

TL;DR
- Wellbeing programs fail when they start with perks instead of data: Baseline your workforce health risks before selecting a single initiative.
- Link wellbeing directly to safety performance: Fatigued, stressed, and disengaged workers drive incident rates — not just absence rates.
- Start small with three to five measurable initiatives: Overambitious launches collapse within six months.
- Secure visible leadership commitment before day one: Programs without management participation become poster campaigns.
- Build feedback loops from the start: Quarterly pulse checks prevent your program from becoming irrelevant.
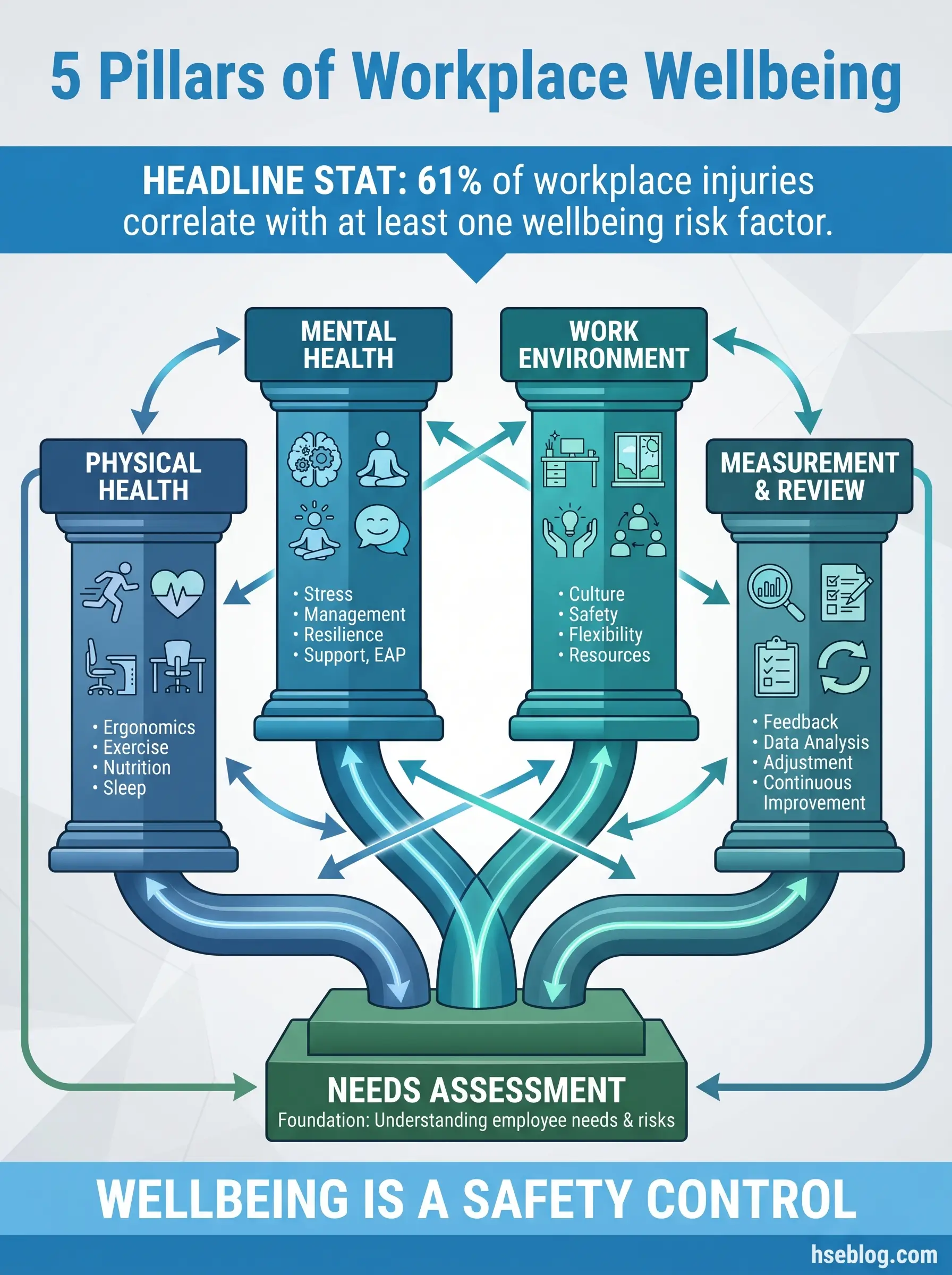
I was reviewing lost-time injury data at a logistics hub in Western Europe when something in the trend line caught my attention. Incident rates had climbed 22% over eight months — but nothing had changed operationally. Same routes, same fleet, same shift patterns. The investigation took me somewhere I wasn’t expecting: a workforce survey buried in HR’s filing system. Sixty-one percent of drivers reported poor sleep quality. Forty-three percent described their stress levels as “high” or “very high.” The injuries weren’t an operations problem. They were a wellbeing problem hiding behind safety metrics.
That experience reshaped how I approach occupational health management. A workplace wellbeing program isn’t a nice-to-have benefit sitting alongside gym discounts and fruit baskets. It’s a frontline risk control. Workers who are physically depleted, mentally distracted, or emotionally disengaged make the kind of errors that show up in your LTIFR, your near-miss register, and — in the worst cases — your fatality statistics. This article walks through exactly how to create a workplace wellbeing program from scratch, from the initial needs assessment through to sustained measurement and improvement. Every step is drawn from programs I’ve built or audited across construction, oil and gas, manufacturing, and healthcare operations.
