

At 0340 on an offshore production platform, the central control room sits at a deliberate 21°C and smells faintly of coffee that has been in the pot too long. Two operators watch separator trends on opposing screens. One of them, a man I have worked with for six years, takes nine seconds to respond to a low-level alarm he normally clears in two. He is not hungover, careless, or inexperienced. He is working inside the narrow window between 0200 and 0600 when the human brain is biologically primed to be anywhere except alert.
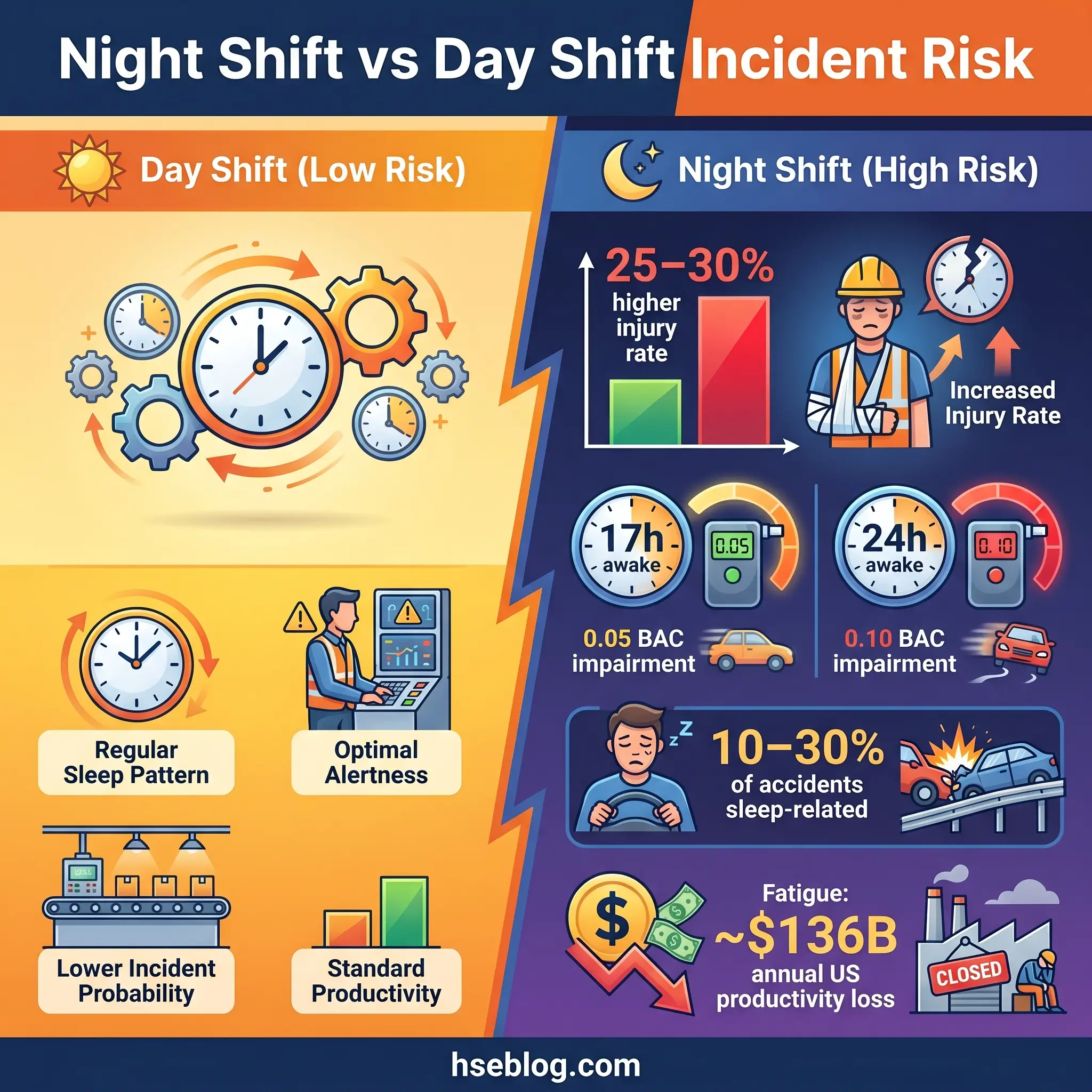
Circadian rhythm and workplace safety are tied together by biology we cannot negotiate. Injury rates on night shifts run 25–30% higher than day shifts, and 17 hours without sleep impairs performance to roughly the same degree as a blood alcohol content of 0.05. Yet most organisations still treat shift work as a scheduling problem rather than a hazard requiring engineered controls. The sections below explain how the human clock creates workplace risk, where the danger concentrates inside a 24-hour period, what standards now require employers to do about it, and which control strategies actually move the needle on site.
