

TL;DR
- Baseline first, annual after: OSHA requires a baseline audiogram within 6 months of first noise exposure at or above 85 dBA TWA, then annual testing every 12 months per employee — not per facility calendar.
- UK schedule differs significantly: Under L108, baseline audiometry is followed by annual tests for two years, then every three years unless hearing deterioration is detected.
- Standard Threshold Shift (STS) triggers a chain of actions: A 10 dB average shift at 2000, 3000, and 4000 Hz requires employee notification within 21 days, HPD refitting, retraining, and potential OSHA 300 Log recording.
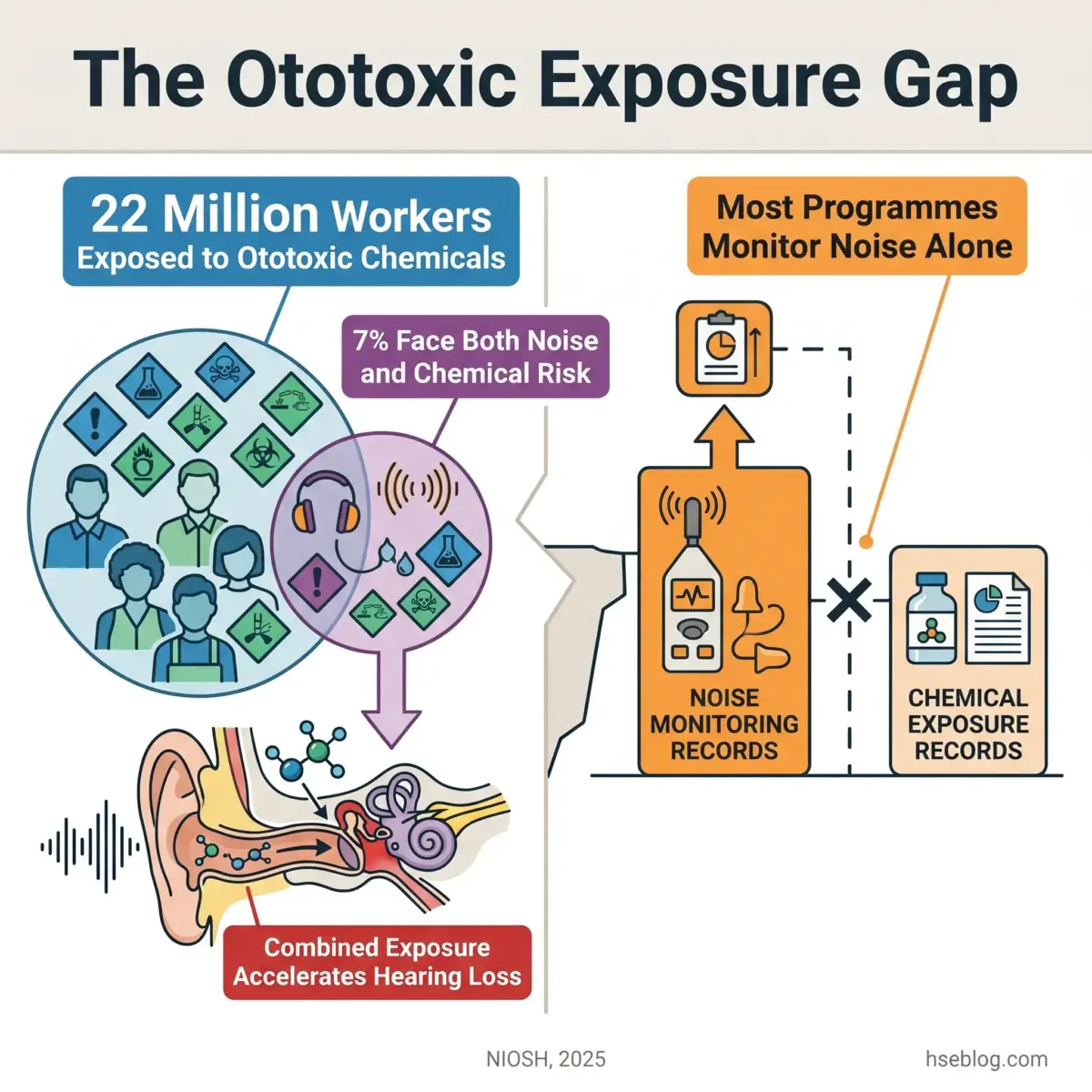
- Ototoxic chemicals accelerate hearing loss beyond noise alone: Approximately 13% of US workers are exposed to ototoxic chemicals (NIOSH, 2025), yet most hearing conservation programmes ignore chemical co-exposure entirely.
- Boothless audiometry is now validated and OSHA-compliant: Peer-reviewed research confirms clinical equivalence to booth-based testing when ambient noise is controlled.
Audiometric testing frequency depends on jurisdiction. Under OSHA (US), a baseline audiogram is required within 6 months of first noise exposure at or above 85 dBA, followed by annual tests every 12 months. Under UK regulations (L108), baseline testing is followed by annual audiometry for the first two years, then every three years unless problems are detected. EU Directive 2003/10/EC leaves specific frequency to member states but mandates health surveillance above 85 dB(A).
This article provides general HSE and occupational health knowledge. Content covering audiometric testing, hearing threshold interpretation, and health surveillance is for HSE practitioner reference. It is not medical advice. Workers with specific symptoms, hearing concerns, or exposure questions should consult a qualified audiologist or occupational health physician for individual assessment.
