

TL;DR
- Workplace wellbeing is more than a wellness program: It covers the physical, mental, social, and organizational conditions that affect how workers feel, function, and stay safe on the job — and it belongs squarely within HSE management.
- Psychosocial hazards are real hazards: Stress, fatigue, bullying, and poor work-life balance cause measurable harm — from increased incident rates to chronic disease — and regulators are starting to enforce controls.
- Wellbeing failures show up in your incident data: Fatigued workers make errors. Stressed supervisors skip checks. Disengaged crews ignore near-miss reporting. The connection between wellbeing and safety performance is direct and documented.
- ISO 45003 now provides a framework: The first global standard for managing psychosocial risk at work gives HSE professionals a structured, auditable approach to wellbeing — not just posters and fruit bowls.
- Implementation starts with honest assessment: Walk the site, talk to workers, review absence data, and treat wellbeing with the same rigor you apply to chemical exposure or fall protection.
I was conducting a behavioral safety observation on a gas compression station in the Gulf when I noticed a technician sitting alone behind a pipe rack during his shift. He wasn’t on break. He wasn’t injured. He was staring at nothing, hands on his knees, hard hat tilted back. When I approached him, he told me he hadn’t slept properly in three weeks, his rotation schedule had been extended twice, and he’d just learned his father was seriously ill back home — with no option to fly out. Fifteen minutes later, his supervisor radioed him to perform a live isolation on a high-pressure system. I stopped the job. That man was in no condition to make safety-critical decisions, and no permit-to-work system in the world would have caught what I saw in his eyes.
That moment crystallized something I’d been seeing across projects for years: we spend enormous resources controlling physical hazards — gas, gravity, electricity, pressure — but routinely ignore the human conditions that determine whether workers can actually respond to those hazards competently. Workplace wellbeing is not a corporate perk or an HR initiative. It is a core occupational health and safety issue that directly influences incident rates, decision-making quality, worker retention, and operational reliability. This article explains what workplace wellbeing actually means in an operational HSE context, why it matters far more than most organizations acknowledge, and how to approach it with the same rigor we apply to any other workplace hazard.
Defining Workplace Wellbeing in Operational HSE Terms
The phrase “workplace wellbeing” gets thrown around in corporate brochures and HR presentations until it loses all meaning. For HSE professionals, it needs a precise, operational definition — one that connects directly to hazard identification, risk assessment, and incident prevention.