What Is Circadian Rhythm and Why Does It Matter at Work?
The body’s 24-hour clock is a physical structure: a cluster of roughly 20,000 neurons in the hypothalamus called the suprachiasmatic nucleus, or SCN. It receives light signals through the optic nerve and uses them to synchronise hormone release, core body temperature, digestion, and — critically for safety — alertness and cognitive performance. Left to itself, the clock runs slightly longer than 24 hours; daylight resets it every morning.
Light is by far the strongest zeitgeber, the term chronobiologists use for an external cue that entrains the internal clock. Blue-wavelength light around 480 nanometres suppresses melatonin most aggressively. That matters at 0300 when an operator working nights is fighting the biology of a body that thinks it should be asleep — and also at 0700 when that same operator steps into daylight on the helideck and accidentally resets their own clock in the wrong direction.
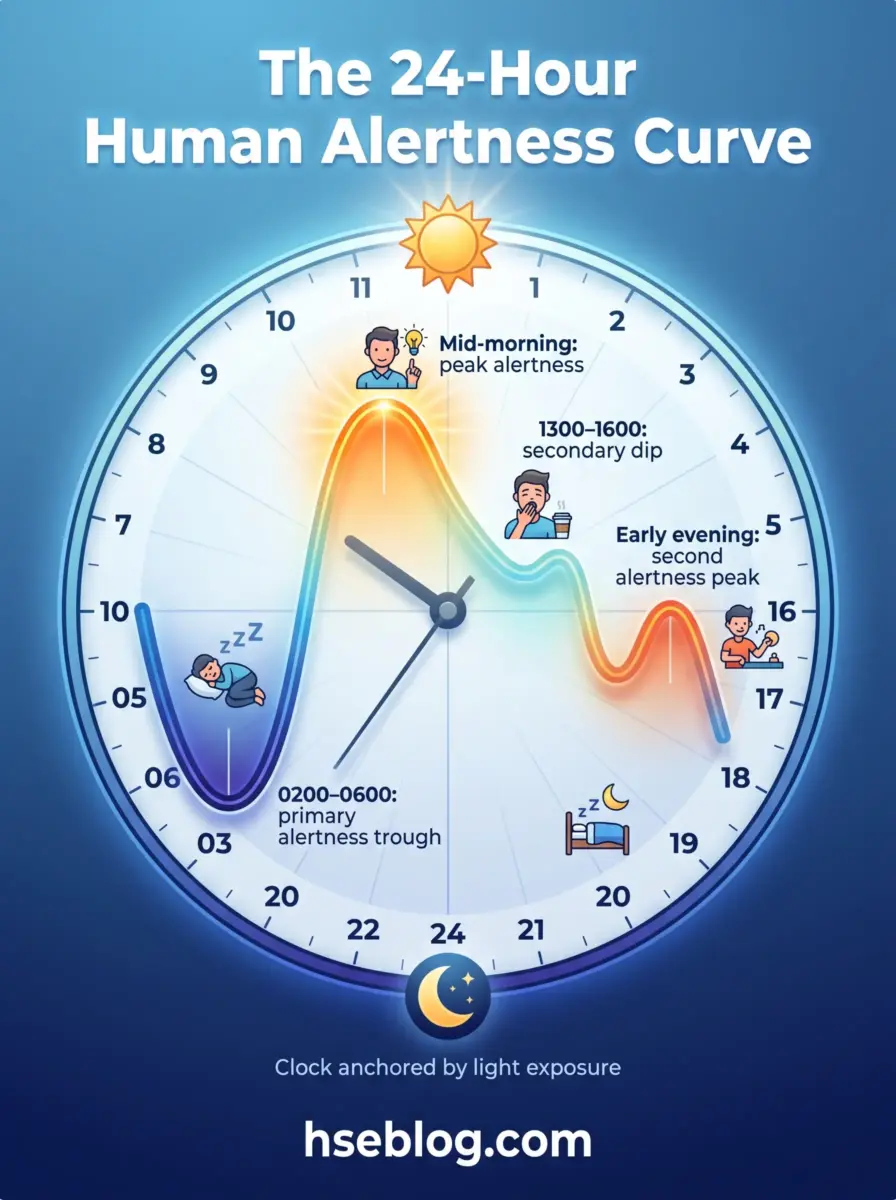
Alertness does not stay flat across 24 hours. It dips sharply between 0200 and 0600, rises through mid-morning, falls again between 1300 and 1600, peaks in the early evening, and descends into the next low. Every workplace schedule runs over the top of this curve whether we acknowledge it or not.
