

TL;DR
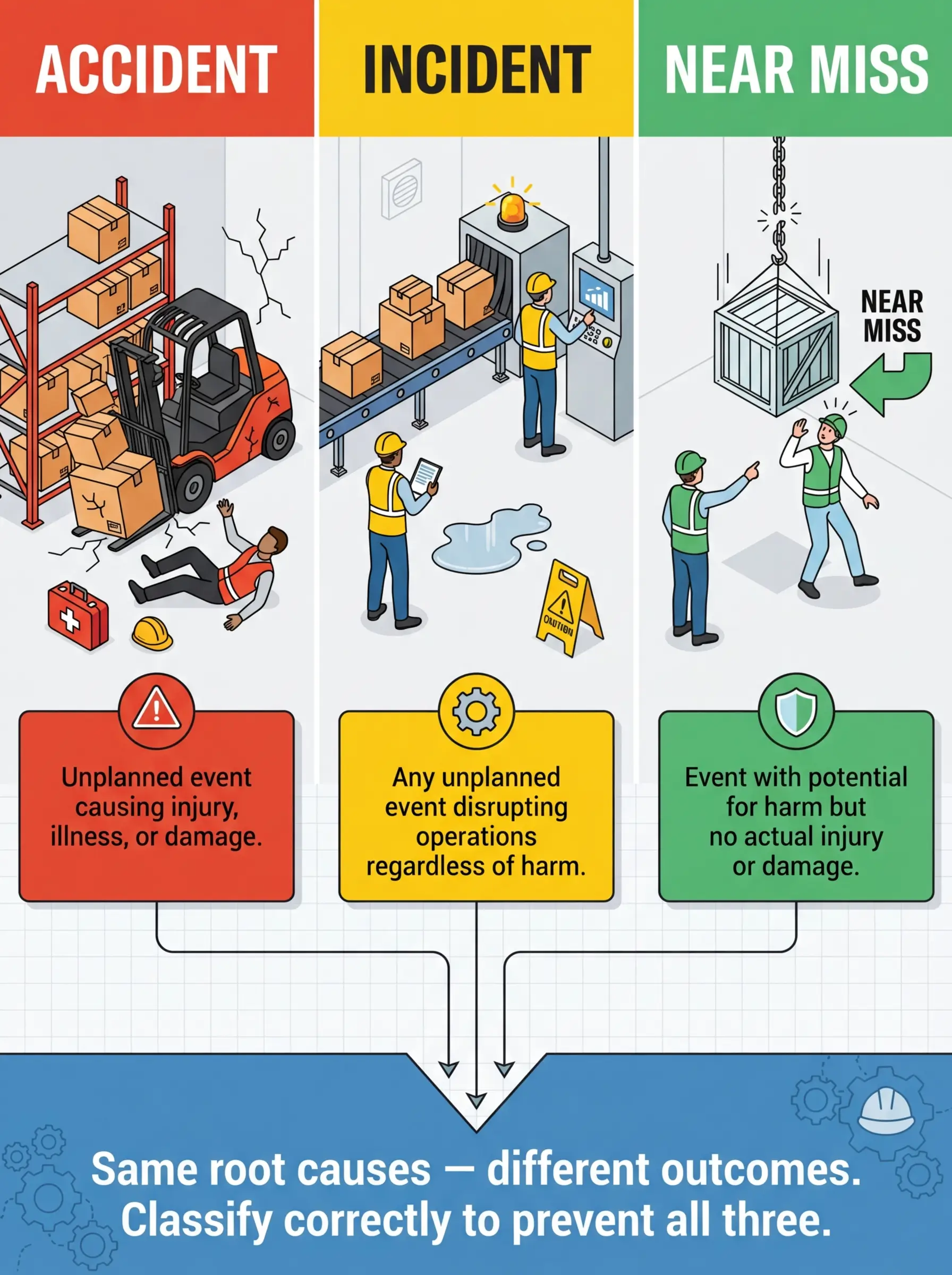
- These three terms are not interchangeable: An accident causes actual harm or damage, an incident is any unplanned event that disrupts operations (with or without harm), and a near miss is an event that could have caused harm but didn’t — the distinction drives how you investigate, report, and prevent recurrence.
- Near misses are your best free intelligence: Every near miss is a warning shot — the same conditions that produced a near miss today will produce an accident tomorrow if the controls aren’t fixed.
- Misclassification kills prevention: When sites lump everything under “incident” or ignore near misses entirely, they lose the data trail that predicts serious injuries and fatalities.
- Reporting culture determines survival: Organizations that punish near miss reporting don’t get fewer events — they get fewer reports, and then they get blindsided by a fatality they could have prevented.
- Classification is a skill, not a technicality: Getting this right isn’t academic — it determines your investigation depth, regulatory notification obligations, corrective action scope, and whether your safety management system actually learns from failure.
I was reviewing a contractor’s monthly safety report on a refinery turnaround when I noticed something that stopped me mid-page. The report listed zero accidents, zero incidents, and zero near misses for thirty consecutive days. Thirty days of hot work, confined space entries, scaffold erections, heavy crane lifts, and simultaneous operations — and apparently nothing unplanned had happened. Not a dropped tool. Not a tripped worker. Not a single moment where someone thought, “that was close.” I walked the site for two hours that afternoon and personally identified eleven conditions that qualified as near misses before lunch. The reporting system hadn’t failed. The understanding of what constitutes an accident, an incident, and a near miss had never been established in the first place.