Workplace wellbeing refers to the overall state of a worker’s physical, mental, and social health as influenced by working conditions, organizational culture, job demands, and the psychosocial environment. It is the degree to which work supports — rather than degrades — a person’s capacity to function safely, make sound decisions, and sustain health over a career. The World Health Organization defines it as a state where every individual realizes their own potential, can cope with the normal stresses of life, can work productively, and can contribute to their community.
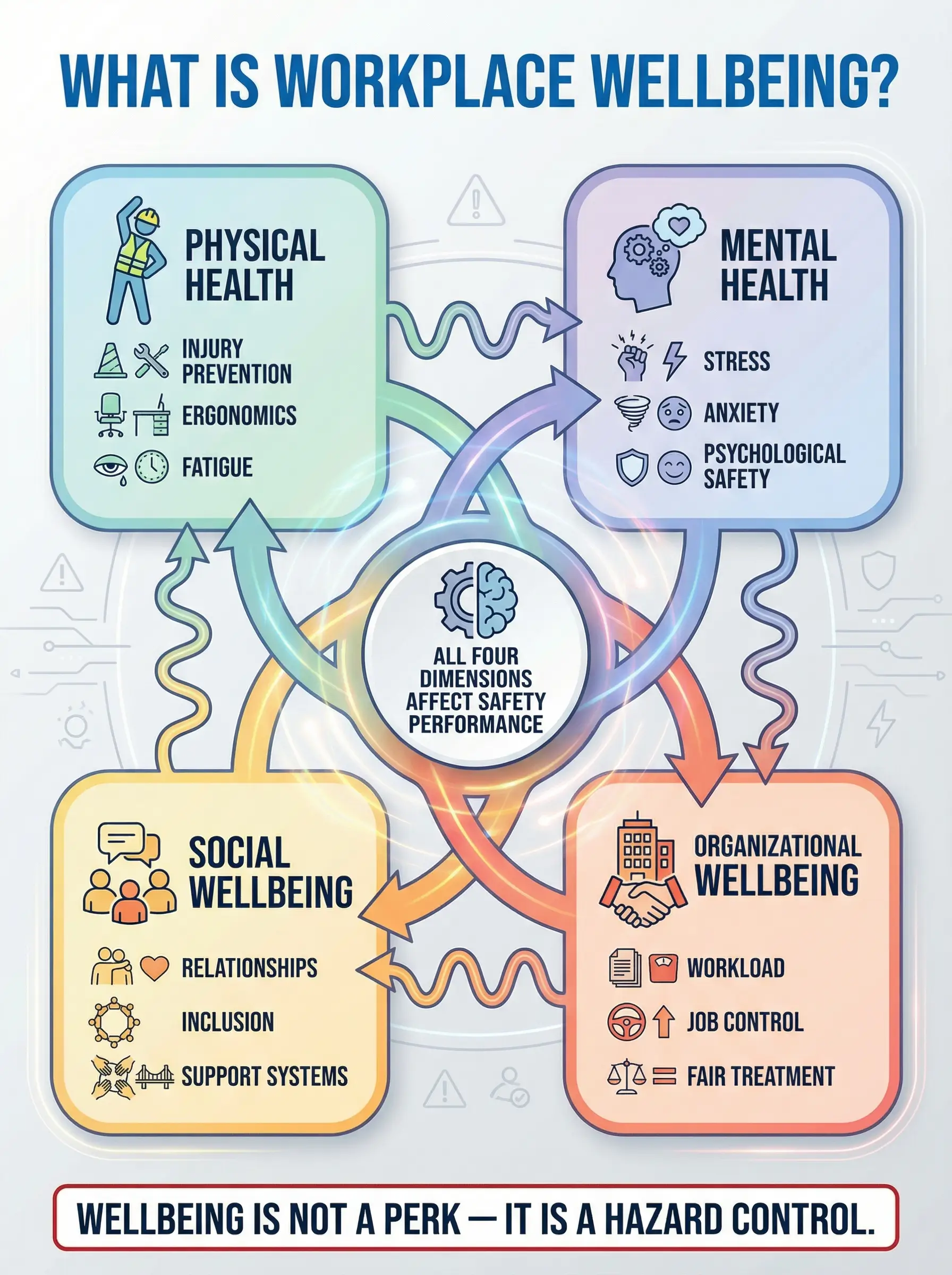
In practice, this means wellbeing is not one thing. It is a collection of interacting factors that HSE professionals already encounter daily — they just don’t always label them as “wellbeing.” The following dimensions make up the operational framework:
- Physical wellbeing: Absence of injury and occupational disease, adequate rest and recovery, ergonomic work design, access to clean water, nutrition, sanitation, and appropriate PPE. This is the dimension most HSE systems already address — but often incompletely, especially around fatigue and recovery time.
- Mental and psychological wellbeing: Freedom from chronic stress, anxiety, depression, burnout, and psychological harm caused by work. Includes cognitive capacity to perform safety-critical tasks, emotional regulation under pressure, and resilience to operational demands.
- Social wellbeing: Quality of workplace relationships, sense of belonging, freedom from bullying and harassment, access to peer support, and the ability to communicate openly — including raising safety concerns without fear of retaliation.
- Organizational wellbeing: Fairness of workload distribution, degree of job control and autonomy, clarity of roles, quality of leadership, work-life balance, and whether the organization’s systems and culture actively support or undermine the other three dimensions.
ISO 45003:2021 — Occupational health and safety management — Psychological health and safety at work provides the first international standard for managing psychosocial risk within an ISO 45001 framework. It explicitly requires organizations to identify psychosocial hazards, assess their risks, and implement controls — applying the same plan-do-check-act cycle used for physical hazards. [External Link: ISO 45003:2021 — https://www.iso.org/standard/64283.html]
Pro Tip: If your site’s hazard register includes noise, dust, and chemical exposure but has zero entries for fatigue, bullying, excessive workload, or shift-pattern risk — your HIRA is incomplete. Psychosocial hazards belong on the register alongside everything else.
Why Workplace Wellbeing Matters — The Evidence That Cannot Be Ignored
Many HSE professionals instinctively agree that wellbeing “matters,” but struggle to articulate exactly why — especially to operations managers who see it as soft, unmeasurable, or outside the safety function’s scope. The evidence base is now strong enough to end that debate. Wellbeing failures cause measurable, preventable harm across every metric that matters to an organization.