How Circadian Rhythm Disruption Creates Workplace Safety Risks
Slowed reaction time is the first symptom. Psychomotor Vigilance Task response latencies measured at 0400 regularly run 30–50% longer than those taken at 1400 by the same worker. The gap widens with consecutive night shifts, and it is not subjective — the worker often insists they feel fine.
After reaction time comes judgment. Sleep-deprived decision-makers struggle with novel situations, default to familiar patterns, and underweight risk. A night-shift permit signatory approves a job they would have paused during the day. A 2024 review in npj Biological Timing and Sleep concluded that sleep-related problems are implicated in 10–30% of workplace accidents across studies from the United States, United Kingdom, and France.
Then come microsleeps — involuntary lapses of consciousness lasting two to thirty seconds, often unnoticed by the worker. Microsleeps sit in the investigation histories of Three Mile Island, Chernobyl, the Bhopal disaster, the Exxon Valdez grounding, and the Challenger launch decision. None of those events had a single cause, but the hour at which they occurred is not accidental.
The quantitative picture is clear. OSHA’s drowsy-driving guidance notes that 17 consecutive hours awake produces impairment roughly equivalent to a blood alcohol content of 0.05, and 24 hours roughly equivalent to 0.10. The National Safety Council estimates night-shift incident risk at about 30% above morning shifts. HSE-referenced fatigue guidance puts night-shift injury risk 25–30% higher than day shifts, rising further on 12-hour rotations compared with 8-hour patterns. Fatigue is estimated to cost US employers around $136.4 billion annually in lost productive work time.
The Biological Mechanism: Circadian Misalignment
Shift workers rarely achieve full circadian adaptation. The internal clock stays day-oriented even when the schedule is night-oriented. Partial phase shifts of one to two hours per day are typical, and full inversion almost never happens in standard rotations because daylight on the commute home, meals, and social life keep pulling the clock back toward day-awake timing.
Offshore crews adapt further than their land-based counterparts because they spend two-week rotations isolated from normal zeitgebers and in controlled-light accommodation. Even then, the adaptation is incomplete. Chronic misalignment produces a mismatch between when the body wants to sleep and when the roster allows it, and that mismatch — not the hours themselves — drives most of the long-term safety and health damage.
Who Is Most Affected? High-Risk Workers and Industries
Roughly a quarter of the US adult workforce does some form of shift work, and approximately 15% of full-time US employees work shifts according to National Safety Council data drawn from the Bureau of Labor Statistics. The risk profile is not uniform across that population.
Certain industries carry structurally higher circadian risk because their work cannot stop. The groups most exposed, in my experience, include:
- Healthcare staff — nurses, anaesthetists, and emergency physicians making drug-dosing and triage decisions inside the 0200–0600 trough
- Transport operators — long-haul drivers, locomotive engineers, pilots on transmeridian flights, and mariners on bridge watches
- Oil, gas and petrochemical operators — offshore platforms, refineries, and LNG terminals with continuous process control
- Utility and nuclear control-room staff — life-safety consequences per decision, with decisions often required at 0400
- Manufacturing crews — continuous-process plants and assembly lines on 24-hour patterns
- Emergency responders and security personnel — callout peaks overlap the alertness trough
- Commercial drivers commuting home — often the single most vulnerable subgroup, because the risk leaves the workplace with them
Individual vulnerability varies. Chronotype matters — a strong evening type will adapt slightly better to night work than a morning type, and the reverse is true for early starts. Age reduces shift tolerance after about 45–50. Undiagnosed sleep apnoea and shift work disorder compound the problem. This is well documented in the StatPearls Shift Work Hazards review and replicated across occupational medicine literature.
The Science of Circadian Dips: When Accidents Peak
The 2005 Folkard, Lombardi and Spencer analysis of occupational injury timing produced a finding that reshaped how I think about scheduling. When they fitted cosinor models to large injury datasets, the acrophase — the time of peak risk — clustered around midnight, with elevated risk stretching from late evening through early morning. The dip that biology predicts is also the dip the injury data measures.
