

TL;DR
- If your air monitoring shows compliance with the OEL for a sensitiser, that does not mean sensitisation risk is controlled — conventional occupational exposure limits are not designed to prevent immunological sensitisation, and sensitised workers can react at concentrations far below the limit.
- If a worker’s asthma symptoms improve on weekends and holidays, do not treat this as confirmation of occupational asthma — work-exacerbated asthma produces the same temporal pattern, and the distinction requires objective diagnostic testing, not history alone.
- If your organisation uses products containing ≥0.1% diisocyanates anywhere in the EU, every industrial and professional user must have completed mandatory REACH training since August 2023, with certification valid for five years (EU Commission Regulation 2020/1149).
- If you are designing a health surveillance programme for workers exposed to respiratory sensitisers in the UK, COSHH Regulation 11 requires surveillance — and HSE guidance G402 recommends questionnaire plus spirometry at baseline, six-weekly for the first year, then annually.
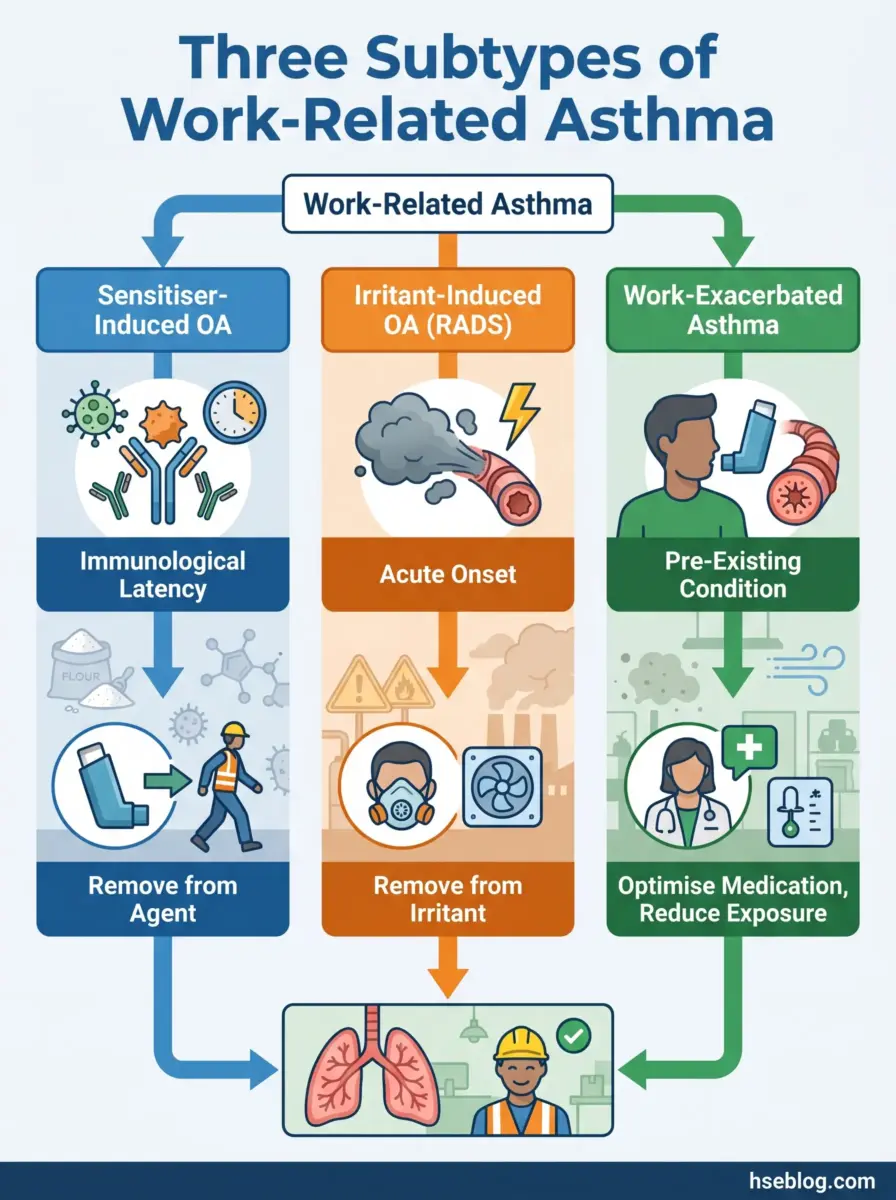
Occupational asthma is new-onset asthma caused by inhaling a sensitising or irritant substance at work, while work-exacerbated asthma is pre-existing asthma worsened by workplace exposures. The distinction determines whether the worker requires complete removal from the causative agent, qualifies for workers’ compensation, and whether co-workers face ongoing exposure risk — making accurate classification both a legal and clinical necessity.
Approximately 15% of adult-onset asthma cases are attributable to occupational exposures (European Respiratory Society, consensus estimate cited in 2024 reviews). That figure is not a rounding error. It represents hundreds of thousands of workers globally developing a chronic, often irreversible respiratory disease because of what they breathe at work — and in many cases, because the systems meant to protect them failed at the point of early detection or exposure control. Asthma affected an estimated 363 million people worldwide in 2023 and caused 442,000 deaths (WHO, 2024, citing Global Burden of Disease Study 2023 data). The occupational fraction of that burden is preventable.
Most available guidance on occupational asthma covers what it is. This article addresses what practitioners actually need to do about it — from the diagnostic algorithm that separates genuine occupational asthma from work-exacerbated asthma, through the uncomfortable reality that occupational exposure limits offer incomplete protection against sensitisers, to the design of surveillance programmes that detect disease early enough to matter. Where regulatory frameworks conflict across jurisdictions, those conflicts are presented side-by-side. Where emerging science is changing the field, the implications for current practice are interpreted rather than left in academic isolation.
What Distinguishes Occupational Asthma from Work-Exacerbated Asthma — and Why the Distinction Matters
The classification of work-related respiratory disease into its correct subtype is not an academic exercise. It drives every downstream decision: diagnostic pathway, management strategy, whether the worker can remain in the role, and whether they qualify for compensation. Getting it wrong — in either direction — has consequences that compound over years.
