion
Workplace wellbeing initiatives work when they are designed as operational controls — integrated into the safety management system, measured against real outcomes, and backed by leadership who show up on site, not just on the policy signature page. The ten initiatives in this article are not theoretical frameworks. Every one of them has been tested on active construction sites, offshore platforms, refineries, and mining operations. Every one has produced measurable improvements in worker health, safety performance, or both. And every one failed somewhere else because an organization treated it as an HR decoration rather than a risk control.
The shift that needs to happen across high-risk industries is fundamental: psychosocial hazards belong in the HIRA register, fatigue belongs in the permit-to-work system, and mental health support belongs in the emergency response plan — not on a wellness poster in the break room. ISO 45003 has formalized this. EU psychosocial directives are tightening it. The regulatory direction is clear. Organizations that build genuine wellbeing systems now will be ahead of compliance requirements and — far more importantly — ahead of the incidents that unmanaged psychosocial risk inevitably produces.
No safety management system is complete if it controls the pressure in a pipeline but ignores the pressure on the person operating it. The workers who go home healthy at the end of every shift — physically, mentally, and emotionally — are the only KPI that ultimately matters. Build systems that protect the whole person, not just the parts of them that appear in a hazard register.