Two windows carry most of the risk. The primary trough between 0200 and 0600 coincides with the lowest core body temperature and the highest endogenous sleep pressure. Microsleeps concentrate here. The secondary dip between 1300 and 1600 — the post-lunch window — is smaller but operationally significant because workers rarely attribute it to biology and usually blame lunch.
Consecutive nights compound the problem. Risk rises measurably on the second night, climbs on the third, and accelerates from the fourth onward as cumulative sleep debt grows. Working Time Society consensus documents, updated through the 2024–2025 cycle, continue to recommend no more than three consecutive night shifts for exactly this reason.
Watch For: On 12-hour rotations, the last two hours of a night shift are the highest-risk window of the entire roster — circadian trough, cumulative fatigue, and end-of-shift cognitive tunnelling stacking on the same two hours.
Shift-end risk deserves attention in its own right. After ten hours on the console, an operator is both physiologically exhausted and mentally already at home. The last two hours of a 12-hour night shift are where a disproportionate share of near-miss reports cluster.

Health Consequences That Feed Back into Safety
Most safety guides treat health and safety separately. They are not separate. A worker whose cardiovascular, metabolic, or mental health has been eroded by years of circadian disruption is a different worker, from a fitness-for-duty perspective, than the one who was hired.
The International Agency for Research on Cancer classifies shift work that involves circadian disruption as Group 2A — probably carcinogenic to humans — in IARC Monograph Volume 124, published in 2020. The US National Toxicology Program’s 2021 cancer hazard assessment reached a high-confidence conclusion that persistent night-shift work can cause breast cancer in women. More than ten million US adults frequently work night shifts, and the NTP review associated shift-work disruption with a contribution of approximately 12,000 new breast cancer cases per year in the United States.
Cardiovascular and metabolic conditions follow the same pattern. Long-term shift workers show elevated rates of hypertension, type 2 diabetes, and metabolic syndrome. Gastrointestinal complaints cluster in the same population. Depression, anxiety, and burnout all run measurably higher among shift workers than matched day-work comparison groups.
Shift Work Disorder, recognised in the ICSD-3 classification, sits at the intersection of these. Its core features are insomnia and excessive sleepiness aligned to a work schedule that overlaps habitual sleep hours. Prevalence runs 29–38% for insomnia symptoms against roughly 6% in the general population. HSE has additionally flagged reproductive-health concerns, particularly around pregnancy outcomes. Each of these conditions narrows the margin a worker has to cope with a bad day at work.
Is There a Safest Shift Pattern? Schedule Design Principles
Yes — and it is specific enough to put on paper. The evidence base, summarised in HSE’s HSG256 Managing Shift Work and in NIOSH’s shift-rotation literature, points to a small number of design rules that consistently reduce risk:
- Rotate forward, not backward. A day → evening → night sequence lets the clock phase-delay, which the body does more easily than phase-advance. Rotating the other way fights biology.
- Limit consecutive night shifts to three where possible, and no more than five in any case. Risk accumulates across sequential nights.
- Cap shift length at 12 hours, and at 8 hours for safety-critical, monotonous or highly cognitive night-time tasks.
- Provide at least 11 consecutive hours of rest between shifts, the minimum under the EU Working Time Directive and a floor rather than a target.
- Avoid early starts before 0700 where possible. Workers sacrifice sleep to accommodate them rather than extending their evening.
- Build in at least two full nights of recovery sleep after a block of nights before returning to any shift pattern.
Permanent night schedules are a special case. They produce better adaptation for a minority of workers — typically strong evening chronotypes with supportive home environments — but worse outcomes for most. Unless a worker has clearly self-selected a permanent night role and has the domestic conditions to protect daytime sleep, rotation is safer.
