

03:12 in the control room. The screens throw a dim blue wash over four operators holding a continuous caster that hasn’t stopped running in seventeen days. Between roughly 2 and 5 a.m., the human body drops into its deepest biological trough of the day. Core temperature falls. Melatonin peaks. Reaction time slows. On a 24/7 industrial site, that is the exact window where shift work safety becomes something much harder than a scheduling problem — the crew still has to keep a 40-tonne ladle moving, confirm a permit over crackling radios, and not miss the one anomaly on a screen full of normal.
Shift work sits behind major industrial incidents, chronic disease burdens that cost more than most occupational illnesses combined, and a fatal commute-home risk that many employers still don’t even log as work-related. This guide covers what two decades of chronobiology and epidemiology tell us shift work actually does to workers, and — more usefully for a safety professional — the hierarchy of controls, risk-assessment methods, and management-system structures that convert that evidence into a defensible programme.
What Shift Work Actually Is in Safety Terms
Shift work, in regulatory terms, means any working pattern that falls outside the conventional 07:00–18:00 window, with particular attention to any shift that includes at least three hours between midnight and 05:00. That is NIOSH’s working definition, and HSE guidance effectively aligns with it. Roughly 20 to 25% of the workforce in industrialised economies works non-standard hours, and in 24/7 process environments like the mill floor I spent most of last year embedded in, that figure sits closer to 70% of operational headcount.
Not every shift pattern carries the same fatigue load. Five configurations dominate across 24/7 industries:
- Fixed day, evening, or night shifts — workers stay on one pattern, for better or worse.
- Rotating shifts — workers cycle through two or three patterns, forward (day → evening → night) or backward.
- Extended 12-hour shifts — often compressed into a four-on, four-off structure.
- Split shifts — divided by a long unpaid break.
- On-call or standby — unpredictable call-outs with short notice periods.
Each configuration produces a different fatigue fingerprint, and employers who treat them interchangeably in a risk assessment tend to miss where the actual risk concentrates. HSE’s Managing Shift Work guidance (HSG256), available at hse.gov.uk, is explicit that this is a hazard requiring a formal assessment under the Management of Health and Safety at Work Regulations 1999 — not a workforce-planning preference.
How Shift Work Harms the Body: The Circadian Mechanism
The human body runs on a roughly 24.2-hour internal clock, anchored in a cluster of cells called the suprachiasmatic nucleus above the optic chiasm. Light hitting the retina — especially blue wavelengths — is the dominant zeitgeber synchronising that master clock to the external day. When light arrives at the wrong biological time, the system misaligns.
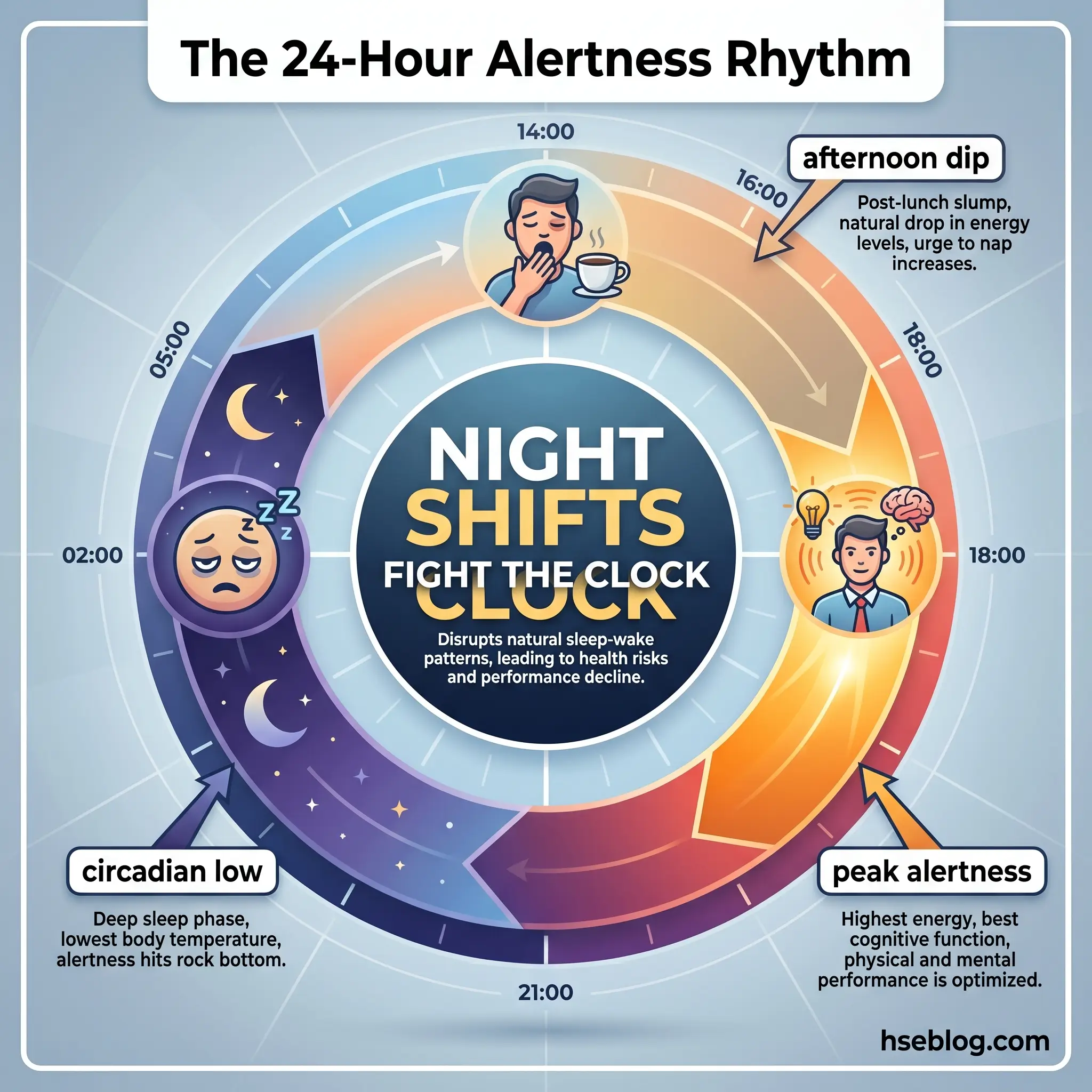
Three things happen during a night shift that account for most of the downstream harm. First, melatonin — the hormone the pineal gland releases in darkness to promote sleep — is suppressed by workplace ambient light. Second, cortisol, which normally rises before dawn to prepare the body for activity, is pushed out of phase with actual wake time. Third, core body temperature continues falling through the early hours regardless of what the worker is doing, bottoming out between 04:00 and 05:00 — precisely when continuous operations often require the highest vigilance.