This confusion isn’t rare — it’s epidemic. Across construction sites, manufacturing plants, oil and gas facilities, and mining operations worldwide, the terms “accident,” “incident,” and “near miss” are used interchangeably, misunderstood by supervisors, and inconsistently applied in reporting systems. The consequences are severe: regulatory violations, missed prevention opportunities, flawed safety metrics, and — ultimately — injuries and fatalities that a properly classified near miss report could have prevented months earlier. This article breaks down the precise, operational difference between accidents, incidents, and near misses, explains why correct classification is a life-safety issue, and provides a practical framework you can implement on any site tomorrow.
What Exactly Is an Accident in the Workplace?
An accident is an unplanned, uncontrolled event that results in actual harm to people, damage to property, or disruption to the environment. The defining characteristic is consequence — something measurable and negative has already happened.
The term carries weight in regulatory frameworks and insurance contexts. Under most occupational health and safety legislation, an “accident” triggers specific obligations: medical treatment, lost-time recording, statutory notifications, and formal investigation. OSHA’s recordkeeping standard under 29 CFR 1904 requires employers to record work-related injuries and illnesses that meet specific severity criteria — and every one of those recorded cases traces back to what most people would call an “accident.”
There are important characteristics that separate a true accident from other safety events on site:
- Actual harm has occurred: A worker has sustained an injury (from a minor laceration to a fatality), developed an occupational illness, or experienced a health effect requiring medical attention.
- Property or equipment damage is measurable: A vehicle collision, structural collapse, equipment failure, or fire has caused quantifiable material loss — even if no one was injured.
- Environmental impact has been realized: A chemical spill has reached soil or water, an emission has exceeded permitted limits, or ecological damage has occurred that requires remediation.
- The event was unplanned and uncontrolled: The harm was not an expected outcome of the work activity. If it was foreseeable and accepted without controls, that’s a management failure layered on top of the accident.
OSHA defines a recordable injury or illness as one that results in death, days away from work, restricted work activity, transfer to another job, medical treatment beyond first aid, loss of consciousness, or a significant injury or illness diagnosed by a physician or licensed healthcare professional. — 29 CFR 1904.7
Pro Tip: On every project I manage, I require supervisors to answer one question before classifying any event: “Did this event result in actual, measurable harm to a person, property, or the environment?” If yes — it’s an accident, and the investigation depth and reporting obligations escalate accordingly. That single question eliminates 80% of classification arguments on site.
What Is an Incident — and How Is It Different from an Accident?
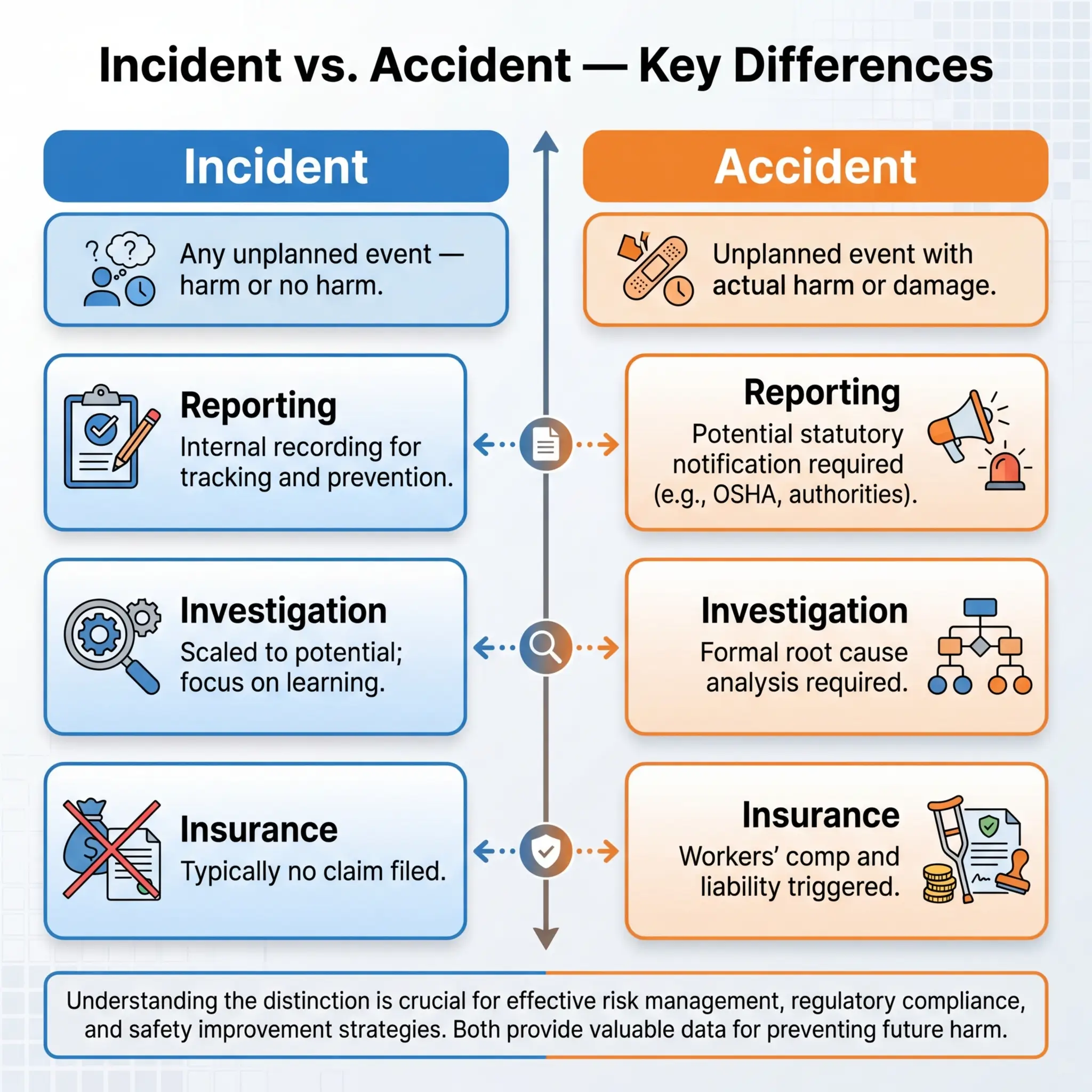
This is where most of the confusion lives. An incident is the broadest category — it covers any unplanned event that disrupts or has the potential to disrupt normal operations, regardless of whether harm actually occurred. Every accident is an incident, but not every incident is an accident.