Approximately 22 million US workers face potentially damaging noise levels every year (CDC/NIOSH, current). Among adults aged 20–69 who report five or more years of exposure to very loud occupational noise, roughly 18% have bilateral speech-frequency hearing loss — compared to just 5.5% among those with no occupational noise exposure (NIDCD, current). These figures represent permanent, irreversible damage that developed silently while workers reported no symptoms.
Audiometric testing exists to catch that silent progression before it becomes disabling. This article covers the full scope of workplace audiometry — what triggers the requirement, how testing schedules differ across the US, UK, and EU, what a standard threshold shift means and what must happen after one is identified, and why the most dangerous gap in most hearing conservation programmes is not the test itself but everything that should follow it. The primary keyword driving this piece — audiometric testing — reflects a search from professionals who need both the regulatory rationale and the operational detail to run these programmes correctly.
What Is Audiometric Testing and Why Does It Matter in the Workplace?
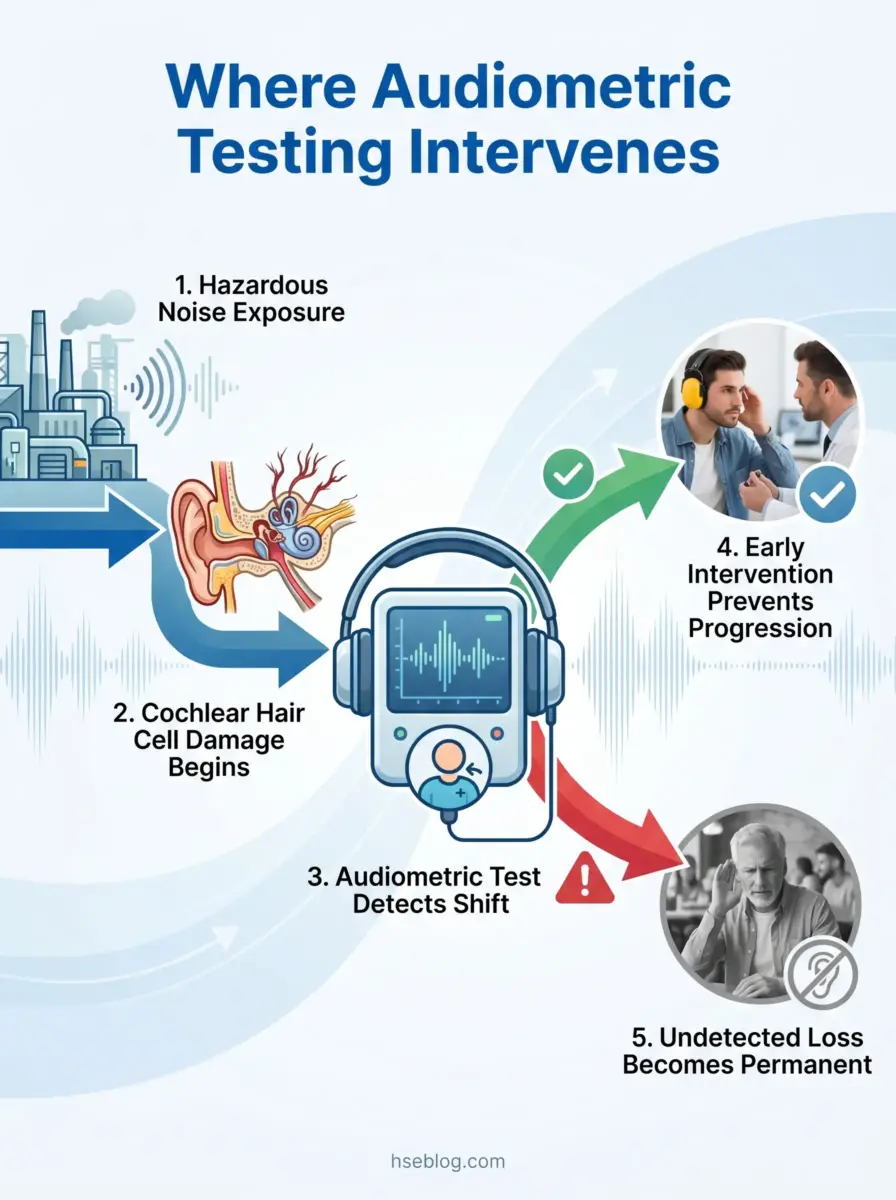
Audiometric testing is a pure-tone air-conduction measurement of hearing thresholds across specified frequencies, and it remains the only objective method for detecting hearing shifts before a worker notices any subjective change.
Noise-induced hearing loss is cumulative, permanent, and initially painless. Cochlear hair cells, once damaged, do not regenerate. Workers rarely self-report hearing difficulty until the loss has progressed well beyond the point of early intervention. That characteristic delay is precisely what makes periodic audiometric testing non-negotiable in any noise-exposed workplace.
The test serves two distinct purposes:
- Individual protection: Detecting threshold shifts early enough to adjust controls, refit hearing protection, or refer a worker for clinical evaluation before further damage accumulates.
- Programme evaluation: Aggregate audiometric trend data across a workforce reveals whether noise controls and hearing protection device (HPD) programmes are actually working — or simply present on paper.
A consistent pattern across hearing conservation programmes is that employers treat audiometric testing as a compliance checkbox. The annual test gets scheduled, results get filed, and no one systematically reviews whether STS rates in a given department are climbing. The real diagnostic power of audiometric testing is the trend line across a workforce over years, not the pass/fail status of any individual audiogram.
When aggregate data shows a cluster of threshold shifts in one production area, it signals that engineering controls may be insufficient, HPD selection may be wrong, or fit-testing is failing. That feedback loop — from individual audiograms to programme-level intervention — separates a compliant programme from an effective one.