Daytime sleep after a night shift is typically 2 to 4 hours shorter than an equivalent night sleep, and REM architecture is degraded. Even workers on permanent nights for years rarely achieve complete circadian adjustment, because morning sunlight on the drive home resets the central clock while peripheral clocks in the liver, pancreas, and gut stay desynchronised. That internal desynchronisation — not “tiredness” — is what drives the chronic disease risk downstream.
Short-Term Health and Safety Effects
Within days of starting a night roster, most workers experience measurable cognitive impairment. Sustained wakefulness of 24 hours produces performance decrements comparable to a blood alcohol concentration of 0.05 to 0.10% — levels at which driving is an offence in most jurisdictions. The impact is not linear: attention lapses and microsleeps cluster in the 02:00–05:00 window and stretch further into the shift on each consecutive night.
Watch For: A crew that goes quiet on the radio between 03:00 and 04:30 is not necessarily disciplined. It is the hour when microsleeps are most common, and a quiet handover channel can mean operators are blinking hard to stay awake, not that the site is running smoothly.
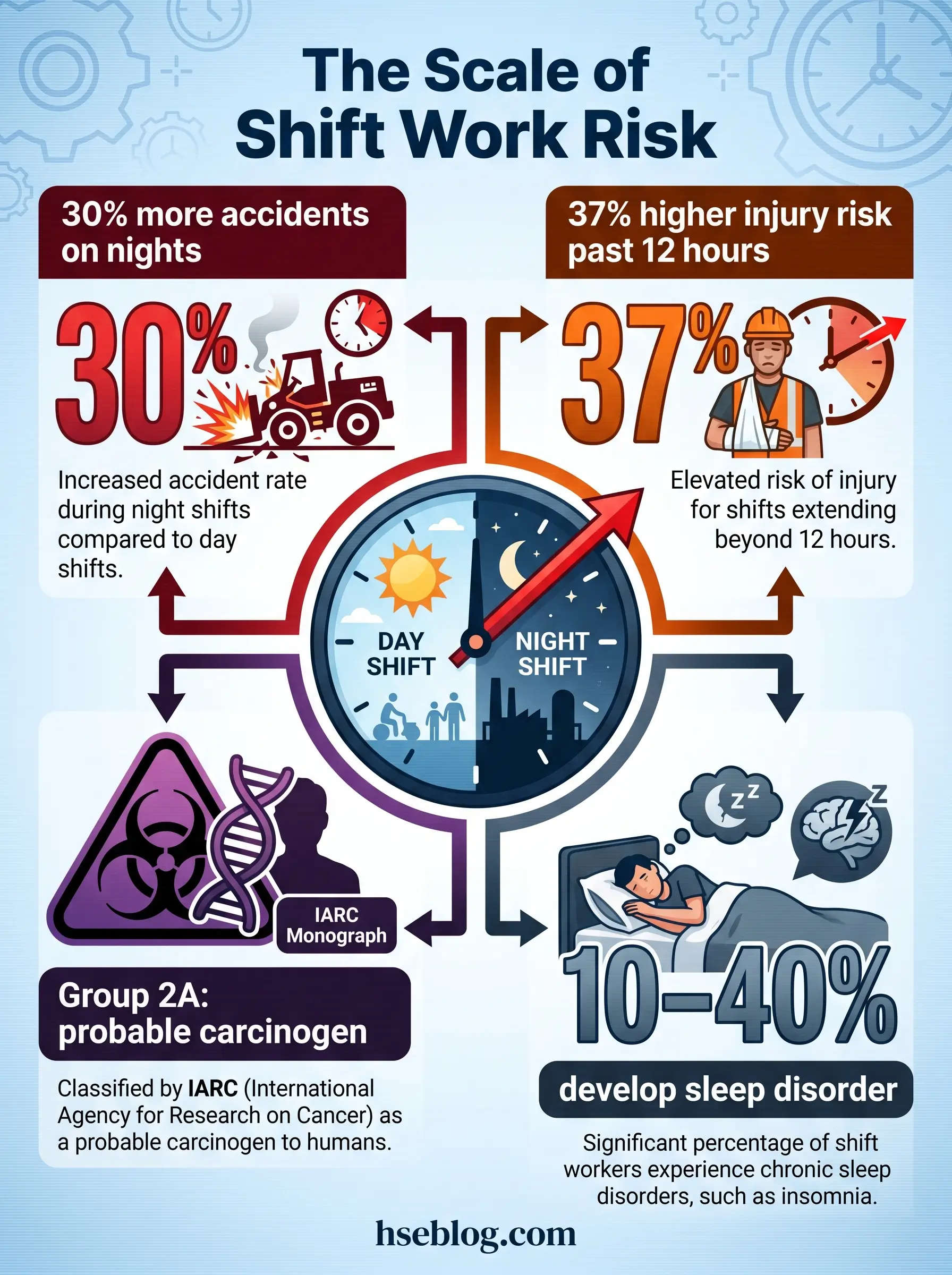
Beyond cognition, the acute physical effects show up quickly. Gastrointestinal complaints — heartburn, constipation, irregular appetite — are near-universal. Mood disturbance and irritability degrade the quality of shift handovers, which is where a startling proportion of serious injuries actually originate. And a recognised clinical condition — Shift Work Sleep Disorder (SWSD) — develops in 10 to 40% of shift workers, characterised by insomnia during the main sleep period, excessive sleepiness during the work period, and symptoms persisting for at least three months.