Why Workplace Wellbeing Programs Are a Safety Imperative
The business case for wellbeing is well-documented, but most HSE professionals don’t need another ROI slide. What they need is a clear line between wellbeing failures and safety outcomes. That connection is direct, measurable, and consistently underestimated.
The evidence linking poor worker wellbeing to elevated incident rates is not theoretical — it shows up in every post-incident investigation I’ve conducted where human factors played a role. Consider what actually happens on the ground:
- Fatigued workers miss critical cues. A crane banksman operating on four hours of sleep doesn’t see the tag line drift. A process operator fighting chronic pain skips a gauge reading because standing hurts. These are not carelessness — they’re predictable failures from depleted people.
- Chronic stress narrows decision-making. Workers under sustained psychological pressure default to shortcuts. They lose the cognitive bandwidth to assess dynamic risk properly. I’ve watched experienced operators walk past obvious trip hazards during periods of high organizational stress — their attentional capacity was simply saturated.
- Disengagement erodes safety culture. When workers feel unsupported, they stop reporting near-misses. They stop challenging unsafe conditions. The reporting pipeline dries up, and leadership misreads silence as compliance.
- Musculoskeletal disorders drive presenteeism. A worker with untreated lower back pain doesn’t take sick leave — they modify their lifting technique in ways that create new hazards for themselves and their crew.
ISO 45001 Clause 6.1.2.1 requires organizations to identify hazards related to “work organization” — including workload, working hours, and psychosocial factors. A wellbeing program is not separate from your safety management system. It belongs inside it.
Pro Tip: If your incident investigation template doesn’t include questions about sleep quality, stress levels, and personal wellbeing, you’re missing a root cause category that may account for 30% or more of your human factor findings.
Step 1 — Conduct a Workforce Wellbeing Needs Assessment
Every failed wellbeing program I’ve audited shares one origin story: someone in management picked initiatives based on what sounded good in a meeting. Yoga classes at a refinery. Mindfulness apps for night-shift workers. These aren’t bad ideas in isolation — they’re bad ideas when they don’t match the actual health risks of the actual workforce. A proper needs assessment prevents this mismatch.
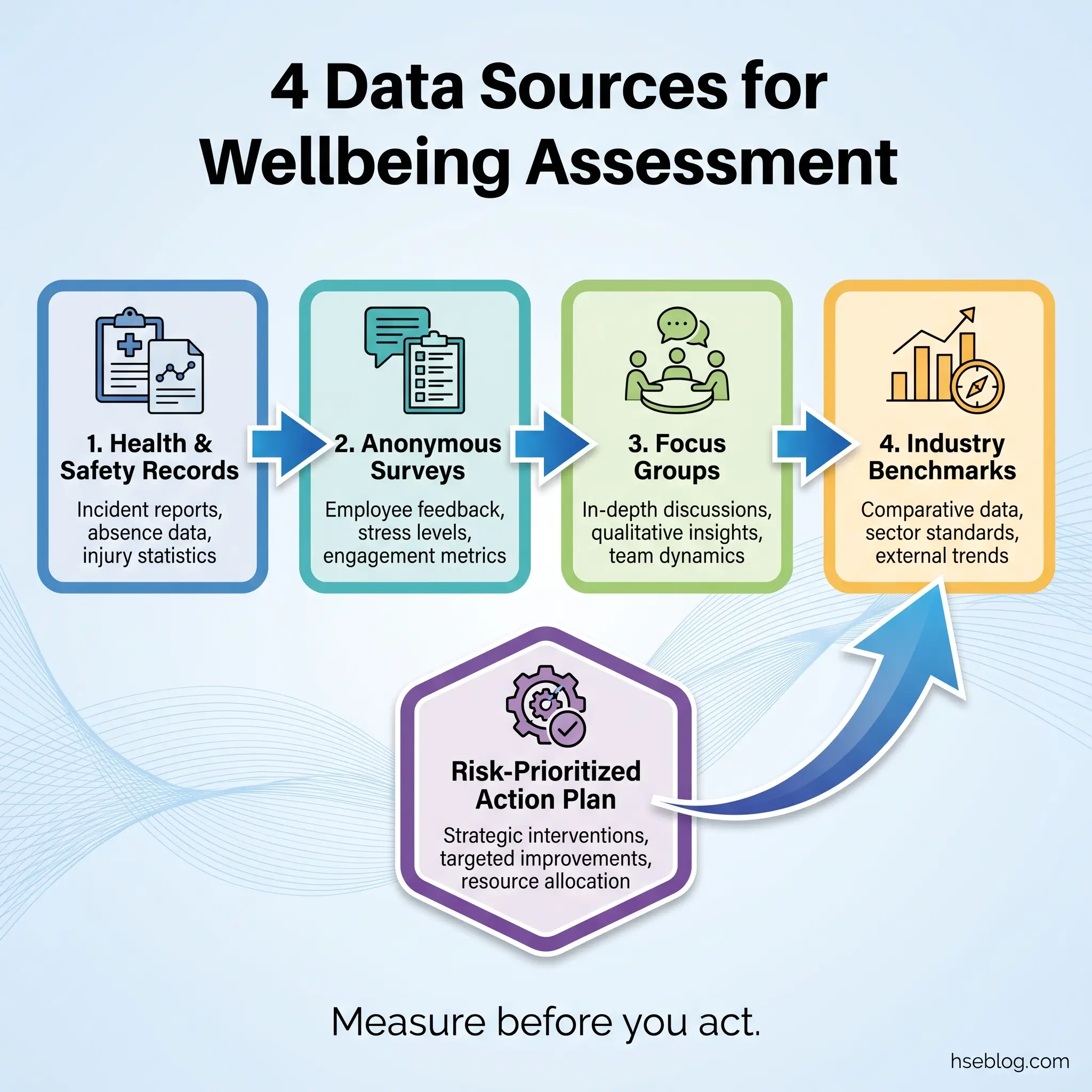
The assessment should combine quantitative data with qualitative insight, drawn from multiple sources to avoid single-source bias. Here’s the process I’ve used successfully across four industries:
- Pull existing health and safety data. Review sickness absence records, occupational health referrals, EAP utilization rates, incident reports flagging fatigue or human error, workers’ compensation claims by injury type, and any prior health surveillance results. Look for patterns, not individual cases.