The Safety Performance Connection
The relationship between worker wellbeing and safety outcomes is not theoretical. It has been documented across industries and confirmed by both regulatory agencies and independent research. The following connections appear consistently in incident investigation data and epidemiological studies:
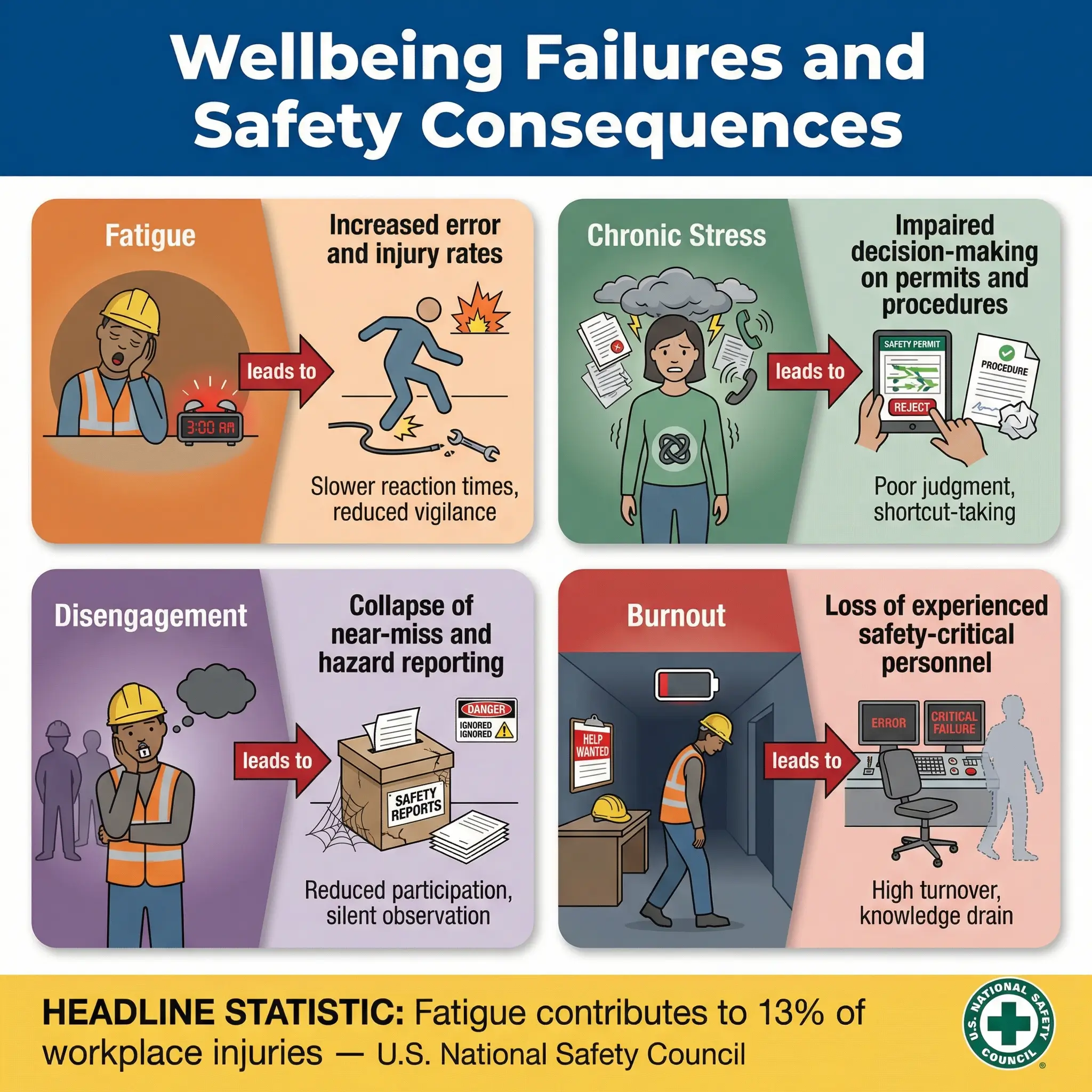
- Fatigue increases error rates dramatically. A worker operating on less than six hours of sleep performs cognitive tasks at a level comparable to a blood alcohol content of 0.05–0.08%. The U.S. National Safety Council estimates that fatigue contributes to 13% of workplace injuries. On safety-critical sites — where a single procedural error can trigger a major accident — this is an unacceptable risk multiplier.
- Stress degrades decision-making. Chronic workplace stress narrows attention, reduces situational awareness, and impairs risk perception. I have reviewed incident investigations where supervisors under extreme deadline pressure signed off on permits without verifying isolations — not because they were incompetent, but because their cognitive bandwidth was consumed by production demands.
- Disengagement kills reporting culture. Workers who feel unsupported, undervalued, or psychologically unsafe stop reporting near-misses, hazards, and unsafe conditions. Your leading indicators collapse — not because hazards disappear, but because the data pipeline dries up. By the time you notice, the lag indicators (injuries, incidents) are already climbing.
- Burnout drives experienced workers out. High-performing safety professionals and skilled tradespeople leave organizations — and sometimes the industry entirely — when wellbeing is chronically neglected. The institutional knowledge they take with them is irreplaceable and creates competency gaps that directly increase risk.
