

The exothermic reactor sat at the centre of everything — three feed streams converging into a jacketed vessel running at 185°C, with a pressure relief system sized for runaway conditions that the original designers hoped would never materialise. The piping and instrumentation diagram showed seventeen safety-critical instruments on that single reactor loop. But a diagram does not tell you what happens when the cooling water supply valve fails closed during a feed transition at 2 a.m. on a weekend shift with a contract operator at the board. That is what Process Hazard Analysis exists to answer.
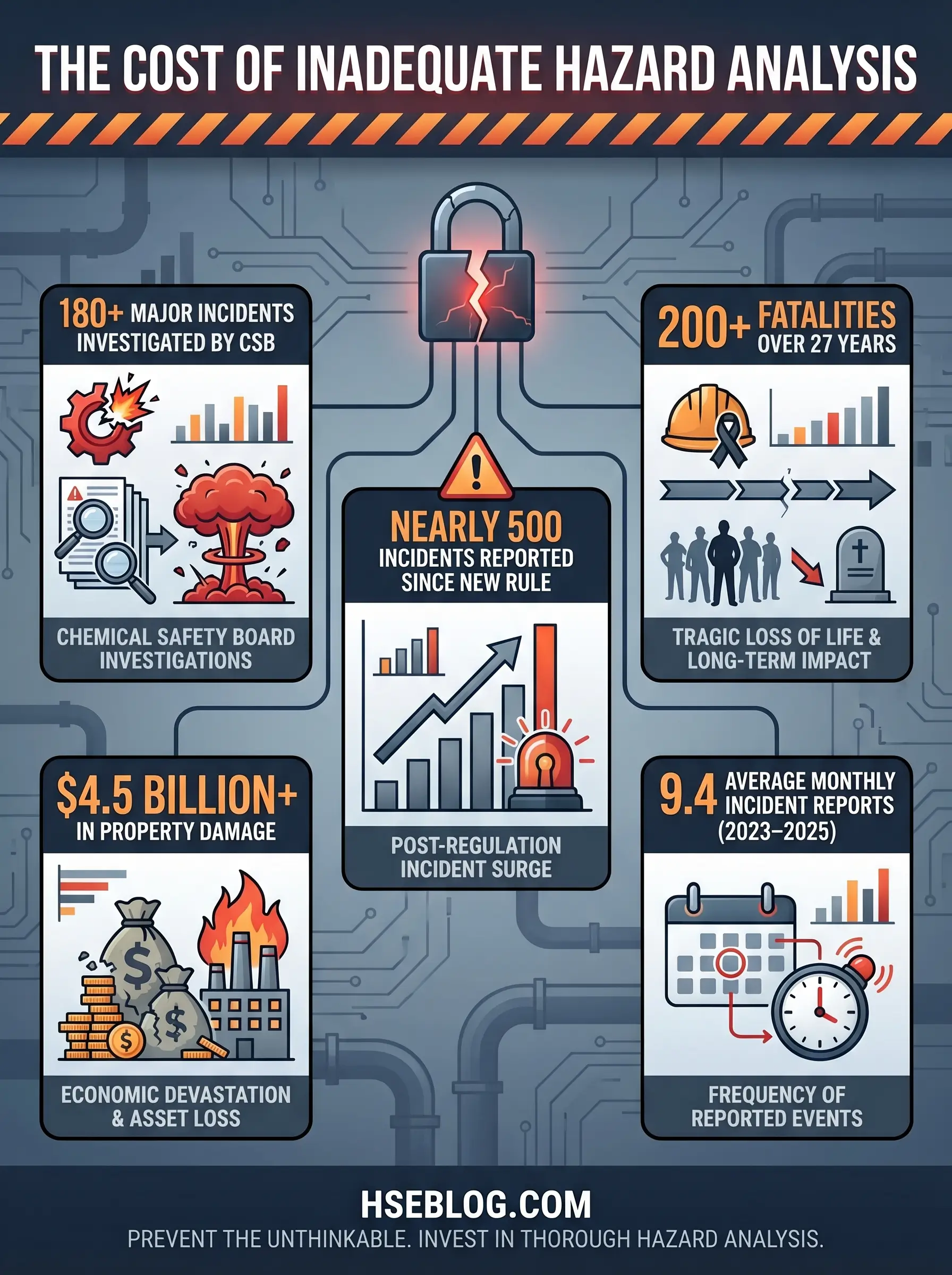
The consequences of skipping that question — or answering it superficially — are measured in lives, injuries, and billions in damage. The U.S. Chemical Safety Board has investigated nearly 180 major chemical incidents over 27 years, resulting in more than 200 fatalities and over 1,300 serious injuries. Since the CSB’s accidental release reporting rule took effect, the agency has received reports of nearly 500 serious chemical incidents across 43 states. These are not abstract numbers. They represent moments where a process hazard existed, was either unidentified or inadequately controlled, and found a path to harm. This article breaks down the PHA methods available, the steps to conduct one that actually protects people, the regulatory framework mandating it, and the common failures that reduce a critical safety exercise to a paper-filing obligation.
What Is a Process Hazard Analysis (PHA) and Why Does It Matter?
A Process Hazard Analysis is a systematic, team-based evaluation designed to identify, assess, and recommend controls for hazards associated with industrial processes handling highly hazardous chemicals. The Centre for Chemical Process Safety (CCPS) defines it as an organised effort to identify and evaluate the significance of hazards in a process — examining equipment, instrumentation, utilities, human actions, and external factors that could contribute to a loss event.
That definition matters because it distinguishes PHA from a generic risk assessment. A general risk assessment might evaluate slip-and-trip hazards in a warehouse. A PHA examines scenarios like the simultaneous failure of a high-pressure interlock and a relief valve on a reactor containing a thermally unstable intermediate — and asks what the blast radius looks like, whether the control room survives, and what happens to the community downwind. The scope encompasses fires, explosions, toxic releases, and major chemical spills across every mode of operation: normal production, startup, shutdown, maintenance, and emergency conditions.
The end objective is not to label a process “safe.” No process handling hazardous materials earns that label unconditionally. The objective is to detect unprotected scenarios — gaps where the existing safeguards are insufficient — and generate recommendations that trigger specific, assignable, trackable safety improvements. PHA applies across chemical processing, oil and gas, pharmaceuticals, power generation, and any manufacturing operation where a loss of containment could cause catastrophic harm.