- Distribute an anonymous wellbeing survey. Cover five domains: physical health (pain, sleep, fitness), mental health (stress, anxiety, mood), work-life balance (hours, commute, recovery time), job satisfaction (workload, autonomy, management support), and workplace environment (noise, temperature, ergonomics). Keep it under 30 questions.
- Conduct focus groups or confidential interviews. Surveys tell you what — conversations tell you why. Facilitate small groups by shift pattern, department, or job role. Ask open questions: “What makes it hard to stay healthy while working here?”
- Benchmark against industry norms. Compare your findings against published health data for your sector. A 15% musculoskeletal complaint rate might sound high until you discover the industry average is 22% — or until you discover it’s 8%.
- Map findings to the risk register. This is the step most organizations skip. Every wellbeing finding with a plausible link to safety performance should be captured as a health risk, assessed for severity and likelihood, and prioritized alongside traditional hazards.
The influence of personal factors on health and safety is well-documented in occupational health literature — individual lifestyle, sleep patterns, and coping mechanisms directly affect a worker’s capacity to perform safely. Your needs assessment must capture these personal dimensions without crossing into invasive territory.
Pro Tip: Run the survey during mid-shift, not at the end of a Friday. Response quality drops dramatically when people are rushing to leave. Allocate 15 minutes of paid time specifically for completion, and watch your participation rate climb above 70%.
Step 2 — Define Clear Objectives Linked to Safety Outcomes
A wellbeing program without measurable objectives becomes a permanent pilot project — always running, never evaluated, quietly consuming budget until someone in finance asks what it actually does. I’ve seen this exact scenario play out at a manufacturing plant in Central Europe where a wellbeing initiative ran for three years without a single defined KPI. When the new operations director asked for results, no one could produce a number.
Your objectives must tie wellbeing improvements to outcomes the business already tracks. This keeps the program visible, fundable, and defensible during budget reviews.
Effective objectives follow a specific structure — each one connects a wellbeing input to a measurable safety or operational output:
- Reduce fatigue-related incidents by 15% within 12 months by implementing structured rest break schedules and fatigue risk management training.
- Decrease musculoskeletal disorder referrals by 20% over 18 months through proactive ergonomic assessments and early intervention physiotherapy.
- Improve mental health disclosure rates by 25% within the first year by training supervisors in mental health first aid and normalizing EAP access.
- Achieve 80% workforce participation in at least one wellbeing initiative within six months of launch.
- Reduce sickness absence rate from 5.2% to 4.0% within two years by addressing the top three health risk factors identified in the needs assessment.
| Objective Type | Example Metric | Data Source | Review Frequency |
|---|---|---|---|
| Safety-linked | Fatigue-flagged incident rate | Incident database | Monthly |
| Health-linked | MSD referral rate | Occupational health records | Quarterly |
| Engagement-linked | Wellbeing survey participation | HR platform | Per survey cycle |
| Culture-linked | Near-miss reporting rate | Safety reporting system | Monthly |
| Absence-linked | Sickness absence % | Payroll / HR system | Monthly |
HSE UK’s HSG65 framework — Plan, Do, Check, Act — applies to wellbeing programs just as it applies to any health and safety management process. Set targets, implement controls, measure outcomes, and revise.
Step 3 — Secure Leadership Commitment and Budget
Here’s a pattern I’ve seen repeat across three continents: an HSE manager builds a solid wellbeing proposal, presents it to leadership, gets verbal approval, and then receives zero budget, no dedicated headcount, and a suggestion to “integrate it into existing activities.” That’s not commitment. That’s delegation disguised as support.
Genuine leadership commitment for a workplace wellbeing program requires visible, specific, and sustained actions. Without it, workers see the program as performative — and they’re usually right. I’ve learned that getting leadership buy-in requires speaking their language, which means framing wellbeing as a risk control with financial consequences.