The Business and Legal Case
Beyond safety performance, workplace wellbeing carries significant financial, legal, and reputational weight. Organizations that dismiss it as a “nice to have” are increasingly exposed on multiple fronts:
- Absenteeism and presenteeism costs are enormous. The Health and Safety Executive (UK) reports that work-related stress, depression, and anxiety accounted for approximately 17.1 million working days lost in a single reporting year. Presenteeism — where workers attend but perform poorly due to ill health — costs even more but is rarely measured.
- Regulatory enforcement is tightening. Several jurisdictions now explicitly require psychosocial risk management. EU Directive 89/391/EEC requires employers to assess all risks to worker health and safety — including psychosocial risks. Australia’s model WHS regulations include specific psychosocial hazard provisions. The UK’s Management of Health and Safety at Work Regulations 1999 require risk assessment of all work-related health hazards, which courts have interpreted to include stress.
- Litigation and compensation claims are rising. Workers’ compensation claims for psychological injury, stress-related illness, and burnout are increasing across jurisdictions. Employers who cannot demonstrate proactive wellbeing management face both legal liability and reputational damage.
- Investor and client scrutiny is intensifying. ESG frameworks, IFC Performance Standards, and major EPC client pre-qualification questionnaires increasingly include worker wellbeing metrics. Organizations without credible wellbeing programs lose contracts.
The UK Health and Safety Executive states: “Employers have a legal duty to protect employees from stress at work by doing a risk assessment and acting on it.” [External Link: HSE UK — Work-related stress — https://www.hse.gov.uk/stress/]
| Wellbeing Failure | Safety Impact | Business Impact | Legal Exposure |
|---|---|---|---|
| Chronic fatigue | Increased incident rate, procedural errors | Productivity loss, overtime costs | Duty of care breach, negligence claims |
| Workplace bullying | Reporting culture collapse, crew conflicts | Turnover, recruitment costs | Harassment litigation, regulatory action |
| Excessive workload | Cognitive overload, shortcut-taking | Quality failures, rework | WHS prosecution for inadequate risk assessment |
| Poor work-life balance | Mental health deterioration, substance misuse | Absenteeism, presenteeism | Compensation claims, duty of care |
| Lack of psychological safety | Near-miss under-reporting, silence culture | Hidden risk accumulation | Failure to consult workers (legal requirement) |