Sensitiser-induced occupational asthma involves an immunological mechanism with a latency period that can range from weeks to over thirty years after first exposure. The worker develops specific sensitisation to an agent, after which even very low concentrations can trigger bronchoconstriction. Irritant-induced occupational asthma, including reactive airways dysfunction syndrome (RADS), follows a fundamentally different pathway: acute high-concentration exposure causes airway injury without immunological latency, sometimes within hours. Work-exacerbated asthma (WEA) is different again — the worker already has asthma, and non-specific workplace triggers (dust, cold air, fumes, exercise) worsen it.
A consistent failure mode in practice is treating the temporal symptom pattern — improvement on weekends and holidays, worsening during work periods — as definitive evidence of occupational asthma. This pattern does appear in sensitiser-induced OA, but it also appears in WEA and even in non-occupational asthma where weekday triggers happen to overlap with work schedules. Relying on history alone, without objective testing, leads to misclassification in both directions: workers with WEA labelled as having OA (triggering unnecessary removal from work) and workers with genuine OA labelled as having WEA (leaving them in continued exposure while their airways remodel irreversibly). The distinction requires objective diagnostic evidence, which the next section addresses.
| Feature | Sensitiser-Induced OA | Irritant-Induced OA (RADS) | Work-Exacerbated Asthma |
|---|---|---|---|
| Mechanism | Immunological sensitisation (IgE or non-IgE) | Acute airway injury from high-concentration irritant | Pre-existing asthma worsened by non-specific triggers |
| Latency | Weeks to >30 years | None — onset within 24 hours of single exposure | Not applicable (pre-existing) |
| Prognosis after removal | ~30% full remission; many have persistent symptoms | Variable; some recover, some develop chronic airway hyperresponsiveness | Can often be managed without job change |
| Compensation eligibility | Yes, in most jurisdictions (with objective evidence) | Yes, typically classified under OA | Varies — often excluded or requires stronger evidence |
| Management | Complete removal from causative agent | Remove from further irritant exposure; pharmacotherapy | Medication optimisation + exposure reduction; may continue in role |
High-Molecular-Weight vs. Low-Molecular-Weight Asthmagens
The molecular weight classification of a sensitising agent is not just a toxicological detail — it determines the diagnostic pathway available and shapes the exposure monitoring strategy.
High-molecular-weight (HMW) agents — flour dust, laboratory animal allergens, natural rubber latex proteins, enzymes used in detergent manufacturing — typically produce IgE-mediated immune responses. This makes them detectable through skin prick testing and specific serum IgE assays, giving the diagnosing physician a relatively clear immunological marker to work with. Flour dust and laboratory animal allergens remain among the most commonly reported HMW causes of OA globally.
Low-molecular-weight (LMW) agents present a harder problem. Isocyanates, acid anhydrides, reactive dyes, platinum salts, and certain wood dusts often sensitise through non-IgE mechanisms that are poorly understood and difficult to detect with standard immunological tests. Diisocyanates — particularly toluene diisocyanate (TDI) and methylene diphenyl diisocyanate (MDI) — are the leading cause of occupational asthma in the EU, with more than 5,000 new cases estimated annually across member states (ECHA Annex XV Restriction Report, published in Annals of Work Exposures and Health, 2021). When IgE-based testing is unreliable, diagnosis for LMW sensitisers often depends on serial peak expiratory flow monitoring or specific inhalation challenge — both of which demand time, patient compliance, and specialist facilities.
Advanced Diagnostic Pathways: Moving Beyond Clinical History
Clinical history has high sensitivity for occupational asthma — if a worker reports new-onset wheeze, chest tightness, and dyspnoea that improve away from work, the diagnosis should be suspected. The problem is specificity. Multiple conditions produce the same symptom pattern, and medicolegal decisions about compensation, job removal, and workplace investigation cannot rest on suspicion alone.
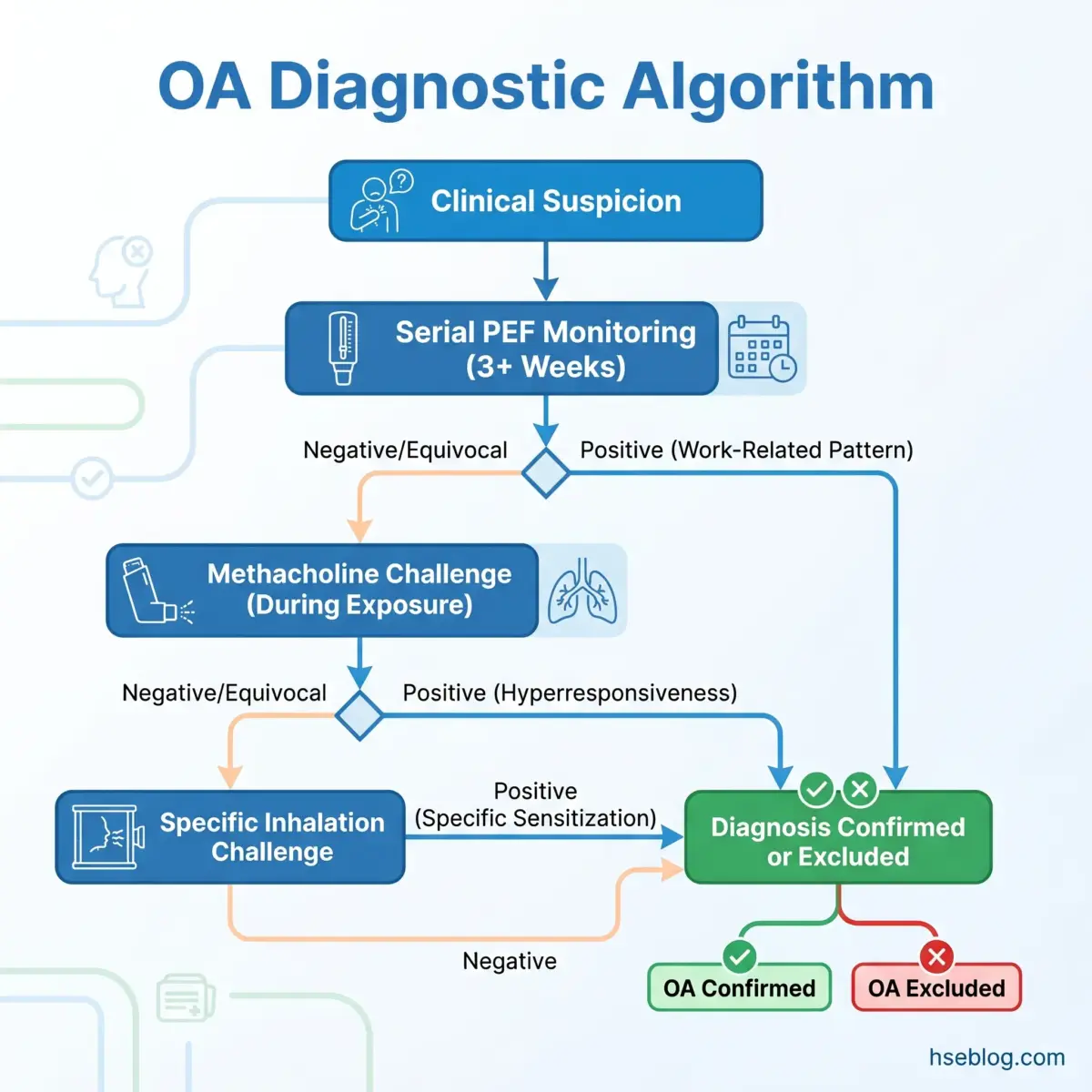
The diagnostic algorithm for suspected OA proceeds through several levels of objective testing, each adding specificity:
- Serial peak expiratory flow (PEF) monitoring — The worker records at least four PEF measurements daily over a minimum of three weeks, including both work and away-from-work periods. Software analysis (such as the Oasys programme) compares work-day versus rest-day patterns. This is the most accessible objective test, but it depends on patient compliance and honesty — and it can miss cases where the worker has already been removed from exposure before testing begins.