SWSD is not a diagnosis workers tend to volunteer. In one year at the mill’s on-site occupational health clinic, three operators came in complaining of depression; the clinic nurse’s first questions about sleep patterns uncovered SWSD in every case.
Long-Term Chronic Health Effects
The damage shift work does over years is where the safety conversation usually stops and the medical literature takes over. Both need to be in the room for a control programme to make sense.
Cardiovascular and metabolic disease
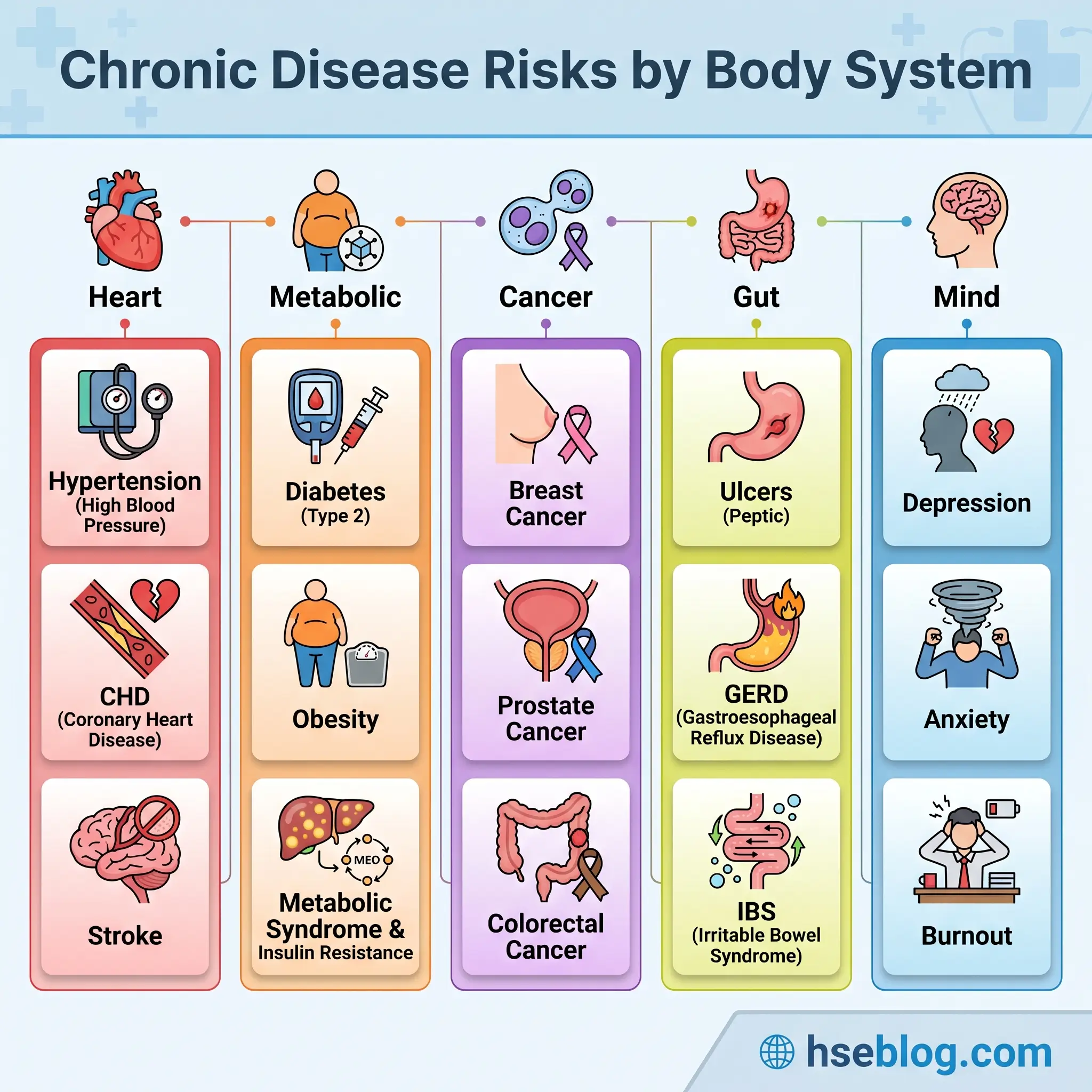
Shift work is independently associated with hypertension, coronary heart disease, and ischaemic stroke. The likely mechanisms include chronic sympathetic activation, disrupted blood-pressure dipping during daytime sleep, and metabolic knock-on effects from circadian misalignment. Metabolic effects — obesity, type 2 diabetes, dyslipidaemia, metabolic syndrome — show the clearest dose-response relationship with years of night work, and they cluster in workers who combine shift work with inactivity and poor-quality eating windows.