I have facilitated PHA sessions on reactor systems, distillation trains, bulk storage terminals, and batch blending operations. The single constant across all of them is this: the study always finds something the design team missed. Always. Sometimes it is a valve that fails to the wrong position. Sometimes it is a human factors gap — an alarm that fires during a high-workload period when the operator cannot respond. The value of the exercise is directly proportional to the rigour applied.
Regulatory Requirements for Process Hazard Analysis
OSHA 29 CFR 1910.119(e) establishes the legal mandate: employers must perform an initial Process Hazard Analysis on every covered process and must use a methodology appropriate to the complexity of that process. The regulation does not leave the content to interpretation. Each PHA must address the hazards of the process, identify any previous incidents with catastrophic potential, evaluate engineering and administrative controls and their failure modes, assess consequences of control failures, examine facility siting relative to hazard zones, and consider human factors.
The team requirement is equally specific. OSHA mandates that the PHA team include at least one employee experienced with the process being analysed, one person with expertise in the specific PHA methodology, and personnel with relevant engineering and operations knowledge. A solo analyst reviewing drawings in an office does not meet this standard — a point that still generates compliance citations during PSM audits.
Documentation and lifecycle obligations complete the regulatory picture. PHA records must be retained for the life of the process — not archived and forgotten, but maintained as living references. Under 29 CFR 1910.119(e)(6), employers must update and revalidate each PHA at least every five years. The clock starts from the PHA completion date, not the initiation date.
The EPA’s Risk Management Program under 40 CFR Part 68 mirrors these requirements for facilities handling regulated substances above threshold quantities. Section 68.67 parallels OSHA’s PHA requirements for Program 3 processes, adding offsite consequence analysis obligations. Internationally, the EU Seveso III Directive (2012/18/EU) requires operators of major-accident-hazard establishments to prepare safety reports including systematic hazard identification and risk evaluation — achieving similar outcomes through a different regulatory mechanism.
Audit Point: During PSM compliance audits, inspectors commonly verify whether PHA revalidation dates have been met, whether recommendation resolution is documented with management sign-off, and whether the team composition met the minimum regulatory requirements. Missing any one of these triggers a finding.
How to Select the Right PHA Method for Your Process
Method selection is where most organisations either get PHA right or set themselves up for a study that consumes weeks of engineering time without proportional safety value. I have watched teams apply a full HAZOP — guide words, nodes, structured documentation — to a simple chemical storage tank with two connections and a vent. The study took three days. A What-If/Checklist review would have covered the same hazard space in four hours with equivalent thoroughness.
The selection should be driven by five factors: the complexity of the process, its lifecycle stage, whether a PHA has been conducted before, the experience level of the available team, and the regulatory expectations specific to the jurisdiction or facility type.
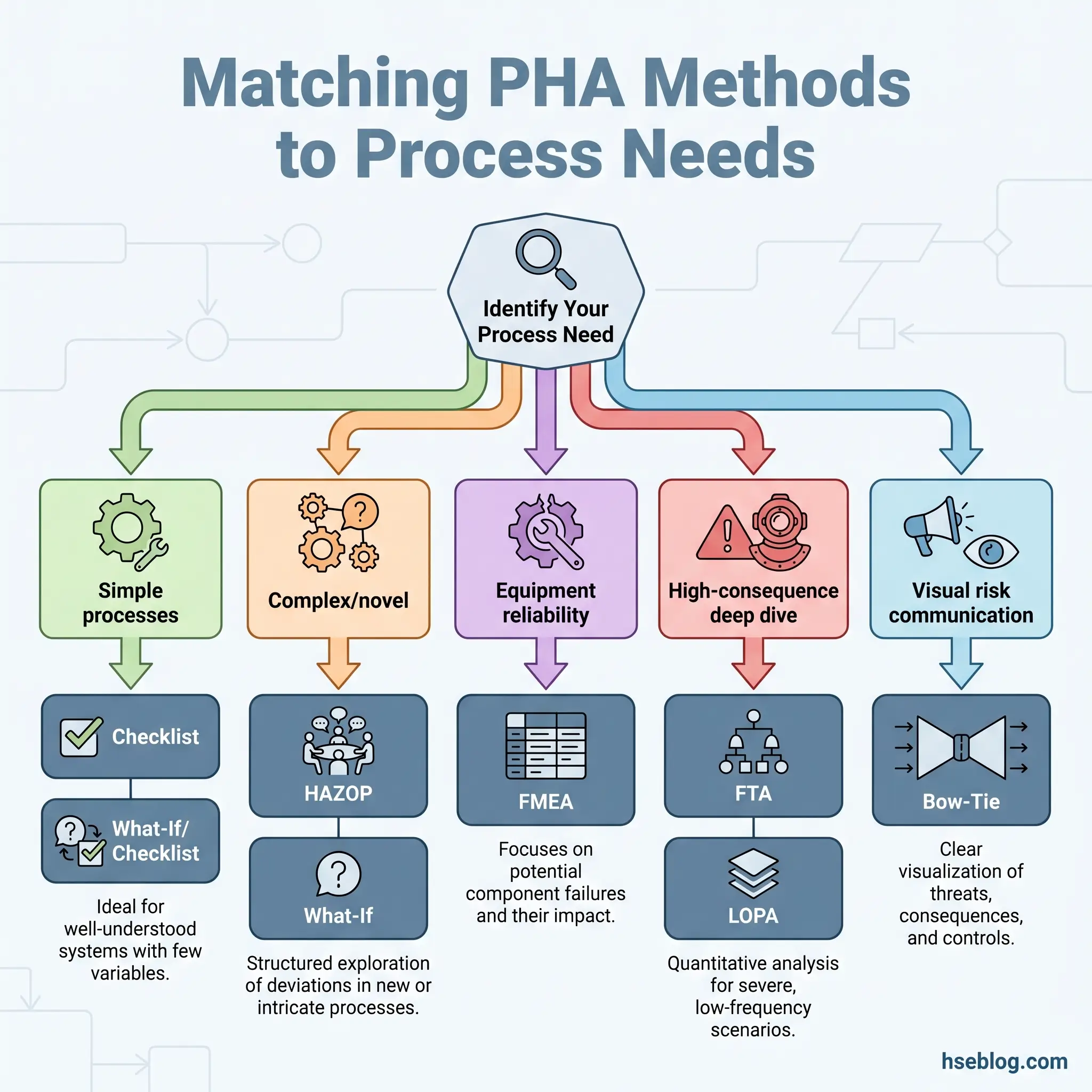
Non-scenario-based methods — checklists, safety reviews, and relative ranking approaches — suit well-understood processes with established operating histories and limited deviation potential. They verify compliance against known standards rather than exploring unknown hazard territory. Scenario-based methods — HAZOP, What-If, FMEA, and Fault Tree Analysis — suit complex, novel, or modified processes where the team needs to systematically explore “what could go wrong” beyond the obvious.