Think of “incident” as the umbrella term. It captures the full spectrum: a worker sprains an ankle stepping off a scaffold platform (accident — harm occurred), a scaffold board comes loose and falls to a barricaded area below with no one underneath (near miss — potential for harm, no actual harm), and a crane operator notices unusual hydraulic pressure readings and shuts down the lift (abnormal condition — early intervention prevented escalation). All three are incidents. Only the first is an accident.
The practical differences between accidents and incidents become critical when you’re deciding investigation scope, regulatory notifications, and corrective action depth:
- Scope of consequence: Accidents always involve realized harm. Incidents may involve harm, potential harm, or simply unplanned operational disruption with no safety consequence at all.
- Regulatory notification triggers: Most jurisdictions require notification to regulators only for specific accident types — fatalities, hospitalizations, amputations, loss of sight (OSHA’s criteria under 29 CFR 1904.39), or dangerous occurrences listed in the UK’s RIDDOR regulations. A general incident without harm rarely triggers statutory reporting, though it must still be recorded internally.
- Investigation depth: Accidents demand formal root cause investigation with documented findings and corrective actions. Incidents without harm still warrant investigation — but the depth and formality scale with severity potential, not just actual outcome.
- Insurance and liability: Accidents with harm generate workers’ compensation claims, potential litigation, and insurance notifications. Incidents without harm typically don’t — but they create the documentary evidence that proves (or disproves) an organization’s due diligence if a future accident does occur.
I investigated a case on a pipeline construction project where a backhoe operator struck a live 11kV underground electrical cable that wasn’t marked on the utility survey drawings. The bucket contacted the cable, the circuit breaker tripped at the substation, and the power went out to a section of the nearby community for forty minutes. No one was injured. No equipment was damaged. But this was absolutely an incident — and a high-potential one at that. If the operator had been standing on wet ground instead of sitting in a rubber-tracked excavator, or if the cable insulation had been degraded, that same event would have been a fatal electrocution. The outcome was luck. The hazard exposure was identical to a fatality scenario.
Near Misses: The Most Valuable Safety Data You’re Probably Ignoring
A near miss — also called a near hit, close call, or good catch — is an unplanned event that had the realistic potential to cause injury, illness, property damage, or environmental harm but did not result in any actual harm due to chance, timing, or last-second intervention. The hazard was real. The exposure was real. The only thing that separated the near miss from an accident was luck or a narrow margin of circumstance.
Near misses are not minor events. They are not trivial observations. They are failed accidents — events where every condition for harm was present except the final contact between hazard and person. And that distinction makes them the single most valuable data source in any safety management system.
Why Near Misses Matter More Than Accident Data
The logic is straightforward, and it’s backed by decades of safety research and practical experience across every high-hazard industry. Here’s why near miss data consistently outperforms accident data as a prevention tool:
- Volume advantage: For every serious injury on a site, there are hundreds of near misses involving the same hazard conditions. Herbert William Heinrich’s research, later refined by Frank Bird and others, established the ratio principle — the base of the safety pyramid is populated overwhelmingly by near misses and unsafe conditions. You have far more near miss data points to analyze than accident data points, which gives you a statistically meaningful picture of where your real risks live.
- No human cost: Investigating a near miss gives you the same causal chain and contributing factors as investigating an accident — except no one got hurt. You get the learning without paying the price.
- Leading indicator power: Near miss frequency and type distribution are leading indicators — they tell you what’s about to go wrong. Accident rates are lagging indicators — they tell you what already went wrong. By the time your TRIR spikes, someone has already been injured.
- System failure visibility: Near misses expose the same system failures that cause accidents — inadequate procedures, poor supervision, missing barriers, training gaps, equipment deficiencies. The failure chain is identical. The outcome is the only variable.