Cancer and the IARC classification
In its 2019 re-evaluation, published as Monograph Volume 124, the International Agency for Research on Cancer classified night shift work as Group 2A — probably carcinogenic to humans. The strongest evidence is for female breast cancer, with supporting signals for prostate and colorectal cancers. The US National Toxicology Program’s hazard assessment at ntp.niehs.nih.gov concluded with high confidence that persistent night shift work that disrupts circadian rhythms can cause breast cancer in women and may cause prostate cancer in men.
Why “persistent” matters for risk assessment
“Persistent night shift work” in the IARC and NTP sense means long-duration (often 20+ years), frequent (multiple nights per week), and starting in early adulthood. That matters operationally: a 22-year-old starting as a permanent night furnace operator is not in the same exposure category as a 55-year-old rotating through two nights a month. Employer health-surveillance programmes should reflect that gradient.
Gastrointestinal, reproductive, and mental health effects
Peptic ulcers, GERD, and irritable bowel syndrome are elevated in shift workers, as are depression, anxiety, and burnout — the last driven partly by the erosion of family and social routines. Reproductive effects matter for risk assessment: menstrual irregularity, reduced fertility, and in pregnant night workers, higher rates of preterm birth and miscarriage. The EU Pregnant Workers Directive 92/85/EEC codifies this into a duty to offer day-work alternatives or paid suspension where night work is medically contraindicated.
Safety Risks: Accidents, Errors, and the Drive Home
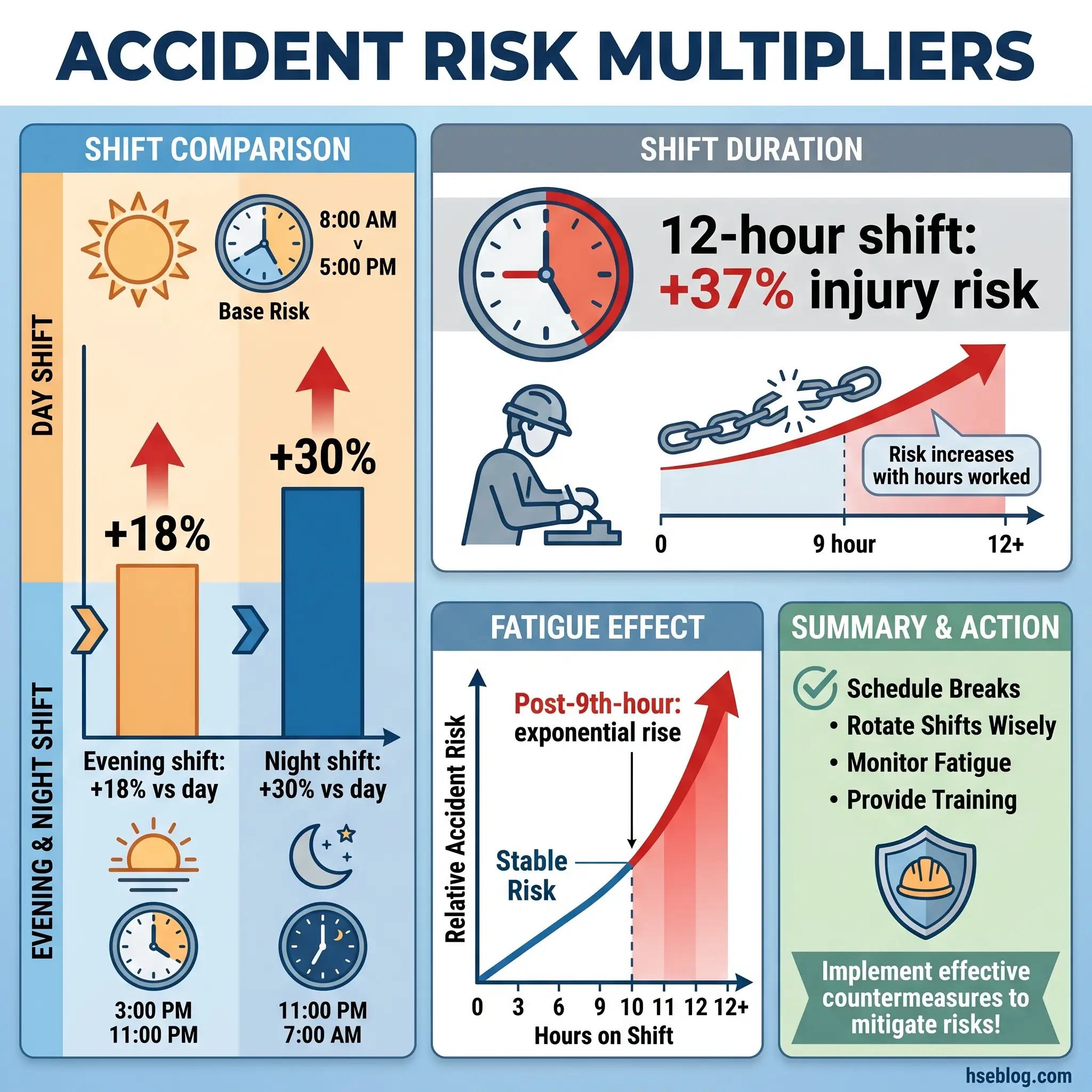
Health risks accumulate over years. Safety risks fire within a single shift — and the curve is steep. The OSHA synthesis of international shift-work epidemiology, at osha.gov/worker-fatigue, puts accident and injury rates 18% higher on evening shifts and 30% higher on night shifts compared with day shifts. Injury risk rises roughly 37% on 12-hour shifts, with the steepest climb after the ninth hour on task. Risk compounds across consecutive nights: the fourth night of a block is demonstrably worse than the first.