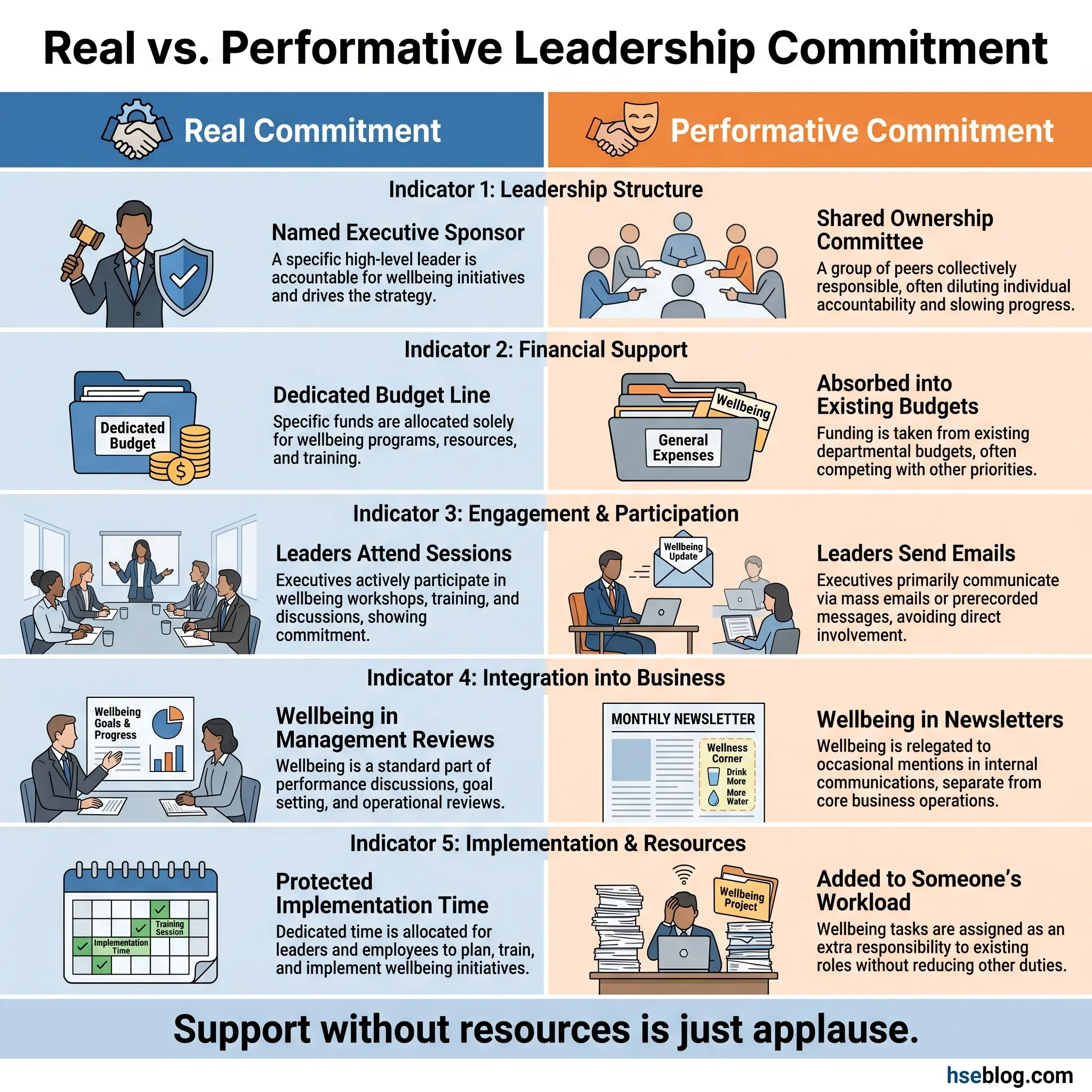
The following elements distinguish real commitment from cosmetic endorsement:
- Named executive sponsor. One senior leader accountable for the program’s success — not a committee, not “shared ownership,” one person whose performance review includes wellbeing outcomes.
- Dedicated budget line. Even a modest allocation signals seriousness. A wellbeing budget buried inside “general HSE” or “HR initiatives” disappears during Q3 reforecasting.
- Leadership participation in wellbeing activities. When the operations director attends a stress management workshop alongside frontline crew, it sends a signal that no poster campaign can replicate.
- Wellbeing metrics included in management reviews. If your monthly HSE review covers LTIFR, near-misses, and audit scores but never mentions sickness absence trends or EAP usage, wellbeing isn’t part of your management system — it’s an accessory.
- Protected time for implementation. The HSE team or wellbeing coordinator needs ring-fenced hours. Bolting wellbeing onto someone’s already-overloaded role guarantees shallow execution.
Pro Tip: Present the business case using your own data from the needs assessment — not generic statistics from external reports. When you show leadership that their specific workforce has a 43% high-stress rate correlating with a 22% rise in incidents, the conversation changes from “nice to have” to “when do we start.”
Step 4 — Design the Program Around Your Workforce’s Actual Risks
This is where the needs assessment pays off. Instead of browsing a catalogue of generic wellbeing offerings, you’re selecting interventions that directly target the health risks your workforce actually faces. A wellbeing program for offshore rotation workers looks nothing like one for hospital nursing staff, which looks nothing like one for warehouse logistics teams.