Pro Tip: When presenting the business case for wellbeing to senior management, stop talking about “employee happiness” and start talking about incident causation, absence costs, competency retention, and legal liability. Speak their language.
Common Psychosocial Hazards — What to Look For on Site
Most HSE professionals can walk a site and spot a missing guardrail, an expired fire extinguisher, or an incorrect lifting technique within seconds. Psychosocial hazards are harder to see — but once you know what to look for, they become just as identifiable. The challenge is that they rarely present as a single, dramatic event. They accumulate quietly until they manifest as an incident, a medical case, or a resignation.
The following psychosocial hazards appear consistently across industries. Every one of them has appeared in incident root cause analyses I have been involved in:
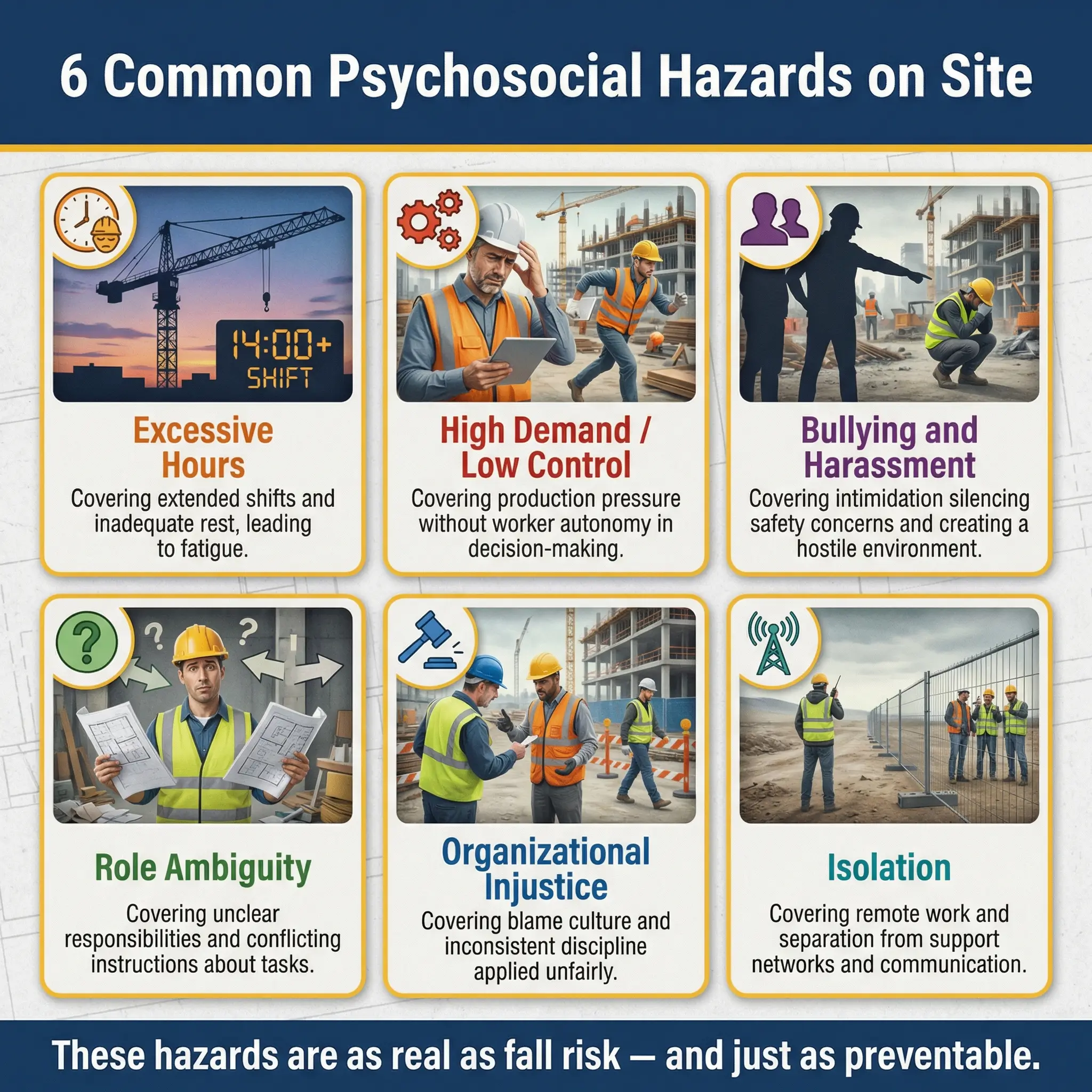
- Excessive working hours and inadequate rest: Rotation schedules that exceed recommended limits (typically 12 hours on, 12 off, with adequate days off per cycle). Extended rotations without proper breaks. Informal expectations to work through breaks or answer calls during rest periods.
- High job demands with low job control: Workers facing intense production pressure with no authority to pace their work, request resources, or flag concerns without repercussion. This combination — high demand, low control — is the strongest predictor of work-related stress in occupational health research (the Demand-Control Model, Karasek 1979).
- Bullying, harassment, and intimidation: Verbal abuse from supervisors, exclusion of individuals from safety briefings or team activities, public humiliation for mistakes, and systemic intimidation that silences safety concerns. On one construction megaproject in Southeast Asia, I traced a complete absence of near-miss reports from an entire work crew to a single foreman who punished anyone who submitted a hazard card.
- Role ambiguity and conflict: Workers unclear about their responsibilities, reporting lines, or authority — particularly around stop-work authority. Conflicting instructions from different supervisors. Being held accountable for outcomes without being given the resources or authority to influence them.
- Poor organizational justice: Inconsistent application of disciplinary procedures, visible favoritism, blame culture after incidents, and lack of recognition for safe performance. Workers who perceive the system as unfair disengage from it.
- Remote and isolated work conditions: FIFO (fly-in, fly-out) and offshore rotations that separate workers from family and social support networks for extended periods. Limited recreational facilities. Poor accommodation quality. Restricted communication access.