Who Needs Audiometric Testing? Noise Exposure Triggers Across Jurisdictions
The threshold that triggers mandatory audiometric testing is not universal — it differs by jurisdiction, and applying the wrong standard is a common compliance failure for multinational employers.
All three major regulatory frameworks agree that workers exposed to hazardous noise need audiometric health surveillance. Where they diverge is the exposure level that activates the requirement and the scope of protection offered to workers between the lower and upper action thresholds.
| Requirement | US (OSHA 29 CFR 1910.95) | UK (Regulations 2005 / L108) | EU (Directive 2003/10/EC) |
|---|---|---|---|
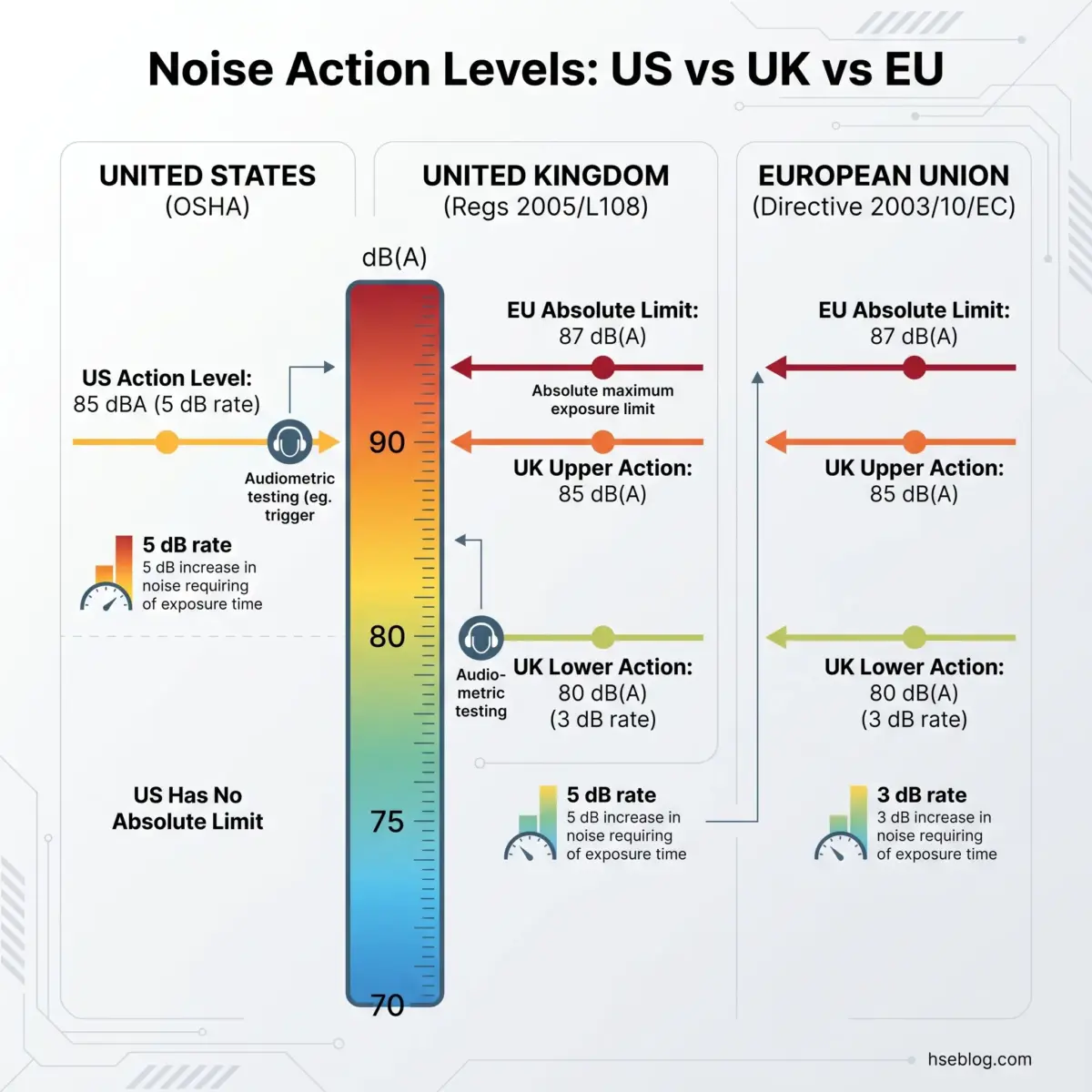
| Lower action level | 85 dBA TWA (action level) | 80 dB(A) LEP,d | 80 dB(A) LEP,d |
| Upper action level | 90 dBA TWA (PEL) | 85 dB(A) LEP,d | 85 dB(A) LEP,d |
| Audiometric testing triggered at | 85 dBA TWA | 85 dB(A); also 80–85 dB(A) for at-risk workers | 85 dB(A); preventive testing available at 80 dB(A) |
| Absolute exposure limit | None specified | 87 dB(A) (accounting for HPD attenuation) | 87 dB(A) (accounting for HPD attenuation) |
| Exchange rate | 5 dB | 3 dB | 3 dB |
The practical impact of the exchange rate difference is substantial. Under OSHA’s 5 dB exchange rate, exposure to 90 dBA for eight hours equals 100% dose. Under the UK/EU 3 dB exchange rate, the same 90 dBA for eight hours equals 200% dose. A worker who is compliant under OSHA calculations may be over-exposed under UK or EU methodology for the identical noise environment.