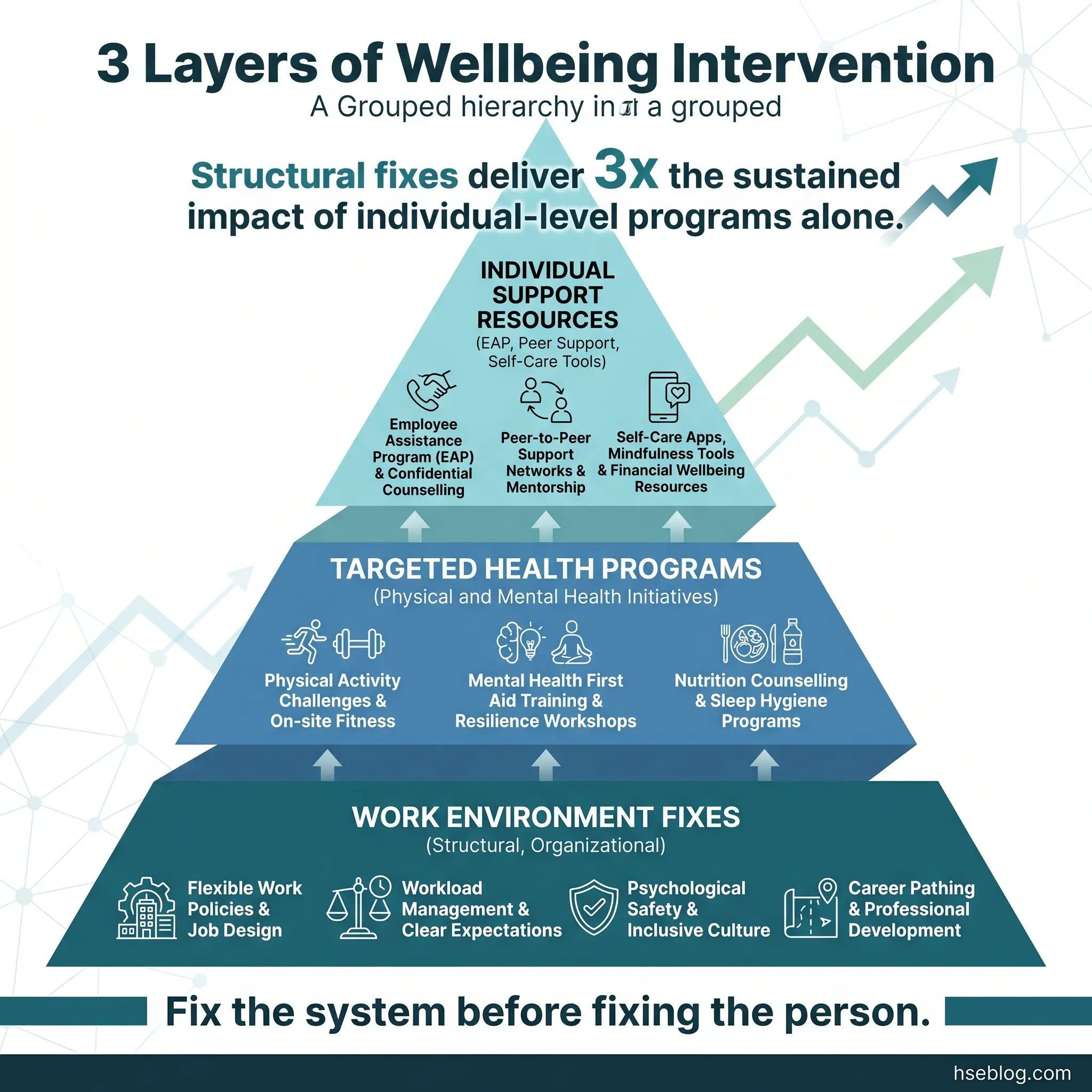
Physical Wellbeing Interventions
Physical health initiatives should address the specific musculoskeletal, cardiovascular, and fatigue risks identified in your data. Generic gym memberships are the lowest-impact option because uptake in high-risk industries rarely exceeds 15%.
Higher-impact alternatives include:
- On-site physiotherapy or occupational health clinics. Pre-shift screening and early intervention for musculoskeletal discomfort reduces the progression from minor strain to chronic disorder. I’ve seen this single measure cut MSD-related restricted duty cases by 35% at a steel fabrication facility.
- Structured fatigue management programs. Shift-specific sleep hygiene training, nap room access for night workers, and fatigue risk scoring integrated into pre-start checks. Effective breaks and rest periods combat employee fatigue more reliably than any wellness app.
- Nutritional support aligned to shift patterns. Healthy meal options available at 2 a.m. for night shift crews — not just during daytime canteen hours. At one oil and gas facility in the Gulf, switching the night-shift catering contract reduced gastrointestinal complaints by 40%.
- Pre-employment and periodic health surveillance. Baseline and ongoing health monitoring catches emerging conditions before they become safety-critical. This is a legal requirement in many jurisdictions under occupational health regulations, but it also generates the longitudinal data your program needs to evolve.
Mental Health and Psychosocial Interventions
Mental health at work remains the area where most wellbeing programs fall short — not because organizations don’t care, but because they default to passive resources (posters, hotlines, leaflets) instead of active, integrated interventions.
Effective mental health components require a layered approach:
- Supervisor mental health literacy training. Front-line supervisors are the early warning system. They notice behavioral changes before anyone else — if they know what to look for. A two-hour training module covering recognition, response, and referral pathways is one of the highest-value investments in any wellbeing program.