Countermeasures: A Hierarchy-of-Controls Approach to Circadian Risk
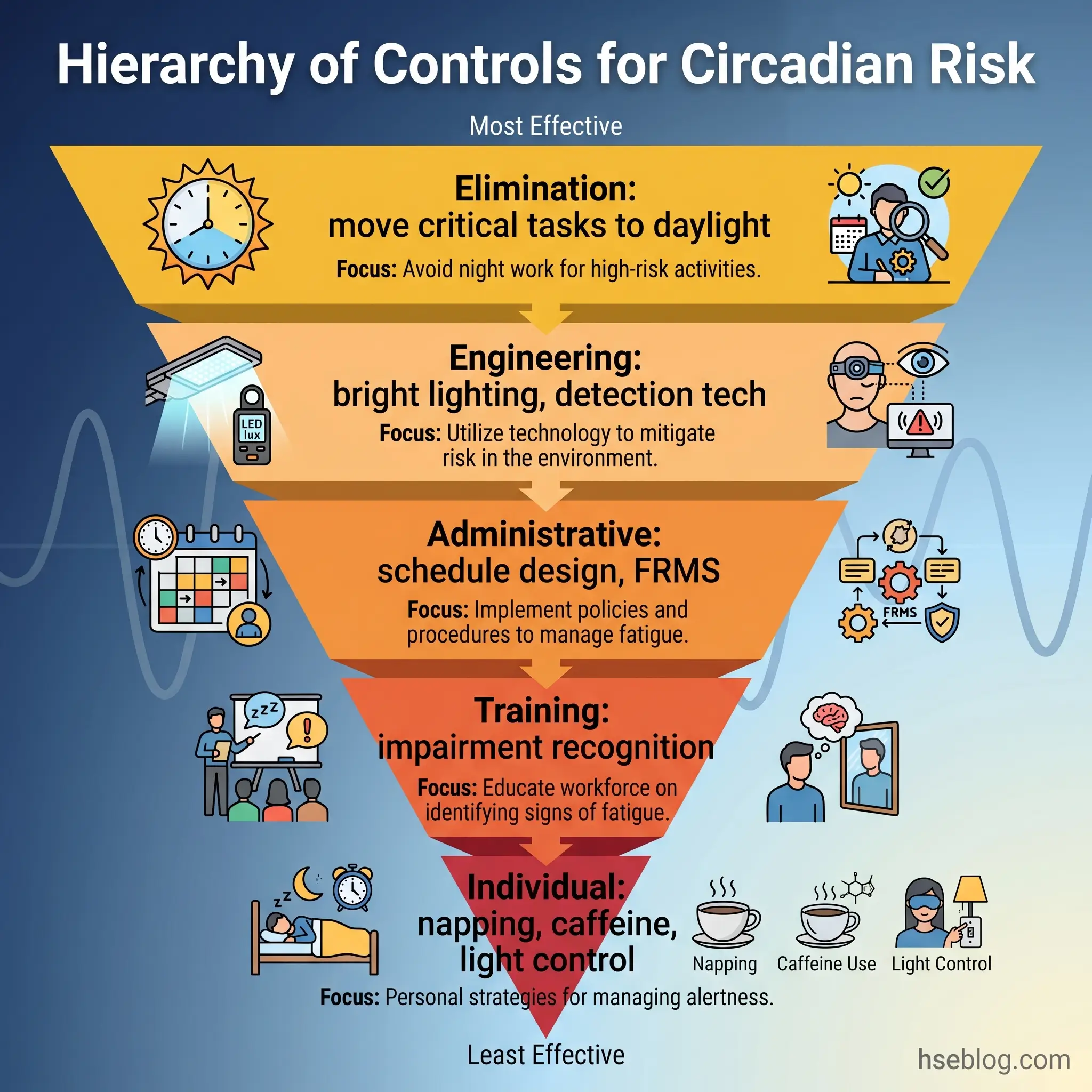
Thinking about circadian risk through the hierarchy of controls, which every HSE professional already uses for chemical, mechanical and electrical hazards, brings the problem into operational focus. Each tier has specific applications.
Elimination and substitution. The highest-value move is scheduling safety-critical work outside the circadian trough. Commissioning activities, first-time procedures, heavy lifts, confined-space entries, and complex permit work should, where at all possible, happen in daylight hours. On the platform I work, we moved our monthly emergency shutdown test from 0300 to 1000 two years ago. The rationale was not convenience; it was the evidence that detection and response errors concentrated in the early morning.
Engineering controls. Bright, blue-enriched lighting in control rooms and operational areas during the first half of a night shift measurably improves alertness. Workspace temperature, seating, screen glare, and ventilation all matter more at 0300 than at 1500. Fatigue-detection technology — eye-tracking in vehicles, heart-rate-variability wearables — is increasingly viable as an engineering control in transport and heavy-equipment operations.
Administrative controls. Schedule design is the largest administrative control. Mandatory rest breaks, enforced napping windows on long shifts, dual verification for night-time safety-critical tasks, ride-home programmes, and supervisor training in impairment recognition all sit in this tier. A written fatigue policy, backed by a non-punitive reporting route, is the foundation.
Individual countermeasures. Strategic napping, caffeine timing, pre-shift daylight exposure, sleep-hygiene practices, and blue-light management are all worker-level controls. They work, and they are necessary, but they are the last line — not the first.