Behind those averages sits a well-known catalogue of incidents in which fatigue featured as a contributory factor: Three Mile Island’s early-morning operator errors, the Exxon Valdez grounding, the Challenger pre-launch decision, the Texas City BP refinery explosion, and Chernobyl’s 01:23 test sequence. None of these happened because of shift work alone, but the shift-work contribution is present in every investigation report.
The commute home is the part most programmes underweight. Research published in PNAS tracked near-crash events in night-shift workers immediately after their shifts and found drowsy-driving risk spikes sharply after roughly 45 minutes on the road. An estimated 9.5 million US shift workers — about 15% of the workforce — are in the elevated drowsy-driving category, and drowsy drivers were involved in around 21% of fatal crashes analysed between 2009 and 2013. For medical residents, NEJM data showed every extended shift scheduled in a month increased the monthly commute-crash risk by 16.2%.
The Fix That Works: If your operators drive home after a 12-hour night shift, the commute is part of the occupational risk profile whether your legal team likes it or not. Pool vehicles, taxi provision, on-site sleep rooms, and a two-hour nap option after consecutive nights change the fatality arithmetic in ways that no amount of sleep-hygiene training ever will.
Who Is Most Vulnerable
On paper, a shift roster treats workers as interchangeable. In practice, shift tolerance varies substantially between individuals, and regulators expect employers to identify vulnerable groups rather than apply one-size-fits-all schedules. Chronotype is the first filter: morning-oriented workers tolerate early starts poorly but handle late-afternoon finishes well, while evening-oriented workers are the opposite. Age is the second: tolerance drops sharply after 40 to 45, which is often the exact point at which senior operators with the deepest technical knowledge are still being assigned to the most demanding rotations.
The specifically recognised vulnerable categories — the ones a competent risk assessment must name — are:
- Pregnant workers and new mothers, with transfer rights under the EU Pregnant Workers Directive and the UK Management Regulations.
- Workers with pre-existing cardiovascular, metabolic, gastrointestinal, psychiatric, or sleep disorders (diabetes, epilepsy, major depression, obstructive sleep apnoea, IBD).
- Workers over 50, particularly on rotating or backward-rotating schedules.
- Workers with long commutes (more than 45 minutes each way, especially on rural or high-speed networks).
- Workers holding second jobs, where total hours across employers push into fatigue-critical territory.
The UK Working Time Regulations and the EU Working Time Directive both give night workers a right to a free health assessment before assignment and at regular intervals thereafter. In practice, that assessment is the single most useful point at which vulnerabilities are identified — and the single most underused.
The Regulatory Framework for Managing Shift Work
The international regulatory structure around shift work is layered, and a safety professional leading a programme needs to be able to locate a decision in the right tier. At the top sit two ILO instruments: the Hours of Work (Industry) Convention, 1919 (No. 1), which established the 8-hour-day and 48-hour-week baseline still embedded in most national laws, and the Night Work Convention, 1990 (No. 171), which requires health assessments, transfer rights to day work where medically indicated, and specific protections for pregnant workers.
At the European level, the Working Time Directive 2003/88/EC sets operational limits that apply across the EU and, in modified form, the UK: 11 consecutive hours of daily rest, 24 hours of weekly rest, an average 48-hour working week measured over a reference period, an 8-hour limit on night shifts involving particular hazards or heavy physical or mental strain, and a statutory right to free health assessments for night workers. The UK’s HSG256 operationalises these duties into a risk-based programme under the Management of Health and Safety at Work Regulations 1999.
In the United States, there is no federal shift-work standard as such, but OSHA applies the General Duty Clause — Section 5(a)(1) of the OSH Act — to require employers to address recognised fatigue hazards from extended or irregular shifts. Sector-specific hours-of-service rules layer on top: FMCSA for trucking, FRA for rail, FAA for aviation, and in the process industries, API Recommended Practice 755 on Fatigue Risk Management Systems, developed in the aftermath of the 2005 Texas City refinery incident.
ISO 45001:2018 ties the programme to the management system. Clauses 6.1.2 (hazard identification) and 8.1.2 (eliminating hazards and reducing OH&S risks) require shift work and fatigue to be identified as hazards and managed through the Plan-Do-Check-Act cycle. Overarching the surveillance question, the IARC 2A classification now gives employers in most jurisdictions an evidentiary basis for including cancer-relevant screening in long-term night-worker programmes.