The What-If/Checklist combination deserves specific attention because it offers the efficiency advantages of brainstorming with the completeness assurance of a checklist backstop. For moderate-complexity processes, this combined approach frequently delivers the best balance of thoroughness and resource investment.
When a qualitative PHA identifies high-consequence scenarios with uncertain risk levels, quantitative follow-up methods — particularly Layer of Protection Analysis (LOPA) and Fault Tree Analysis (FTA) — provide the numerical rigour needed for decisions about Safety Instrumented Systems and additional protection layers.
The CCPS Guidelines for Hazard Evaluation Procedures, referenced in OSHA PSM Appendix C as the primary industry resource, provides detailed selection guidance mapped to process characteristics. Primatech’s comparison of PHA methods offers a practical reference matrix for matching techniques to specific situations.
| Factor | Non-Scenario Methods (Checklist, Safety Review) | Scenario Methods (HAZOP, What-If, FMEA) | Quantitative Follow-Up (LOPA, FTA) |
|---|---|---|---|
| Process Complexity | Simple, well-established | Complex, novel, or modified | High-consequence scenarios from prior PHA |
| Lifecycle Stage | Operating, routine review | Design, major modification, initial PHA | Post-PHA risk quantification |
| Team Experience Required | Moderate | High | Specialist analysts |
| Time Investment | Low | Moderate to high | Moderate |
| Output Type | Compliance verification | Scenario-based recommendations | Numerical risk reduction verification |
Core PHA Methods Explained
Each PHA method occupies a specific position in the hazard evaluation landscape. Understanding how each one works — its mechanics, its strengths, and its blind spots — is essential for selecting and applying the right tool.
Checklist Analysis
A checklist-based PHA compares a process systematically against a pre-developed list of known hazards, applicable standards, and accepted engineering practices. The analyst works through each item, confirming compliance or identifying gaps.
The method’s strength lies in its consistency and speed. For well-understood processes with extensive operating history — a standard acid storage system, a routine utility boiler, a conventional water treatment plant — a well-maintained checklist captures the known hazard landscape efficiently. The weakness is equally clear: a checklist can only identify hazards that someone has already anticipated and included. It cannot surface novel failure modes, unexpected interactions, or scenarios unique to a specific installation’s configuration.
Checklists require ongoing maintenance. A list developed in 2010 for a chlorine dosing system will not include failure modes associated with variable-speed drives retrofitted in 2019. An outdated checklist creates false assurance — every box ticked, critical hazards missed. On one facility I supported, the team was using a 12-year-old checklist for a process that had undergone three major modifications. The checklist passed the process. A subsequent What-If review identified four uncontrolled scenarios.
What-If Analysis
What-If analysis operates on structured brainstorming. The team examines a process by posing open-ended hypothetical questions: “What if the feed pump loses suction?” “What if the wrong raw material is charged?” “What if the nitrogen blanket is lost during a thunderstorm?” Each scenario is then evaluated for causes, consequences, existing safeguards, and the need for additional controls.
The flexibility of the method makes it particularly valuable for situations that resist the rigid structure of HAZOP — batch operations with variable recipes, startup and shutdown sequences, Management of Change reviews where the team needs to rapidly assess a proposed modification. During a MOC review for a solvent changeover on a reactor unit, the What-If approach let us explore the implications across vapour pressure differences, static accumulation characteristics, and waste treatment compatibility in a single session.
The method’s limitation is its dependence on the team’s collective experience and the facilitator’s ability to steer the discussion comprehensively. An inexperienced team may fail to ask the critical questions. The What-If/Checklist combination addresses this by using the checklist as a systematic backstop — the brainstorming explores creative scenarios while the checklist ensures no established hazard category is overlooked.
HAZOP Study (Hazard and Operability Study)
HAZOP is the most widely applied PHA technique globally, and for good reason. Its structured, guide-word-driven methodology provides the most auditable, repeatable, and comprehensive hazard identification process available for continuous chemical operations. IEC 61882:2016, aligned with ISO 31000:2018, provides the international standard for HAZOP application, terminology, and documentation.