Employers operating across both the US and UK frequently assume the OSHA 85 dBA action level and the UK 85 dB(A) upper action value are interchangeable requirements. The numerical similarity obscures a critical difference: UK regulations require health surveillance to begin at 80 dB(A) for workers identified as particularly at risk — for example, those with pre-existing hearing conditions or early signs of loss. OSHA has no equivalent provision at 80 dBA.
Which Industries Have the Highest Audiometric Testing Requirements?
Construction, manufacturing, and mining consistently produce the highest rates of occupational noise-induced hearing loss. Approximately 28% of all US workers have been exposed to hazardous noise, with 16% (27 million) exposed in the last year alone (NIOSH Occupational Hearing Loss Surveillance, 2023 data).
A significant regulatory gap exists in US construction: OSHA’s occupational noise exposure standard (29 CFR 1910.95) applies to general industry, while construction falls under 29 CFR 1926.52, which does not explicitly require a full hearing conservation programme including audiometric testing. This leaves construction workers — among the most noise-exposed in any sector — without a mandatory audiometric testing requirement under federal OSHA.
The music and entertainment sectors were specifically flagged in EU Directive 2003/10/EC as requiring adapted implementation measures, recognising the unique exposure patterns and cultural resistance to hearing protection in those industries.
How Often Is Audiometric Testing Required?
The testing schedule runs per employee, not per facility — and the baseline and periodic frequencies differ across jurisdictions.
Baseline Audiogram Timing
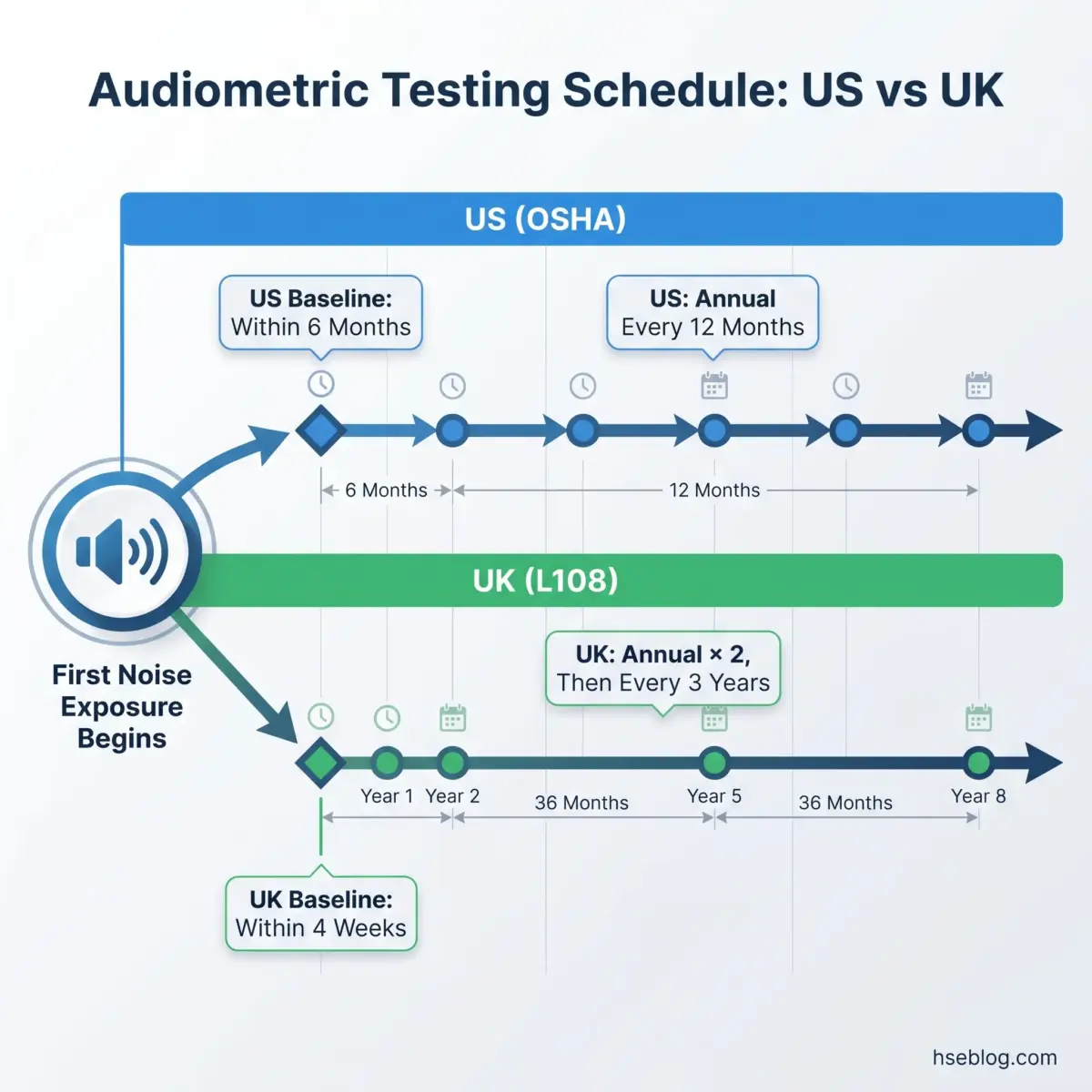
- US (OSHA): Within 6 months of first exposure at or above 85 dBA TWA. If a mobile testing van is used, the deadline extends to 12 months — but the employee must wear hearing protection during the entire extension period. A 14-hour quiet period (no workplace noise exposure) must precede the baseline; HPD use can satisfy this requirement.
- UK (L108): Within 4 weeks of first exposure above 80 dB(A), per HSE guidance on health surveillance for noise. The tighter window reflects the UK framework’s lower initial action threshold.