Using Light Strategically
Light is a tool and a hazard on the same shift. Illumination in the 2500–10000 lux range during the first half of a night shift supports alertness and can partially phase-shift the internal clock. The same exposure on the morning commute home undermines sleep by telling the SCN the day is starting. Wraparound sunglasses with 95%+ blue-light attenuation, worn from leaving the workplace to the bedroom, protect daytime sleep. They should not be used while driving if the worker is already severely sleepy — no filter fixes that problem.
Napping and Alertness Management
The strongest practical countermeasure is a short pre-shift or mid-shift nap. NIOSH and the American Academy of Sleep Medicine converge on 20–30 minutes as the optimum window. That length captures stages 1 and 2 sleep without dropping into slow-wave sleep, which produces sleep inertia — the grogginess that lingers for up to 30 minutes after a longer nap. Caffeine helps, but only in the first half of a shift; caffeine consumed after about 0200 interferes with daytime sleep at home. A useful field pattern on our platform is a 25-minute break-room nap around 0100, followed by controlled caffeine intake and bright light re-entry into the control room.
Fatigue Risk Management Systems (FRMS): Making Circadian Safety Operational
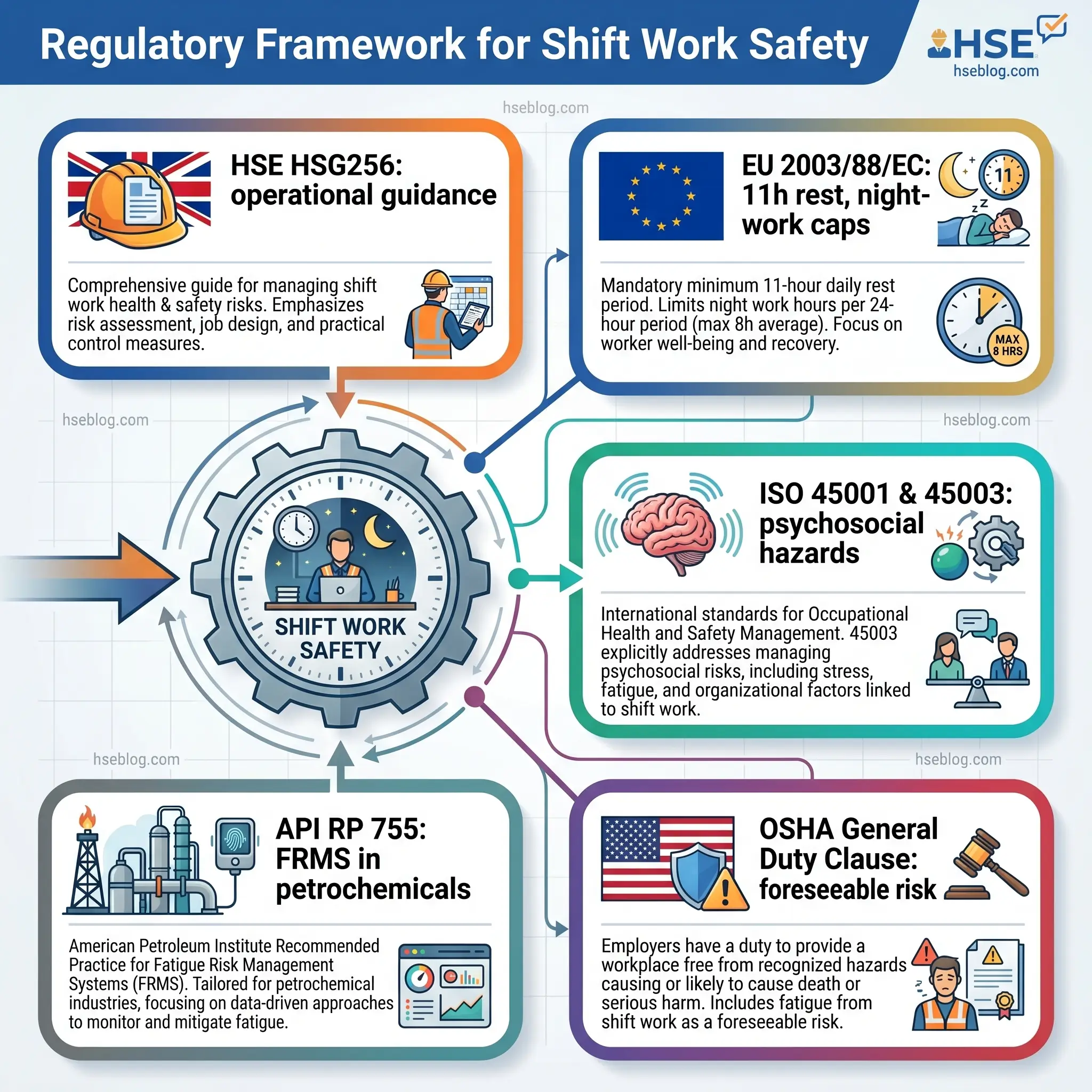
A Fatigue Risk Management System is the organisational framework that holds the controls above together. It is no longer optional in several safety-critical sectors. API Recommended Practice 755 requires a formal FRMS in refining and petrochemical operations. The Energy Institute has equivalent guidance. Rail and aviation regulators in most jurisdictions expect one. HSE expects duty-holders in high-hazard industries to demonstrate structured fatigue-risk management.