How to Assess Workplace Wellbeing — Practical Field Approaches
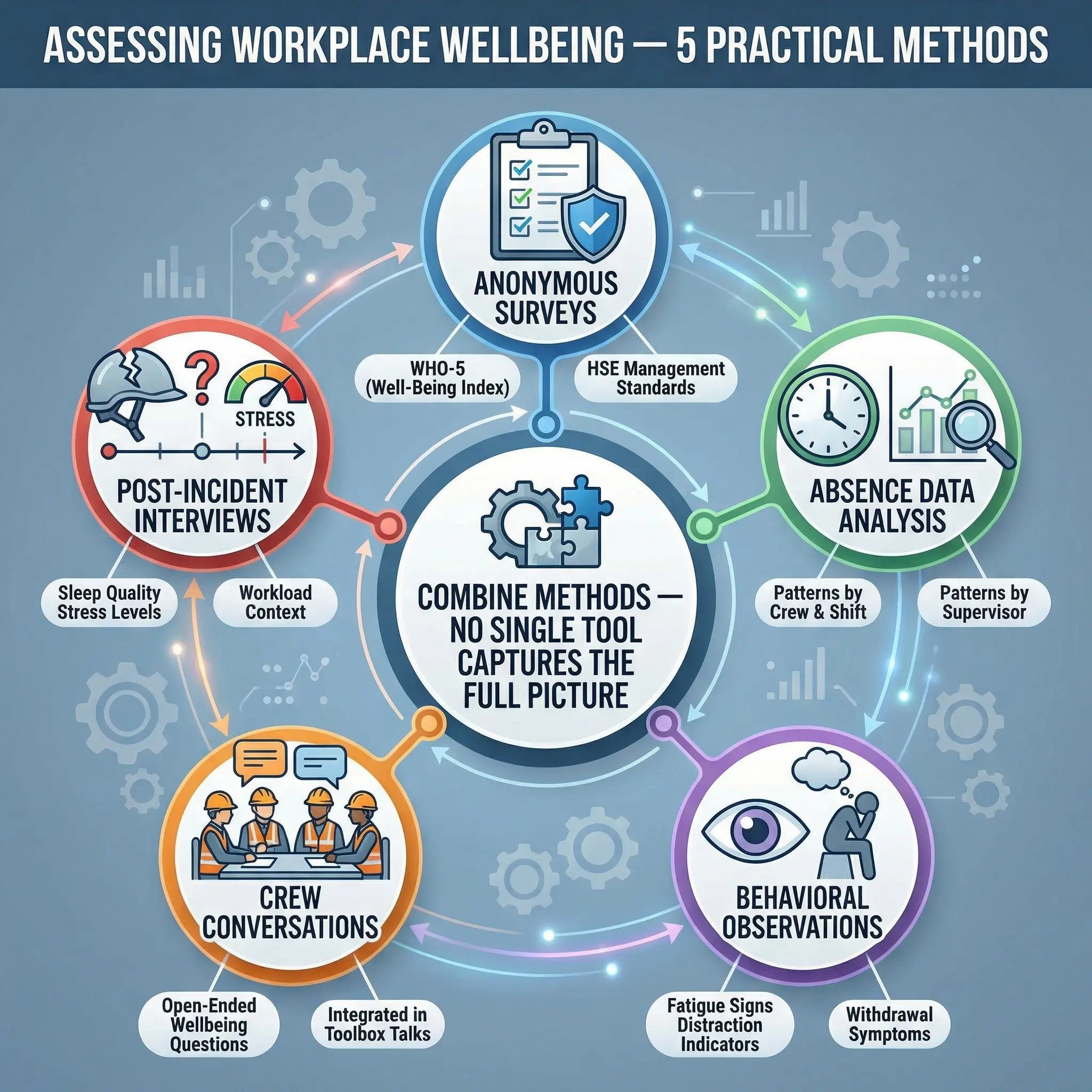
If you cannot measure it, you cannot manage it — and that principle applies to wellbeing just as much as it applies to atmospheric monitoring or noise dosimetry. The difference is that wellbeing assessment requires a mix of quantitative data and qualitative observation. No single tool captures the full picture. Effective assessment combines several methods, each revealing a different layer.
The following assessment approaches have proven effective across projects I have managed, from offshore platforms to urban construction sites:
- Worker wellbeing surveys (anonymous): Short, validated questionnaires administered quarterly. Use established tools such as the WHO-5 Wellbeing Index (five questions, takes two minutes) or the HSE UK Management Standards Indicator Tool. Anonymous submissions increase honesty. Track trends over time — absolute scores matter less than directional changes.
- Absence and turnover data analysis: Review sick leave patterns by department, crew, and shift pattern. Spikes in short-term absence often signal wellbeing issues before workers articulate them. High turnover in a specific crew or under a specific supervisor is a leading indicator.
- Behavioral safety observation integration: Add wellbeing indicators to your existing behavioral observation program. Train observers to note signs of fatigue (yawning, slow reaction, disorientation), distraction, withdrawal from team interaction, or visible emotional distress — alongside traditional unsafe act observations.
- Toolbox talks and crew conversations: Use structured but informal conversations during toolbox talks to ask open-ended wellbeing questions. “How’s the rotation treating you?” and “Is there anything outside the normal hazard list that’s making your job harder right now?” yield surprisingly honest responses when asked genuinely.
- Return-to-work and post-incident interviews: Integrate wellbeing questions into return-to-work assessments after absence and into all incident investigation protocols. Ask about sleep quality, stress levels, personal pressures, and workload in the period leading up to the event.
Pro Tip: Never launch a wellbeing survey without first committing to act on the results. Workers who share honest feedback and see nothing change become more disengaged than those who were never asked. If you are not prepared to respond, do not ask the question.