- Non-specific bronchial hyperresponsiveness testing — Methacholine or histamine challenge measured during exposure periods and repeated during time away from work. A significant decline in PC20 (the concentration provoking a 20% FEV₁ fall) during work periods suggests occupational causation. A critical practitioner interpretation: a negative methacholine challenge performed after several weeks away from exposure does not rule out OA. Bronchial hyperresponsiveness can normalise within weeks of exposure cessation. Timing of testing relative to last exposure is decisive.
- Specific inhalation challenge (SIC) — The closest approximation to a diagnostic gold standard. The worker is exposed to the suspected agent under controlled laboratory conditions while lung function is monitored. SIC provides the most direct evidence of causation, but availability is limited to specialised centres, the procedure is resource-intensive, and standardisation varies between facilities.
- Biomarkers — Sputum eosinophil counts and fractional exhaled nitric oxide (FeNO) provide supporting evidence for airway inflammation and can help phenotype the asthma, but neither is diagnostic for occupational causation on its own.
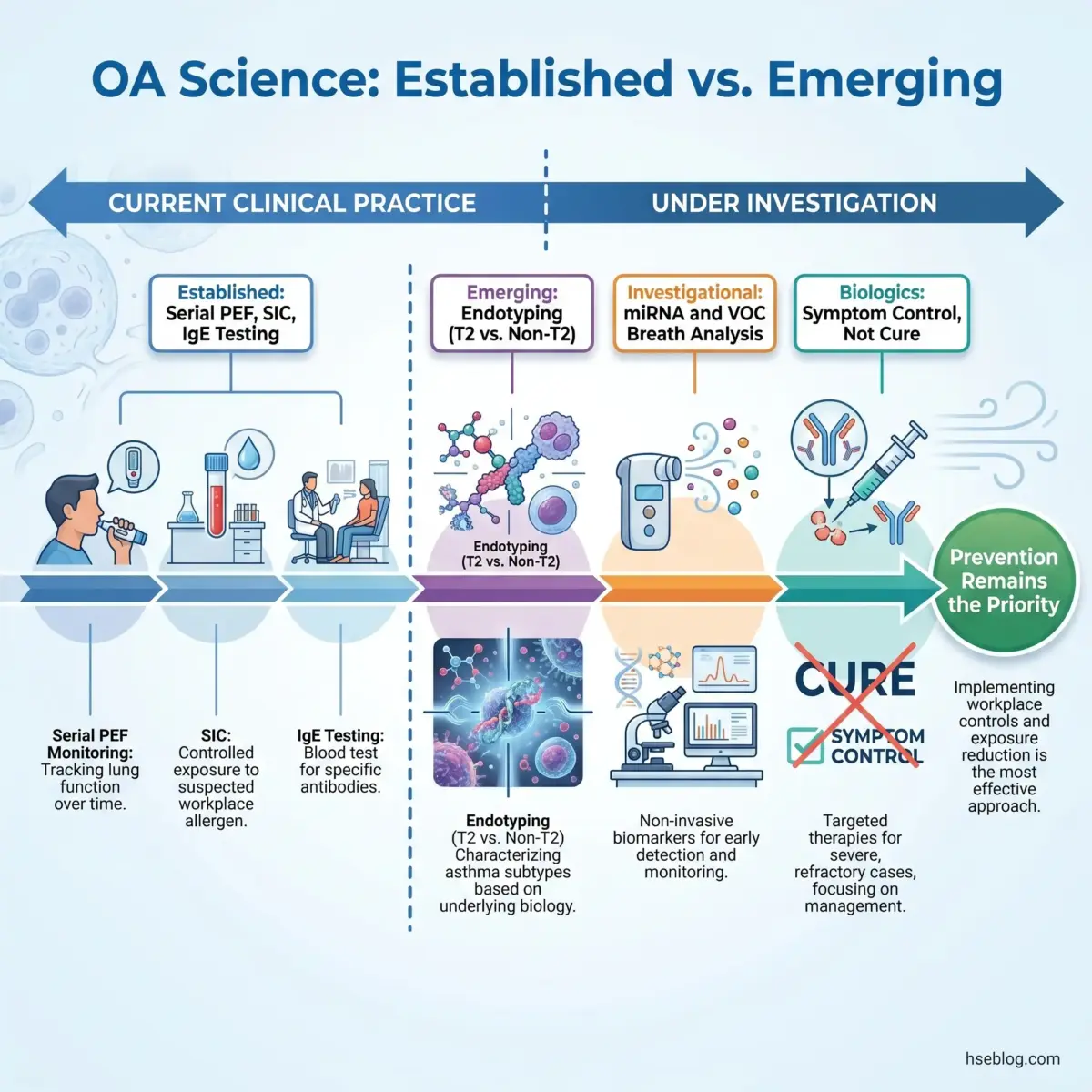
- Investigational approaches — MicroRNA (miRNA) profiling and volatile organic compound (VOC) breath analysis are under active clinical investigation as potential biomarkers for distinguishing OA from non-occupational asthma. Neither is validated for clinical use at the time of writing.