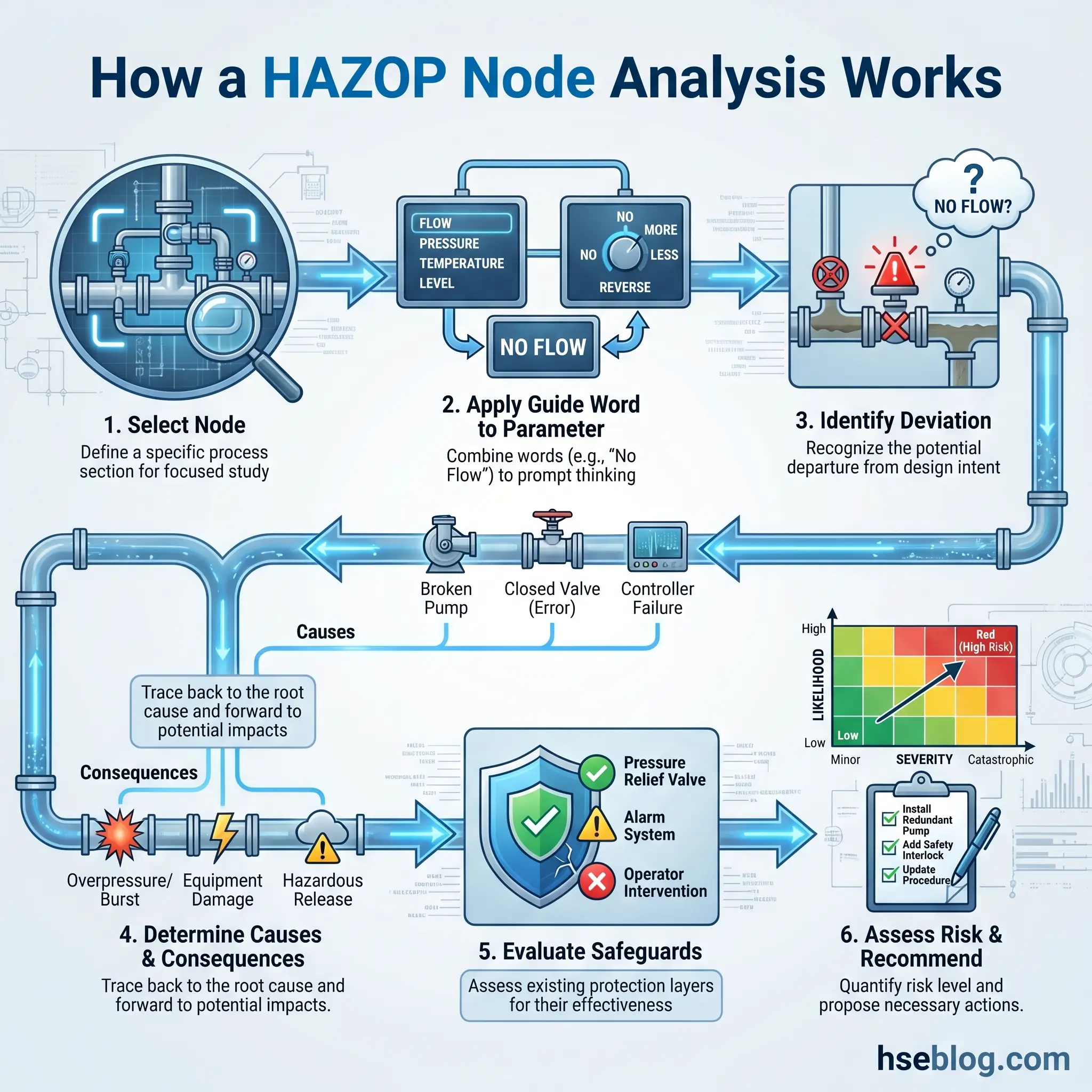
The process divides the system into discrete nodes — typically defined by major equipment boundaries or significant changes in process conditions. At each node, the team applies standardised guide words (No, More, Less, Reverse, As Well As, Part Of, Other Than) to process parameters (flow, pressure, temperature, level, composition, phase, reaction rate) to generate deviations from the design intent.
Consider a reactor feed system. Applying “No” to “Flow” generates the deviation “No Flow to Reactor.” The team then identifies causes (pump failure, blocked line, closed valve, loss of feed supply), evaluates consequences (reaction starvation, thermal runaway due to loss of cooling capacity utilisation, batch quality failure), reviews existing safeguards (low-flow alarm, pump status interlock, batch management system), and assesses residual risk. If the risk is unacceptable, the team generates a recommendation — a new interlock, a procedure change, a design modification — with an assigned owner and deadline.
“What does the operator actually see when this happens?” That question, posed during a HAZOP on a distillation column feed system, shifted the entire discussion. The team had been evaluating a high-temperature deviation assuming the DCS alarm would alert the board operator. The senior operator on the team pointed out that during column startup, the operator was physically at the column base, monitoring the reboiler — not watching the screen. That single contribution changed the safeguard assessment and generated a recommendation for a field alarm horn.
HAZOP’s limitation is its time intensity. A complex process unit with fifty nodes can require two to three weeks of team sessions. For simple, well-understood processes, that investment is disproportionate. HAZOP is also less naturally suited to batch operations or procedural analysis without modification to the standard continuous-process approach.
Failure Mode and Effects Analysis (FMEA)
FMEA takes a bottom-up, component-level approach. Rather than examining process deviations at a system level, it asks three questions about each piece of equipment: What can fail? How can it fail? What happens when it fails?
This equipment-level focus makes FMEA the natural complement to HAZOP’s process-level analysis. Where HAZOP identifies that “loss of cooling flow to the reactor” creates a runaway scenario, FMEA examines the cooling water control valve specifically: the valve can fail open (overcooling, potential thermal shock), fail closed (loss of cooling, runaway conditions), fail to respond (stuck in position, gradual deviation), or develop a leak (loss of containment, environmental release). Each failure mode receives a Risk Priority Number (RPN) combining severity, probability of occurrence, and detectability.
FMEA excels in mechanical integrity reviews and equipment reliability programmes. It is less effective at identifying systemic hazards — those arising from the interaction between multiple components, human actions, and process conditions simultaneously.
Fault Tree Analysis (FTA)
FTA inverts the analytical direction. Where most PHA methods work forward from causes to consequences, FTA starts with a defined undesired “top event” — a reactor runaway, a toxic release, an explosion — and works backward through Boolean logic gates (AND, OR) to map every possible combination of failures, errors, and conditions that could produce it.
This deductive approach is typically not a standalone PHA method. It requires a top event to be defined first, which means an initial qualitative PHA must have already identified the scenarios worth deeper investigation. FTA’s value lies in quantifying the probability of high-consequence events and identifying critical failure combinations — the specific sets of simultaneous failures that represent the most credible threat paths.
Unlike team-based methods, FTA is usually performed by one or two specialist analysts with strong backgrounds in reliability engineering and probability theory. Its output — a logic diagram with quantified failure probabilities — feeds directly into safety integrity level determination and protective system design.
Bow-Tie Analysis
Bow-Tie analysis has gained significant traction in oil and gas, major hazard facilities, and regulatory environments because it communicates risk in a format that non-technical stakeholders can immediately understand. The visual structure places a central hazardous event — a loss of containment, an ignition, a toxic release — at the centre of a diagram, with causes mapped on the left side (drawing from Fault Tree logic) and consequences mapped on the right side (drawing from Event Tree logic).
Preventive barriers appear between causes and the central event. Mitigative barriers appear between the central event and consequences. Each barrier is specific, identifiable, and auditable — a relief valve, a gas detection system, an emergency shutdown procedure, a blast wall. The format makes it immediately visible where barriers are thin, missing, or degraded.
Increasingly, Bow-Tie is used alongside HAZOP and LOPA as part of an integrated barrier management framework. The hazard scenarios identified in HAZOP feed the Bow-Tie’s central events. The barriers mapped in the Bow-Tie provide the structure for ongoing barrier health monitoring during operations.