The UK Health and Safety Executive (HSE) guidance states that near miss reporting provides “an opportunity to identify and address hazards before they cause harm” and that organizations with effective near miss reporting systems consistently demonstrate lower accident rates.
The Real Problem: Why Near Misses Go Unreported
I’ve audited near miss reporting systems across dozens of organizations in construction, oil and gas, manufacturing, and mining. The pattern is remarkably consistent. The reporting forms exist. The procedures exist. The monthly statistics exist. But the actual near miss reports are either absent, superficial, or obviously fabricated to meet a KPI target.
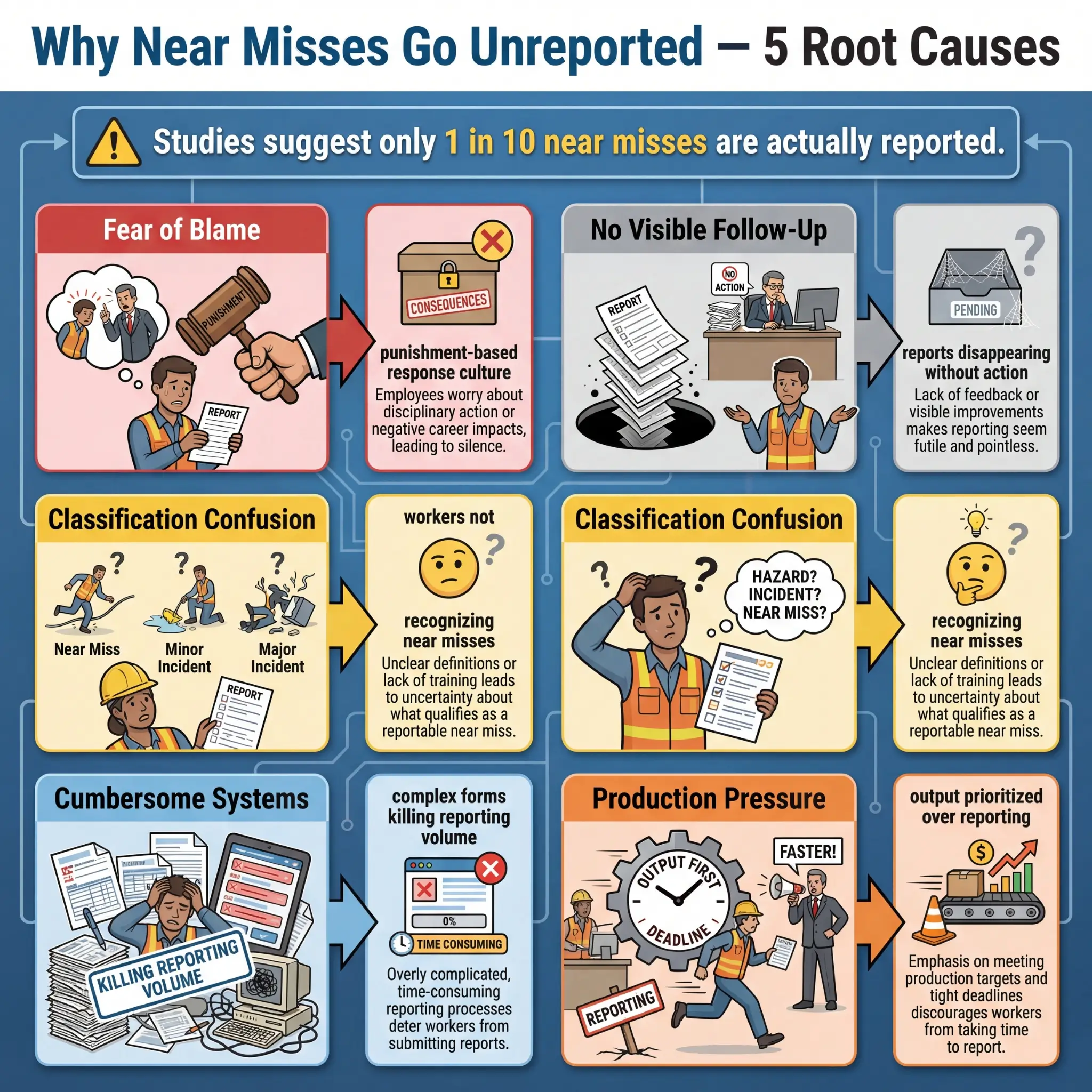
The root causes of underreporting trace back to the same organizational failures every time:
- Fear of blame: Workers won’t report near misses if they believe the report will be used to discipline them or their crew. This is the single biggest barrier, and it persists even in organizations that claim to have a “no-blame culture.” Words on a poster mean nothing if the supervisor’s first reaction to a near miss report is, “Who was responsible?”
- No visible response: When a worker submits a near miss report and sees zero follow-up — no investigation, no feedback, no corrective action — they learn that reporting is pointless. The system trained them to stop reporting.
- Classification confusion: Workers don’t report near misses because they don’t recognize them as near misses. They see a falling object that missed everyone and think, “Nothing happened, so there’s nothing to report.” This is a training failure, not a worker failure.
- Cumbersome reporting systems: A near miss report should take less than three minutes to submit. If it requires a 20-field form, supervisor countersignature, safety department approval, and a root cause analysis before submission, the friction will kill reporting volume within weeks.