- Peer support networks. Trained peer supporters — not therapists, not counselors, but colleagues equipped with listening skills and referral knowledge — normalize help-seeking in cultures where mental health stigma runs deep. These programs have been particularly effective on construction mega-projects.
- Psychosocial risk assessment integrated into the SMS. Workload, job control, social support, role clarity, organizational change — these six factors drive psychosocial harm. Assess them systematically, not anecdotally.
- Confidential EAP with proactive promotion. An EAP that nobody knows about is an EAP that nobody uses. Utilization rates below 5% indicate a visibility problem, not a need problem.
Work Environment and Organizational Factors
Sometimes the most impactful wellbeing intervention isn’t a program — it’s fixing the working conditions that erode wellbeing in the first place.
These structural changes often deliver more sustained improvement than any standalone initiative:
- Noise reduction and thermal comfort improvements. Workers exposed to sustained noise above 80 dB(A) or temperatures outside the 16–24°C comfort range experience chronic physiological stress that compounds psychological strain.
- Workload rebalancing. If your overtime data shows one crew consistently working 60+ hours while another averages 42, the problem isn’t individual resilience — it’s resource allocation. Fix the schedule before launching stress workshops.
- Communication and consultation improvements. Workers who feel heard are measurably more engaged and report higher wellbeing scores. Effective communication methods in health and safety aren’t just about conveying rules — they’re about creating dialogue.
- Bullying and harassment zero-tolerance enforcement. Signs of a toxic workplace — exclusion, intimidation, favoritism — are wellbeing destroyers that no amount of individual-level programming can overcome.
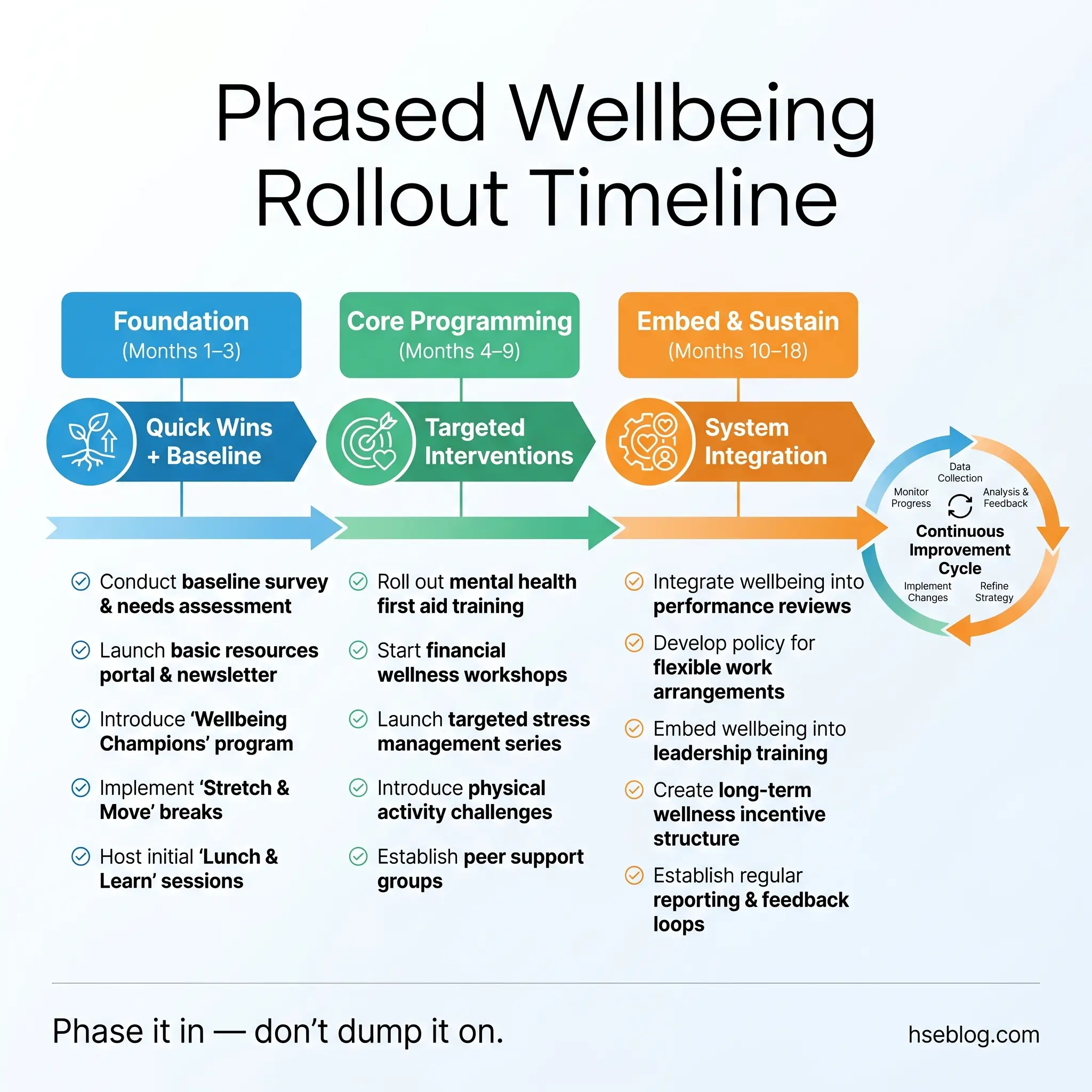
Step 5 — Build the Implementation Roadmap
A common failure mode is launching everything at once. I’ve watched organizations announce twelve wellbeing initiatives simultaneously, create a beautiful intranet page, and then watch participation crater within eight weeks because nobody could remember what was available or how to access it. Phased implementation with clear milestones works. Everything-at-once launches don’t.