Layer of Protection Analysis (LOPA)
LOPA bridges the gap between qualitative PHA and quantitative risk decisions. It is a semi-quantitative method applied after a qualitative PHA identifies scenarios requiring deeper evaluation — typically those where the team cannot confidently determine whether existing safeguards reduce risk to tolerable levels.
The method evaluates each scenario by assigning order-of-magnitude frequency estimates to the initiating event and probability of failure on demand values to each Independent Protection Layer (IPL). An IPL must be independent, auditable, and capable of preventing the consequence on its own. The combined risk reduction from all IPLs is compared against the facility’s tolerable risk target.
LOPA’s most common application is determining whether a Safety Instrumented Function is needed and, if so, at what Safety Integrity Level. This directly connects PHA findings to the IEC 61511 framework for functional safety in the process industries. Without LOPA or an equivalent quantitative step, the link between hazard identification and protective system specification remains subjective.
Field Test: After your next PHA session, review each recommendation. Can you trace a clear line from the identified scenario, through the risk assessment, to the specific control action recommended? If that chain is broken at any point — if the recommendation does not directly address the scenario’s uncontrolled risk — the study has a documentation gap that will surface during revalidation.
Step-by-Step Procedure for Conducting a Process Hazard Analysis
The procedural framework for conducting a PHA follows a logical sequence from scoping through documentation and resolution. Each step builds on the previous one, and shortcuts at any stage compromise the final product.
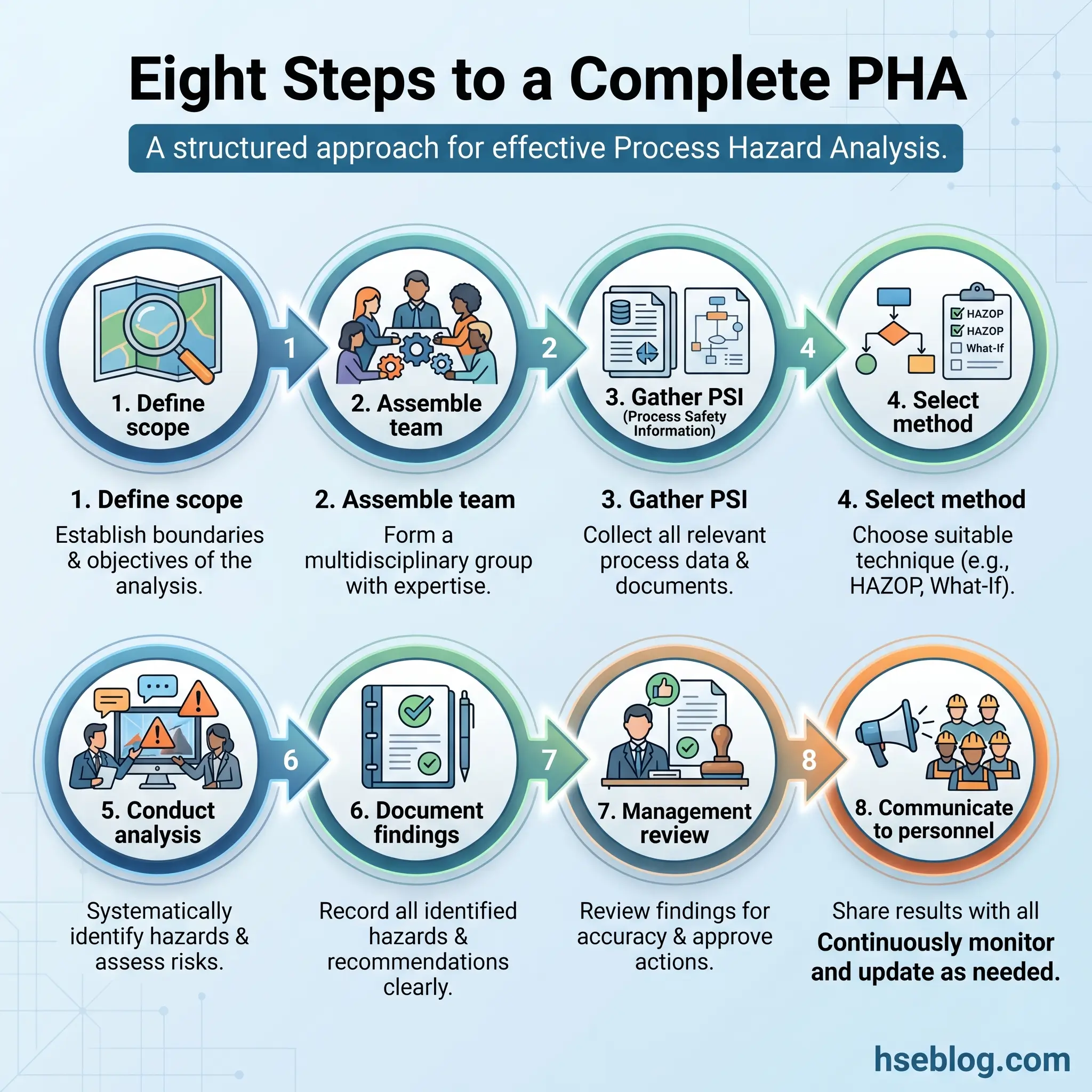
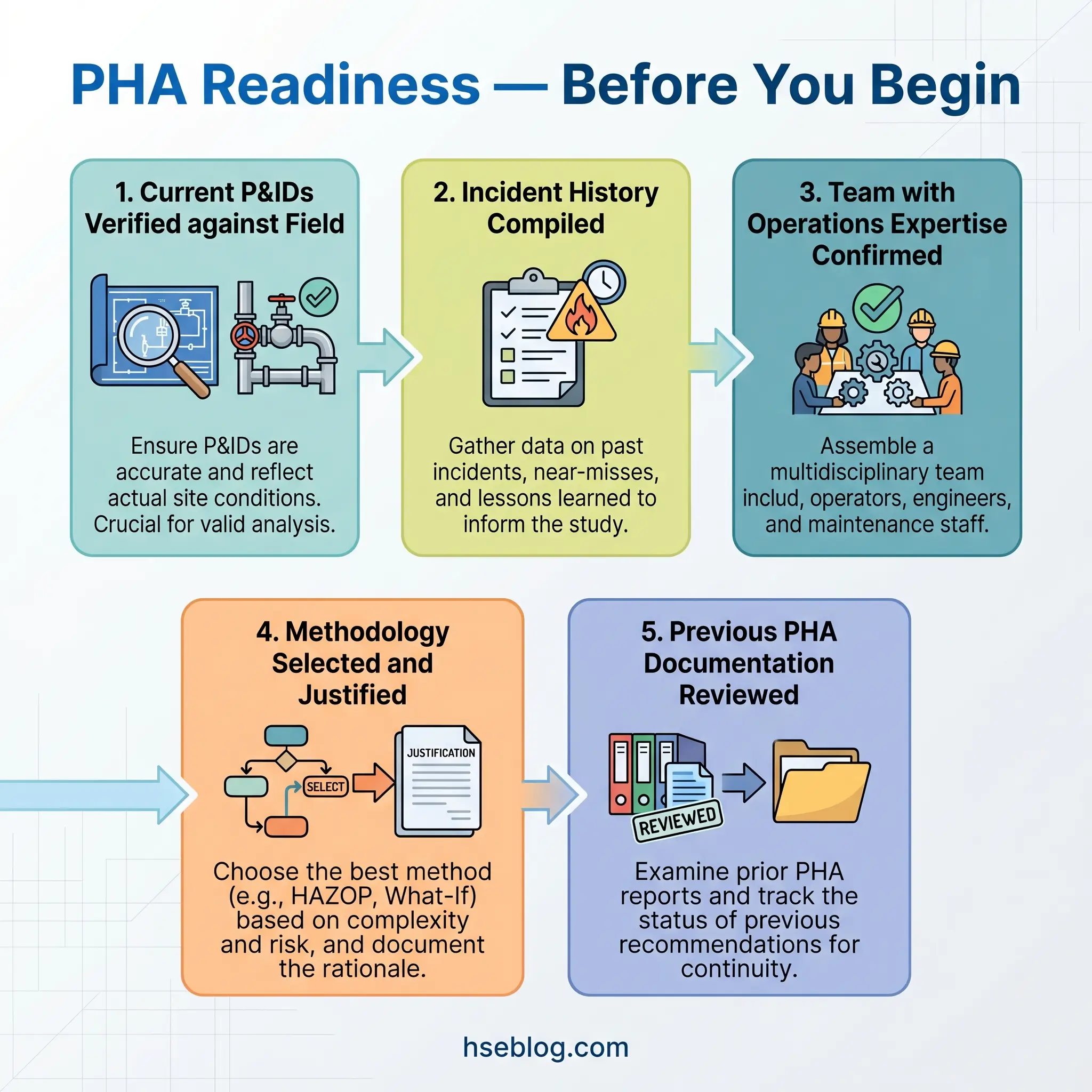
- Define scope, objectives, and boundaries. Establish which process or process section will be analysed, which operating modes are included (normal, startup, shutdown, maintenance, emergency), and which lifecycle phase the study addresses (design, commissioning, operating, modification, decommissioning). A scope that is too broad produces an unfocused study. A scope that is too narrow misses interactions between connected systems.
- Assemble the PHA team. OSHA requires, at minimum, one person experienced with the process, one person with engineering expertise, and one person knowledgeable in the PHA methodology being used. Effective teams add experienced operators, maintenance technicians who know the equipment’s actual condition, and instrument or controls engineers who understand the safety system architecture. The facilitator must be someone who can maintain analytical structure while managing the interpersonal dynamics of a multidisciplinary group.
- Gather process safety information. Before the first session, the team needs current piping and instrumentation diagrams, process flow diagrams, operating procedures, emergency procedures, equipment data sheets, safety data sheets for all hazardous materials, incident and near-miss history, and previous PHA documentation. “I once sat down for a PHA kickoff where the P&IDs were three revisions behind,” a colleague who facilitates PHAs across multiple sites told me. “We spent the first day updating drawings instead of identifying hazards.”