Conducting a Shift Work Risk Assessment
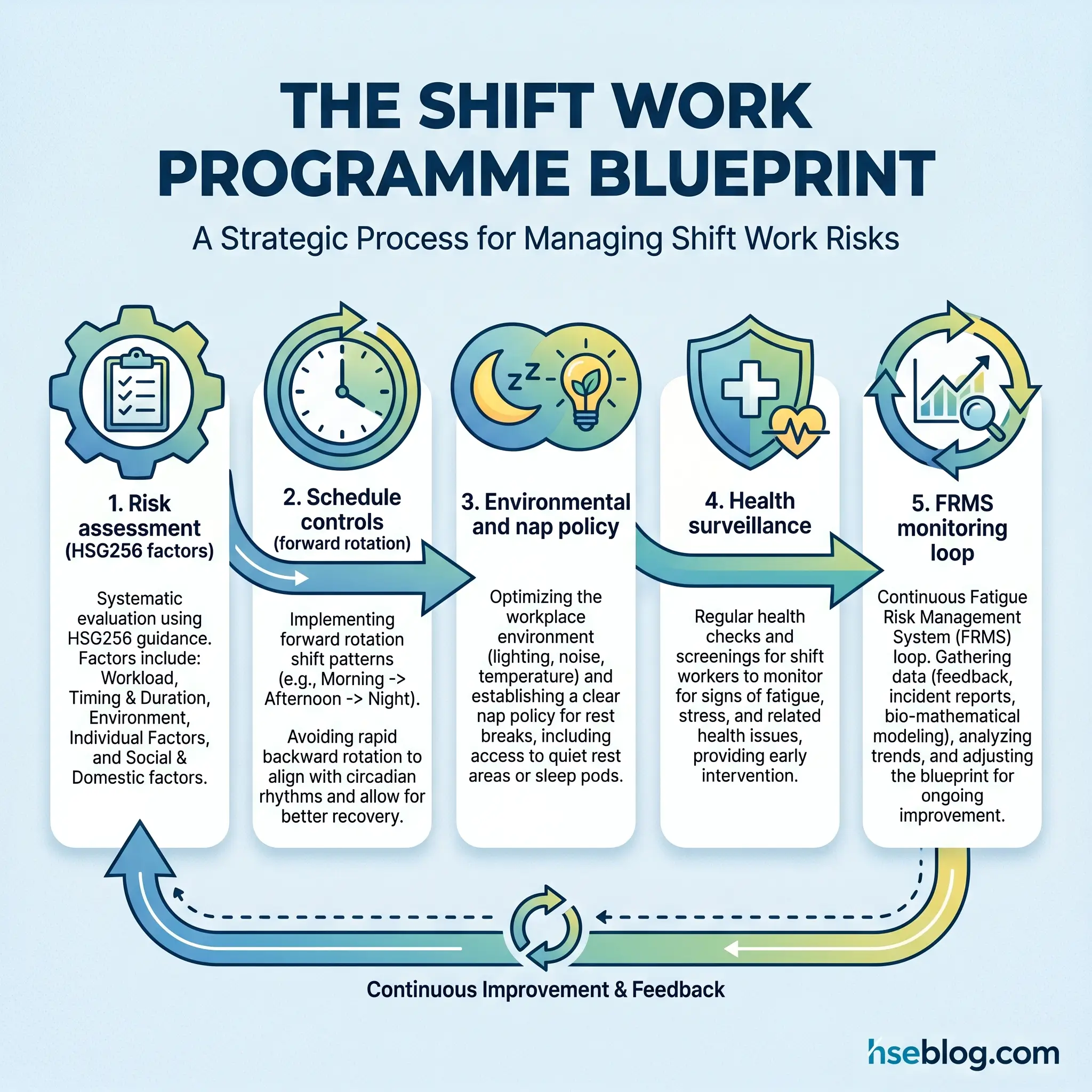
The problem with most shift-work risk assessments is that they assess the schedule on paper rather than the shift as it actually runs. A functional assessment — using the HSG256 methodology — works through five factors, then layers environmental and individual modifiers on top.
The HSG256 assessment sequence runs like this:
- Map the workload for each shift — physical, cognitive, safety-critical, monotonous — and score its fatigue-generating potential.
- Analyse the work activity — sedentary monitoring, heavy manual work, or safety-critical decision-making.
- Examine shift timing and duration — start times, length, frequency of night shifts, consecutive-shift patterns.
- Evaluate direction and speed of rotation — forward or backward, rapid, weekly, or slow.
- Check rest provision — breaks within shifts, hours between shifts, days off between blocks.
On top of those five, environmental modifiers matter: lighting, noise, temperature, lone working, and whether safety-critical tasks coincide with the 02:00–05:00 alertness trough. Individual modifiers include the vulnerability categories named above.
The assessment tool worth naming is the HSE Fatigue and Risk Index, a free spreadsheet-based calculator that takes a shift schedule and outputs quantitative fatigue scores. Alongside it, two validated sleepiness scales — the Karolinska Sleepiness Scale (KSS) and the Epworth Sleepiness Scale — and the Pittsburgh Sleep Quality Index give you survey instruments for worker self-report. The STOP-BANG questionnaire should be part of any health-surveillance screen, because undiagnosed obstructive sleep apnoea is the single most dangerous comorbidity in a shift-working population.
The data sources that matter most are usually already in the HSE system: incident timing analysis, overtime records, near-miss reports clustered in the 02:00–05:00 window, worker fatigue surveys, and turnover data. Map each identified risk to the hierarchy of controls and you have the starting point for an actual programme.
Engineering and Administrative Control Measures
Shift-work controls sit overwhelmingly in the administrative tier of the hierarchy, because elimination is rarely operationally feasible in 24/7 industries. What matters is that administrative controls here are evidence-based rather than customary.