The roadmap below reflects a sequencing strategy I’ve refined across multiple program launches:
Phase 1 — Foundation (Months 1–3)
The first phase establishes infrastructure and quick wins that build credibility:
- Appoint a wellbeing coordinator or champion network. This person (or team of volunteer champions across departments) owns the day-to-day execution. Without a named owner, actions drift.
- Launch two to three high-visibility, low-barrier initiatives. Pick items from your needs assessment that are easy to implement and immediately noticeable. Free fruit in break rooms. Stretch-and-flex programs before shifts. A mental health awareness poster campaign with QR codes linking to the EAP.
- Train all supervisors in wellbeing basics. A 90-minute session covering what the program is, what’s expected of them, and how to refer a worker who’s struggling. This is non-negotiable — supervisors who don’t understand the program will undermine it.
- Establish baseline metrics. Record current sickness absence rates, incident rates with human factor tags, EAP utilization, and the first wellbeing survey scores. These are your “before” numbers.
Phase 2 — Core Programming (Months 4–9)
This phase delivers the substantive interventions identified in your needs assessment:
- Roll out targeted health programs (physiotherapy, fatigue management, ergonomic assessments) in priority order based on risk ranking.
- Activate mental health peer support networks with trained volunteers and clear referral pathways.
- Integrate wellbeing checks into existing safety processes — toolbox talks, pre-start meetings, permit briefings.
- Launch a mid-point pulse survey at month six to assess awareness, participation, and early satisfaction.
Phase 3 — Embed and Sustain (Months 10–18)
The final phase transitions from “program” to “business as usual”:
- Incorporate wellbeing metrics into the formal management review cycle. This is the moment the program stops being a project and becomes part of the management system.
- Conduct the second full wellbeing survey and compare against baseline.
- Refine or retire underperforming initiatives. If nobody uses the mindfulness app after nine months, stop funding it and redirect resources to something workers actually want.
- Celebrate and communicate results. Share improvements in incident rates, absence figures, and participation data. Workers need to see that their engagement produced measurable change.
Pro Tip: Attach at least one wellbeing topic to every safety toolbox talk. Not as an add-on — as a standing agenda item. Over twelve months, this normalizes wellbeing conversations more effectively than any standalone campaign.
Step 6 — Measure, Review, and Continuously Improve
Measurement is where wellbeing programs either mature into permanent organizational capabilities or fade into forgotten initiatives. I’ve audited programs that ran for years without a single data review — the coordinator could describe activities but couldn’t name a single outcome. That’s an activity log, not a management system.
Your measurement framework needs leading indicators (inputs and process measures) and lagging indicators (outcome measures) — the same dual-indicator approach you already use for safety performance.
Leading indicators tell you whether the program is active and reaching workers:
- Participation rates per initiative, segmented by department, shift, and seniority
- Supervisor referral rates to EAP or occupational health
- Toolbox talk coverage for wellbeing topics
- Training completion rates for mental health literacy and fatigue awareness
- Wellbeing champion activity logs — are champions actually facilitating, or did the role go dormant?
Lagging indicators tell you whether the program is producing results:
- Sickness absence rate trend (overall and by category — MSD, mental health, respiratory)
- Incident rate with human factor tag filtering (fatigue, distraction, stress-related)
- Workers’ compensation claim frequency and cost
- Staff turnover in high-risk roles
- Wellbeing survey scores compared against baseline and industry benchmarks
| Indicator Type | Metric | Target Direction | Review Cycle |
|---|---|---|---|
| Leading | EAP utilization rate | Increase (indicates access, not distress) | Quarterly |
| Leading | Supervisor referral count | Increase in Year 1, stabilize in Year 2 | Monthly |
| Lagging | MSD-related restricted duty cases | Decrease | Quarterly |
| Lagging | Fatigue-flagged incidents | Decrease | Monthly |
| Lagging | Annual wellbeing survey — stress domain | Improve by 10%+ over baseline | Annually |
The Plan-Do-Check-Act cycle in ISO 45001 Clause 10.3 applies directly: use your review data to identify what’s working, what’s underperforming, and what emerging risks need new interventions. A static wellbeing program is already a failing one.