Leading vs. Lagging Wellbeing Indicators
Just as safety management distinguishes between leading and lagging indicators, wellbeing monitoring benefits from the same structure. Most organizations only track lagging indicators — by which point the damage is done.
| Indicator Type | Wellbeing Metric | What It Tells You |
|---|---|---|
| Leading | Wellbeing survey participation rate | Worker trust and engagement level |
| Leading | Toolbox talk wellbeing discussion frequency | Supervisor commitment to wellbeing |
| Leading | Voluntary near-miss reports per crew | Psychological safety of the team |
| Leading | Hours worked vs. scheduled (overtime tracking) | Fatigue exposure risk |
| Lagging | Stress-related sick leave days | Existing psychological harm |
| Lagging | Workers’ compensation claims (psychological) | System failure — harm already occurred |
| Lagging | Turnover rate in safety-critical roles | Loss of competency, burnout result |
| Lagging | Incident investigations citing fatigue/stress | Wellbeing as a contributing cause |
Building a Workplace Wellbeing Program That Actually Works
The gap between organizations that “have a wellbeing program” and organizations where workers actually feel well is enormous. I have audited sites where the wellbeing program consisted of a poster on the canteen wall, a mental health hotline number nobody had ever called, and a fruit basket in the site office on Fridays. Meanwhile, the crews were working 14-hour days, seven days a week, under a foreman who screamed at anyone who asked a question. That is not a wellbeing program. That is a liability.
Effective wellbeing programs share a set of characteristics that distinguish them from performative ones. The following elements form the foundation of every program I have seen produce genuine results:
- Leadership commitment that is visible and consistent: Senior management must actively participate — not just sign a policy. Site managers who attend wellbeing briefings, ask workers about fatigue during walk-arounds, and adjust schedules based on crew feedback send a signal that no poster can replicate.
- Integration into existing HSE systems: Wellbeing must be embedded in the hazard register, risk assessments, permit-to-work reviews, incident investigations, and management of change processes — not managed as a standalone HR initiative. If your OHSMS runs on ISO 45001, ISO 45003 provides a direct integration pathway for psychosocial risk.
- Supervisor training on psychosocial awareness: Frontline supervisors interact with workers more than anyone else. Training them to recognize fatigue signs, respond to distress disclosures, manage workload distribution fairly, and create psychologically safe team environments is the highest-leverage intervention available.
- Reasonable working hours and rotation design: Evidence-based shift patterns with adequate rest periods. Hard limits on overtime. Rotation schedules reviewed by occupational health professionals. On one LNG project, reducing the standard rotation from 28/28 days to 21/21 days reduced recordable incidents by 18% in the first six months — and the operations team initially resisted the change.
- Accessible and confidential support services: Employee assistance programs (EAPs) that workers actually know about, trust, and can access without stigma. Peer support programs where trained colleagues provide first-line support. On-site occupational health professionals who do more than pre-employment medicals.
- Reporting mechanisms without retaliation: Workers must be able to report psychosocial hazards — bullying, excessive hours, unfair treatment — through the same channels used for physical hazards, with the same protections. If your safety reporting system accepts hazard cards for “missing guardrail” but not for “supervisor bullying,” it is incomplete.
The Hierarchy of Controls Applied to Psychosocial Risk
HSE professionals already understand the hierarchy of controls for physical hazards. The same logic applies to psychosocial risk — and it is just as important to prioritize higher-order controls over individual-level interventions. Most organizations default to the bottom of the hierarchy (telling workers to be more “resilient”) while ignoring the organizational factors that cause the harm.
The following table applies the standard hierarchy to psychosocial hazards, showing what each level looks like in practice:
| Control Level | Physical Hazard Example | Psychosocial Hazard Equivalent |
|---|---|---|
| Elimination | Remove the hazard entirely | Eliminate unnecessary night shifts, remove bullying supervisors from leadership roles |
| Substitution | Replace with less hazardous alternative | Replace 14-hour shifts with 10-hour shifts, replace high-isolation roles with team-based work design |
| Engineering controls | Physically separate worker from hazard | Redesign job tasks to reduce monotony, implement automated fatigue monitoring on mobile equipment |
| Administrative controls | Procedures, training, signage | Wellbeing policies, supervisor training, rotation scheduling, EAP access, workload management protocols |
| PPE (Individual) | Personal protective equipment | Personal resilience training, mindfulness programs, stress management workshops |
Notice where most “wellbeing programs” operate: at the PPE level — asking individuals to cope better with harmful conditions rather than fixing the conditions. The hierarchy demands that we control the organizational hazard first, then support the individual. Not the reverse.