Watch For: A negative methacholine challenge during time away from work is not a negative diagnosis. If testing is conducted after several weeks of exposure cessation, bronchial hyperresponsiveness may have resolved — a false reassurance that has led to missed OA diagnoses and continued exposure.
| Diagnostic Test | Sensitivity | Specificity | Availability | Key Limitation |
|---|---|---|---|---|
| Serial PEF monitoring | Moderate-high | Moderate | High (primary care) | Requires patient compliance; 3+ weeks |
| Methacholine challenge | High (during exposure) | Moderate | Moderate | Timing-dependent; normalises away from exposure |
| Specific inhalation challenge | High | High | Low (specialist centres) | Resource-intensive; not fully standardised |
| Specific IgE / skin prick test | Variable (good for HMW) | Variable | High | Unreliable for many LMW sensitisers |
| FeNO / sputum eosinophils | Moderate | Low for OA specifically | Moderate | Supporting evidence only; not diagnostic |
When Specific Inhalation Challenge Is — and Isn’t — Necessary
The judgment call on whether SIC is warranted turns on the clinical and medicolegal context. SIC is most valuable when serial PEF records are equivocal, the causative sensitiser is uncertain, the worker cannot return to the workplace for a supervised exposure period, or a compensation dispute requires the highest level of diagnostic certainty. In Quebec, SIC is virtually mandatory for workers’ compensation purposes — a jurisdictional requirement that does not apply in most other regions.
SIC is unnecessary when serial PEF monitoring clearly demonstrates work-relatedness, when specific IgE testing confirms sensitisation to a known HMW agent already present in the workplace, or when the clinical picture and exposure history are unambiguous. Subjecting a worker to SIC when simpler, validated tests have already established the diagnosis adds cost, delay, and discomfort without changing management.
Occupational Exposure Limits for Asthmagens: Why the Numbers Don’t Tell the Whole Story
Compliance with an occupational exposure limit is the benchmark most organisations use to determine whether airborne chemical risk is controlled. For conventional toxic effects — irritation, organ damage, narcosis — this approach is defensible. For respiratory sensitisers, it creates a dangerous false assurance.
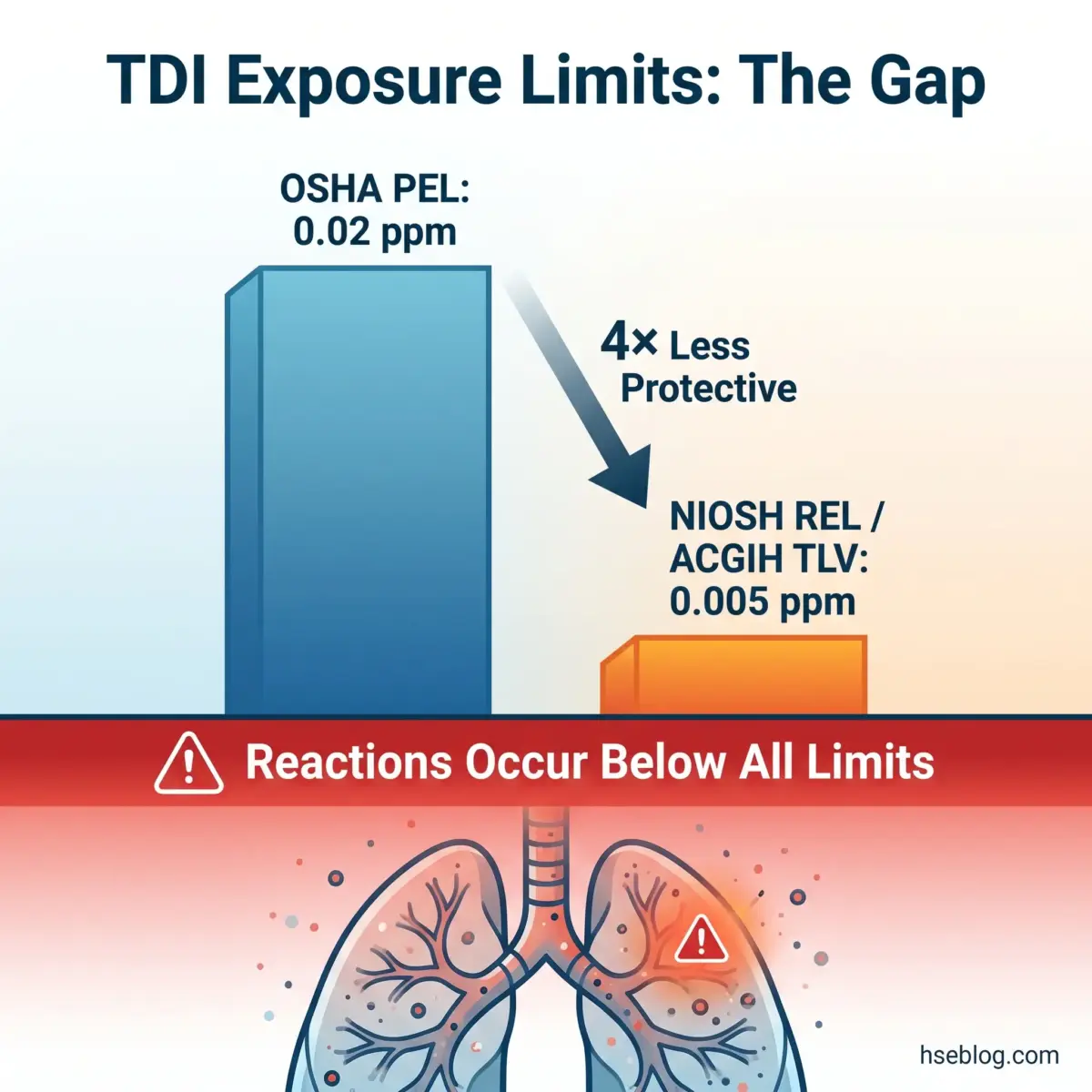
The fundamental limitation is this: traditional OELs are designed to prevent toxic effects from repeated exposure using a dose-response model. Immunological sensitisation does not reliably follow that model. No safe threshold for sensitisation has been established for most respiratory sensitisers. Once a worker is sensitised, asthmatic responses can be triggered at concentrations far below the OEL — sometimes at levels undetectable by standard air monitoring.