- Select the appropriate methodology. Match the PHA technique to the process complexity, team experience, and study objectives using the selection framework described earlier. Document the rationale for the selection — auditors verify this.
- Conduct the analysis sessions. Divide the process into logical nodes or subsystems. For each node, systematically identify hazards using the selected methodology, evaluate causes, determine consequences with and without existing safeguards, and assess risk using the facility’s risk matrix. The facilitator must ensure the team explores all operating modes for each node — not just steady-state normal operation.
- Document findings and develop recommendations. Each identified scenario must be recorded with its cause, consequence, existing safeguards, risk ranking, and — where risk is unacceptable — a specific recommendation. Recommendations need assigned owners, clear descriptions of the required action, and completion deadlines.
- Conduct management review and resolve recommendations. Management must formally respond to every recommendation, documenting acceptance, alternative action, or rejection with written rationale. This is not optional. OSHA requires that recommendations be resolved in a timely manner and that the resolution be documented. Open recommendations that persist across revalidation cycles are a compliance red flag and, more importantly, represent ongoing uncontrolled risk.
- Communicate findings to affected personnel. Operators, maintenance workers, and contractors working on the process must be informed of relevant PHA findings — particularly new procedures, modified interlocks, and updated emergency response actions.
Who Should Be on the PHA Team?
The quality of a Process Hazard Analysis is determined more by who sits around the table than by which methodology is applied. I have seen thorough, well-documented PHAs conducted with a simple What-If approach by an experienced, multidisciplinary team — and I have seen expensive, software-driven HAZOPs produce shallow, repetitive findings because the wrong people were in the room.
OSHA establishes the minimum: expertise in engineering, expertise in process operations, experience with the specific process being studied, and competence in the PHA methodology. In practice, the effective minimum is broader.
The PHA facilitator sets the analytical standard. This person guides the systematic discussion, prevents the team from fixating on familiar scenarios while ignoring uncomfortable ones, manages dominant personalities, draws out quiet operators who hold critical knowledge, and maintains documentation quality. Third-party facilitators bring independence and reduce the groupthink that can develop within a facility’s own engineering team — an investment that consistently improves study rigour.
Experienced operators provide the ground-truth reality check. They know which alarms are nuisance alarms that get silenced. They know which procedures are followed as written and which have unofficial workarounds. They know what actually happens at 3 a.m. when staffing is reduced and equipment is running differently than the daytime engineering team assumes. A PHA without experienced operator input is a theoretical exercise.