Core components are consistent across frameworks: a written policy, hazard identification that explicitly includes circadian factors, risk assessment of schedules and activities, layered controls, monitoring, training, and continuous improvement. HSE’s Fatigue and Risk Index calculator is the most widely used quantitative tool in the UK and European space. It scores a schedule against the percentage probability that a worker will reach a Karolinska Sleepiness Scale level of 8–9 — “extremely sleepy, fighting sleep.” Scores must be driven “as low as reasonably practicable.”
Audit Point: An FRMS that cannot produce schedule-level FRI scores or KSS-based monitoring data when an auditor asks for them is a paper system. The regulator wants to see circadian risk being measured, not just acknowledged.
An FRMS sits cleanly inside an ISO 45001 management system. Clause 6.1.2 requires hazard identification that includes psychosocial factors, and clause 8.1.2 requires eliminating hazards or reducing risks. ISO 45003:2021 then provides the psychosocial framework specifically — “work hours and schedule” is named as a psychosocial hazard — and completes the integration. For safety professionals building an FRMS from scratch, that pair of standards is the right scaffold.
Commuting and Drowsy Driving: The Hidden Shift-Related Risk
Motor vehicle crash risk for shift workers runs two to four times that of day workers, according to Rajaratnam and colleagues in the Medical Journal of Australia in 2013. In the American Nurses Association 2011 Health and Safety Survey, one in ten nurses reported a motor vehicle accident they attributed to shift-work fatigue. The National Highway Traffic Safety Administration estimated 91,000 police-reported drowsy-driving crashes in 2017, with approximately 50,000 injuries and 800 fatalities.
Most organisational safety metrics never capture any of this. The worker is off-site, off-shift, off-clock. Under OSHA’s General Duty Clause, Section 5(a)(1), employers have a recognised obligation to address known hazards where feasible controls exist — and OSHA’s fatigue hazards page explicitly frames long-hours fatigue in those terms. Ride-home programmes, taxi or ride-share vouchers, on-site nap rooms available before the drive home, and a no-questions-asked policy for workers who decline to drive when exhausted are all feasible and increasingly common.
A quick field test I use with supervisors: if a worker has to wait for the next helicopter in the morning because seas were too rough overnight, and they nap in the accommodation block for two hours before boarding, why are they allowed to get behind the wheel at the heliport after a nine-hour flat ferry transit the following morning? The risk calculus is identical; the intervention is cheaper than the crash.
Legal and Regulatory Expectations
International frameworks line up with reasonable consistency, even as jurisdictional detail varies. The International Labour Organization’s Night Work Convention (C171, 1990) sets baseline protections including free health assessments for night workers. The EU Working Time Directive (2003/88/EC) extends that floor — minimum daily rest of 11 consecutive hours, a 48-hour average working week, and night-work durations generally capped at 8 hours averaged over a reference period. UK Working Time Regulations 1998 implement the Directive domestically, and HSG256 is the operational guidance under the Management of Health and Safety at Work Regulations 1999.
In the United States, there is no single federal hours-of-work rule for general industry, but OSHA uses the General Duty Clause to pursue employers where recognised fatigue hazards are foreseeable and uncontrolled. Sector rules fill the gaps: FMCSA hours-of-service for commercial drivers, FAA Part 117 for pilots, and API RP 755 in refining and petrochemicals. NIOSH training modules — most notably the nurses’ long-hours programme — define expected employer practice.