The regulatory landscape reflects this uncertainty in contradictory ways. OSHA PELs for key asthmagens remain legally enforceable in the US, but most were adopted in 1971 from 1968 ACGIH TLVs and have not been updated since (OSHA, 29 CFR 1910.1000). OSHA itself has acknowledged these limits are outdated. For toluene diisocyanate (TDI), the OSHA PEL sits at 0.02 ppm TWA — four times less protective than the NIOSH REL and ACGIH TLV, both at 0.005 ppm TWA. Research has documented asthmatic responses in sensitised workers at concentrations at or below the ACGIH TLV. The practical implication: the stricter value should govern workplace controls, regardless of which limit carries legal force. OSHA’s annotated PELs present these discrepancies side-by-side for practitioners to evaluate.
In the UK, workplace exposure limits (WELs) are published in EH40 under the COSHH Regulations 2002. For substances recognised as respiratory sensitisers where no safe threshold can be identified, the regulatory expectation is exposure reduction to as low as reasonably practicable — not mere compliance with a numerical limit.
The EU is taking the most aggressive regulatory step in this space. The European Parliament approved the first binding occupational exposure limits for diisocyanates in late 2024 — 6 µg NCO/m³ as an 8-hour TWA and 12 µg NCO/m³ as a short-term exposure limit — pending Council adoption. This represents a significant tightening of enforceable limits across all member states.
| Asthmagen | OSHA PEL (US) | NIOSH REL (US) | ACGIH TLV | UK WEL | Proposed EU OEL |
|---|---|---|---|---|---|
| TDI | 0.02 ppm TWA | 0.005 ppm TWA (10-hr) | 0.005 ppm TWA | 0.02 mg/m³ TWA | 6 µg NCO/m³ TWA |
| MDI | 0.02 ppm ceiling | 0.005 ppm TWA (10-hr) | 0.005 ppm TWA | 0.02 mg/m³ TWA | 6 µg NCO/m³ TWA |
| Flour dust | 15 mg/m³ total / 5 mg/m³ resp. | 0.5 mg/m³ TWA | 0.5 mg/m³ inhalable | 10 mg/m³ inhalable / 4 mg/m³ resp. | — |
Audit Point: Biological monitoring (e.g., urinary isocyanate metabolites) frequently detects worker exposure even when air monitoring shows levels below detection limits. This indicates dermal absorption or peak-exposure underestimation by time-weighted air sampling. Air monitoring compliance alone is an insufficient basis for declaring sensitiser exposure controlled.
Hierarchy of Controls Applied to Asthmagen Exposure
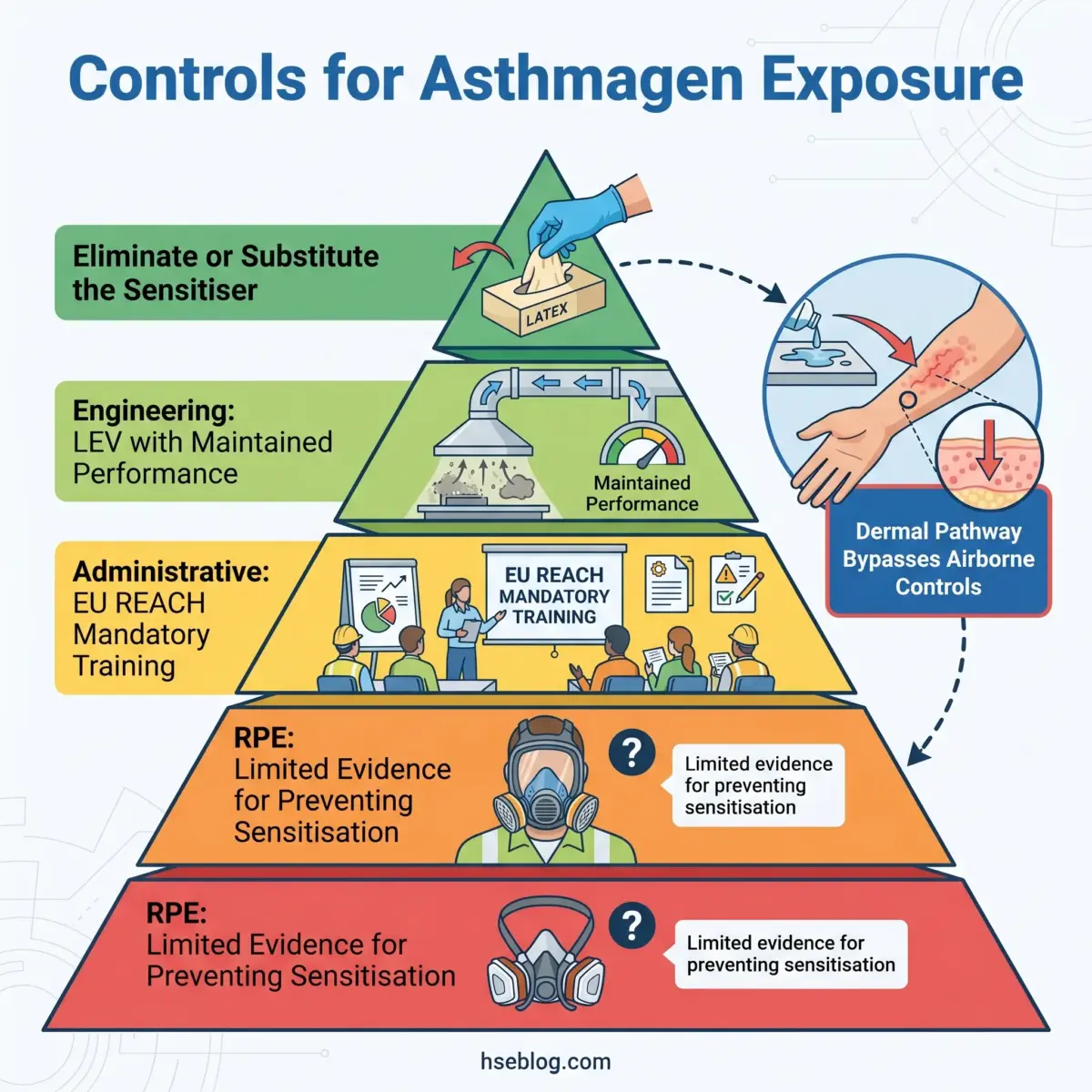
The hierarchy of controls is a familiar framework, but its application to respiratory sensitisers involves specific challenges that standard chemical-hazard implementations do not address. The most significant: unlike most toxic substances, sensitisers cause harm through an immunological mechanism that does not reliably respond to dose reduction below a threshold. This changes the calculus at every tier of the hierarchy.