- Production pressure: On fast-paced sites, stopping to fill out a near miss report competes with task completion. Unless the organization demonstrates that near miss reporting is valued as much as production output, production will always win.
Pro Tip: The single most effective near miss reporting intervention I’ve ever implemented is a 48-hour visible feedback loop. Every near miss report gets acknowledged within 24 hours and receives a visible corrective action or explanation within 48 hours — communicated directly to the person who reported it and posted on the site safety board. Reporting rates typically triple within the first month. Workers report when they see that reporting changes something.
The Safety Pyramid: How Accidents, Incidents, and Near Misses Relate
The relationship between these three categories isn’t random — it follows a well-documented pattern that every HSE professional should understand and apply operationally. The safety pyramid, originally conceptualized by H.W. Heinrich in 1931 and later validated and refined by Frank Bird (1969) and the ConocoPhillips Marine study (2003), illustrates a consistent ratio between the severity levels of safety events.
The core principle is simple and field-proven: for every serious or fatal accident at the top of the pyramid, there exists a much larger base of minor injuries, near misses, and unsafe acts or conditions that share the same root causes. The pyramid doesn’t suggest that every near miss will escalate to a fatality — it demonstrates that fatalities and near misses share the same causal DNA.
The approximate ratios from Bird’s study of 1.7 million accidents across 297 organizations illustrate this relationship clearly:
| Pyramid Level | Event Type | Approximate Ratio (Bird, 1969) |
|---|---|---|
| Top | Serious or Fatal Injury | 1 |
| Second | Minor Injury | 10 |
| Third | Property Damage (no injury) | 30 |
| Base | Near Misses / No Visible Loss | 600 |
The operational implication is direct. If you want to prevent the one fatality at the top, you have to address the 600 near misses at the base. Waiting until someone gets seriously hurt before investigating and implementing controls is the most expensive, most harmful, and least effective approach to safety management. The data is sitting at the bottom of the pyramid — in near miss reports, hazard observations, and unsafe condition reports — if you choose to collect and act on it.
I worked on a mining operation where the safety team tracked near misses involving falling ground in underground development headings for eighteen months. The data showed a clear pattern: 73% of falling ground near misses occurred within the first two meters behind the active face, in ground that had been scaled and declared safe. The investigation revealed that the scaling procedure didn’t account for stress redistribution in the hours after blasting. The procedure was revised, a mandatory re-scaling protocol was added four hours after each blast, and falling ground incidents dropped by 61% over the following year. That prevention came entirely from near miss data — not from waiting for a rock fall fatality.

A Practical Classification Framework for Site Use
Theory is useful, but supervisors need a tool they can apply on the ground — at the moment an event occurs, under pressure, without consulting a textbook. The classification framework below is one I’ve refined across multiple projects and industries, and it works because it asks simple, sequential questions.
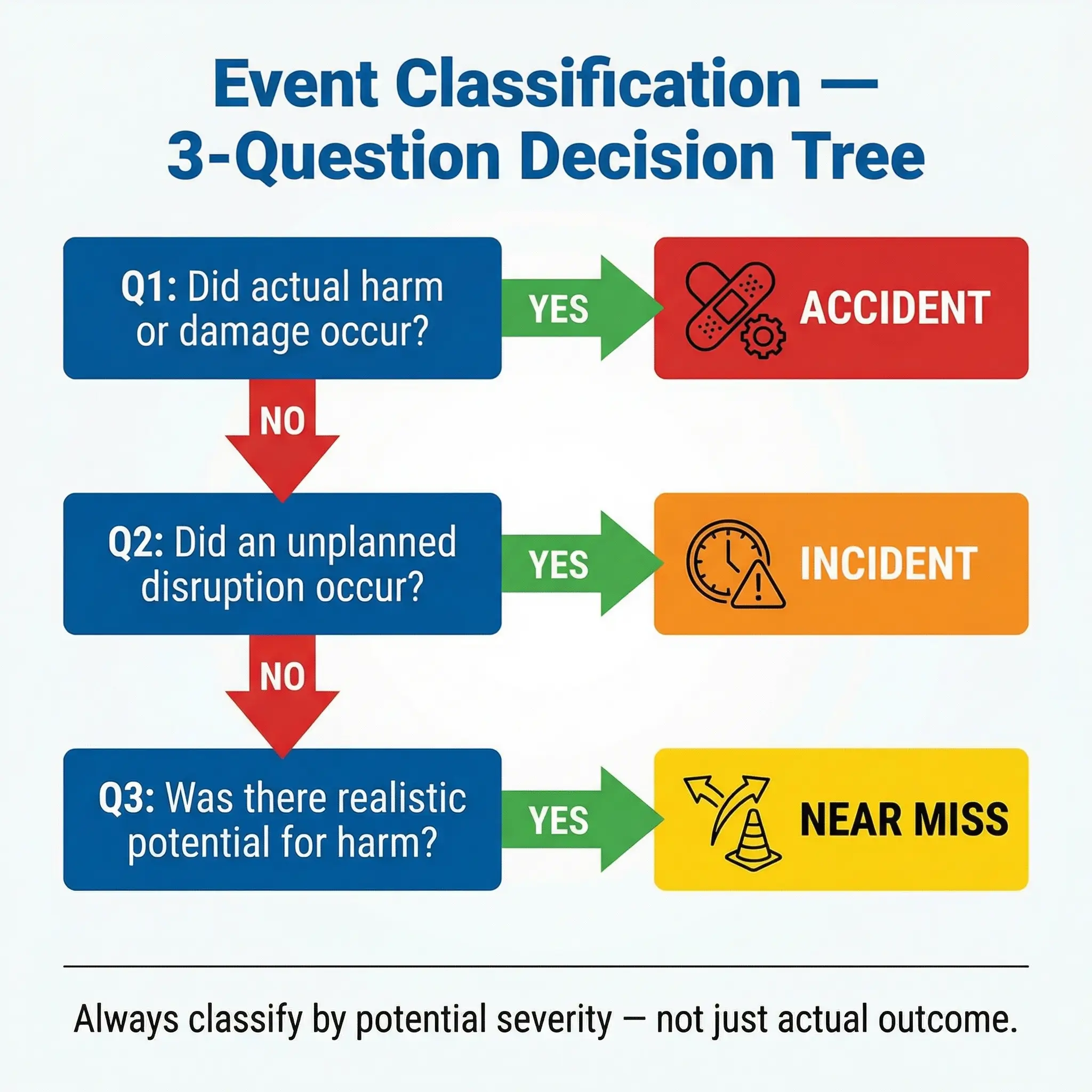
The following decision-tree approach has been tested and validated on construction mega-projects, refinery turnarounds, and mining operations. It requires the supervisor to answer three questions in order:
- Did anyone sustain an injury, illness, or health effect — or was there measurable property damage or environmental impact? If YES → classify as Accident. Initiate formal investigation, assess regulatory notification requirements, and begin corrective action process immediately.
- Did an unplanned event occur that disrupted or could have disrupted normal operations? If YES → classify as Incident. Determine severity potential (what could have happened under slightly different circumstances), and scale investigation depth accordingly.