Process engineers contribute the design-intent perspective — why the system was designed this way, what the equipment limitations are, where the design margins sit. Maintenance personnel bring equipment condition knowledge — which valves are difficult to operate, which instruments drift, which relief devices have a history of fouling. Instrument and controls engineers understand the safety system architecture, the interlock logic, and the failure modes of the automated safeguards the team relies on.
Specialist subject matter experts enter when the process demands it: reactive chemistry consultants for processes with runaway potential, corrosion engineers for ageing equipment or aggressive services, human factors specialists for control room and procedural analysis.
PHA Revalidation: The Five-Year Lifecycle Requirement
OSHA 29 CFR 1910.119(e)(6) mandates that each PHA must be updated and revalidated at least every five years by a qualified team. This is not a re-reading of the old study with a fresh signature. It is a substantive review to determine whether the original PHA remains valid against the current process configuration, operating experience, and regulatory landscape.
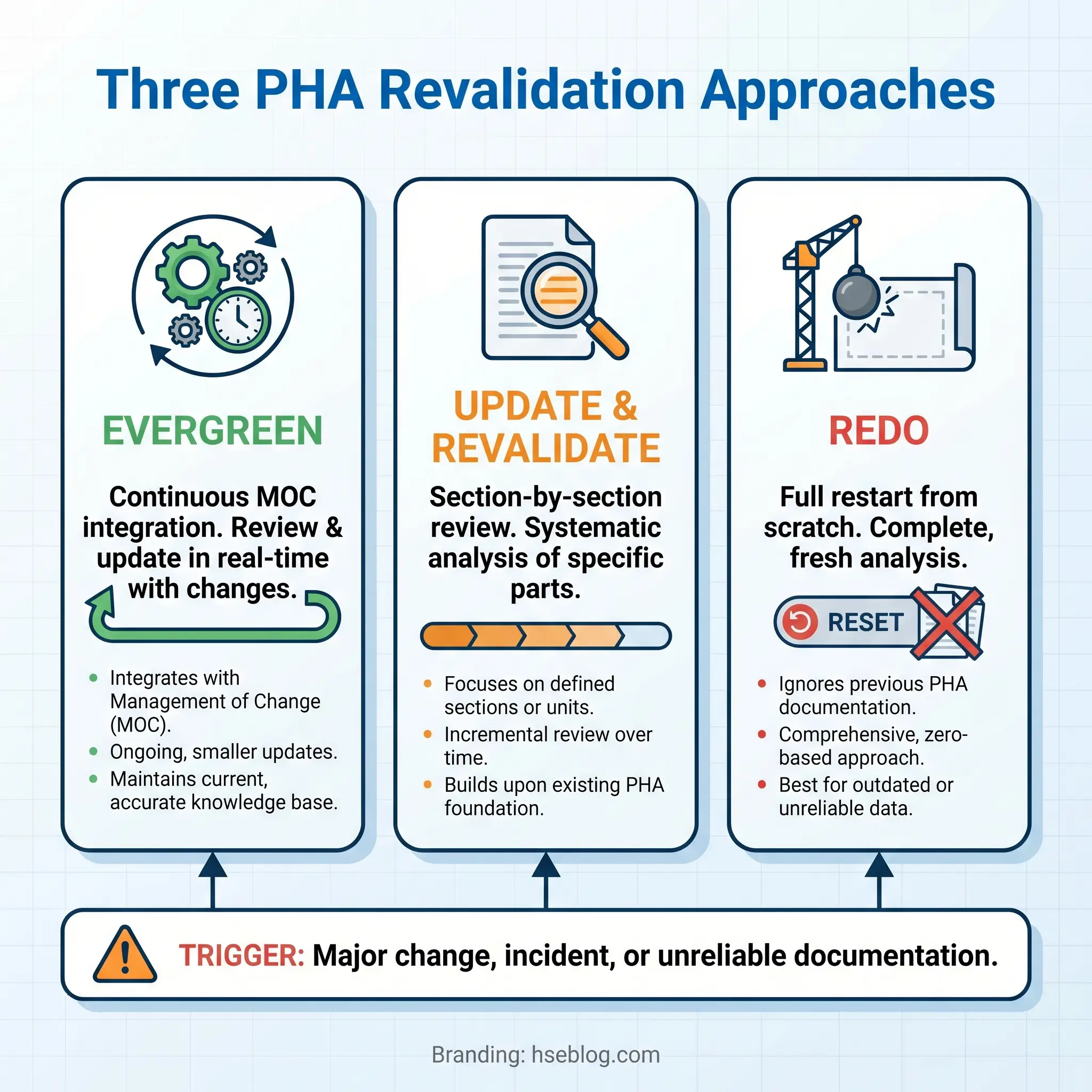
Three distinct revalidation approaches exist, and the choice depends on how well the original PHA has been maintained.
The Evergreen approach works for facilities with disciplined Management of Change programmes. Every process modification triggers a hazard review, and those reviews are documented and incorporated into the PHA record continuously. At the five-year mark, the revalidation becomes a confirmation that all changes have been captured and that no systemic gaps have developed. This is the most efficient approach — and the hardest to sustain.
The Update and Revalidate approach is the industry standard. The team reviews the previous PHA section by section against the current process. Changes since the last study — new equipment, modified procedures, resolved and unresolved recommendations, incidents that have occurred — are evaluated for their impact on the existing analysis. New scenarios are added. Obsolete scenarios are retired. Risk rankings are reassessed against current conditions.
The Redo approach starts from scratch. This becomes necessary when the original PHA used an inappropriate methodology, when the process has changed so substantially that the original analysis no longer maps to the current operation, or when the documentation quality is so poor that the revalidation team cannot verify completeness. Redoing a PHA is expensive, but building a new study on unreliable foundations is more costly.
Several triggers can require revalidation before the five-year deadline: significant process changes that accumulate beyond what individual MOC reviews addressed, a major incident or near-miss that exposes gaps in the existing analysis, regulatory changes that alter compliance requirements, or the departure of key personnel whose institutional knowledge was not captured in the documentation.
Watch For: The most common revalidation failure is not missing the deadline — it is treating revalidation as a paperwork exercise. If the revalidation team cannot articulate what changed since the last study and how those changes affect the hazard profile, the revalidation is not meeting its regulatory purpose.
How PHA Integrates with Other PSM Elements
Process Hazard Analysis does not exist in isolation. It occupies a central position within the Process Safety Management system, with dependencies running in both directions across nearly every other PSM element.