Elimination and substitution have delivered the most dramatic results where they have been achievable. The healthcare sector’s transition from powdered natural rubber latex gloves to powder-free or nitrile alternatives substantially reduced latex sensitisation rates among healthcare workers — a genuine elimination success story. In industries dependent on isocyanates — polyurethane foam manufacturing, automotive painting, adhesive formulation — substitution remains difficult because isocyanate chemistry is often integral to the product performance. Where elimination is not feasible, the pressure on lower-tier controls intensifies.
Engineering controls — primarily local exhaust ventilation (LEV) — are the next line of defence. LEV effectiveness depends entirely on design, installation, and ongoing maintenance. COSHH requires LEV systems to undergo thorough examination and testing at least every 14 months, with records maintained. A common enforcement finding in HSE UK inspections of bakeries, woodworking shops, and spray-paint facilities is LEV that exists on paper but has degraded in practice — blocked ductwork, worn fan belts, inadequate capture velocity at the emission point. Equipment that is installed but not maintained provides a documentation trail without providing protection.
The dermal exposure pathway adds a complication that the standard hierarchy of controls often underestimates. Emerging evidence indicates that skin absorption of LMW sensitisers — particularly isocyanates — contributes to respiratory sensitisation even when air monitoring shows compliance with exposure limits. Workers handling uncured polyurethane products, adhesives, or coatings without adequate skin protection may develop respiratory sensitisation through dermal uptake, bypassing the airborne-exposure controls entirely. This finding has significant implications: respiratory protection and LEV alone may be insufficient if dermal contact is not also controlled.
Respiratory protective equipment (RPE) sits at the bottom of the hierarchy for good reason. Evidence for RPE effectiveness in preventing initial sensitisation (as opposed to managing exposure in already-sensitised workers) is limited. RPE reduces inhaled dose, but given the absence of a reliable no-effect threshold for sensitisers, dose reduction without elimination does not guarantee prevention. Under OSHA 29 CFR 1910.134, RPE use requires medical evaluation, fit testing, and training — requirements that are frequently underimplemented.
The EU REACH diisocyanate restriction (Regulation 2020/1149) introduced a control measure at the administrative-training tier that is without precedent for a specific chemical group. Since August 2023, all industrial and professional users of products containing ≥0.1% diisocyanates by weight must complete mandatory training across three tiers — general, intermediate, and advanced — with certification valid for five years. This applies across all EU member states and affects spray painters, foam manufacturers, adhesive users, automotive repair workers, and many other sectors. The restriction explicitly aims to reduce the estimated 5,000+ annual new OA cases from diisocyanates in the EU.
Designing an Effective Health Surveillance Programme
A health surveillance programme for occupational asthma has one purpose: detect sensitisation or early airway changes before irreversible disease is established. If the programme only documents confirmed cases after symptoms are entrenched and airway remodelling has occurred, it is performing an administrative function, not a preventive one.
The regulatory mandate differs sharply across jurisdictions. Under COSHH Regulation 11 (UK), employers must provide health surveillance for all employees exposed to substances listed in Schedule 6, which includes respiratory sensitisers. HSE guidance G402 provides the practical framework: respiratory symptom questionnaire plus spirometry at pre-placement, six-weekly intervals for the first year of exposure (when sensitisation risk is highest), and annually thereafter. The first-year frequency reflects the evidence that most sensitisation occurs within the initial months of exposure.
OSHA (US) has no equivalent universal surveillance mandate for respiratory sensitiser exposure. Requirements are scattered across substance-specific standards and general recordkeeping obligations under 29 CFR 1904. An employer may be legally compliant without any health surveillance programme, even where workers are exposed to known sensitisers daily. This jurisdictional gap is a direct risk factor for multinational companies applying their US-based compliance frameworks globally — a programme that satisfies OSHA may violate COSHH.
The NIOSH work-related asthma reporting guidelines, updated in February 2025, provide surveillance case definitions that classify work-related asthma into OA and WEA subtypes — a framework that supports state-level reporting through the SENSOR programme but does not create an employer surveillance mandate.
Effective programme design includes several components whose absence undermines the entire effort:
- Pre-placement assessment — Baseline respiratory questionnaire, spirometry meeting quality standards, and where feasible, immunological testing (specific IgE or skin prick test) for the relevant sensitiser before first exposure. This establishes the worker’s pre-exposure respiratory function as a comparator.
- Periodic surveillance — Questionnaire and spirometry at the intervals specified by the applicable jurisdiction. Frequency matters: annual-only surveillance in the first year of exposure misses the window where most sensitisation occurs.
- Action triggers — Defined criteria for what findings prompt referral to an occupational physician, immediate removal from exposure, or enhanced monitoring. Without pre-determined triggers, abnormal results are noted but not acted upon — a pattern that appears repeatedly in HSE UK enforcement notices.
- Spirometry quality — Spirometry is only useful if performed to recognised quality standards (ATS/ERS criteria). Poorly performed spirometry generates noise, not data.
- Reporting — UK employers must report confirmed OA cases under RIDDOR 2013, Schedule 1. US employers must record work-related respiratory conditions under OSHA 29 CFR 1904.
Field Test: Review your surveillance programme’s referral-trigger criteria. If the criteria are vague (“abnormal findings should be reviewed”) rather than specific (“a decline of >15% in FEV₁ from baseline, or new positive responses on the respiratory questionnaire, triggers referral within two weeks”), the programme is unlikely to catch early-stage sensitisation before symptoms become established.