- EU (Directive 2003/10/EC): Baseline timing deferred to member state transposition. No specific deadline at the directive level.
Periodic Testing Frequency
The periodic schedule is where jurisdictional differences become operationally significant:
- US (OSHA): Annual — at least every 12 months from each employee’s prior test date. The 12-month clock is individual, which means a facility with 200 enrolled workers has 200 separate annual testing deadlines.
- UK (L108): Annual for the first two years following baseline, then every three years — unless deterioration is detected, the worker requests more frequent testing, or the risk assessment identifies particular risk factors. Any Category 3 or 4 result (see STS section below) resets the schedule to annual.
- EU: Frequency delegated to member states. No pan-European periodic testing mandate exists at the directive level.
The most common compliance failure in US programmes is lapsed annual testing cycles. Employers who batch-test everyone on a single annual date inevitably discover that mid-cycle hires fall out of compliance within months. The regulatory requirement is clear — the clock runs from each employee’s last test, not from a company-wide scheduling convenience.
What Does an Audiometric Test Involve? The Testing Procedure
Occupational audiometry is a standardised screening procedure — not a full diagnostic evaluation. Understanding the distinction prevents both under-testing and over-interpreting results.
OSHA mandates pure-tone air-conduction testing only. The procedure measures the softest sound a person can detect at each test frequency, in each ear separately. Clinical diagnostic audiometry — which may include speech audiometry, bone conduction, tympanometry, or otoacoustic emissions — is a different scope of evaluation reserved for specialist referral.
The Test Sequence
- Pre-test history: The technician collects information on recent noise exposure, ear complaints, medication use, and whether the 14-hour quiet period has been met.
- Headphone placement: Supra-aural or insert earphones are positioned. Poor placement is one of the most frequent sources of invalid results — particularly with supra-aural headphones on workers with heavy facial hair or eyeglass frames.
- Threshold testing: Pure tones are presented at 500, 1000, 2000, 3000, 4000, and 6000 Hz in each ear. The worker signals when a tone is heard, and the technician records the threshold for each frequency.
- Results recording: Thresholds are plotted on an audiogram for comparison against baseline.
Test Environment and Equipment
The test environment must meet maximum permissible ambient noise levels specified in Appendix D to OSHA’s occupational noise exposure standard (29 CFR 1910.95). This does not require a sound booth — it requires that ambient noise be low enough not to mask test tones. The practical field reality is that some test rooms technically pass the ambient noise check during quiet periods but fluctuate above permissible levels when production ramps up.
Audiometer calibration follows a three-tier schedule:
- Daily: Biological check using a person with known, stable thresholds (bioacoustic simulator)
- Annual: Acoustic calibration by a qualified technician
- Exhaustive: Required when deviations exceed 15 dB at any frequency
Who Can Administer the Test?
Under OSHA, audiometric testing may be performed by a licensed audiologist, otolaryngologist, physician, or a technician certified by the Council for Accreditation in Occupational Hearing Conservation (CAOHC) under the supervision of an audiologist or physician. The supervising professional is responsible for reviewing problem audiograms — the technician identifies the shift, but the professional determines its significance.
Screening typically takes 5–10 minutes per employee. Detailed diagnostic audiometry, when needed after referral, can take up to one hour.
What Is a Standard Threshold Shift (STS) and Why Does It Matter?
An STS is the single most important outcome metric in occupational audiometry — it is the regulatory trigger that converts a routine screening result into a mandatory response chain.
OSHA Definition and Calculation
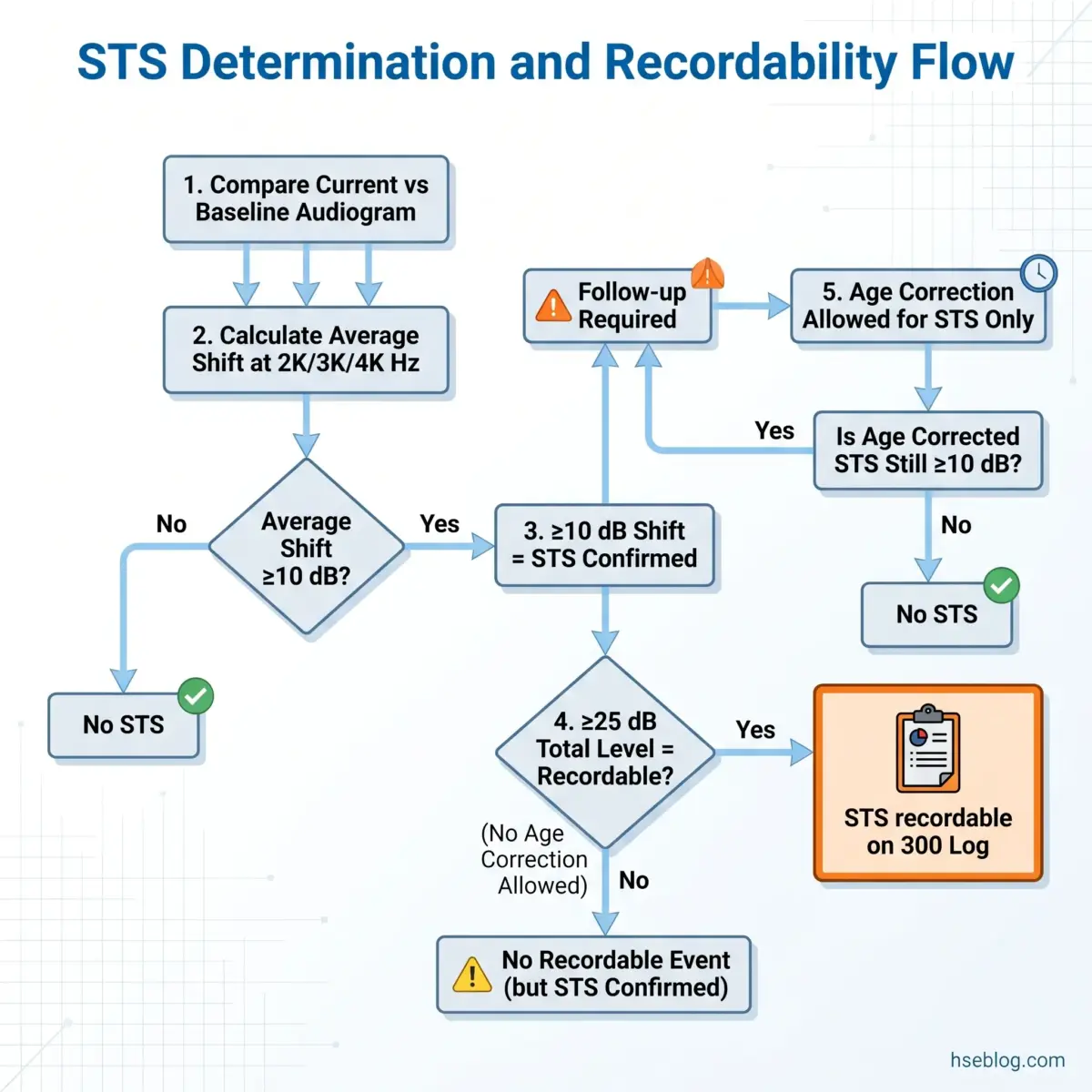
Under 29 CFR 1910.95, an STS is defined as an average shift of 10 dB or more at 2000, 3000, and 4000 Hz in either ear, compared to the baseline audiogram.