PHA depends on accurate Process Safety Information (PSI). If the P&IDs are outdated, the operating procedures incomplete, or the equipment data sheets missing, the PHA team is analysing a process that does not exist as described. I have walked into PHA kickoff meetings and asked the team to verify three specific instrument tag numbers against the field installation. In two separate cases, instruments shown on the drawings had been removed during a previous turnaround without the P&ID being updated. The PHA would have credited safeguards that were physically absent.
In the other direction, PHA findings feed directly into Operating Procedures — new steps, modified sequences, additional precautions identified during the study. They feed into Training Programs — operators must understand the hazard scenarios relevant to their unit and the reasoning behind safety-critical procedures. They feed into Emergency Response Plans — PHA scenarios involving toxic releases, fires, or explosions define the emergency scenarios that response plans must address.
Management of Change (MOC) represents the most dynamic integration point. Every process modification — new equipment, changed operating parameters, different raw materials, altered procedures — requires a hazard review. That review frequently uses PHA methodology. The findings from MOC reviews must be incorporated back into the master PHA documentation so that the next revalidation reflects the current process.
Incident Investigations should be cross-referenced against the existing PHA. When an incident occurs, one of the first questions should be: “Was this scenario identified in the PHA?” If yes, the investigation examines why the safeguards failed. If no, the PHA has a gap that requires immediate correction.
Pre-Startup Safety Reviews (PSSR) verify that PHA recommendations for new or modified processes have been implemented before the process goes live. Mechanical Integrity programmes implement PHA recommendations related to equipment-based safeguards — inspection frequencies, testing protocols, and replacement criteria for safety-critical components.
Common Mistakes That Undermine PHA Quality
Certain failure patterns repeat across facilities, industries, and regulatory jurisdictions. Recognising them is the first step toward preventing them.
- Inadequate team composition is the most damaging error. A PHA conducted without experienced operations representation misses the ground-level reality of how the process actually runs. A study led by an inexperienced facilitator drifts into unfocused discussion, skips difficult scenarios, and produces documentation that cannot withstand audit scrutiny.
- Rushing the study produces predictable results. When management schedules a three-day HAZOP for a process that requires five, the team either cuts nodes short, skips non-normal operating modes, or reduces the depth of consequence evaluation. Every one of these shortcuts leaves hazard scenarios unexamined. On a specialty chemicals unit I supported, the original PHA had allocated two days for a reactor system with six distinct operating phases. The revalidation team — given adequate time — identified eleven additional scenarios that the rushed original study had missed, three of which required hardware modifications.
- Using the wrong methodology wastes resources in one direction and misses hazards in the other. A full HAZOP on a simple tank farm is disproportionate. A checklist review on a novel reactive process is dangerously insufficient.
- Failing to address all modes of operation is a gap that persists across the industry. Many PHAs focus overwhelmingly on normal steady-state operation and give cursory treatment to startup, shutdown, maintenance, and emergency conditions. Yet historical incident data consistently shows that non-routine operations — particularly startups after maintenance and emergency shutdowns — account for a disproportionate share of process safety events.
- Leaving recommendations unresolved across revalidation cycles signals a systemic management failure. If a PHA identifies a scenario requiring action in 2019 and the same recommendation appears unresolved in the 2024 revalidation, the facility has been operating with a known, acknowledged, uncontrolled risk for five years.
- Not updating PSI before beginning the PHA means the team is analysing a process that may not match the physical installation. This is not a procedural nicety. It directly compromises the validity of every finding.
The Role of Technology and AI in Modern Process Hazard Analysis
Digital tools have been part of PHA practice for years — software platforms that manage study documentation, track recommendations, and enable teams to work from structured databases rather than spreadsheets. What has shifted in 2024–2026 is the entry of artificial intelligence into the hazard identification process itself.
AI-assisted PHA tools are moving from research prototypes to commercial deployment. Natural language processing algorithms parse historical incident databases, maintenance records, and operating logs to suggest hazard scenarios that a team might not generate through brainstorming alone. DEKRA’s Digital PHA approach, for example, has demonstrated time savings of up to 70% for medium-sized projects compared to conventional studies by automating portions of the scenario generation and documentation phases.
Digital twin technology introduces another dimension. Virtual process models allow PHA teams to simulate deviations — what happens to reactor temperature if this valve fails, how quickly does pressure build if the relief path is partially blocked — before or during the study session. This converts abstract what-if questions into visible, quantifiable process responses.
Academic research published in early 2026 on AI-enabled HAZOP studies, along with AIChE publications from 2024, explores how machine learning can automate portions of the brainstorming phase by predicting likely deviations and failure scenarios from process configuration data. The potential extends to knowledge continuity: as experienced process safety professionals retire, AI systems trained on decades of PHA documentation could help preserve institutional hazard knowledge that would otherwise be lost.
The critical limitation remains unchanged. AI systems are only as good as their training data, and they cannot replicate the contextual judgement that an experienced operator or engineer brings to a PHA session. A machine learning model can flag that a loss-of-cooling scenario is statistically likely on a reactor system. It cannot tell you that the cooling water header on this specific unit drops pressure every summer when the adjacent unit runs its cooling tower at full capacity — a site-specific condition that a veteran operator mentions in the first five minutes of the session.
AI augments PHA. It does not replace the multidisciplinary team that OSHA requires and that effective hazard analysis demands.
Frequently Asked Questions
The pattern the industry gets wrong most consistently is treating PHA as a compliance event rather than an operational intelligence exercise. A study conducted to satisfy a regulatory deadline produces a binder that sits on a shelf. A study conducted to find out what can kill someone on this unit, under these conditions, with this crew — that study changes how people operate, maintain, and manage the process.
The single highest-impact change any facility can make is investing in team quality. Budget for experienced facilitators. Protect operator time so they can attend full sessions without being pulled back to the unit. Bring in the maintenance technician who has been troubleshooting that temperamental control valve for six years. The method matters less than the minds applying it.
Process safety is not static. The CSB’s February 2026 incident data — 81 serious chemical incidents in 31 states resulting in 16 fatalities and 75 serious injuries — confirms that the gap between regulatory intent and field execution remains wide. Process Hazard Analysis, conducted with rigour, is the mechanism designed to close that gap. Whether it succeeds depends entirely on whether the people responsible for it treat it as an obligation or as an opportunity to prevent the next catastrophic loss.