- Was there a realistic potential for injury, illness, damage, or environmental harm — but no actual harm occurred? If YES → classify as Near Miss. Record, investigate root causes, and implement corrective actions as if the harm had actually occurred.
The critical concept embedded in this framework is severity potential — not just actual outcome. A near miss where a 20kg fitting falls from a pipe rack and lands one meter from a worker’s head has the severity potential of a fatality. It must be investigated with the same rigor as a fatal accident, even though the actual outcome was zero harm. This is where most organizations fail. They scale investigation effort to actual consequence instead of potential consequence, and they systematically under-investigate the events that are most predictive of future fatalities.
Common Classification Mistakes to Avoid
Even experienced supervisors make classification errors that distort safety data and compromise prevention efforts. These mistakes are preventable with clear definitions and regular reinforcement:
- Calling everything an “incident” to avoid the word “accident”: Some organizations have banned the word “accident” because they believe it implies the event was unavoidable. While the intent is good, replacing all classification with a single term (“incident”) destroys the severity differentiation that drives investigation depth and corrective action priority. Use all three terms with clear definitions.
- Downgrading accidents to near misses: When a worker sustains a minor laceration but doesn’t report it, or when the supervisor classifies a first-aid case as “no harm,” the accident gets reclassified as a near miss or not recorded at all. This is data falsification — whether intentional or not — and it blinds the organization to its actual injury trends.
- Ignoring near misses because “nothing happened”: This is the most dangerous classification failure. The near miss contained every causal factor of a serious accident. Dismissing it because no one was hurt is equivalent to ignoring a fire alarm because the building hasn’t burned down yet.
- Confusing hazard observations with near misses: A hazard observation identifies a condition that could lead to an event — an unguarded floor opening, a missing fire extinguisher, a frayed sling. A near miss is an event that actually occurred — a worker nearly stepped into the unguarded opening, a small fire started where the extinguisher was missing. Both are valuable reports, but they require different response protocols.
Pro Tip: On every project kickoff, I conduct a 30-minute classification exercise with supervisors using ten real-world scenario cards. Each card describes an event, and supervisors must classify it as accident, incident (non-injury), or near miss — and explain their reasoning. The exercise consistently reveals that even experienced supervisors misclassify 3–4 out of 10 scenarios. It’s the single fastest way to calibrate site-wide classification consistency.
Why Correct Classification Drives Real Prevention
Getting the terminology right isn’t a semantic exercise — it directly determines how effectively an organization prevents injuries and fatalities. The classification of a safety event sets off a chain reaction that affects investigation depth, resource allocation, regulatory compliance, and organizational learning. Get the classification wrong, and every downstream decision is compromised.
Here is how correct classification connects to tangible safety outcomes across the system:
- Investigation quality: An event classified as an accident triggers a formal root cause investigation — typically using a structured methodology like TapRooT, ICAM, or the “5 Whys” technique backed by barrier analysis. An event misclassified as a near miss might receive only a superficial review. If the event was actually an accident, the root causes go unidentified, and the same conditions persist until the next — potentially more severe — occurrence.
- Corrective action adequacy: The corrective actions that emerge from an investigation are scaled to the event’s classification and severity potential. An accident investigation typically generates engineering controls, procedural revisions, and systemic changes. A misclassified near miss might generate only a toolbox talk reminder. The hazard remains.