ISO 45001:2018 applies globally, and ISO 45003:2021 was the first international standard to explicitly name shift work and unpredictable hours as psychosocial hazards requiring management. Adoption is accelerating through 2024–2026, and auditors working against ISO 45001 are increasingly asking to see 45003-aligned controls specifically. The IARC Monograph Volume 124 classification adds an occupational-health obligation that sits alongside the hours-of-work frameworks rather than replacing them.
Compliance with hours legislation alone is not a defence. A roster that satisfies the Working Time Directive on paper can still produce an FRI score in the red band and still result in an incident; regulators and courts have consistently held that meeting the hours rule is necessary but not sufficient.
Training and Worker Engagement: What Employers Must Communicate
Training is where most FRMS programmes quietly fail. HSG256 and ISO 45001’s consultation clauses both expect workers to be engaged in managing fatigue, but the training most sites deliver is a 20-minute e-learning module on sleep hygiene. That does not change behaviour.
Effective shift-work training, in my experience, covers:
- Sleep hygiene specifics — dark bedroom design, sleep-temperature, caffeine timing, and protection of daytime sleep
- Personal fatigue recognition — the Karolinska Sleepiness Scale used as a self-check before and during shift
- Supervisor-level impairment recognition — slowed speech, missed communication loops, repeated errors, head nods
- Commute-risk planning — when to decline to drive, what alternatives the employer offers, and how to access them
- Household education — because a spouse or family member who does not understand shift-work biology can undermine every control on the list
- Reporting routes into a just-culture system where workers can raise fatigue concerns without career consequences
When a charge hand on my platform first told me he was too tired to lead the morning handover, he expected push-back. The only correct answer was “thank you for telling me.” If that answer is not culturally available on your site, your training is not working regardless of what the course sign-off sheets say.
Emerging Developments in Circadian Workplace Safety
The field is moving quickly. Wearable fatigue monitoring — actigraphy watches, heart-rate-variability trackers, in-cab eye-tracking cameras — is maturing from novelty into operational tool, particularly in transport and heavy-equipment sectors. Biomathematical scheduling software built on the SAFTE and Three-Process models is increasingly used to stress-test rosters before they are issued rather than after an incident exposes them.
On the health side, the US National Toxicology Program’s 2021 cancer hazard conclusion formalised what IARC had found in 2020 — that persistent night-shift work disrupting circadian rhythms is a credible cancer hazard. The regulatory implications are still working through the system, but employer duty-of-care debates are already changing as a result.
Chrononutrition — eating patterns aligned to circadian biology rather than clock time — is an emerging research area with practical implications for shift-work mess-hall design and meal timing. The Working Time Society’s consensus statements, refreshed through 2024–2025, continue to update the evidence base on rotation direction, shift length, and light-management interventions. ISO 45003 adoption, now the fastest-growing strand of HSE management-system certification activity, is becoming the shorthand auditors use when they ask “how are you managing shift work as a psychosocial hazard?”
Key Takeaways
Circadian rhythm is a workplace hazard, not a lifestyle topic. The reasoning that controls other hazards — hierarchy of controls, FRMS, ISO 45001/45003 alignment, measurable leading indicators — works equally well here, and it is what regulators and courts will increasingly expect to see.
- Injury risk on night shifts runs 25–30% higher than day shifts, peaking between 0200 and 0600.
- Forward-rotating schedules, no more than three consecutive nights, and capped shift length cut risk.
- Working Time compliance is a floor, not a ceiling — an FRMS with FRI scoring is the standard.
- ISO 45003 now expects shift work to be managed as a psychosocial hazard.
- The commute home is often the highest-risk hour of the roster.
Frequently Asked Questions
Assess Your Own Roster — Three Questions
Take the schedule your site is running next month and answer three questions honestly. What safety-critical activities are scheduled to occur between 0200 and 0600, and could any of them be moved? What is the FRI score of your worst roster, and when did you last measure it? If one of your night-shift workers had a fatigue-related crash on the way home tomorrow, would your records show that the employer took recognised steps to address the hazard, or would they show a Working Time compliance check and nothing else?
Those three questions are where circadian rhythm and workplace safety stop being abstract. The biology is settled. The standards have caught up. The tools — FRI, KSS, forward rotation design, FRMS frameworks, ISO 45003 — exist and are operational today. The remaining variable is whether the organisation treats the body’s clock as a hazard with the seriousness it treats any other predictable, quantifiable risk on site. The operator staring nine seconds too long at a separator trend line at 0340 has told you that it is one.