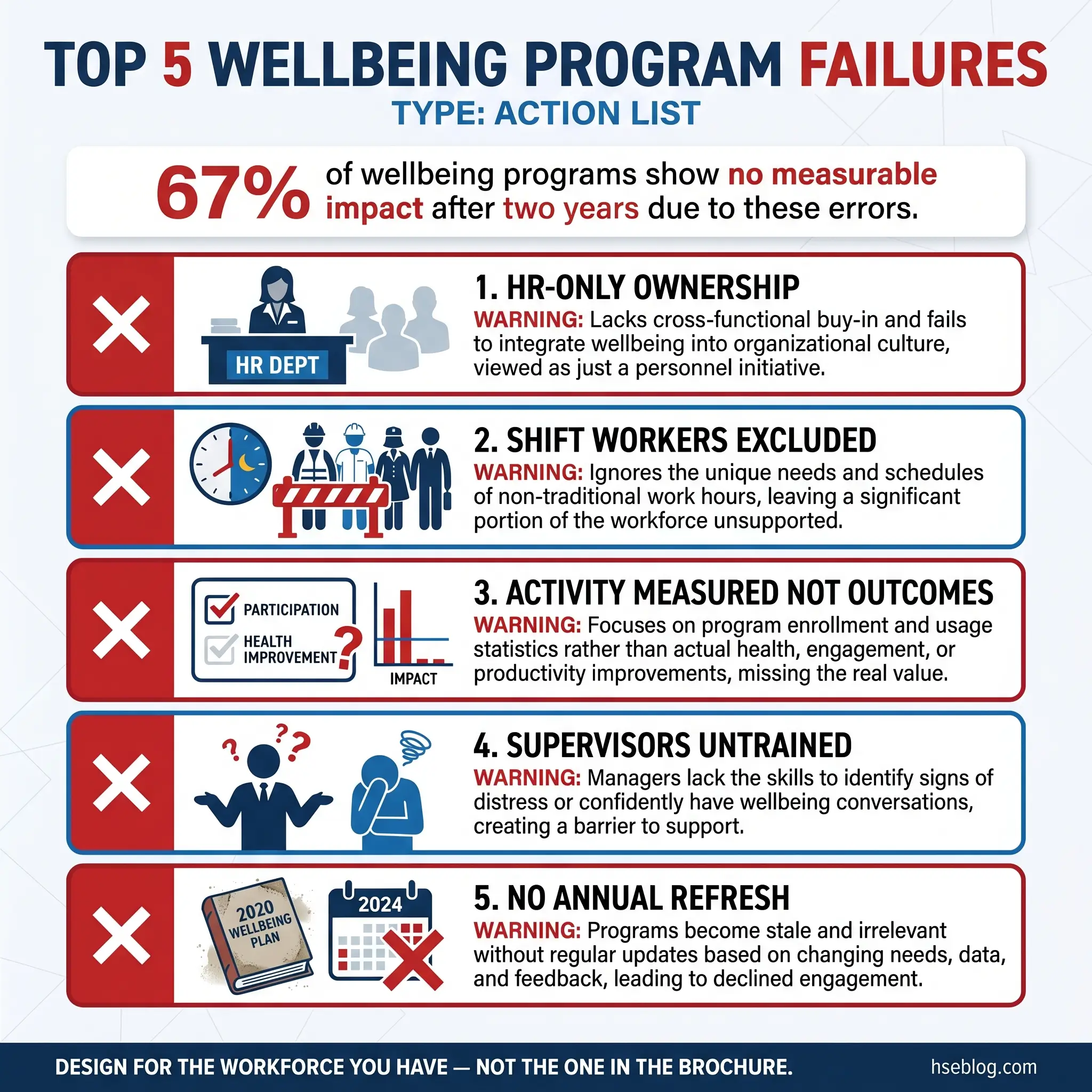
Common Mistakes That Derail Wellbeing Programs
Even well-designed programs can fail if these recurring errors aren’t anticipated and blocked. Every mistake on this list comes from a real program I’ve either managed or assessed — none are hypothetical.
The following failures are the most frequent and most damaging:
- Treating wellbeing as HR’s territory. If the program sits entirely within HR, it never integrates with the safety management system. Wellbeing affects safety outcomes — it must live where safety lives.
- Ignoring shift workers in program design. Initiatives scheduled during office hours exclude the workforce segment with the highest fatigue and isolation risk. Every activity must have a shift-accessible version.
- Confusing activity with impact. Running 30 wellbeing sessions per year means nothing if sickness absence hasn’t moved. Measure outcomes, not effort.
- Launching without supervisor training. Supervisors who don’t understand the program will dismiss it, mock it, or ignore disclosures. They are the program’s most critical enablers — or its most effective saboteurs.
- Over-relying on digital solutions. Wellness apps suit desk-based workers. A welder on a scaffold at 40 meters doesn’t check a mental health app during a break. Match the delivery method to the operational context.
- Failing to refresh the program annually. Workforce risks change. New contracts bring new demographics. Organizational restructures create psychosocial strain. A program built on last year’s data is already falling behind.
Conclusion
Creating a workplace wellbeing program from scratch demands the same rigor you’d apply to any safety-critical management system — needs assessment, objective-setting, resource allocation, implementation planning, and continuous measurement. The programs that fail are the ones built on assumptions instead of data, championed by posters instead of leaders, and measured by activities instead of outcomes. The programs that succeed become embedded into the operational rhythm of the organization, visible in management reviews, referenced in toolbox talks, and felt on the shop floor.
The hardest part isn’t designing the program — it’s sustaining the discipline to keep measuring, keep listening, and keep adjusting. Worker wellbeing isn’t a fixed state. It shifts with workload, with seasons, with organizational change, and with personal circumstances. A wellbeing program that stopped evolving twelve months ago is no longer serving its workforce.
Every incident investigation that traces back to fatigue, stress, distraction, or disengagement is a reminder that wellbeing isn’t a soft initiative bolted onto the side of your safety system. It’s a control measure. Treat it like one — resource it, inspect it, review it, and hold it to the same accountability standard as every other barrier between your people and harm.