- Regulatory compliance: Misclassifying a recordable injury as a non-recordable incident or a near miss is a violation of OSHA’s recordkeeping standard (29 CFR 1904) and can result in citations, penalties, and — critically — the loss of the organization’s credibility with the regulator. Under the UK’s RIDDOR 2013, failure to report specified accidents and dangerous occurrences is a criminal offence.
- Safety metrics integrity: TRIR, LTIFR, DART rate, and severity rate calculations all depend on accurate accident classification. If accidents are underreported or misclassified, the metrics tell a false story — and management makes resource decisions based on that false story. The site looks safe on paper while the real risk profile deteriorates.
- Organizational learning: The difference between an organization that learns from failure and one that repeats it often comes down to whether safety events are correctly classified, properly investigated, and honestly reported. A robust near miss reporting system feeds the lessons-learned pipeline. A system where near misses are ignored and accidents are downgraded produces nothing but a false sense of security.
| Classification Outcome | Investigation Triggered | Corrective Action Scope | Regulatory Reporting | Learning Value |
|---|---|---|---|---|
| Accident (correctly classified) | Formal root cause analysis | Engineering, procedural, systemic | Statutory notifications as required | High — full causal chain identified |
| Near Miss (correctly classified) | Investigation scaled to severity potential | Proportional to potential consequence | Internal recording | High — same causal DNA as accident |
| Accident misclassified as Near Miss | Superficial or none | Minimal — toolbox talk at best | Missed statutory obligation | Near zero — root causes unidentified |
| Near Miss ignored entirely | None | None | Not applicable | Zero — prevention opportunity lost |
Building a Reporting Culture That Actually Works
The best classification framework in the world is worthless if workers don’t report events. And workers won’t report events unless the organizational culture makes reporting safe, simple, and visibly valued. This isn’t a poster campaign problem — it’s a leadership behavior problem that must be solved at every level from the CEO to the frontline supervisor.
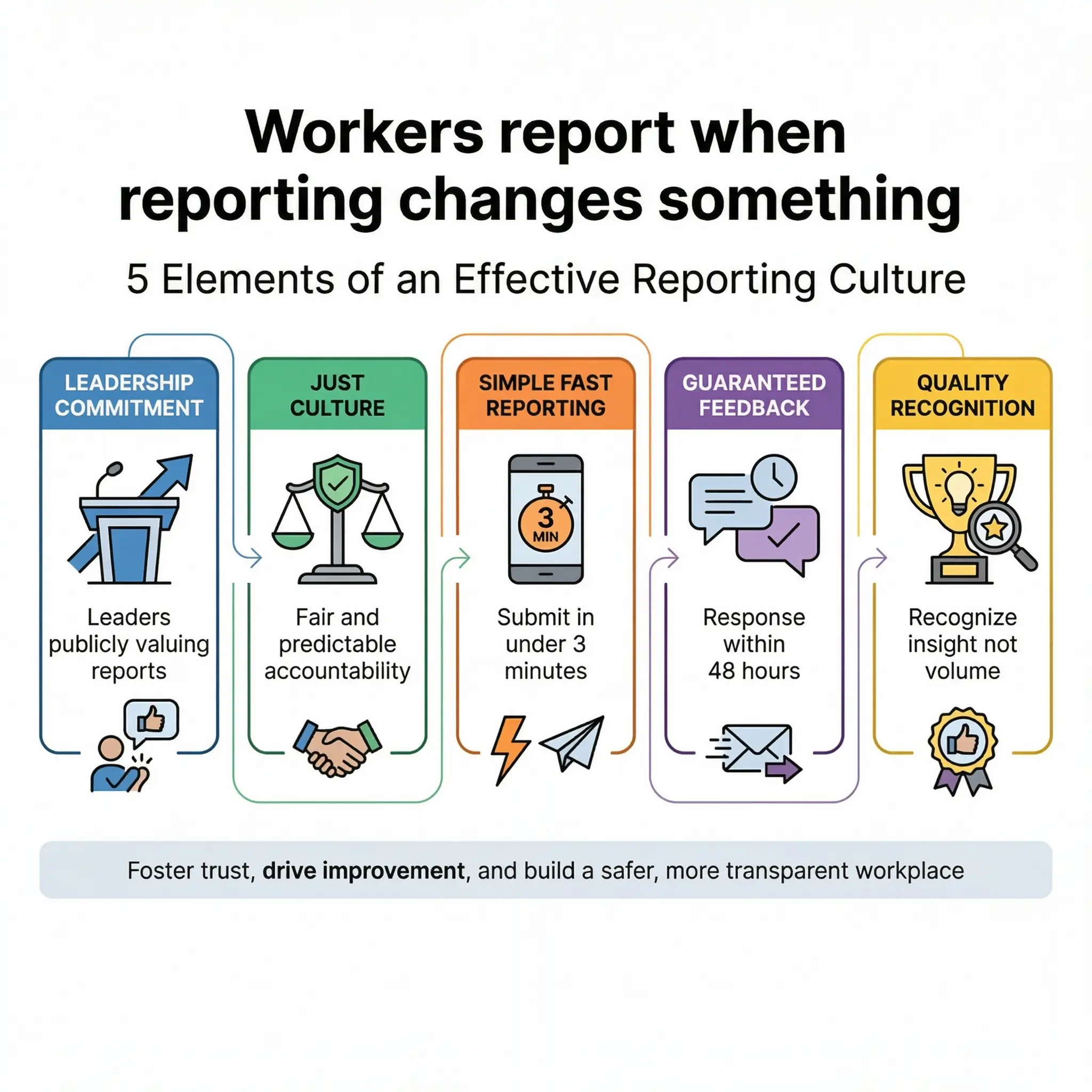
The following elements are present in every effective reporting culture I’ve encountered — and absent in every dysfunctional one:
- Visible leadership commitment: Senior leaders publicly acknowledge near miss reports, reference them in safety reviews, and allocate resources to address them. When a project director opens a weekly meeting by discussing a near miss and the corrective action taken, that signal propagates through the entire organization within days.