A worked example clarifies the calculation:
- Baseline thresholds (left ear): 2000 Hz = 10 dB, 3000 Hz = 10 dB, 4000 Hz = 15 dB → average = 11.7 dB
- Current thresholds (left ear): 2000 Hz = 20 dB, 3000 Hz = 25 dB, 4000 Hz = 25 dB → average = 23.3 dB
- Shift: 23.3 − 11.7 = 11.7 dB → STS confirmed
Age Correction and Recordability
Two critical distinctions that programme administrators frequently confuse:
- Age correction is permitted but not required when determining whether an STS has occurred. Applying age correction tables (Appendix F to 1910.95) can reduce the calculated shift below the 10 dB threshold, eliminating the STS determination.
- Age correction is NOT permitted when determining the 25 dB recordability threshold under OSHA recording criteria for occupational hearing loss (29 CFR 1904.10).
An STS becomes OSHA-recordable on the 300 Log only when both conditions are met: the STS is confirmed, AND total hearing level is 25 dB or more above audiometric zero (averaged at 2000, 3000, 4000 Hz) in the same ear, AND work-relatedness has not been ruled out by a physician.
The Counterintuitive Reality
A misconception that undermines many programmes: an STS can be detected and require full follow-up even when the worker’s hearing falls within clinically “normal” range. A worker whose baseline was exceptionally good — thresholds at 0–5 dB — can register a confirmed STS while still hearing at levels most clinicians would call “normal.” Dismissing that shift because the worker “can still hear fine” defeats the entire purpose of the metric. The STS catches decline while it is still early enough to intervene, not after the damage is functionally noticeable.
UK Categorisation System
The UK uses a different classification framework under L108:
- Category 1 (Acceptable): No significant hearing loss
- Category 2 (Mild loss): Monitor — continue surveillance
- Category 3 (Poor): Referral for specialist assessment, review noise controls
- Category 4 (Rapid decline): Urgent referral, consider redeployment
Category 3 and 4 results trigger immediate occupational health referral and a mandatory review of workplace noise controls — a more structured escalation pathway than OSHA’s STS framework.
Baseline Revision
OSHA permits revising the baseline audiogram when an STS is persistent on the subsequent annual test, or when hearing has significantly improved. The supervising audiologist or physician makes this determination. Once revised, all future comparisons use the new baseline — which resets the STS calculation window.
What Happens After an Audiometric Test Shows a Hearing Shift?
Most guidance on audiometric testing stops at “notify the employee.” The actual post-STS workflow involves a structured chain of actions — and the most frequently missed step is the last one.
The OSHA Post-STS Response Sequence
- Employee notification: Written notice within 21 days of the STS determination — not 21 days from the test date, but from the date the reviewing professional confirms the shift.
- Retest option: A retest within 30 days of the original test is permitted. If the retest audiogram does not confirm the STS, the employer may use the retest as the annual audiogram, and no further follow-up is required.
- HPD intervention: Workers not currently using hearing protection must be fitted immediately. Workers already using HPDs must be refitted with more effective protection or provided with an alternative device.
- Retraining: The worker must receive retraining on the effects of noise on hearing, the purpose of audiometric testing, and the correct selection and use of hearing protection devices.
- Clinical referral: When the STS or audiogram pattern suggests pathology beyond noise exposure (e.g., asymmetric loss, conductive component), referral for further audiological or otological evaluation is required.
- Baseline revision: If the STS persists on the following annual audiogram, the reviewing professional may revise the baseline. All subsequent comparisons then use the new reference point.
- Recordability determination: If the STS ear also shows total hearing level ≥25 dB above audiometric zero (averaged at 2000, 3000, 4000 Hz), and work-relatedness is not ruled out by a physician, the case is recorded on the OSHA 300 Log.