Prognosis, Return to Work, and the Long-Term Outlook
The question that matters most to the diagnosed worker — “will I recover?” — does not have a reassuring answer for sensitiser-induced occupational asthma. Only approximately 30% of patients with sensitiser-induced OA achieve full remission after complete cessation of exposure (multiple peer-reviewed studies, cited in University Hospital Strasbourg clinical trial protocol, 2024/2025). The remaining majority experience persistent bronchial hyperresponsiveness, ongoing symptoms requiring pharmacotherapy, or both. Prognosis correlates with two factors more strongly than any others: how early the diagnosis is made and how quickly exposure is eliminated after diagnosis. This is the single strongest argument for investing in robust surveillance.
Irritant-induced OA and work-exacerbated asthma follow a fundamentally different management trajectory. Workers with WEA may be able to remain in the same role with medication optimisation and targeted reduction of non-specific triggers — a pathway that preserves employment without ongoing sensitiser exposure. RADS prognosis is variable: some workers recover airway function over months, while others develop chronic hyperresponsiveness.
The tension between the medical recommendation — complete removal from all exposure to the causative agent — and the socioeconomic reality that many workers cannot afford to change industries is real and unresolved. Effective occupational health practice navigates this tension. Return-to-work planning should explore modified duties, workplace modifications that eliminate the specific agent from the worker’s environment, and interim respiratory protective equipment while permanent controls are implemented. Workers’ compensation systems vary dramatically by jurisdiction — province-level in Canada, state-level in the US, national in the UK — and eligibility typically requires the objective diagnostic evidence discussed earlier, not clinical history alone.
Every confirmed OA diagnosis is a sentinel event. It signals that at least one worker has been exposed sufficiently to develop sensitisation, meaning other workers in the same environment are at risk. Diagnosis should trigger workplace investigation and co-worker protection — not just individual case management.
Emerging Science: Endotyping, Biomarkers, and Biologics in Occupational Asthma
The science underlying occupational asthma classification is shifting in ways that will eventually change both diagnosis and management. The changes are not yet clinical practice, but practitioners should understand them because they will shape the next generation of guidance.
Endotyping — classifying asthma by its underlying inflammatory mechanism rather than its trigger — is revealing that occupational asthma is more heterogeneous than previously assumed. The standard assumption that OA is predominantly eosinophilic (Type 2 inflammation) is challenged by sputum studies finding neutrophilic predominance in a substantial proportion of HMW-agent OA cases. This matters because anti-inflammatory treatment strategies, monitoring biomarkers, and prognostic predictions all depend on the inflammatory endotype.
Emerging biomarkers offer potential improvements in diagnostic accuracy. MicroRNA (miRNA) profiling has shown promise in distinguishing OA from non-occupational asthma in early-stage research. Volatile organic compound (VOC) breath analysis — including platforms like the Owlstone Medical Breath Biopsy system currently in clinical trials — represents a non-invasive diagnostic approach that could eventually complement or replace serial PEF monitoring.
Type 2 biomarkers as predictors of remission after exposure cessation are under active clinical investigation. A trial registered at the University Hospital Strasbourg (ClinicalTrials.gov NCT07006285, 2024/2025) is specifically evaluating whether T2 biomarker profiles can predict which OA patients will achieve remission after removal from exposure — a finding that would directly influence return-to-work decision-making.
Biologic therapies — omalizumab, mepolizumab, dupilumab, tezepelumab — have transformed the management of severe non-occupational asthma. Their applicability to severe occupational asthma is being explored, but remains off-label and understudied in the OA population specifically. The fundamental question these therapies raise is provocative: if biologics can control symptoms effectively, does that change the recommendation to remove the worker from exposure? The current clinical consensus is clear: no. Removal from exposure remains the standard, because biologics suppress symptoms without addressing the ongoing immunological sensitisation process. Continued exposure in a symptom-controlled but still-sensitised worker risks progressive airway remodelling that biologics may mask rather than prevent.
The excitement around these therapeutic advances should not distract from the primary-prevention imperative. The most cost-effective intervention for occupational asthma remains preventing sensitisation in the first place — not managing established disease with expensive therapies that cost thousands per month and require indefinite administration.
Employer Duties and Regulatory Frameworks: A Jurisdictional Comparison
Multinational organisations and HSE professionals operating across borders face a fragmented regulatory landscape for occupational asthma. No single framework covers all the duties an employer must fulfil, and what constitutes compliance in one jurisdiction may represent a violation in another.