Schedule architecture
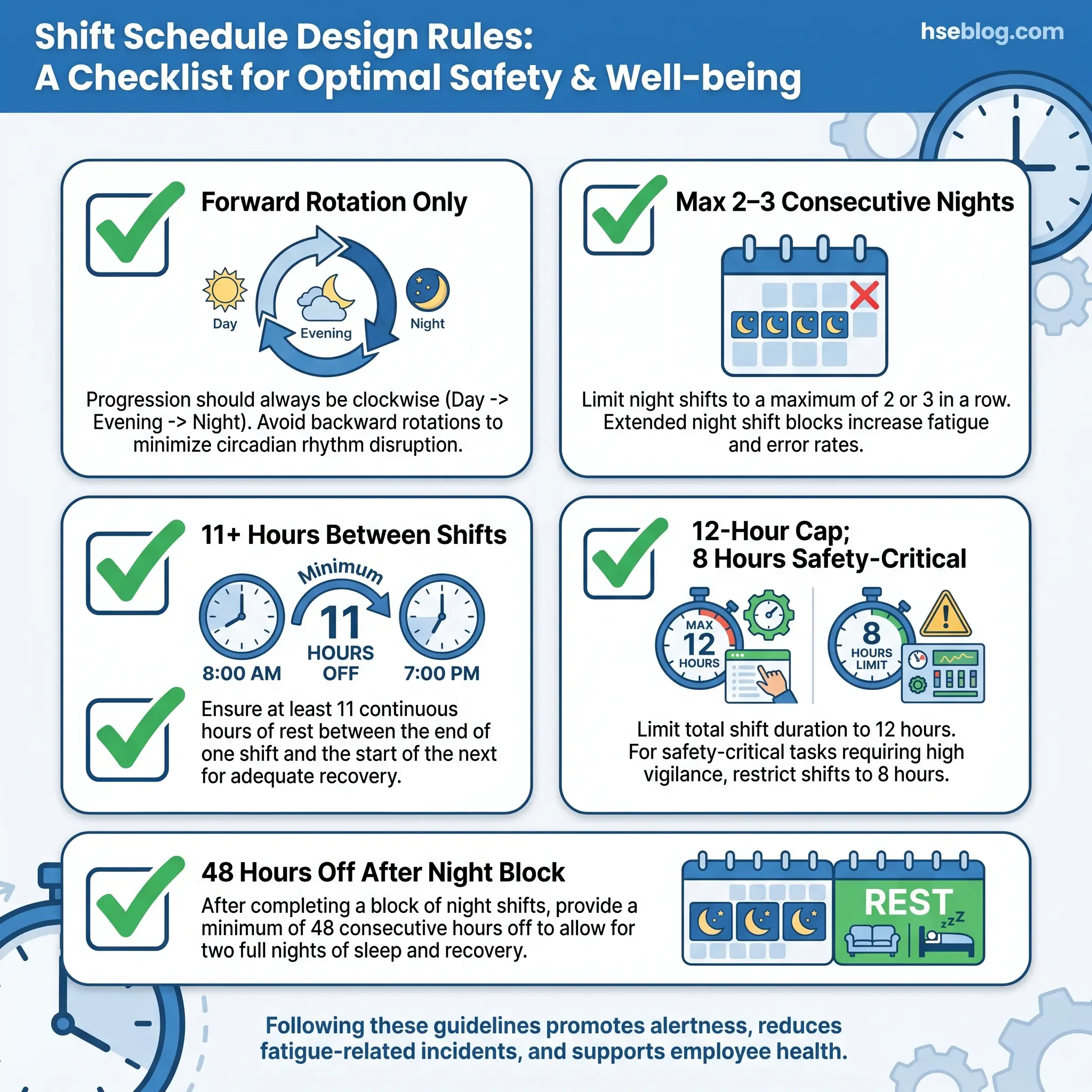
The headline schedule rules, drawn from HSG256 good practice and the NIOSH scheduling guidance at cdc.gov/niosh, are consistent across the evidence base:
- Forward rotation (day → evening → night) beats backward rotation. It works with the natural tendency of the human clock to drift later.
- Short rotations (2–3 days on each shift) or slow rotations (3–4 weeks) both outperform weekly rotations, which leave the worker chronically mis-synchronised.
- Limit consecutive night shifts to 2–3, with at least 48 hours off before the next work block.
- 11 or more hours between shifts, non-negotiable for safety-critical roles.
- Cap shift length at 12 hours including overtime, and at 8 hours for safety-critical or monotonous work — the EU Working Time Directive’s 8-hour night-work limit for hazardous work maps onto this.
- Avoid permanent night schedules where operationally possible; where they are unavoidable, structure health surveillance to match.
The operational argument that always comes up against these rules is that workers prefer 12-hour four-on-four-off patterns because of the block days off. That preference is real and should not be dismissed. But the trade-off needs to be named honestly: the accident curve above nine hours, and the commute risk after the last of four consecutive nights, are what the preference is being traded against.
Environmental and on-shift controls
Lighting is the single most underused environmental control in night operations. Bright, blue-enriched lighting during the first half of a night shift boosts alertness; warmer, lower-intensity lighting in the final hour eases the circadian wind-down and reduces post-shift driving risk. Noise management, thermal comfort, and reduced lone working during the alertness trough all contribute.
Napping policy is the most contested on-shift control, and the evidence is clear. A sanctioned 20-minute power nap boosts alertness without triggering sleep inertia, and a full 90-minute nap completes a sleep cycle and produces longer-lasting benefit. The 30-to-60-minute range is what to avoid — it drops workers into slow-wave sleep and leaves them disoriented on waking. Formalising napping is a cultural lift; pretending operators are not already micro-napping on the quiet end of the shift is a safety liability.