UK Post-Assessment Actions
Under L108, Category 3 or 4 results trigger a parallel but distinct pathway:
- Occupational health referral for specialist audiological assessment
- Mandatory review of the worker’s noise exposure and existing controls
- Consideration of redeployment to a lower-noise role if further exposure would accelerate loss
- Health surveillance records updated and retained for 40 years
The Missing Step: Programme-Level Feedback
The action most consistently absent from post-STS workflows is the feedback loop to the noise control programme itself. A cluster of STS cases within the same department, production line, or job role is a systemic signal — not a collection of individual worker problems.
When three workers in one area all register threshold shifts within the same testing cycle, the investigation should ask whether area noise levels have changed, whether HPD selection for that environment is adequate, and whether engineering controls have degraded. Treating each STS as an isolated HPD-refitting exercise misses the diagnostic value of the data entirely.
Emerging Developments: Boothless Audiometry and Ototoxic Co-Exposure
Two developments are reshaping how effective hearing conservation programmes approach audiometric testing — and most current programmes have not yet incorporated either.
Boothless Audiometry
Traditional occupational audiometry assumes a sound-treated booth. Boothless (out-of-booth) audiometry uses noise-attenuating headphones combined with automated software to deliver valid threshold testing outside a booth environment.
Peer-reviewed research has confirmed clinical equivalence to booth-based testing when ambient noise conditions are controlled. Sheffield et al. (2023) and Meinke & Martin (2023) published validation data in the Journal of the Acoustical Society of America, and a January 2026 publication in the International Journal of Audiology (Kulinski, Sheffield & Brungart) extended this work to explore how personal attenuation rating data from HPD fit-testing can predict audiometric threshold shifts.
OSHA does not mandate a sound booth. The requirement is that the test environment meets the maximum permissible ambient noise levels in Appendix D to 1910.95. Boothless systems that achieve this through headphone attenuation are fully compliant.
The practical advantage is operational: automated boothless systems reduce scheduling barriers, enable more frequent monitoring, and can be deployed at remote or mobile worksites where transporting a booth is impractical.
Ototoxic Chemical Co-Exposure
The more consequential gap in most hearing conservation programmes is the complete absence of chemical exposure integration.
NIOSH occupational hearing loss surveillance data published in 2025 (Masterson, Morata & Themann, using 2023 NHIS data) reported that approximately 13% of all US workers — 22 million people — have been exposed to ototoxic chemicals in the workplace. Approximately 7% have been exposed to both hazardous noise and ototoxic chemicals simultaneously.
The chemicals involved include:
- Solvents: Toluene, xylene, styrene, carbon disulfide
- Heavy metals: Lead, mercury
- Certain medications: Aminoglycoside antibiotics, cisplatin
Combined noise-plus-ototoxic exposure accelerates hearing loss beyond what either hazard would produce alone. Yet the standard hearing conservation programme is built exclusively around noise dosimetry data, with zero integration of chemical exposure records from industrial hygiene monitoring.
The judgment call for HSE professionals designing audiometric testing programmes is whether to expand enrollment criteria beyond the noise-only action level to include workers with significant ototoxic chemical exposure — even if their noise levels fall below 85 dBA. The NIOSH data increasingly supports this expansion as best practice, though OSHA’s standard does not yet require it.
How to Build and Maintain a Compliant Audiometric Testing Programme
A compliant programme meets every regulatory deadline. An effective one uses the data those deadlines generate. Building both requires attention to logistics, personnel, and — above all — the feedback systems that connect individual test results to programme-level decisions.
Programme Foundation
Before enrolling any worker in audiometric testing, establish the noise exposure baseline through area and personal noise monitoring. Without accurate exposure data, the programme cannot determine which workers require enrollment, which HPDs are adequate, or which areas need engineering controls.
Testing Model Selection
Each testing approach involves trade-offs:
| Model | Advantage | Limitation |
|---|---|---|
| In-house booth | Consistent environment, year-round availability | Capital cost, space requirement, requires calibrated equipment and trained staff |
| Mobile van | Reaches multiple sites, no facility space needed | Extends baseline deadline to 12 months (US), scheduling constraints, equipment transit risk |
| Off-site clinic | Professional-grade environment, specialist staff | Worker downtime for travel, scheduling coordination, higher per-test cost |
| Boothless automated | Deployable anywhere, reduced scheduling barriers | Requires ambient noise verification, newer technology with less institutional familiarity |
The hybrid approach — a permanent in-house station supplemented by mobile testing for remote or short-term sites — addresses the most common scheduling failures while maintaining environmental control.
Personnel Requirements
- Testing: CAOHC-certified occupational hearing conservationist (OHC) under professional supervision, or licensed audiologist/physician directly
- Programme oversight: Audiologist or physician responsible for reviewing problem audiograms, confirming STS determinations, and authorising baseline revisions
- CAOHC certification requires renewal every 5 years — lapsed certification is a compliance gap that rarely surfaces until an audit
Recordkeeping
Retention requirements differ substantially by jurisdiction:
- US (OSHA): Audiometric test records retained for duration of employment. Noise exposure measurement records retained for at least 2 years.
- UK (L108): Health surveillance records retained for 40 years.
For multinational employers, the UK 40-year retention requirement effectively governs — it is impractical to maintain parallel retention policies when the longer standard applies to any UK-exposed worker.