Common Mistakes Organizations Make With Wellbeing
Having audited wellbeing provisions across multiple industries and continents, I can confirm that the same mistakes repeat with remarkable consistency. These are not theoretical risks — they are patterns I have documented, raised in audit reports, and watched organizations either correct or ignore at their cost.
The following mistakes undermine wellbeing efforts more frequently than anything else:
- Treating wellbeing as an HR function, not an HSE function: When wellbeing sits entirely within HR, it gets disconnected from hazard identification, risk assessment, and incident investigation. Psychosocial hazards are occupational hazards. They belong in the safety management system.
- Launching programs without baseline assessment: Organizations implement wellbeing initiatives — yoga classes, mental health apps, wellness days — without first understanding what the actual problems are. A fruit basket does not fix a 70-hour work week. Assess first, then intervene based on evidence.
- Ignoring supervisor behavior as a root cause: The single most influential factor in a worker’s daily wellbeing is their immediate supervisor. Training workers in “resilience” while tolerating abusive, incompetent, or disengaged supervision is a systemic contradiction.
- Failing to act on survey results: Asking workers about their wellbeing and then doing nothing with the data is worse than never asking. It demonstrates that the organization is willing to perform the appearance of caring without committing to change.
- Confusing wellbeing with morale events: Barbecues, team outings, and recognition ceremonies are positive — but they are not wellbeing controls. They do not address the underlying conditions that cause harm. An organization can have excellent social events and terrible working conditions simultaneously.
- Measuring only lagging indicators: Tracking compensation claims and stress-related absence tells you what already went wrong. Without leading indicators — survey trends, overtime patterns, observation data — you cannot intervene before harm occurs.
The Role of the HSE Professional in Workplace Wellbeing
There is sometimes an identity question within the profession: “Is wellbeing really my job?” I have heard this from safety officers, safety managers, and even HSE directors. The answer is straightforward — yes. It has always been your job. The scope of occupational health and safety has always included the health of workers, and health is not limited to chemical exposure and hearing conservation.
What changes with an explicit wellbeing focus is not the scope of the role, but the tools and attention required. The following responsibilities sit squarely within the HSE professional’s domain:
- Include psychosocial hazards in risk assessments: Add fatigue, excessive hours, bullying, isolation, and role ambiguity to your site hazard register. Assess them with the same rigor as any physical hazard. If your risk matrix can score a “working at height” risk, it can score a “chronic excessive overtime” risk.
- Integrate wellbeing into incident investigations: When investigating any incident, ask about the human factors beyond immediate unsafe acts. Was the worker fatigued? Under personal stress? Working excessive hours? Pressured to skip steps? These are contributing causes, and they belong in the investigation report — not hidden behind “human error.”
- Challenge production decisions that harm workers: When schedules, manning levels, or rotation patterns create wellbeing risks, the HSE professional has a duty to escalate — just as they would escalate an inadequate scaffold or a missing gas detector. This requires professional courage, organizational support, and clear escalation pathways.
- Advocate for worker consultation on wellbeing: ISO 45001 Clause 5.4 and most national WHS legislation require worker consultation and participation. Extend this explicitly to wellbeing topics. Workers know what is harming them — the system must be designed to hear them.
- Monitor and report wellbeing metrics: Track leading and lagging wellbeing indicators alongside traditional safety KPIs. Present them in the same management review meetings. Normalize wellbeing data as operational safety data.
Conclusion
Workplace wellbeing is not a corporate luxury, a generational trend, or an HR initiative that safety professionals can politely ignore. It is a fundamental component of occupational health and safety — as real and as consequential as fall protection, atmospheric monitoring, or machine guarding. The evidence is unambiguous: workers who are fatigued, stressed, bullied, or burned out make more errors, report fewer hazards, and suffer more injuries. Ignoring wellbeing does not save money or maintain production — it transfers costs from the HR budget to the incident register, the compensation ledger, and the coroner’s report.
The tools to manage workplace wellbeing already exist within the frameworks HSE professionals use every day. ISO 45003 provides the standard. The hierarchy of controls provides the logic. Risk assessment provides the methodology. Incident investigation provides the feedback loop. What has been missing — and what must change — is the professional will to treat psychosocial hazards with the same seriousness we have always given to physical ones. A safety management system that monitors atmospheric oxygen to one decimal place but cannot tell you whether its workforce is sleeping, coping, or breaking is a system with a blind spot large enough to kill.
Every worker who walks onto your site carries more than their PPE and their training. They carry their fatigue, their stress, their family pressures, their dignity, and their trust that you — their HSE professional — will protect not just their body, but the conditions that allow them to stay whole. That trust is the most important permit-to-work you will ever hold. Do not let it expire.