- Just culture implementation: A just culture doesn’t mean no accountability — it means accountability is proportional and predictable. Honest reporting of errors and near misses is protected. Willful violations, reckless behavior, and sabotage are not. Workers must understand the boundary clearly, and the boundary must be applied consistently.
- Simple, fast reporting mechanisms: The near miss report should be submittable in under three minutes — by phone, by app, by card drop, or by verbal report to a supervisor who records it. Every additional friction point reduces reporting volume exponentially.
- Guaranteed feedback loop: Every report receives acknowledgement within 24 hours and a visible outcome (corrective action, investigation finding, or explanation of why no action was needed) within 48–72 hours. This is the mechanism that sustains reporting volume over time.
- Recognition without reward gaming: Recognize reporting quality and thoughtfulness — not volume. When organizations incentivize near miss report quantity, they get fabricated reports and observation inflation. When they recognize the report that identified a critical hazard and prevented a serious injury, they get meaningful data.
I managed a construction project where we implemented this exact framework — simplified reporting cards, 48-hour feedback commitment, and weekly “Best Catch” recognition at the all-hands meeting. Near miss reporting went from 4 reports per month to over 60 within eight weeks. More critically, three of those near miss reports identified fall hazard conditions on temporary works that, upon engineering review, were confirmed to be structurally inadequate. Those structures were being used daily by dozens of workers. The near miss reports didn’t just improve our statistics — they prevented what our structural engineer estimated could have been a multi-casualty collapse.
How Different Regulations Define These Terms
One complication that catches multinational organizations off guard is that different regulatory frameworks define “accident,” “incident,” and “near miss” with subtle but operationally significant differences. Understanding these variations is essential for organizations operating across multiple jurisdictions.
The core definitions align across most frameworks, but the reporting thresholds and terminology differ in ways that affect compliance obligations:
| Framework | Term for Harm Event | Term for No-Harm Event | Reporting Threshold |
|---|---|---|---|
| OSHA (US) | Recordable injury/illness | Near miss (not formally defined in standards) | Fatality within 8 hrs; hospitalization, amputation, eye loss within 24 hrs |
| HSE UK (RIDDOR 2013) | Accident / Dangerous occurrence | Near miss (referenced in guidance, not statute) | Fatal/specified injuries; dangerous occurrences; over-7-day incapacitation |
| ISO 45001:2018 | Incident (includes near misses) | Near miss (subset of incident) | Organization-defined; must investigate all incidents including near misses |
| EU Framework Directive 89/391 | Accident at work | Near miss (member state variation) | Varies by member state transposition |
| IFC Performance Standard 2 | Occupational incident | Near miss | Fatalities, lost-time events; contractor reporting required |
ISO 45001:2018 (Clause 3.35) defines an incident as “an occurrence arising out of, or in the course of, work that could or does result in injury and ill health.” The standard’s note explicitly states: “An incident where no injury and ill health occurs may be referred to as a ‘near miss.'”
The practical takeaway for multinational operations is this: your internal classification system must be at least as rigorous as the most demanding jurisdiction you operate in. If you operate in both the US and the UK, your reporting thresholds must meet both OSHA and RIDDOR requirements. If your management system is certified to ISO 45001, your incident definition must encompass near misses — the standard requires it.
Conclusion
The difference between an accident, an incident, and a near miss is not a vocabulary quiz — it’s the foundation of every investigation you conduct, every corrective action you implement, and every prevention strategy you build. Get the classification wrong, and you investigate the wrong things with the wrong depth. Get it right, and you build a safety system that learns from every event — especially the ones where no one got hurt.
Near misses are not lucky breaks to be grateful for and forgotten. They are the clearest, cheapest, most honest signal your operation will ever give you about where serious harm is waiting to happen. Every near miss report that gets investigated and acted on is a potential fatality that never occurs. Every near miss that goes unreported is a prediction your organization chose to ignore.
The organizations I’ve seen sustain genuinely low injury rates over years — not through data manipulation, but through actual harm prevention — share one characteristic above all others: they treat near misses with the same investigative seriousness as accidents. They understand that the causal chain is identical, that only the outcome differs, and that outcomes are determined by margins too thin to rely on. Classification isn’t paperwork. It’s the mechanism through which an organization decides whether it will learn from failure or repeat it. Get it right, and your people go home the way they arrived.