Annual Training Requirement
OSHA requires annual training for all workers enrolled in the hearing conservation programme, covering:
- Effects of noise on hearing — mechanism and permanence of damage
- Purpose and procedures of audiometric testing — why the test matters and what results mean
- HPD selection, fitting, use, and care — practical and specific to available devices
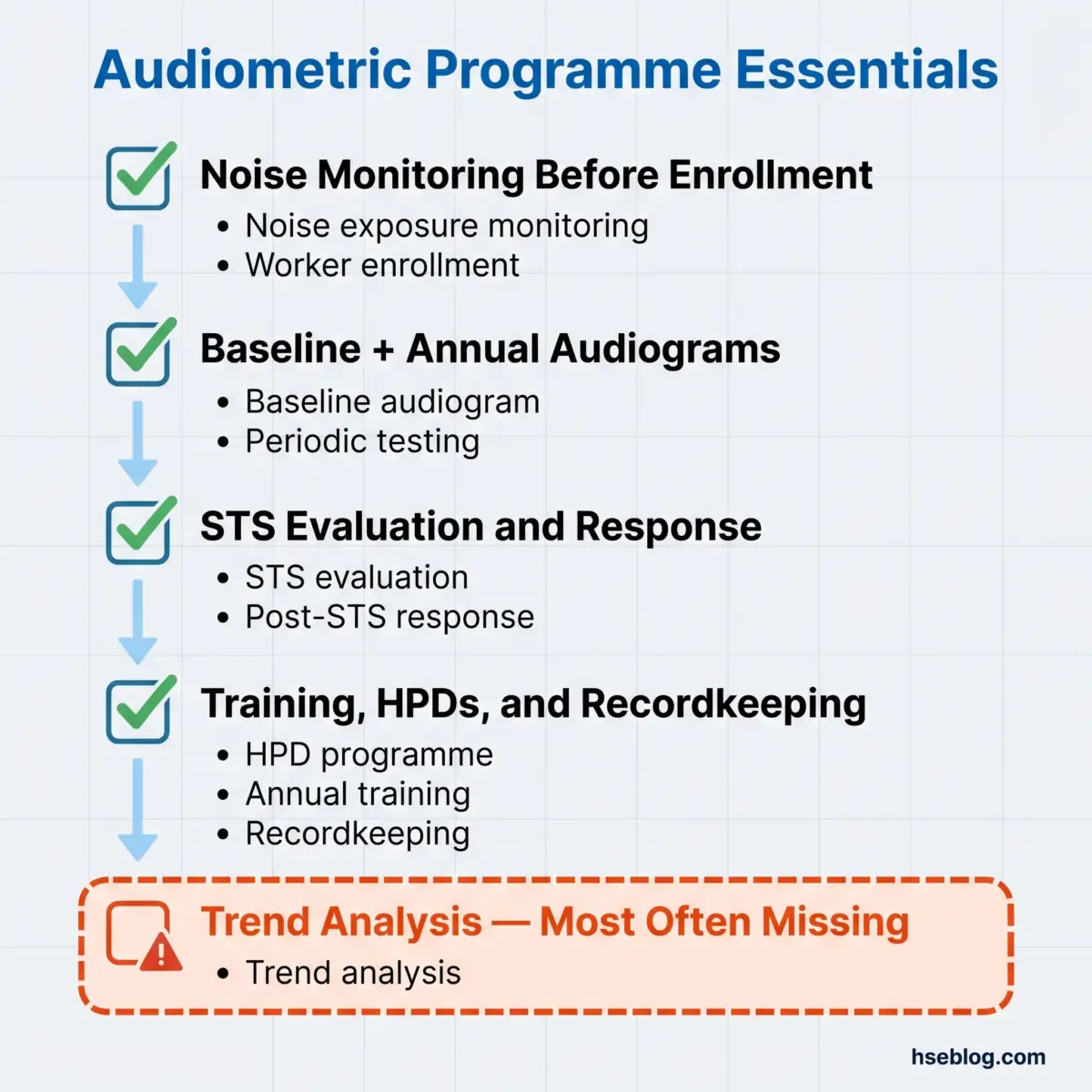
The Single Biggest Programme Failure
The most common systemic failure is not technical, and it is not about calibration schedules or testing intervals. It is administrative: audiometric data accumulates in a database with no one systematically reviewing trends, no one correlating STS rates with departmental noise data, and no feedback loop connecting test outcomes to noise control investment decisions.
A programme that meets every OSHA deadline but never analyses its own aggregate data is compliant. It is not protecting hearing.
Frequently Asked Questions
Conclusion
The industry’s persistent failure with audiometric testing is not in performing the tests — it is in using the results. Programmes that meet every scheduling deadline and produce compliant records still lose workers’ hearing because no one asks what the aggregate data means. A rising STS rate in one department is not a collection of individual misfortunes requiring individual HPD refits. It is a signal that noise controls or hearing protection in that area are failing, and the response belongs at the programme level, not just the worker level.
The highest-impact change most hearing conservation programmes can make requires no new equipment and no regulatory change. It requires someone — an HSE professional, an occupational health coordinator, a programme administrator — to sit down with the audiometric database once per year and look at trends by department, job role, and exposure group. Where are shifts clustering? Do those clusters align with areas where noise levels have changed, where HPD compliance is weakest, or where ototoxic chemical co-exposure exists? That analysis transforms audiometric testing from a regulatory obligation into the early-warning system it was designed to be.
Noise-induced hearing loss is permanent, cumulative, and entirely preventable with competent controls and timely intervention. The audiogram provides the data. Whether that data protects anyone depends on what happens after the test is over.
Regulatory content in this article reflects general HSE professional understanding of OSHA (US), UK, and EU requirements as of 2025–2026. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.