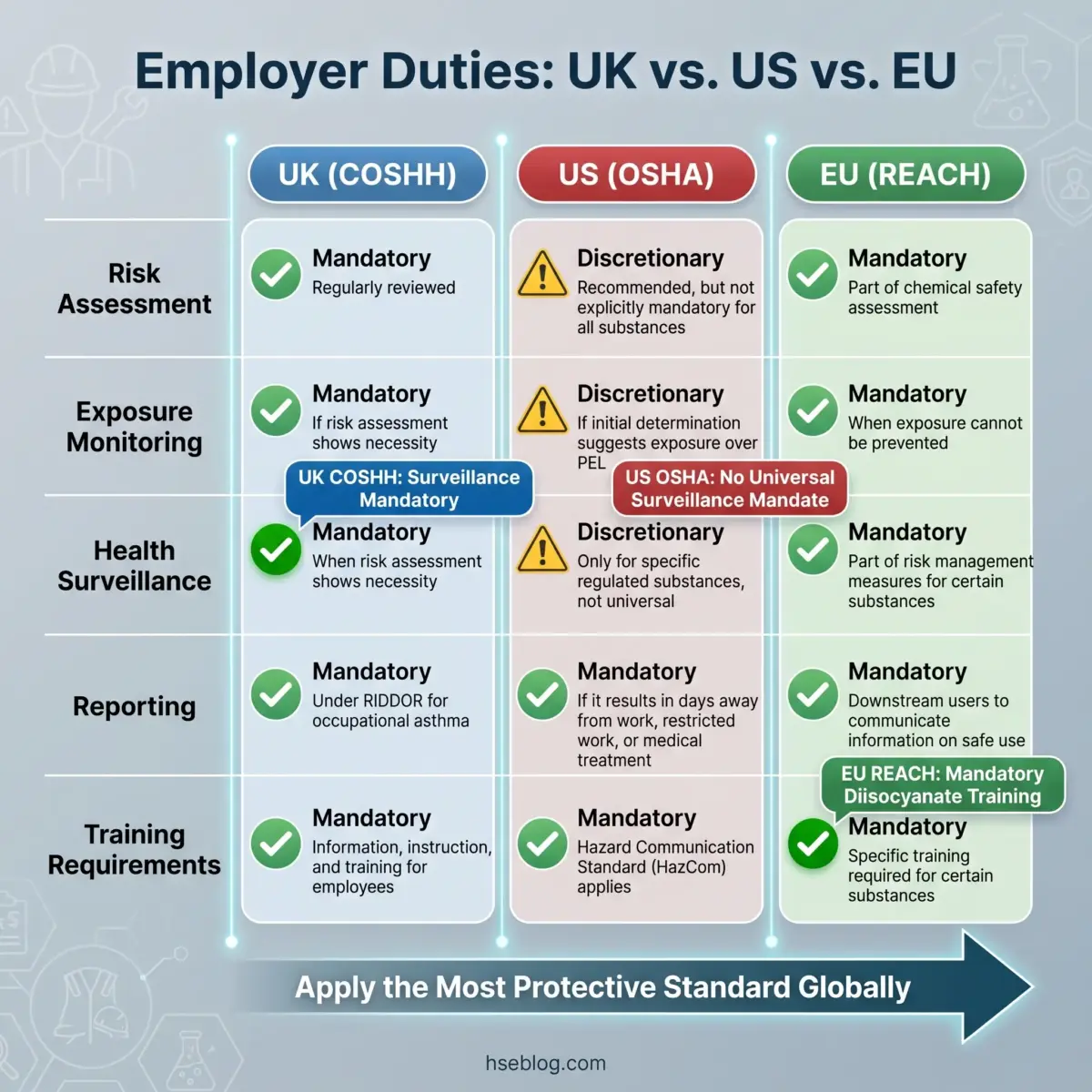
Under the COSHH Regulations 2002 (UK), the employer’s duties are the most explicit: prevent or adequately control exposure to substances hazardous to health, including respiratory sensitisers. Health surveillance under Regulation 11 is mandatory for all workers exposed to known sensitisers — not discretionary. LEV must be examined and tested at least every 14 months. Confirmed OA cases must be reported under RIDDOR 2013. The enforcement mechanism is direct: HSE inspectors can issue improvement and prohibition notices, and prosecutions for COSHH non-compliance carry unlimited fines.
In the US, OSHA has no single occupational asthma standard. Employer obligations are assembled from substance-specific PELs under 29 CFR 1910.1000, the respiratory protection standard (29 CFR 1910.134), and general recordkeeping requirements (29 CFR 1904). Medical surveillance provisions exist in some substance-specific standards but are not universal. An employer can be fully OSHA-compliant without conducting any health surveillance for sensitiser exposure — a gap that COSHH does not permit. NIOSH provides guidance and surveillance infrastructure through the SENSOR programme and its updated WRA reporting guidelines (February 2025), but these are advisory, not enforceable.
The EU framework is evolving rapidly. REACH Regulation 2020/1149 introduced mandatory training for all users of diisocyanate-containing products (≥0.1% by weight) effective August 2023, with three training tiers and five-year certification cycles. The European Parliament’s late-2024 approval of binding OELs for diisocyanates — if confirmed by the Council — will establish enforceable exposure limits across all member states for the first time. The EU approach is explicitly designed to reduce OA incidence, not merely document it.
The ILO provides global guidance frameworks but no enforceable standards. Its value is as a baseline reference in jurisdictions that lack detailed OA-specific regulation.
| Duty | UK (COSHH) | US (OSHA) | EU (REACH + proposed OELs) |
|---|---|---|---|
| Risk assessment | Mandatory, substance-specific | Required under General Duty Clause; substance-specific where standards exist | Mandatory under REACH; COSHH-equivalent duties in national transpositions |
| Exposure monitoring | Required where significant exposure risk | Required for some substance-specific standards | Required under REACH restriction for diisocyanates |
| Health surveillance | Mandatory for all sensitiser-exposed workers (Reg 11) | No universal mandate; some substance-specific provisions | Varies by member state; REACH restriction implies monitoring obligation |
| Reporting | Mandatory under RIDDOR | Recording under 29 CFR 1904; no specific OA reporting mandate | Varies by member state |
| Training | Required under COSHH (general duty) | Required under Hazard Communication Standard | Mandatory REACH training for diisocyanate users (3 tiers, 5-year renewal) |
| LEV testing | Every 14 months (COSHH) | No universal mandate | Varies by member state |
Jurisdiction Note: COSHH’s explicit health-surveillance requirement for sensitiser-exposed workers is a sharper legal duty than anything in OSHA’s general-industry framework. Multinational companies applying their US compliance standards globally risk non-compliance in the UK and EU. The safest approach: design surveillance programmes to the most protective standard and apply them globally.
Frequently Asked Questions
Conclusion
The industry’s most consequential failure in occupational asthma management is not a lack of regulation or technology — it is lateness. Late diagnosis after airway remodelling is irreversible. Late removal from exposure after sensitisation is entrenched. Late surveillance that documents disease rather than preventing it. The evidence consistently points in one direction: the earlier sensitisation is detected and exposure eliminated, the better the prognosis. Everything else — OEL debates, biologic therapies, regulatory harmonisation — is secondary to that timing.
The single highest-impact change most organisations can make is to close the gap between knowing a worker is exposed to a respiratory sensitiser and actually conducting meaningful surveillance. A programme that meets COSHH G402 standards — with pre-placement baselines, first-year six-weekly intervals, defined referral triggers, and quality-controlled spirometry — catches early sensitisation at the stage where removal from exposure still gives the worker a reasonable chance of recovery. Programmes that defer surveillance to annual intervals from the start, or that lack specific action triggers, discover disease rather than preventing it.
For practitioners navigating multi-jurisdictional operations, the approach is straightforward: design to the most protective standard and apply it globally. A surveillance programme built to COSHH and G402 specifications satisfies UK law, exceeds OSHA requirements, and aligns with the direction of EU REACH enforcement. The cost of robust surveillance is measured in spirometry appointments and occupational-physician referrals. The cost of its absence is measured in irreversible lung disease, compensation claims, enforcement action, and workers who cannot breathe.
Regulatory content in this article reflects general HSE professional understanding of UK, US, and EU requirements as of 2025. It is not legal advice. Specific compliance questions, enforcement situations, or prosecution risk should be directed to qualified legal counsel in the applicable jurisdiction.