Audit Point: Most shift-swap registers are not reviewed against fatigue rules. Two swapped shifts can quietly turn a compliant roster into a 16-hour back-to-back. The audit question is not whether you have a swap policy — it is whether any single person has recalculated inter-shift rest after the last round of swaps.
Handover procedures deserve their own line. A structured, documented, redundant shift handover — ideally read-and-sign, face-to-face, at a fixed point in the control room — catches the communication errors that fatigue introduces. Commute controls (pool cars, taxi provision after extended or night shifts, on-site sleep rooms for workers whose drive is long) move commute-home fatality risk from outside the programme to inside it, where it belongs.
Fatigue Risk Management Systems
A Fatigue Risk Management System (FRMS) is the emerging best-practice response to the limits of prescriptive hours-of-service rules. It is a closed-loop system — identify, assess, control, verify — that treats fatigue as a continuous operational risk rather than a scheduling input. The American Academy of Sleep Medicine and Sleep Research Society’s 2021 guiding principles formalised the framework, and it is embedded in API RP 755 for refining and petrochemical operations.
An FRMS integrates the risk-assessment output, scheduling controls, a no-blame fatigue-reporting system, data from objective monitoring tools — wearables measuring sleep duration and heart-rate variability, PERCLOS eyelid-closure vision AI in cabs and control rooms, brief kiosk-based psychomotor vigilance tests at shift start — and ongoing management review. It also gives the programme the closed-loop structure ISO 45001 requires. The organisations now making the strongest progress are those treating FRMS as the backbone and scheduling controls as one input into it, rather than the other way round.
Individual and Health Surveillance Measures
A shift team at the mill once framed it during a training session in a way that stuck: “You can’t sleep-hygiene your way out of a bad roster.” That is the right framing for the individual tier of shift-work controls — real, necessary, but never a substitute for organisational scheduling.
On the employer side, the duties are:
- A free health assessment for night workers before assignment and at regular intervals, as required by the UK Working Time Regulations and the EU Working Time Directive.
- Periodic screening for cardiovascular risk, metabolic syndrome, mental health, and sleep disorders, including STOP-BANG for obstructive sleep apnoea.
- Referral pathways to occupational health for suspected Shift Work Sleep Disorder and related sleep pathologies.
- Breast cancer surveillance aligned with national screening programmes, with awareness that persistent night workers sit in a recognised elevated-risk category per IARC 2A.
- Training for workers, supervisors, and — a point often missed — families, who are the main social enablers of good daytime sleep.
On the supported-worker side, the practices with the best evidence are a fixed, blackout-quality anchor sleep window during daytime; strategic caffeine use (early in the shift, avoided in the final third); alcohol moderation, because it fragments sleep architecture even when it shortens sleep latency; light, easily digestible eating during the 02:00–05:00 window; regular physical activity at predictable times; and vitamin D supplementation where sun exposure is structurally reduced.
Chronotype-based self-rostering, where operationally feasible, allows morning and evening types to bid for compatible shifts. It is not always possible, but where it is, adherence and fatigue scores both improve meaningfully.
Monitoring, Review, and Continuous Improvement
The Check and Act steps of the ISO 45001 cycle are where most shift-work programmes go quiet. Leading indicators — the ones that tell you whether your controls are working before someone gets hurt — include hours worked against hours rostered, consecutive-night compliance, inter-shift rest compliance, fatigue-report submission rates, and the near-miss pattern by time of day. Lagging indicators — incident rates by shift, absenteeism, turnover, health-surveillance findings — tell you whether last year’s programme actually delivered.
A no-blame fatigue-reporting culture is the multiplier on every other control. If workers believe reporting fatigue will put them on a performance-management track, they stop reporting, and the leading-indicator data goes blind. The organisations with the best programmes treat fatigue reports the way they treat near-misses: neutrally, analytically, and with visible follow-through.
Annual schedule review against incident data, combined with genuine worker consultation — required under HSG256 and ISO 45001, and in practice the single highest-leverage input to schedule quality — closes the loop. The schedule you designed two years ago is almost certainly not the right one now.
Frequently Asked Questions
Conclusion
The direction shift work safety is heading in is away from prescriptive hours-of-service rules and toward integrated Fatigue Risk Management Systems that combine schedule design, objective monitoring, and a closed-loop management-system cycle. The American Academy of Sleep Medicine’s 2021 FRMS guiding principles, the continuing uptake of API RP 755 outside its original sector, and the growing deployment of wearables, PERCLOS vision AI, and psychomotor vigilance testing at shift start all point the same direction: fatigue is moving from a static scheduling assumption to a live operational signal.
What that means for a safety professional owning a shift-work programme is that the benchmark is rising. A defensible programme today needs a documented HSG256-style risk assessment, schedule controls that reflect the forward-rotation and consecutive-night evidence, sanctioned napping and environmental controls for the 02:00–05:00 window, a health-surveillance framework aligned with IARC 2A realities, a no-blame fatigue-reporting culture, and a monitoring loop that treats leading indicators as seriously as lagging ones. The programmes that are going to age well over the next five years are the ones that start integrating objective monitoring data into that loop now, rather than treating it as a future project.
The mill floor has not changed much in how it works a 24/7 roster. The science, the regulation, and the technology around how we protect the people working that roster have changed more in the last decade than in the previous three combined. Shift work safety is no longer a scheduling conversation — it is an occupational health discipline with its own evidence base, its own regulatory expectations, and its own management-system place.